
Intrauterine Exposures and Maternal Health Status during Pregnancy in Relation to Later Child Health: A Review of Pregnancy Cohort Studies in Europe

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
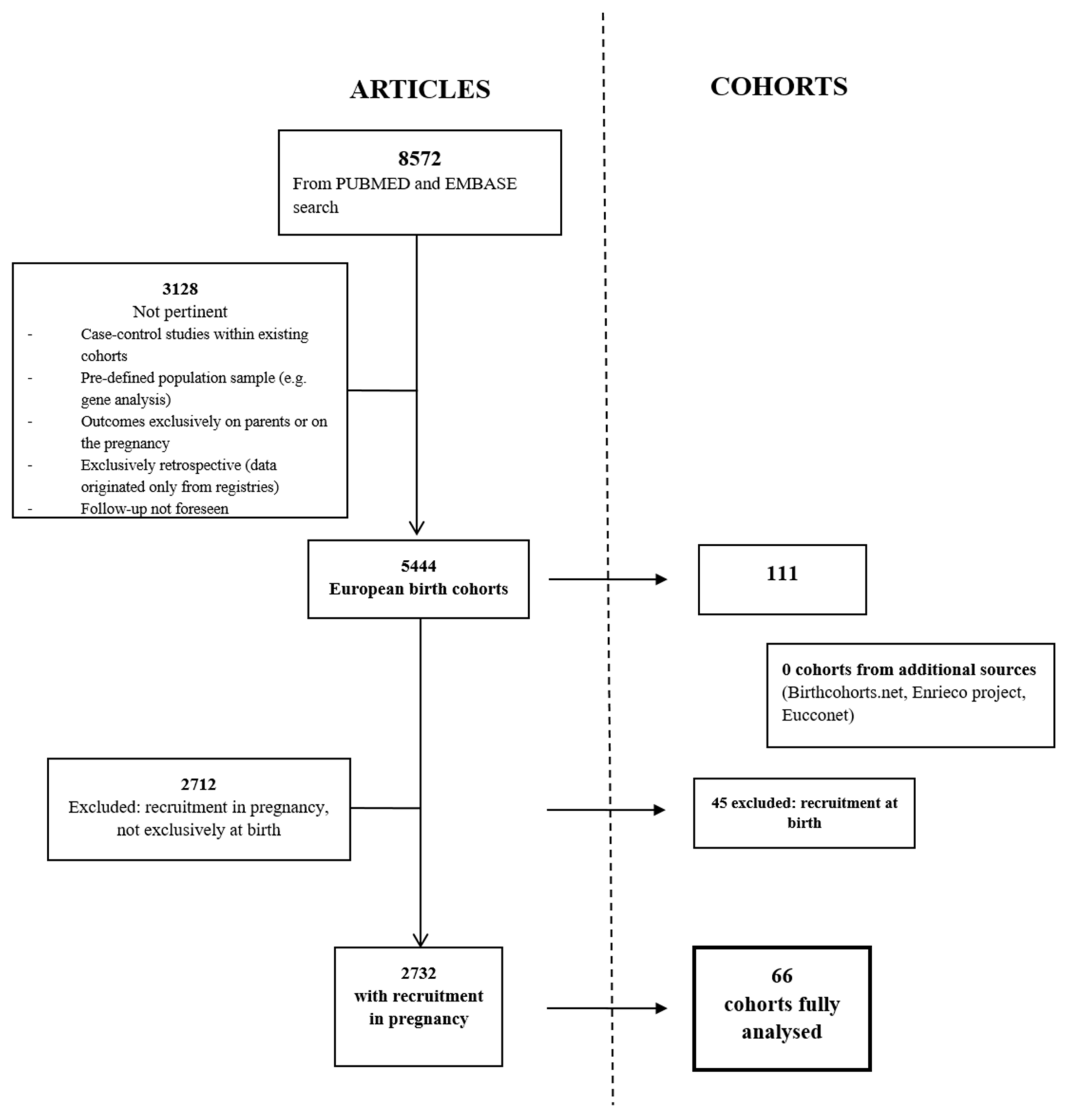
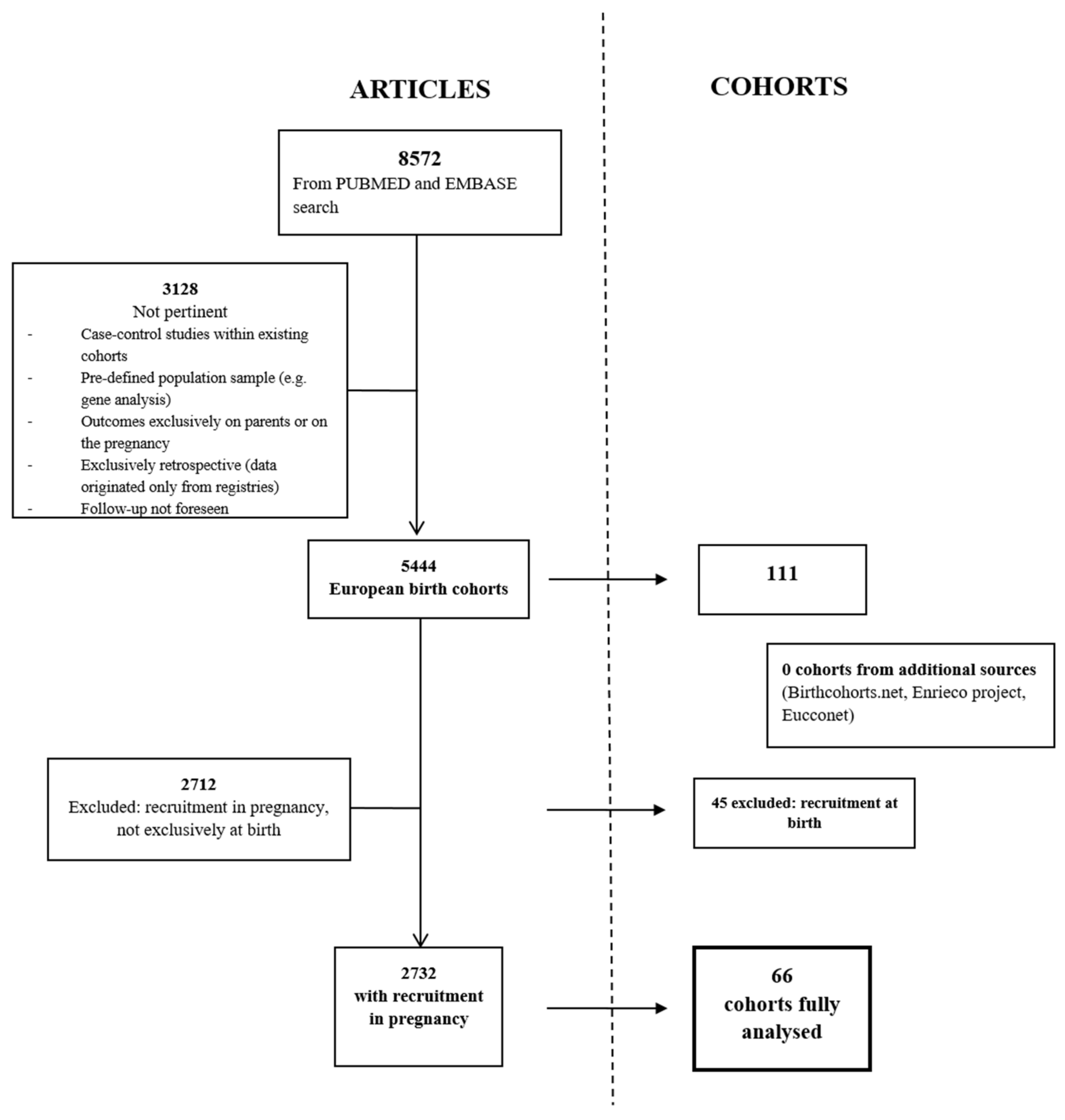
2.1. Cohort Identification and Selection
2.2. Data Extraction
2.3. Data Synthesis
3. Results
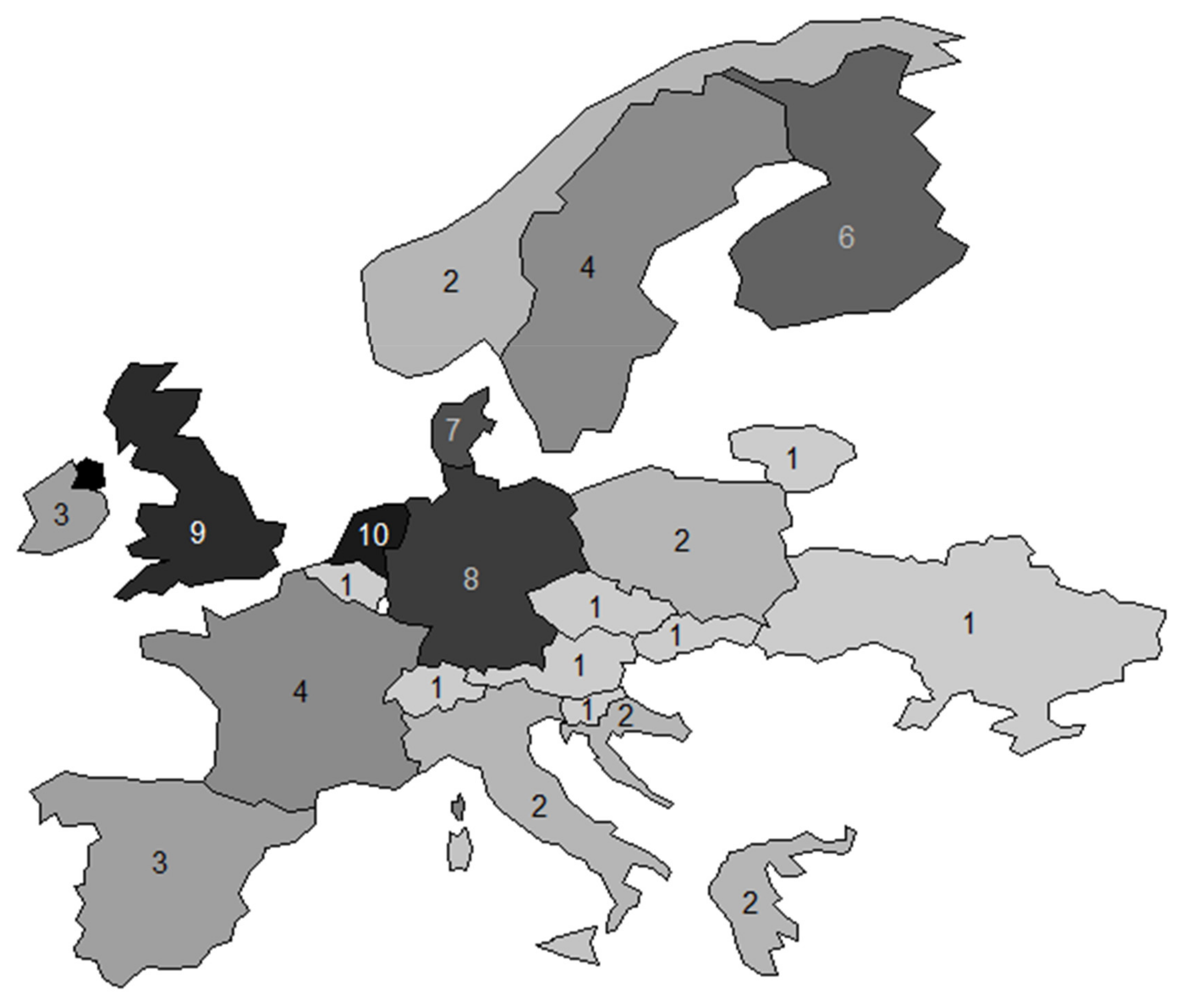
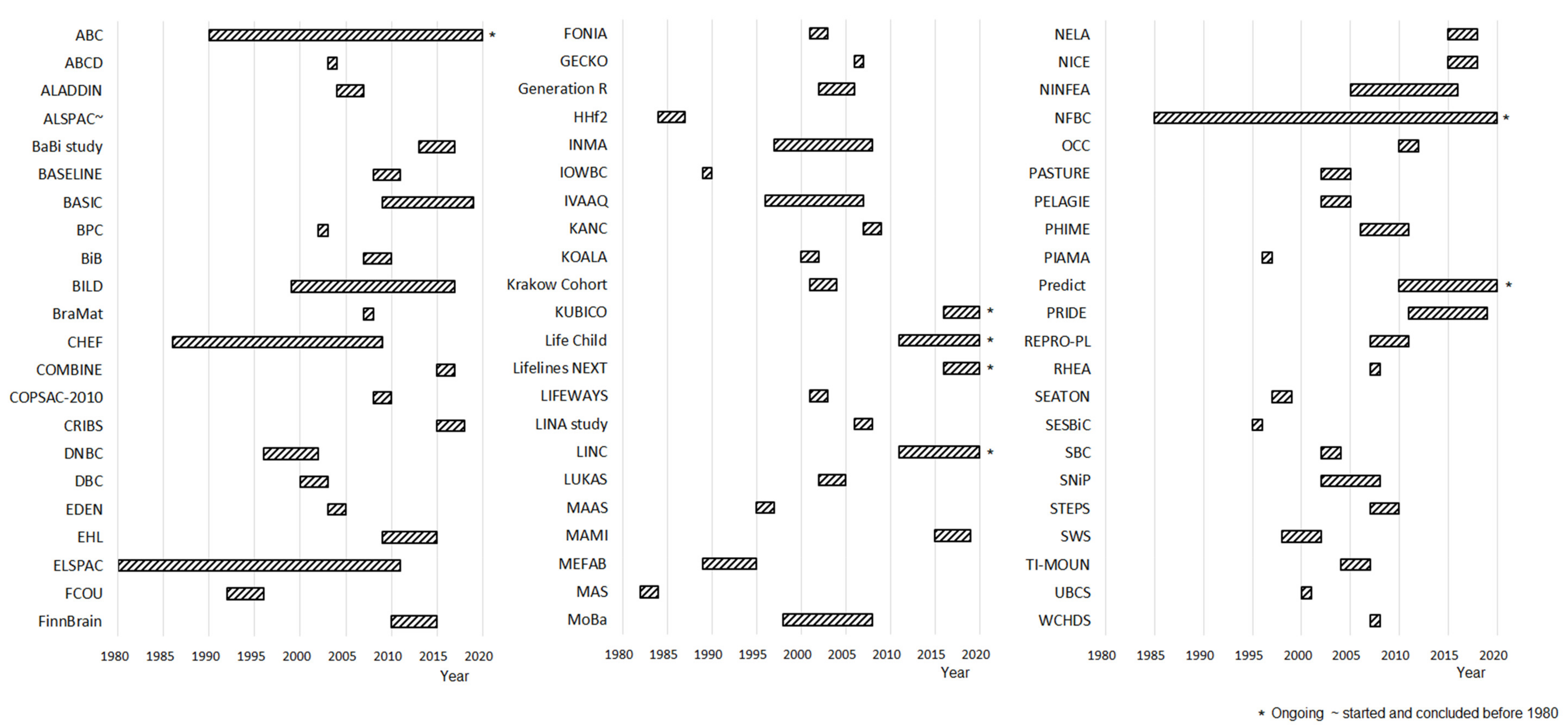
3.1. Characteristics of Included Cohorts
3.1.1. Collection of the Genetic Information
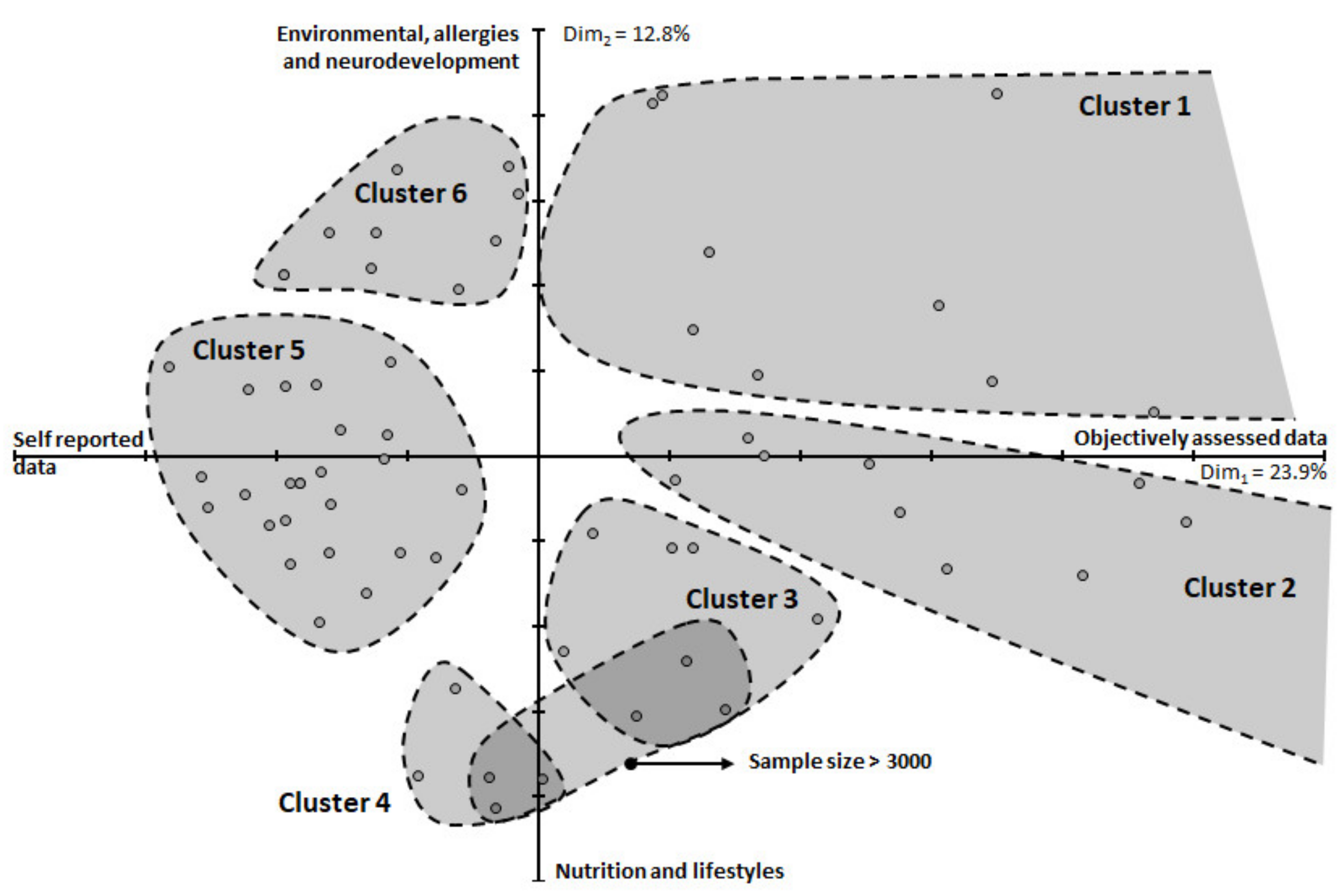
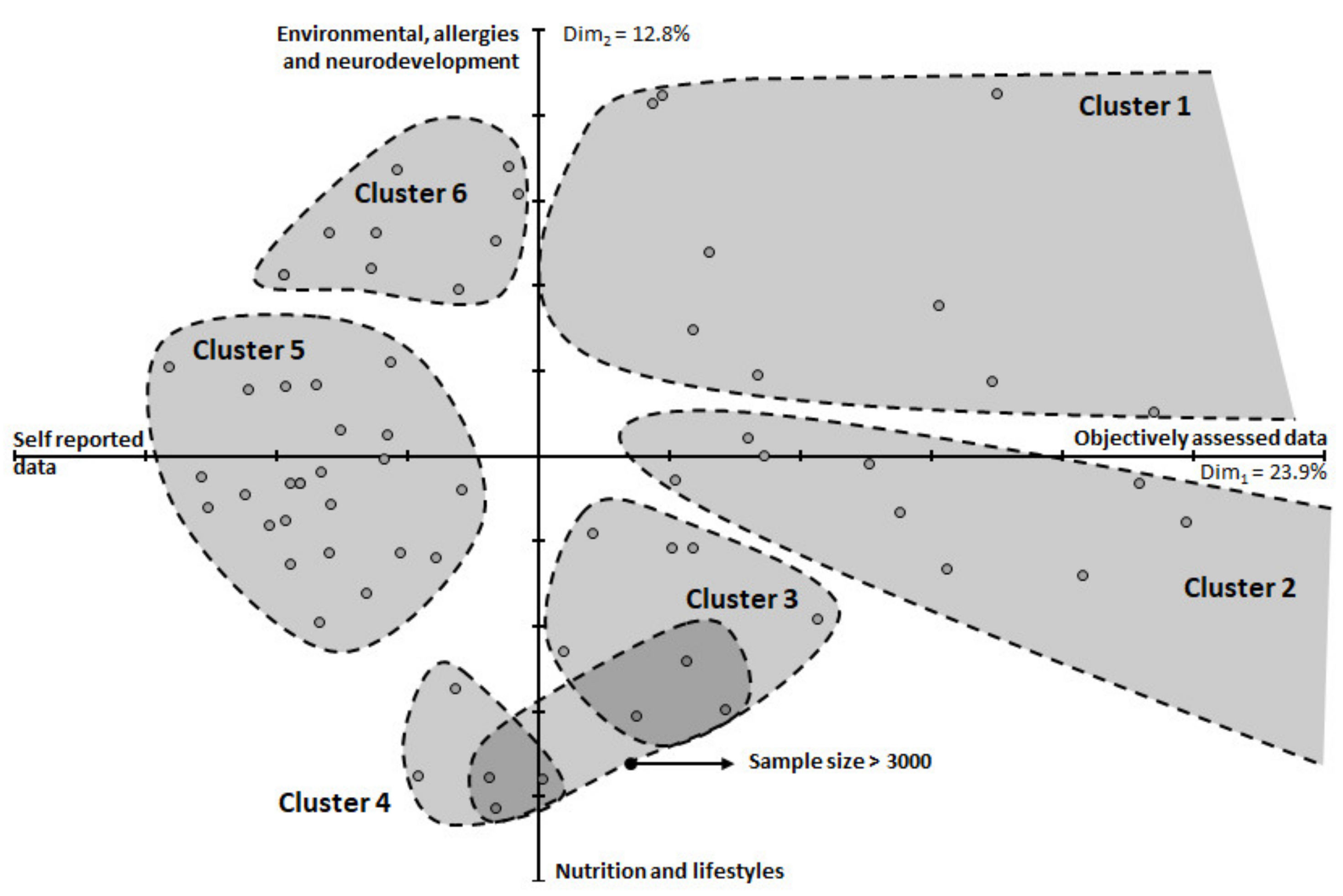
3.1.2. Correspondence Analysis Results and Multivariate Clustering of Cohorts
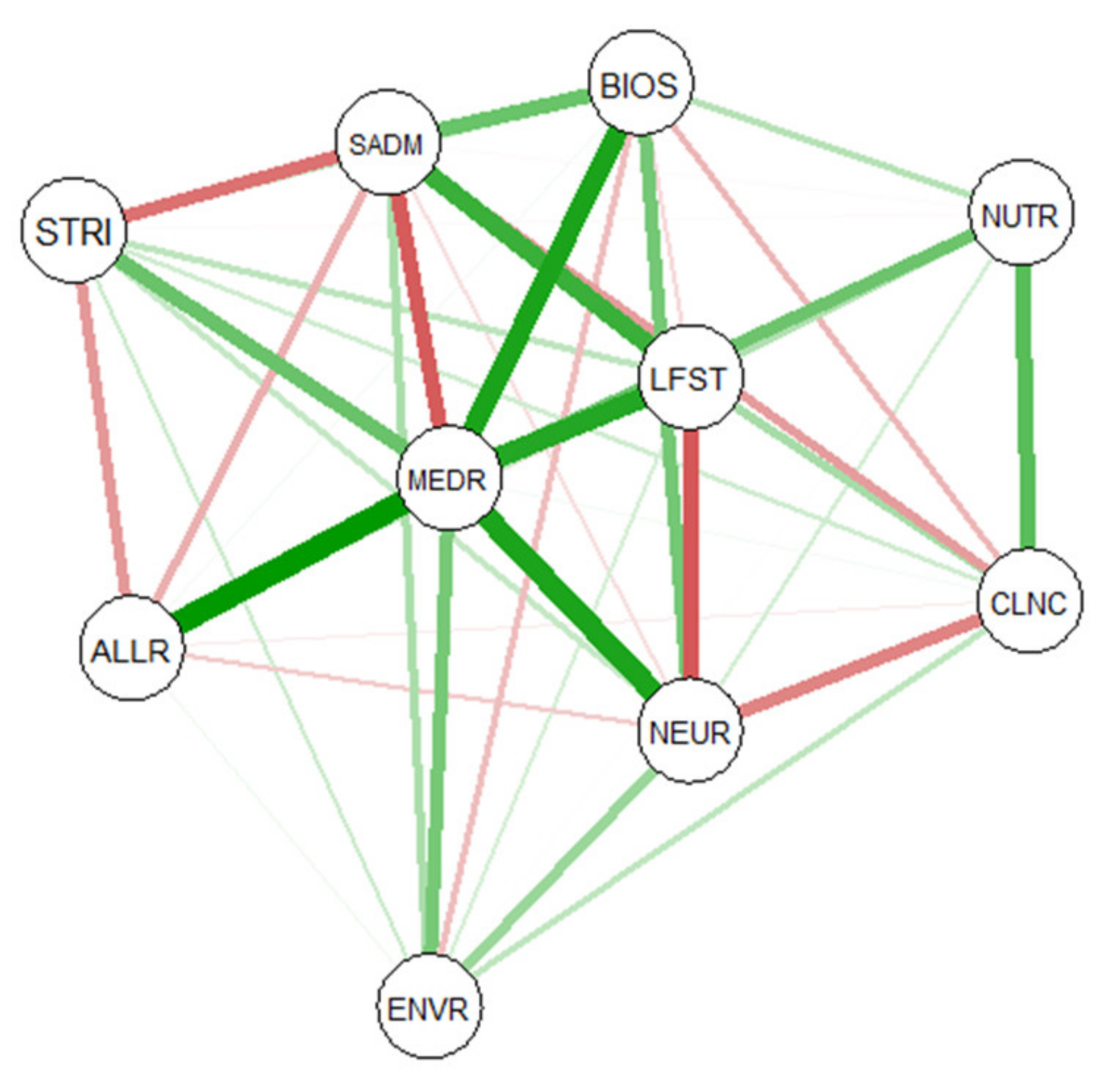
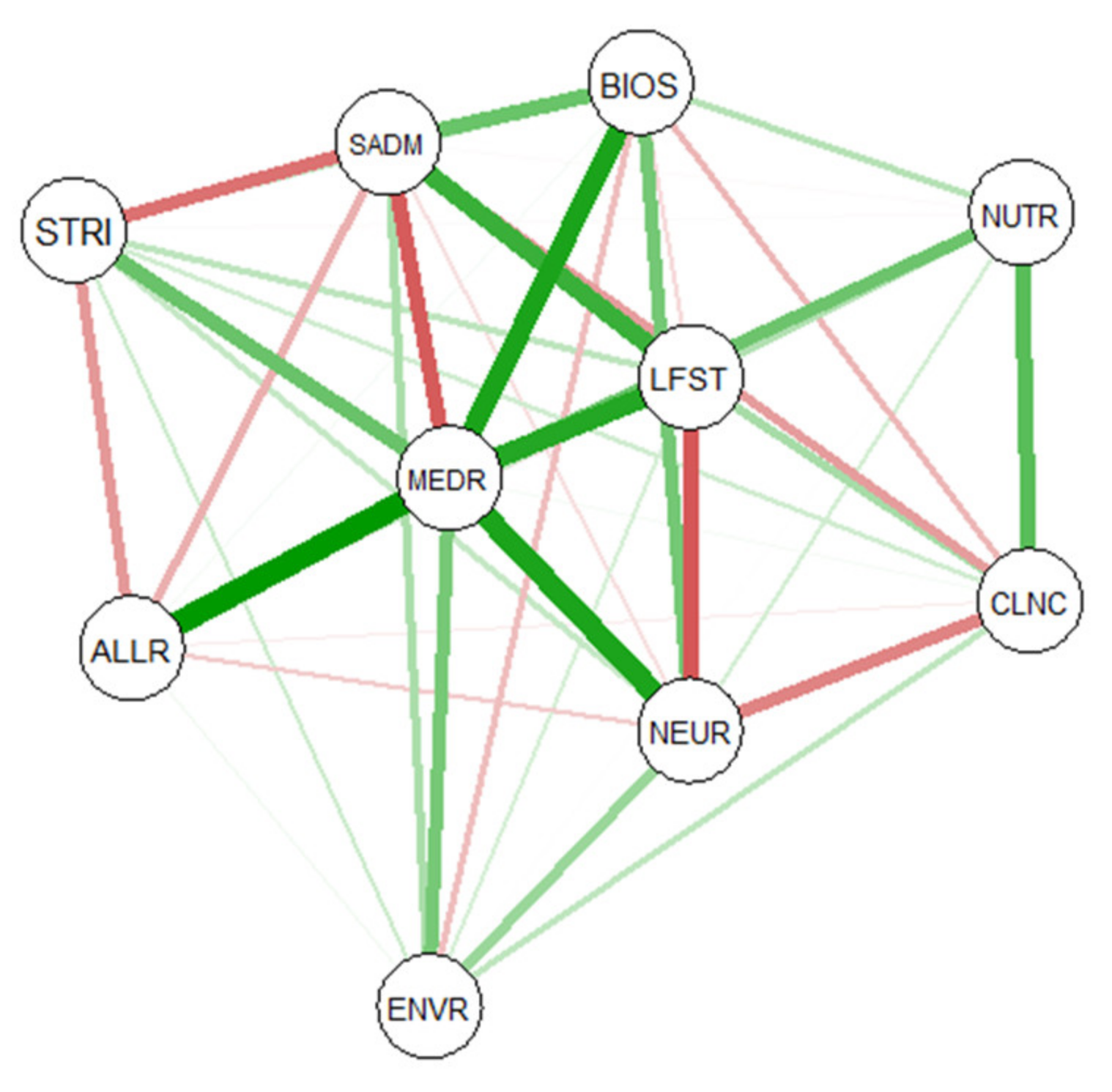
3.1.3. Network Analysis of Key Scientific Areas and Types of Data Collected
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Langie, S.A.S.; Lara, J.; Mathers, J.C. Early determinants of the ageing trajectory. Best Pract. Res. Clin. Endocrinol Metab. 2012, 26, 613–626. [Google Scholar] [CrossRef]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of Lifetime Health Around the Time of Conception: Causes and Consequences. Obstet. Gynecol. Surv. 2018, 73, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Fall, C.H.D.; Kumaran, K. Metabolic programming in early life in humans. Philos. Trans. R. Soc. B Biol. Sci. 2019, 374, 20180123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemette, L.; Wicklow, B.; Sellers, E.A.; Dart, A.; Shen, G.X.; Dolinsky, V.W.; Gordon, J.W.; Jassal, D.S.; Nickel, N.; Duhamel, T.A.; et al. Intrauterine exposure to diabetes and risk of cardiovascular disease in adolescence and early adulthood: A population-based birth cohort study. Can. Med. Assoc. J. 2020, 192, E1104–E1113. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xiao, X. The role of gut microbiota in the effects of maternal obesity during pregnancy on offspring metabolism. Biosci. Rep. 2018, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, C.; Bornemann, R.; Koenig, W.; Reister, F.; Walter, V.; Fantuzzi, G.; Weyermann, M.; Brenner, H.; Genuneit, J.; Rothenbacher, D. Gestational Weight Gain and Fetal-Maternal Adiponectin, Leptin, and CRP: Results of two birth cohorts studies. Sci. Rep. 2017, 7, srep41847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, L.; Chen, H.; Pan, Y.-X. Early-Life Nutritional Programming of Cognition-The Fundamental Role of Epigenetic Mechanisms in Mediating the Relation between Early-Life Environment and Learning and Memory Process. Adv. Nutr. 2017, 8, 337–350. [Google Scholar] [CrossRef]
