
Ethical Problems and Moral Distress in Primary Care: A Scoping Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Step 1: Identify the Research Question
- What ethical dilemmas are experienced by nurses in primary care settings?
- Do nurses experience moral distress in primary care settings?
- How do nurses manage moral distress in primary care settings?
- What are the implications and suggestions for further research?
2.3. Step 2: Identifying Relevant Studies
2.4. Step 3: Selecting Relevant Studies
2.5. Step 4: Extracting Collected Data
2.6. Step 5: Reporting Results
3. Results
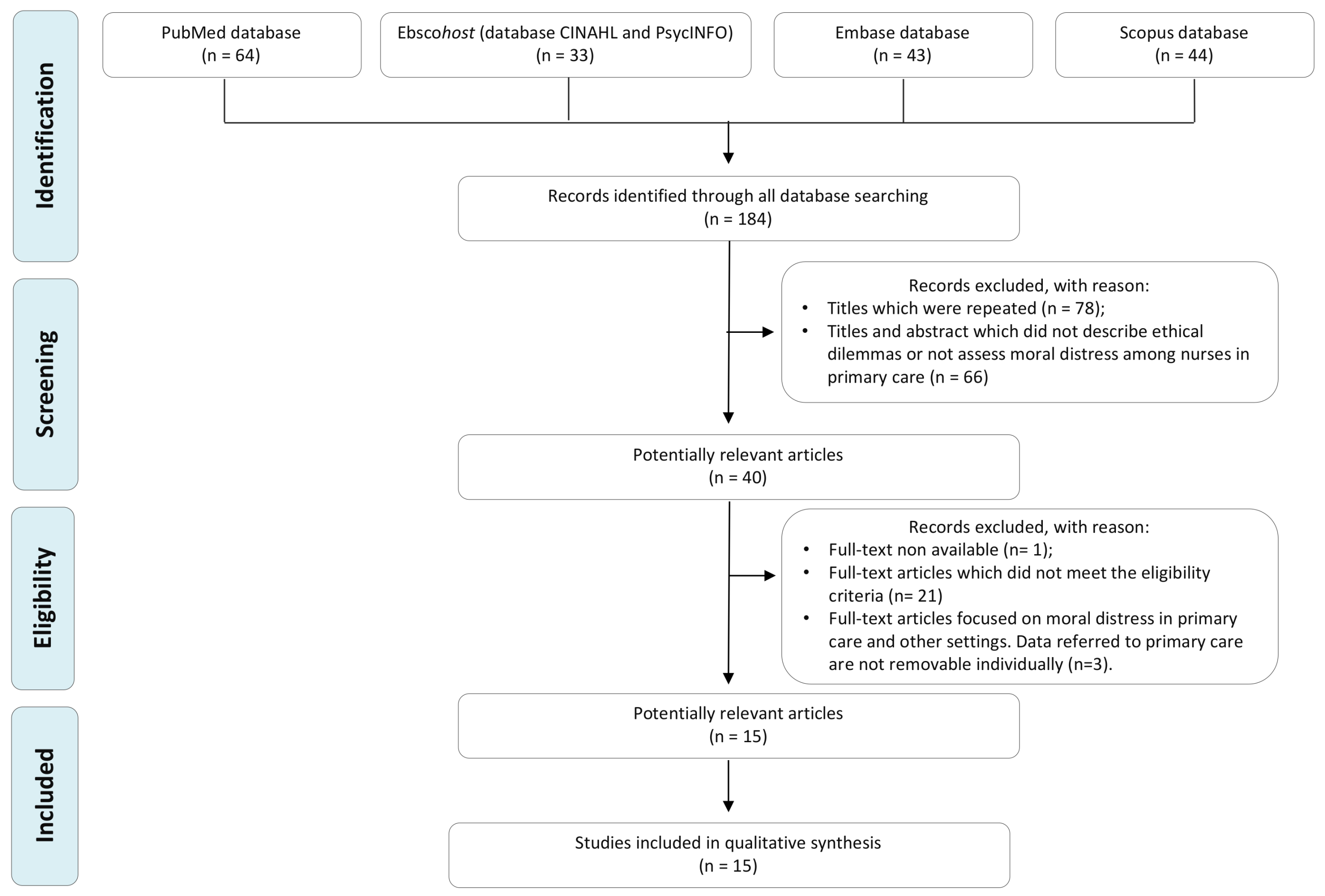
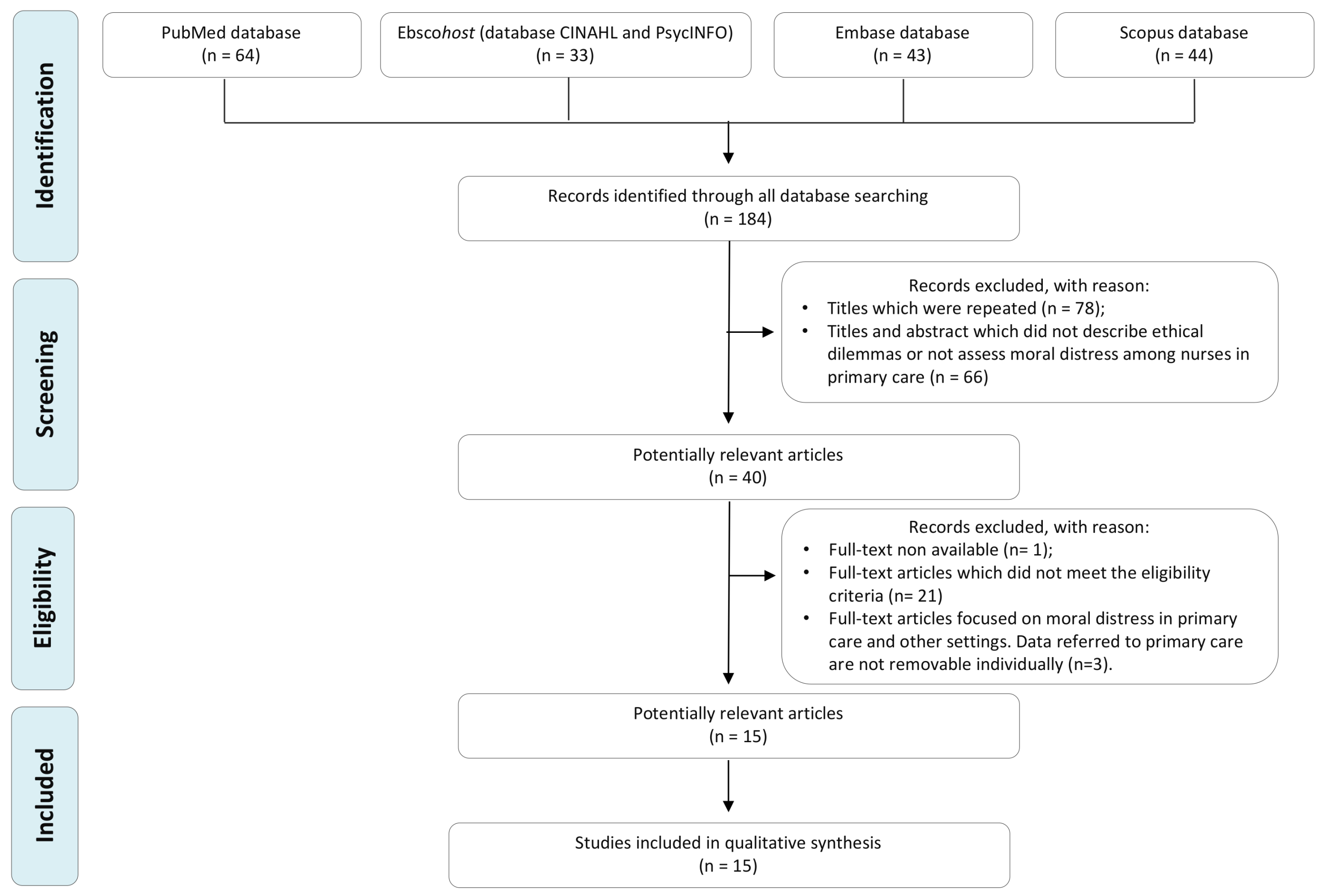
3.1. Study Selection
3.2. Characteristics of the Studies Included
3.3. Focus Areas
3.3.1. Ethical Conflicts and Moral Distress
3.3.2. Moral Distress Measures in Primary Care Settings
3.3.3. Moral Distress Management in Primary Care Settings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Vošner, H.B.; Železnik, D.; Kokol, P.; Vošner, J.; Završnik, J. Trends in nursing ethics research: Mapping the literature production. Nurs. Ethics 2016, 24, 892–907. [Google Scholar] [CrossRef] [PubMed]
