
Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea



Abstract
1. Introduction
2. Materials and Methods
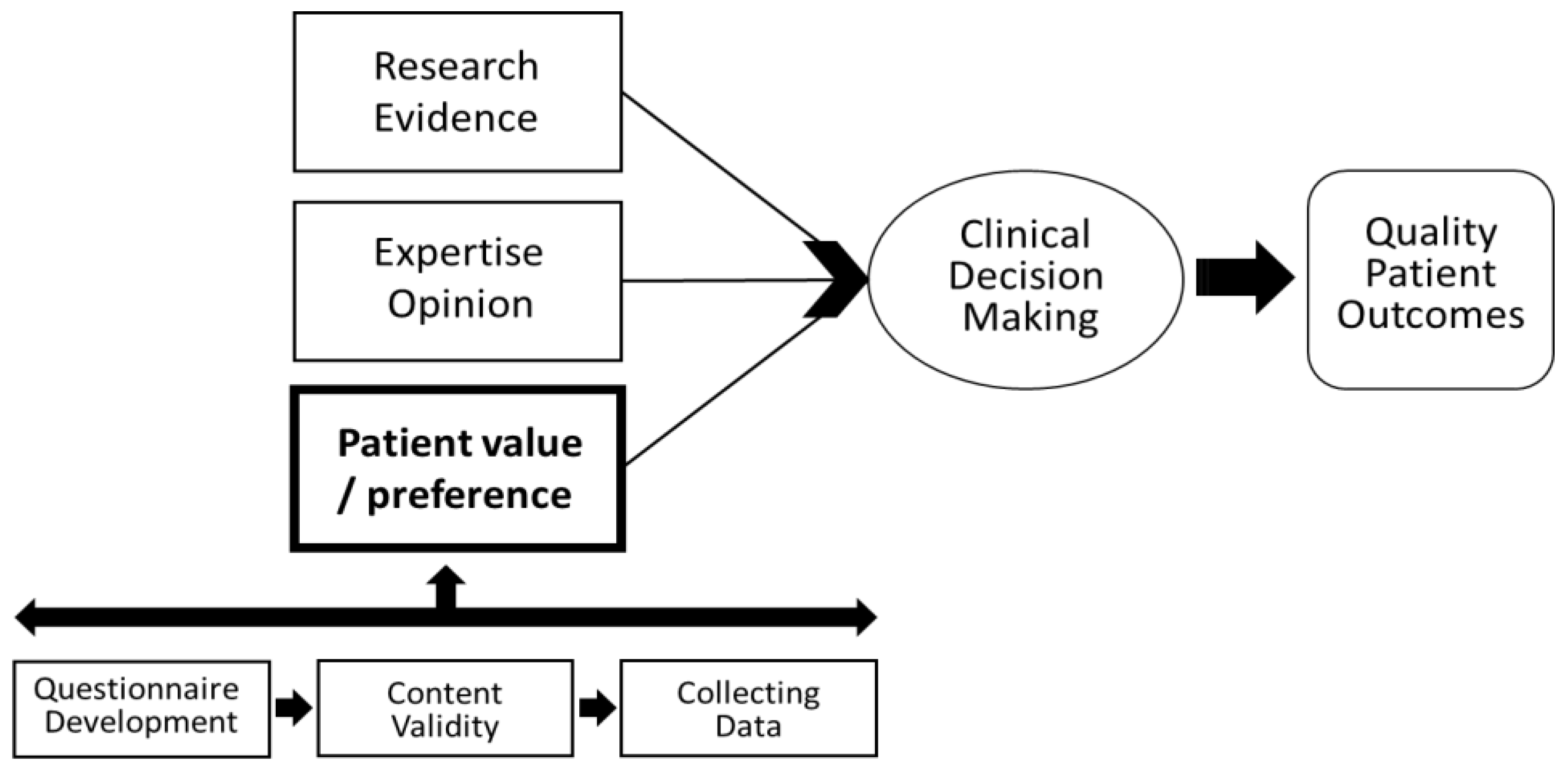
2.1. Research Framework
2.2. Participants
2.3. Preliminary Evaluation Questionnaire Development
2.4. Quantification of Content Validity
2.5. Collecting Data
2.6. Statistical Analysis
3. Results
3.1. Patients’ Awareness and Needs for Home-Based Rehabilitation Programs: The Survey
3.2. Patients’ Awareness and Needs of Home-Based Rehabilitation Programs
3.2.1. Experience of Hearing about Home-Based Rehabilitation Services
3.2.2. Whether Home-Based Rehabilitation Services Are Needed
3.2.3. Whether to Participate in Home-Based Rehabilitation Services
3.2.4. Preferred Number of Home-Based Rehabilitation Treatment Visits, Duration and Cost
3.3. The Importance of the Components of Home-Based Rehabilitation Programs
4. Discussion
4.1. Awareness and Needs of Home-Based Rehabilitation Services
4.2. Preference to Participate in Home-Based Rehabilitation Services
4.3. The Importance of the Components of Home-Based Rehabilitation Programs
4.4. Advantages of Home-Based Rehabilitation Program for Elderly Patients with Hip Fracture Surgery
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Negrete-Corona, J.; Alvarado-Soriano, J.; Reyes-Santiago, L.J.A. Hip fracture as risk factor for mortality in patients over 65 years of age. Case-Control study. Acta Ortop. Mex. 2014, 28, 352–362. [Google Scholar]
- Rapp, K.; Büchele, G.; Dreinhöfer, K.; Bücking, B.; Becker, C.; Benzinger, P.J.Z. Epidemiology of hip fractures. Z. Gerontol. Geriatr. 2019, 52, 10–16. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Ang, S.B.; Chadha, M.; Chow, E.S.-L.; Chung, Y.-S.; Hew, F.L.; Jaisamrarn, U.; Ng, H.; Takeuchi, Y.; Wu, C.-H.; et al. An updated hip fracture projection in Asia: The Asian Federation of Osteoporosis Societies study. Osteoporos. Sarcopenia 2018, 4, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-S.; Lim, J.-Y.; Ha, Y.-C. Recent Epidemiology of Hip Fractures in South Korea. Hip Pelvis 2020, 32, 119–124. [Google Scholar] [CrossRef]
- Hong, S.; Han, K. The incidence of hip fracture and mortality rate after hip fracture in Korea: A nationwide population-based cohort study. Osteoporos. Sarcopenia 2019, 5, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y. An Outlook for Social Changes in an Aged Korea: Implications from the Japanese Case. Health Welf. Policy Forum 2017, 254, 9–17. [Google Scholar]
- Ha, Y.-C.; Kim, T.-Y.; Lee, A.; Lee, Y.-K.; Kim, H.-Y.; Kim, J.-H.; Park, C.-M.; Jang, S. Current trends and future projections of hip fracture in South Korea using nationwide claims data. Osteoporos. Int. 2016, 27, 2603–2609. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Downey, C.; Kelly, M.; Quinlan, J.F. Changing trends in the mortality rate at 1-year post hip fracture-A systematic review. World J. Orthop. 2019, 10, 166–175. [Google Scholar] [CrossRef]