- Lee, H.-S. Impact of Maternal Diet on the Epigenome during In Utero Life and the Developmental Programming of Diseases in Childhood and Adulthood. Nutrients 2015, 7, 9492–9507. [Google Scholar] [CrossRef] [Green Version]
- Kuh, D.; Wong, A.; Shah, I.; Moore, A.; Popham, M.; Curran, P.; Davis, D.; Sharma, N.; Richards, M.; Stafford, M.; et al. The MRC National Survey of Health and Development reaches age 70: Maintaining participation at older ages in a birth cohort study. Eur. J. Epidemiology 2016, 31, 1135–1147. [Google Scholar] [CrossRef] [Green Version]
- Bousquet, J.; Anto, J.; Sunyer, J.; Nieuwenhuijsen, M.; Vrijheid, M.; Keil, T.; MeDALL Study Group; CHICOS Study Group. Pooling birth cohorts in allergy and asthma: European Union-funded initiatives—A MeDALL, CHICOS, ENRIECO, and GA²LEN joint paper. Int. Arch. Allergy Immunol. 2013, 161, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lødrup Carlsen, K.C.; Roll, S.; Carlsen, K.H.; Mowinckel, P.; Wijga, A.H.; Brunekreef, B.; Torrent, M.; Roberts, G.; Arshad, S.H.; Kull, I.; et al. Does pet ownership in infancy lead to asthma or allergy at school age? Pooled analysis of individual participant data from 11 European birth cohorts. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [Green Version]
- Neuman, Å.; Hohmann, C.; Orsini, N.; Pershagen, G.; Eller, E.; Kjaer, H.F.; Gehring, U.; Granell, R.; Henderson, J.; Heinrich, J.; et al. Maternal smoking in pregnancy and asthma in preschool children: A pooled analysis of eight birth cohorts. Am. J. Respir. Crit. Care Med. 2012, 186, 1037–1043. [Google Scholar] [CrossRef] [Green Version]
- Al-Rifai, R.H.; Ali, N.; Barigye, E.T.; Al Haddad, A.H.I.; Al-Maskari, F.; Loney, T.; Ahmed, L.A. Maternal and birth cohort studies in the Gulf Cooperation Council countries: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Batty, G.; Alves, J.; Correia, J.; Lawlor, D. Examining life-course influences on chronic disease: The importance of birth cohort studies from low- and middle- income countries. An overview. Braz. J. Med. Biol. Res. 2007, 40, 1277–1286. [Google Scholar] [CrossRef] [Green Version]