- Norlyk, A.; Haahr, A.; Dreyer, P.; Martinsen, B. Lost in transformation? Reviving ethics of care in hospital cultures of evi-dence-based healthcare. Nurs. Inq. 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Haahr, A.; Norlyk, A.; Martinsen, B.; Dreyer, P. Nurses experiences of ethical dilemmas: A review. Nurs. Ethics 2019, 27, 258–272. [Google Scholar] [CrossRef]
- Goethals, S.; De Casterlé, B.D.; Gastmans, C. Nurses’ ethical reasoning in cases of physical restraint in acute elderly care: A qualitative study. Med. Health Care Philos. 2012, 16, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 5th ed.; Oxford University Press: Oxford, UK, 2001; p. 454. [Google Scholar]
- Jameton, A. Nursing practice, the ethical issues. Int. J. Nurs. Stud. 1985, 22, 343. [Google Scholar] [CrossRef]
- Giannetta, N.; Villa, G.; Pennestrì, F.; Sala, R.; Mordacci, R.; Manara, D.F. Instruments to assess moral distress among healthcare workers: A systematic review of measurement properties. Int. J. Nurs. Stud. 2020, 111, 103767. [Google Scholar] [CrossRef] [PubMed]
- Fourie, C. Who Is Experiencing What Kind of Moral Distress? Distinctions for Moving from a Narrow to a Broad Definition of Moral Distress. AMA J. Ethics 2017, 19, 578–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, S.D.; Allen, D. “Hutch” Moral Distress: One Unit’s Recognition and Mitigation of This Problem. Clin. J. Oncol. Nurs. 2020, 24, 16–18. [Google Scholar] [CrossRef]
- Ando, M.; Kawano, M. Relationships among moral distress, sense of coherence, and job satisfaction. Nurs. Ethics 2018, 25, 571–579. [Google Scholar] [CrossRef]
- Robert, R.; Kentish-Barnes, N.; Boyer, A.; Laurent, A.; Azoulay, E.; Reignier, J. Ethical dilemmas due to the COVID-19 pandemic. Ann. Intensive Care 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Menon, V.; Padhy, S.K. Ethical dilemmas faced by health care workers during COVID-19 pandemic: Issues, implications and suggestions. Asian J. Psychiatry 2020, 51, 102116. [Google Scholar] [CrossRef] [PubMed]
- Manara, D.F.; Giannetta, N.; Villa, G. Violence versus gratitude: Courses of recognition in caring situations. Nurs. Philos. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Technical Series on Primary Health Care. 2018. Available online: https://www.who.int/docs/default-source/primary-health-care-conference/public-health.pdf?sfvrsn=2ca0881d_2 (accessed on 14 July 2021).