- Salpakoski, A.; Törmäkangas, T.; Edgren, J.; Kallinen, M.; Sihvonen, S.E.; Pesola, M.; Vanhatalo, J.; Arkela, M.; Rantanen, T.; Sipilä, S. Effects of a multicomponent home-based physical rehabilitation program on mobility recovery after hip fracture: A randomized controlled trial. J. Am. Med Dir. Assoc. 2014, 15, 361–368. [Google Scholar] [CrossRef]
- Grimmer, M.; Riener, R.; Walsh, C.J.; Seyfarth, A. Rehabilitation, Mobility related physical and functional losses due to aging and disease-a motivation for lower limb exoskeletons. J. Neuroeng. Rehabil. 2019, 16, 2. [Google Scholar] [CrossRef]
- Okamoto, T.; Ridley, R.J.; Edmondston, S.J.; Visser, M.; Headford, J.; Yates, P. Day-of-surgery mobilization reduces the length of stay after elective hip arthroplasty. J. Arthroplast. 2016, 31, 2227–2230. [Google Scholar] [CrossRef]
- Karlsson, Å.; Lindelöf, N.; Olofsson, B.; Berggren, M.; Gustafson, Y.; Nordström, P.; Stenvall, M. Rehabilitation, Effects of geriatric interdisciplinary home rehabilitation on independence in activities of daily living in older people with hip fracture: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2020, 101, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, R., Jr.; Souza, P.P.; dos Reis, K.K.M.; Filoni, E. Home-based physiotherapy programmes for individuals with neurological diseases: Systematic review. Fisioter. Mov. 2019, 32, 32. [Google Scholar] [CrossRef]
- Buhagiar, M.A.; Naylor, J.M.; Harris, I.A.; Xuan, W.; Adie, S.; Lewin, A. Assessment of outcomes of inpatient or clinic-based vs home-based rehabilitation after total knee arthroplasty: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e192810. [Google Scholar] [CrossRef] [PubMed]
- Gelaw, A.Y.; Janakiraman, B.; Gebremeskel, B.F.; Ravichandran, H. Effectiveness of Home-based rehabilitation in improving physical function of persons with Stroke and other physical disability: A systematic review of randomized controlled trials. J. Stroke Cerebrovasc. Dis. 2020, 29, 104800. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Zhu, X.; Zhang, S. Effect of home-based rehabilitation for hip fracture: A meta-analysis of randomized controlled trials. J. Rehabil. Med. 2018, 50, 481–486. [Google Scholar] [CrossRef]
- Chen, J.; Zhu, X.; Jiang, J.; Qi, Y.; Shi, Y. Needs of Chinese patients undergoing home-based rehabilitation after hip replacement: A qualitative study. PLoS ONE 2019, 14, e0220304. [Google Scholar] [CrossRef]