- Vrijheid, M.; Casas, M.; Bergström, A.; Carmichael, A.; Cordier, S.; Eggesbø, M.; Eller, E.; Fantini, M.P.; Fernández, M.F.; Fernández-Somoano, A.; et al. European birth cohorts for environmental health research. Environ. Health Perspect. 2012, 120, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Larsen, P.S.; Kamper-Jørgensen, M.; Adamson, A.; Barros, H.; Bonde, J.P.; Brescianini, S.; Casas, M.; Devereux, G.; Eggesbø, M.; Fantini, M.P. Pregnancy and birth cohort resources in europe: A large opportunity for aetiological child health research. Paediatr Perinat Epidemiol. 2013, 27, 393–414. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Rudan, I. Systematic review of birth cohort studies in Africa. J. Glob. Heal. 2011, 1, 46–58. [Google Scholar]
- Grosser, A.; Razum, O.; Vrijkotte, T.G.M.; Hinz, I.-M.; Spallek, J. Inclusion of migrants and ethnic minorities in European birth cohort studies-a scoping review. Eur. J. Public Health. 2016, 26, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Pansieri, C.; Pandolfini, C.; Clavenna, A.; Choonara, I.; Bonati, M. An Inventory of European Birth Cohorts. Int. J. Environ. Res. Public Heal. 2020, 17, 3071. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.W.; Lyon, A.W.; Benzies, K.M.; McNeil, D.A.; Lye, S.J.; Dolan, S.M.; Pennell, C.E.; Bocking, A.D.; Tough, S.C. The All Our Babies pregnancy cohort: Design, methods, and participant characteristics. BMC Pregnancy Childbirth. 2013, 13 (Suppl. S1), S2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas-Guzik, L.; Ye, C.; Retnakaran, R. Association of Time with Reliability of Maternal Recall of Infant Birth Weight. JAMA Pediatr. 2020, 174, 1208–1210. [Google Scholar] [CrossRef]
- Bullens, D.M.A.; Seys, S.; Kasran, A.; Dilissen, E.; Dupont, L.J.; Ceuppens, J.L. Low cord blood Foxp3/CD3γ mRNA ratios: A marker of increased risk for allergy development. Clin. Exp. Allergy 2015, 45, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Street, M.E.; Bernasconi, S. Endocrine-Disrupting Chemicals in Human Fetal Growth. Int. J. Mol. Sci. 2020, 21, 1430. [Google Scholar] [CrossRef] [Green Version]
- Penkler, M.; Hanson, M.; Biesma, R.; Müller, R. DOHaD in science and society: Emergent opportunities and novel responsibilities. J. Dev. Orig Health Dis. 2019, 10, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Schei, K.; Avershina, E.; Øien, T.; Rudi, K.; Follestad, T.; Salamati, S.; Ødegård, R.A. Early gut mycobiota and mother-offspring transfer. Microbiome 2017, 5, 107. [Google Scholar] [CrossRef] [Green Version]
- Ideraabdullah, F.Y.; Belenchia, A.M.; Rosenfeld, C.S.; Kullman, S.W.; Knuth, M.; Mahapatra, D.; Bereman, M.; Levin, E.D.; Peterson, C.A. Maternal vitamin D deficiency and developmental origins of health and disease (DOHaD). J. Endocrinol. 2019, 241, R65–R80. [Google Scholar] [CrossRef] [Green Version]