- Pennestrì, F.; Gaudioso, A.; Jani, A.; Bottinelli, E.; Banfi, G. Is administered competition suitable for dealing with a public health emergency? Lessons from the healthcare system at the centre of early COVID19 outbreak in Italy. Cent. Eur. J. Public Health 2021, 29, 109–116. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Gágyor, I.; Heßling, A.; Heim, S.; Frewer, A.; Nauck, F.; Himmel, W. Ethical challenges in primary care: A focus group study with general practitioners, nurses and informal caregivers. Fam. Pract. 2018, 36, 225–230. [Google Scholar] [CrossRef]
- Siqueira-Batista, R.; Gomes, A.P.; Motta, L.C.S.; Rennó, L.; Lopes, T.C.; Miyadahira, R.; Vaz Vidal, S.; Cotta, R.M.M. (Bio)ethics and family health strategy: Mapping problems. Saude Soc. 2015, 24, 113–128. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, R.; Junges, J.R. The Construction of Ethical Competence in the Perception of Primary Care Nurses. Rev. Esc. Enferm. USP 2014, 48, 329–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, M.; Karlsson, C.; Da Silva, A.B.; Berggren, I.; Söderlund, M. Community nurses’ experiences of ethical problems in end-of-life care in the patient’s own home. Scand. J. Caring Sci. 2012, 27, 831–838. [Google Scholar] [CrossRef]
- Karlsson, M.; Roxberg, Å.; Da Silva, A.B.; Berggren, I. Community nurses’ experiences of ethical dilemmas in palliative care: A Swedish study. Int. J. Palliat. Nurs. 2010, 16, 224–231. [Google Scholar] [CrossRef]
- Porr, C.; Gaudine, A.; Woo, K.; Smith-Young, J.; Green, C. How Community Nurses Manage Ethical Conflicts: A Grounded Theory Study. Glob. Qual. Nurs. Res. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Barth, P.O.; Ramos, F.R.S.; Barlem, E.L.D.; Rennó, H.M.S.; Brehmer, L.C.D.F.; Rocha, J.M. Generating situations of Moral Distress in Primary Care Nurses. Rev. Bras. Enferm. 2019, 72, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalla Nora, C.R.; Campos Pavone Zoboli, E.L.; Vieira, M.M. Moral sensitivity in Primary Health Care nurses. Rev. Bras. Enferm. 2017, 70, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadıoğlu, F.G.; Can, R.; Nazik, S.; Kadıoğlu, S. Ethical problems in geriatrics: Views of Turkish primary healthcare professionals. Geriatr. Gerontol. Int. 2012, 13, 1059–1068. [Google Scholar] [CrossRef]
- de Veer, A.J.E.; Francke, A.L.; Struijs, A.; Willems, D.L. Determinants of moral distress in daily nursing practice: A cross sectional correlational questionnaire survey. Int. J. Nurs. Stud. 2013, 50, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, R.; Zoboli, E.L.; Vieira, M. Psychometric evaluation of the Moral Distress Risk Scale: A methodological study. Nurs. Ethics 2017, 26, 434–442. [Google Scholar] [CrossRef]
- Barth, P.O.; Ramos, F.R.S.; Barlem, E.L.D.; Dalmolin, G.D.L.; Schneider, D.G. Validation of a moral distress instrument in nurses of primary health care. Rev. Lat. Am. Enferm. 2018, 26, e3010. [Google Scholar] [CrossRef]
- Burston, A.; Eley, R.; Parker, D.; Tuckett, A. Validation of an instrument to measure moral distress within the Australian residential and community care environments. Int. J. Older People Nurs. 2016, 12, e12144. [Google Scholar] [CrossRef]
- Dalla Nora, C.; Zoboli, E.L.; Vieira, M. Ethical problems experienced by nurses in primary health care: Integrative literature review. Rev. Gaucha Enferm. 2015, 36, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Kayser, J.W.; Nault, D.; Ostiguy, G. Resolving Moral Distress When Caring for Patients Who Smoke While Using Home Oxygen Therapy. Home Health Nurse J. Home Care Hosp. Prof. 2012, 30, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Van der Dam, S.; Abma, T.; Kardol, M.; Widdershoven, G. ‘Here’s My Dilemma’. Moral Case Deliberation as a Platform for Discussing Everyday Ethics in Elderly Care. Health Care Anal. 2012, 20, 250–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauwerse, L.; van der Dam, S.; Abma, T. Morality in the mundane: Specific needs for ethics support in elderly care. Nurs. Ethics 2012, 19, 91–103. [Google Scholar] [CrossRef]
- De Brasi, E.L.; Giannetta, N.; Ercolani, S.; Gandini, E.L.M.; Moranda, D.; Villa, G.; Manara, D.F. Nurses’ moral distress in end-of-life care: A qualitative study. Nurs. Ethics 2020. [Google Scholar] [CrossRef] [PubMed]