- Choi, K.J. Research of Demand For the Community-Based Home Visit Physical Therapy; The Graduate School of Medical Science Catholic University of Daegu: Seoul, Korea, 2015. [Google Scholar]
- Kim, B. The Survey of Necessity on Home Visiting Physical Therapy Based on International Classification of Function, Disability and Healt. J. Humanit. Soc. Sci. 2018, 9, 911–922. [Google Scholar]
- Melnyk, B.M.; Gallagher-Ford, L.; Long, L.E.; Fineout-Overholt, E. The Establishment of Evidence-Based Practice Competencies for Practicing Registered Nurses and Advanced Practice Nurses in Real-World Clinical Settings: Proficiencies to Improve Healthcare Quality, Reliability, Patient Outcomes, and Costs. Worldviews Evid. Based Nurs. 2014, 11, 5–15. [Google Scholar] [CrossRef]
- Yu, W. A Study on the Job Analysis of the Home Visiting Physical Therapist; Eulji University: Daejeon, Korea, 2014. [Google Scholar]
- Davis, L.L. Instrument review: Getting the most from a panel of experts. Appl. Nurs. Res. 1992, 5, 194–197. [Google Scholar] [CrossRef]
- Choi, S.-Y.; Yoon, J.-W. Awareness and demand for pediatric home-based physical therapy in Korea. Phys. Ther. Korea 2013, 20, 62–73. [Google Scholar] [CrossRef]
- Kim, J.-H.; Lee, K.-J. Study on the awareness and the necessity of home and visiting physical therapy. J. Korean Soc. Phys. Med. 2014, 9, 465–474. [Google Scholar] [CrossRef][Green Version]
- Boutin-Lester, P.; Gibson, R.W. Patients’ perceptions of home health occupational therapy. Aust. Occup. Ther. J. 2002, 49, 146–154. [Google Scholar] [CrossRef]
- Magaziner, J.; Mangione, K.K.; Orwig, D.; Baumgarten, M.; Magder, L.; Terrin, M.; Fortinsky, R.H.; Gruber-Baldini, A.L.; Beamer, B.A.; Tosteson, A.N.A.; et al. Effect of a Multicomponent Home-Based Physical Therapy Intervention on Ambulation after Hip Fracture in Older Adults: The CAP Randomized Clinical Trial. JAMA 2019, 322, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Yu, S. Effectiveness of multifactorial interventions in preventing falls among older adults in the community: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2020, 106, 103564. [Google Scholar] [CrossRef]
- Sackett, D.L.; Straus, S.E.; Richardson, W.S. Evidence-Based Medicine: How to Practice and Teach EBM; Churchill Livingstone: London, UK, 2000. [Google Scholar]
- Berggren, M.; Karlsson, Å.; Lindelöf, N.; Englund, U.; Olofsson, B.; Nordström, P.; Gustafson, Y.; Stenvall, M. Effects of geriatric interdisciplinary home rehabilitation on complications and readmissions after hip fracture: A randomized controlled trial. Clin. Rehabil. 2019, 33, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Shyu, Y.-I.L.; Liang, J.; Tseng, M.-Y.; Li, H.-J.; Wu, C.-C.; Cheng, H.-S.; Chou, S.-W.; Chen, C.-Y.; Yang, C.