- Bianco-Miotto, T.; Craig, J.M.; Gasser, Y.P.; van Dijk, S.J.; Ozanne, S.E. Epigenetics and DOHaD: From basics to birth and beyond. J. Dev. Orig Health Dis. 2017, 8, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Forestieri, S.; Pintus, R.; Marcialis, M.A.; Pintus, M.C.; Fanos, V. COVID-19 and developmental origins of health and disease. Early Hum. Dev. 2021, 155, 105322. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort/Acronym | Primary Aim |
|---|---|
| ABC | To investigate the role of genetic factors, environmental exposures and lifestyles in pregnancy on the risk of disease in the offspring |
| ABCD | To investigate children’s health at birth as well as in later life, and ethnic disparities therein |
| ALADDIN | Elucidate the role and timing of the anthroposophic lifestyle for the development of allergic disease in childhood |
| ALSPAC | To identify features of the environment, genotypes and the interaction between the two that influence the health, development and well-being of children throughout the life course |
| BaBi study | To disentangle the effects of individual and contextual factors among the offspring of migrants and non-migrant. To untangle the underlying reasons for health inequalities between different population groups |
| Baseline | To establish a prospective paediatrics birth cohort that will have access to detailed information on maternal health, fetal growth and childhood nutrition, growth and development in the first 2 years of life |
| BASIC | To enrich and expand our knowledge on the pathophysiological processes underlying perinatal depression (PPD) and also pinpoint both epidemiological and biological predictors of the disease, to improve early detection |
| BPC | The study was originally designed to identify early markers for subsequent pregnancy complications |
| BiB | To examine how genetic, nutritional, environmental, behavioural and social factors impact health and development during childhood, and subsequently adult life in a deprived multi-ethnic population |
| BILD | To study physiological properties of the respiratory system and environmental and genetic risk factors affecting lung development in healthy individuals as well as in preterm subjects from infancy through childhood in relation to wheeze |
| BraMat | To investigate the effect of prenatal exposure to PFAS on responses to pediatric vaccines and immune-related health outcomes in children up to 3 years of age |
| CHEF | Prenatal and postnatal exposure to methylmercury and organochlorines related to neurodevelopment |