- Epstein, E.G.; Whitehead, P.B.; Prompahakul, C.; Thacker, L.R.; Hamric, A.B. Enhancing Understanding of Moral Distress: The Measure of Moral Distress for Health Care Professionals. AJOB Empir. Bioeth. 2019, 10, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Manara, D.F.; Villa, G.; Moranda, D. In search of salience: Phenomenological analysis of moral distress. Nurs. Philos. 2014, 15, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Adibelli, D.; Kılıç, D. Difficulties experienced by nurses in older patient care and their attitudes toward the older patients. Nurse Educ. Today 2013, 33, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Daniels, N. Just Health: Meeting Health Needs Fairly; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Montgomery, A.; Panagopoulou, E.; Esmail, A.; Richards, T.; Maslach, C. Burnout in healthcare: The case for organisational change. BMJ 2019, 366, l4774. [Google Scholar] [CrossRef]

{kind=link}
| Author(s) | Title | Design of Study | Aim | Sample | Main Measures of MD | Main Findings |
|---|---|---|---|---|---|---|
| Schaefer, R.; Zoboli, E.L.C.P.; Vieira, M.M. (2019) | Psychometric evaluation of the Moral Distress Risk Scale: A methodological study | Validation study | To psychometrically test the Moral Distress Risk Scale. | 268 nurses. Of these, 97 working in primary healthcare services. | Moral Distress Risk Scale (MDRS) | “The Moral Distress Risk Scale is composed of 7 factors and 30 items; it shows evidence of acceptable reliability and validity with a Cronbach’s a = 0.913, a total variance explained of 59%, a Kaiser–Meyer–Olkin = 0.896, and a significant Bartlett <0.001” |
| Porr, C.; Gaudine, A.; Woo, K.; Smith-Young, J.; Green, C. (2019) | How Community Nurses Manage Ethical Conflicts: A Grounded Theory Study | Qualitative study | To uncover the process of behaviors enacted by community nurses when experiencing ethical conflicts | 24 community health (as home nurses or public health nurses) | Interviews | “Moral Compassing comprises processes that resolve this main concern by providing community nurses with the means to attain the moral agency necessary to decide to act or to decide not to act. The processes are undergoing a visceral reaction, self-talk, seeking validation, and mobilizing support for action or inaction. [The authors] also discovered that community nurses may experience continuing distress that we labeled moral residue”. |
| Barth, P.O.; Ramos, F.R.S.; Barlem, E.L.D.; Rennó, H.M.S.; Brehmer, L.C.F.; Rocha, J.M. (2019) | Generating situations of Moral Distress in Primary Care Nurses | Qualitative study | To analyze the situations generating Moral Distress in Primary Care nurses from different regions of Brazil. | 13 nurses of primary health care | Semi-structured interviews | Causes of moral distress in primary care settings are related to the professional’s everyday life, such as lack of conditions and organization of the work process, conflicts in interpersonal relationships (user, community, health professionals) and conflicts related to management of services and the health system |
| Gágyor, I.; Heßling, A.; Heim, S.; Frewer, A.; Nauck, F.; Himmel, W. (2018) | Ethical challenges in primary care: A focus group study with general practitioners, nurses and informal caregivers | Qualitative study | To describe ethical problems from the perspective of these three groups and to investigate whether there is a common experience of ethical issues in primary care. | 7 nurses | Focus groups | “Nurses were concerned about bureaucratic and other barriers to professional care and about dual loyalty if they had to consider the conflicting interests of patients and family members. They often felt powerless and unable to act according to their professional standards. Informal caregivers reported problems that resulted from role strain and being both a family member and a caregiver. GPs, nurses and informal caregivers sometimes perceived the other parties as a source of ethical problems” |
| Barth, P.O.; Ramos, F.R.S.; Barlem, E.L.D.; Dalmolin, G.L.; Schneider, D.G. (2018) | Validation of a moral distress instrument in nurses of primary health care | Validation study | To validate an instrument to identify situations that trigger moral distress in relation to intensity and frequency in primary health care nurses. | 433 nurses | Brazilian Scale of Moral Distress in Nurses | “There were 46 questions validated divided into six constructs: Health Policies, Working Conditions, Nurse Autonomy, Professional ethics, Disrespect to patient autonomy and Work Overload. The instrument had satisfactory internal consistency, with Cronbach’s alpha 0.98 for the instrument, and between 0.96 and 0.88 for the constructs.” |