-T. Enhanced interdisciplinary care improves self-care ability and decreases emergency department visits for older Taiwanese patients over 2 years after hip-fracture surgery: A randomised controlled trial. Int. J. Nurs. Stud. 2016, 56, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Room, J.; Hannink, E.; Dawes, H.; Barker, K. What interventions are used to improve exercise adherence in older people and what behavioural techniques are they based on? A systematic review. BMJ Open 2017, 7, e019221. [Google Scholar] [CrossRef]
- Riemen, A.H.; Hutchison, J.D. The multidisciplinary management of hip fractures in older patients. Orthop. Trauma 2016, 30, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.Y.-H.; Packer, T.; Yau, M. Rehabilitation, When East meets Wests: Community-based rehabilitation in Chinese communities. Disabil. Rehabil. 2011, 33, 697–705. [Google Scholar] [CrossRef]
- Karlsson, Å.; Berggren, M.; Gustafson, Y.; Olofsson, B.; Lindelöf, N.; Stenvall, M. Effects of geriatric interdisciplinary home rehabilitation on walking ability and length of hospital stay after hip fracture: A randomized controlled trial. J. Am. Med Dir. Assoc. 2016, 17, 464.e9–464.e15. [Google Scholar] [CrossRef] [PubMed]
- Crotty, M.; Whitehead, C.H.; Gray, S.; Finucane, P. Early discharge and home rehabilitation after hip fracture achieves functional improvements: A randomized controlled trial. Clin. Rehabil. 2002, 16, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Bae, S. A Strategy of the Home Visiting Physical Therapy. J. Korean Soc. Phys. Ther. 2003, 15, 180–189. [Google Scholar]


{kind=link}
| Characteristics | |
|---|---|
| Age (year), mean ± SD | Total |
| 65–69 years, n (%) | 73.1 ± 8.7 |
| 70–79 years | 35 (39.3) |
| 80–89 years | 32 (36.0) |
| 90 years or older | 19 (21.3) |
| Gender (women), n (%) | 3 (3.4) |
| Education, n (%) | 63 (64.3) |
| No education or elementary school | |
| Middle school | 39 (39.8) |
| High school | 16 (16.3) |
| Undergraduate or graduate school | 32 (32.6) |
| Living status, n (%) | 11 (11.2) |
| Alone | |
| With partner | 23 (23.5) |
| With partner and son or daughter | 34 (34.7) |
| With siblings | 12(12.2) |
| Nursing home | 16 (16.3) |
| Economic status, n (%) | 13 (13.3) |
| Low | |
| Middle | 44 (44.9) |
| High | 25 (25.5) |
| Caregiver | 29 (29.6) |
| Partner | |
| Son or daughter | 31 (31.6) |
| Cousin | 14 (14.3) |
| Professional caregiver | 1 (1.0) |
| Days after hip surgery (days), median (IQR) | 52 (56.0) |
| Walking independently before fracture, n (%) | 30 (7–72) |
| Items | n (%) |
|---|---|
| Have you heard of home-based rehabilitation? | |
| Yes | 26 (26.5) |
| No | 72 (73.5) |
| Necessity of home-based rehabilitation | |
| Strongly agree and agree | 74 (75.6) |
| Strongly disagree and disagree | 12 (12.2) |