| COMBINE | To examine associations of early nutrition, feeding behaviour and early life events with growth, lean and fat mass accrual as well as neurological development to better understand the factors that promote healthy growth and development |
| COPSAC-2010 | How human micro-biome and maternal nutrition during pregnancy interact with the genetic predisposition to cause an abnormal immune modulation in early life towards a trajectory to chronic inflammatory diseases such as asthma and others |
| CRIBS | To assess the prevalence of risk factors (biological, environmental and behavioural) for the Metabolic Syndrome (MetS) |
| DNBC | General, multiple aims to investigate the causal link between exposures in early life and disease later on and the possibilities for disease prevention |
| DBC | Investigate prenatal exposure to PCDD/Fs and dioxin-like PCBs in association with thyroid hormone status |
| EDEN | To study the pre and postnatal determinants of the child’s development and health |
| EHL | To investigate the impact of gestational and postnatal environmental risk factors on infant health and development across the life course |
| ELSPAC | To determine which biological, psychological, social, economic and environmental factors have an impact on pregnancy, birth, adaptation after birth, child development, health of children and adolescents |
| FCOU | To study the biological, psychological and social factors, as well as factors of the external environment, which are associated with survival and health of the fetus, infant and child |
| FinnBrain | To study prospectively the effects of early life stress, also comprising prenatal stress, on child brain development and health |
| FONIA | Association between allergen-induced IL-10 production by cord blood cells and prospective risk of allergy development |
| GECKO | To study the prevalence and early risk factors for the development of childhood overweight and fat distribution at a very young age |
| Generation R | To identify early environmental and genetic causes of normal and abnormal growth, development and health during fetal life, childhood and adulthood |
| HHf2 | To investigate smoking, drinking and eating behaviour in association with child health |
| INMA | To describe the degree of individual prenatal exposure to environmental pollutants and the internal dose of these chemicals during pregnancy, at birth and during childhood |
| IOWBC | To investigate the prevalence, natural history and risk and protective factors for the development of asthma and allergic diseases |
| IVAAQ | To collect information about pregnant women and their newborn children to study the effects of selected exposures on pregnancy outcome and child development |
| KANC | To assess the distribution of risk factors for adverse pregnancy outcomes in pregnant women with detailed information on demographic and lifestyle characteristics, medical history, and genetic to define susceptibility to long-term environmental exposure |
| KOALA | Allergy and asthma development |
| Krakow Cohort | To test the hypothesis that prenatal exposure to airborne polycyclic aromatic hydrocarbons adversely affects fetal growth, after controlling for non-PAH components of particulate matter <2.5 µm (PM2.5), environmental tobacco smoke, nutritional status |
| KUBICO | To investigate genetics and stress factors during pregnancy in association with the health status of the mother and child |
| Life Child | To investigate determinants of healthy child development from pregnancy to adulthood |
| Lifelines NEXT | To investigate the effects of early life or pre-conceptional transgenerational events on health in early childhood |
| LIFEWAYS | To record the physical and psychological health status and socio-economic circumstances of individuals at birth, during early childhood, early adulthood and early middle age |
| LINA study | To investigate prenatal lifestyle and environmental factors in association with newborn allergy |
| LINC | To study associations between early-life environmental exposures and child health, including growth and neurodevelopment |
| LUKAS | Environmental exposure: microbes from stables and from moisture damaged homes, asthma, sIgEs, atopic eczema, hayfever, respiratory symptoms, development of the immune system |
| MAAS | To investigate the risk factors for the development of asthma and other atopic disorders |
| MAMI | To characterize the microbial community, diversity and activity in mother-infant interphase by use of both, culture-dependent microbiological techniques and culture-independent methodologies based on PCR, from stool, oral and breastmilk samples collected during the first two years of infant life |
| MEFAB | To investigate whether prenatal availability of long-chain polyunsaturated fatty acids (LCPUFAs) may be involved in programming birth outcomes and later development |
| MAS | To study prospectively the development of allergy in relation to infant feeding and various environmental factors |
| MoBa | To find causes of diseases |