| Neither agree nor disagree | 12(12.3) |
| Will you participate in home-based rehabilitation? | |
| Yes | 83 (84.7) |
| No | 13 (13.3) |
| The reasons for participating in home-based rehabilitation | |
| Mentally comfortable | 13 (15.7) |
| A lighter burden in terms of time | 3 (3.6) |
| Ongoing treatment even after discharge | 44 (53.0) |
| Less of a burden in the hospital | 23 (27.7) |
| The reason for not participating in home-based rehabilitation | |
| Prefer continued hospitalization or outpatient rehabilitation | 8 (61.5) |
| Lack of reliability of intervention tools or visiting therapist | 4 (30.8) |
| More medical expenses | 1 (7.7) |
| Items | n (%) |
|---|---|
| Number of visits | |
| Once a week | 12 (12.2) |
| Twice a week | 23 (23.5) |
| Three times a week | 40 (40.8) |
| Four times a week | 6 (6.1) |
| Five times a week | 17 (17.3) |
| Duration of one visit | |
| 30 min | 22 (22.4) |
| 45 min | 15 (15.3) |
| 60 min | 51 (52.1) |
| 90 min | 6 (6.1) |
| 120 min | 4 (4.1) |
| Medical cost of one visit | |
| Below KRW 5000 (USD 4.4) | 26 (26.5) |
| Current level (8170 (USD 7.3) home visiting nursing service) | 45 (45.9) |
| KRW 10,000 (USD 8.9) | 19 (19.4) |
| KRW 15,000 (USD 13.3) | 4 (4.1) |
| over 20,000 (USD 17.7) | 4 (4.1) |
| Duty | Task | Importance |
|---|---|---|
| Therapeutic exercises | Strengthening exercises | 4.19 |
| Endurance exercises | 3.86 | |
| Range of Motion exercises | 4.28 | |
| Breathing exercise | 3.31 | |
| Balance exercise | 4.14 | |
| Ambulation exercise | 4.33 | |
| Activities of daily living training | 3.94 | |
| Education | Positioning education | 4.15 |
| Fall prevention | 4.06 | |
| Training in the use of assistive devices | 3.86 | |
| Ability to handle medication | 3.38 | |
| Caregiver education | 3.69 | |
| Pressure ulcer | Pressure ulcer management | 3.37 |
| Nutrition | Provided nutrition advice | 3.45 |
| Vitamin supply counselling | 3.39 | |
| Environmental | Modifications of the home environment | 3.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Lee, S.-H. Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 7632. https://doi.org/10.3390/ijerph18147632
Lee H, Lee S-H. Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(14):7632. https://doi.org/10.3390/ijerph18147632
Chicago/Turabian StyleLee, Haneul, and Seon-Heui Lee. 2021. "Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea" International Journal of Environmental Research and Public Health 18, no. 14: 7632. https://doi.org/10.3390/ijerph18147632
APA StyleLee, H., & Lee, S.-H. (2021). Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea. International Journal of Environmental Research and Public Health, 18(14), 7632. https://doi.org/10.3390/ijerph18147632