| NELA | To investigate the impact of nutrition during pregnancy and early postnatal life on health outcomes in children |
| NICE | To evaluate how multiple environmental exposures such as lifestyle, diet, microbes and toxicants influence the maturation of the immune system and affect allergy development |
| NINFEA | To investigate the effects of exposures acting during pre-natal and early post-natal life on infant, child and adult health |
| NFBC | To investigate factors in association with pre-term birth and intrauterine growth retardation. Investigate the consequences of these early adverse outcomes on subsequent morbidity |
| OCC | To assess environmental factors in pregnancy and early childhood and their impact on child health |
| PASTURE | To identify mechanisms of early protective exposures on allergy development using birth cohort studies with comprehensive measures of the developing immune response |
| PELAGIE | To investigate long-term consequences of prenatal and early childhood exposure to the endocrine-disrupting chemicals |
| PHIME | To describe the degree of individual prenatal exposure to environmental pollutants and the internal dose of these chemicals during pregnancy, at birth and during childhood |
| PIAMA | To investigate the effect of mite-allergen avoidance on the incidence of childhood asthma and to assess lifestyle and environmental risk factors for childhood asthma. |
| Predict Study | To investigate failures and adverse pregnancy outcomes and health of the offspring up to 1 year of age |
| PRIDE Study | To identify factors to which women may be exposed during pregnancy that potentially affect the health of the future mother or her unborn child at any point in life. To evaluate specific aspects of preconceptional, prenatal and perinatal care |
| REPRO_PL | To evaluate the impact of exposure to different environmental factors during pregnancy and after birth on pregnancy outcome and children’s health |
| RHEA | To characterize nutritional, environmental and psychosocial determinants of children’s growth and development, to examine: (i) growth and physical development; (ii) behavioural, cognitive and sociο-emotional development; (iii) allergies |
| SEATON | To study maternal dietary antioxidant intake and atopic disease during childhood |
| SESBiC | To assess whether mothers who reported symptoms of PPD were more likely than others to report depressive symptoms 12 years later |
| SBC | To evaluate and quantify how various modifiable environmental and dietary exposures contribute to the development of infantile atopic eczema |
| SNiP | To investigate biological features from mothers in association to neonatal health, morbidity and mortality and child health prior to attendance at primary school |
| STEPS | To contribute to a comprehensive, integrated view of healthy development: to improve the understanding of the early development of children, and their health and well-being beginning from the prenatal period up to school age, and also to determine the long-term effects of their early development later on in life |
| SWS | Maternal pre-conceptional and pregnancy factors: diet, physical activity, body composition, hormonal levels, genetics, epigenetics. Childhood growth, respiratory health, body composition, cardiovascular health |
| TI-MOUN | To investigate perinatal exposure to chlordecone in association with thyroid hormone status and neurodevelopment in infants |
| UBCS | Investigate lifestyle factors of mother in association to child health |
| WCHDS | To identify the very early risks and processes in the development of behavioural and emotional problems in childhood |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandolfini, C.; Ricci, C.; Siziba, L.P.; Huhn, S.; Genuneit, J.; Bonati, M. Intrauterine Exposures and Maternal Health Status during Pregnancy in Relation to Later Child Health: A Review of Pregnancy Cohort Studies in Europe. Int. J. Environ. Res. Public Health 2021, 18, 7702. https://doi.org/10.3390/ijerph18147702
Pandolfini C, Ricci C, Siziba LP, Huhn S, Genuneit J, Bonati M. Intrauterine Exposures and Maternal Health Status during Pregnancy in Relation to Later Child Health: A Review of Pregnancy Cohort Studies in Europe. International Journal of Environmental Research and Public Health. 2021; 18(14):7702. https://doi.org/10.3390/ijerph18147702
Chicago/Turabian StylePandolfini, Chiara, Cristian Ricci, Linda Precious Siziba, Sebastian Huhn, Jon Genuneit, and Maurizio Bonati. 2021. "Intrauterine Exposures and Maternal Health Status during Pregnancy in Relation to Later Child Health: A Review of Pregnancy Cohort Studies in Europe" International Journal of Environmental Research and Public Health 18, no. 14: 7702. https://doi.org/10.3390/ijerph18147702
APA StylePandolfini, C., Ricci, C., Siziba, L. P., Huhn, S., Genuneit, J., & Bonati, M. (2021). Intrauterine Exposures and Maternal Health Status during Pregnancy in Relation to Later Child Health: A Review of Pregnancy Cohort Studies in Europe. International Journal of Environmental Research and Public Health, 18(14), 7702. https://doi.org/10.3390/ijerph18147702