| Burston, A.; Eley, R.; Parker, D.; Tuckett, A. (2017) | Validation of an instrument to measure moral distress within the Australian residential and community care environments | Validation study | To gain insight into the experience of moral distress within the aged care workforce. To use and validate an existing instrument to measure moral distress within the aged care setting. | 106 nurses | Moral Distress Scale- Revised | “The frequency component of the instrument demon- strated an alpha of 0.89, the intensity component 0.95 and the instrument as a whole 0.94. Three factors were identified and labelled as: Quality of Care, Capacity of Team and Professional Practice. Mean scores indicate a low occurrence of moral distress, but this distress, when experienced, was felt with a moderate level of intensity. Primary causes of moral distress were insufficient staff competency levels, poor quality care because of poor communication and delays in implementing palliation.” |
| Nora, C.R.; Zoboli, E.L.; Vieira, M.M. (2017) | Moral sensitivity in Primary Health Care nurses | Quantitative study | To characterize the profi le and describe the moral sensitivity of primary health care nurses. | 100 nurses | Moral Sensitivity Questionnaire | “the nurses had an average moral sensitivity of 4.5 (out of 7). The dimensions with the greatest moral sensitivity were: interpersonal orientation, professional knowledge, moral confl ict and moral meaning.” |
| Siqueira-Batista, R.; Gomes, A.P.; Motta, L.C.S.; Rennó, L.; Lopes, T.C.; Miyadahira, R.; Vidal, S.V.; Cotta, R.M.M. (2015) | (Bio)ethics and family health strategy: Mapping problems | Qualitative study | To outline the main (bio)ethical problems identified by members of the Family Health Strategy (FHS) teams in the town of Viçosa, Minas Gerais, Brazil. | 73 nurses | Interviews | “It was possible to categorize five major groups of (bio)ethical issues experienced by teams: those related to unequal access to health services; those related to the teaching-work-community relation; those related to secrecy and confidentiality; those related to conflicts between team and users; and those related to conflicts between team members.” |
| Nora, C.R.; Zoboli, E.L.; Vieira, M. (2015) | Ethical problems experienced by nurses in primary health care: integrative literature review | Integrative review | To identify ethical problems experienced by nurses in primary health care and resources for coping based on publications on the subject | - | - | “This analysis resulted in four categories: ethical problems in the relationship between team members, ethical problems in the relationship with the user, ethical problems in health services management and resources for coping with ethical problems. Results showed that nurses need to be prepared to face ethical problems, emphasizing the importance of ethics education during the education process before and during professional practice to enhance the development of ethical sensitivity and competence for problem resolution” |
| Schaefer, R.; Junges, J.R. (2014) | The construction of ethical competence in the perception of primary care nurses | Qualitative study | To understand the per-ception of nurses of Primary Care Services about the construction of ethical compe-tence on their formation and practices. | 10 nurses | Interviews | “The results showed that the interviewed professionals had already experienced situations with ethical conflicts and knew what ethical competen-ce means. The central themes point out three fundamental issues in the construc-tion of the ethical competence: personal values, education and practice. Taking into account that ethical competence is in per-manent construction, the study shows the importance to promote organizational and educational activities in a transversal man-ner, as a tool to cope the moral stress and contribute in improving the quality of care in the primary health attention” |
| Karlsson, M.; Karlsson, C.; Barbosa da Silva, A.; Berggren, I.; Söderlund, M. (2013) | Community nurses’ experiences of ethical problems in end-of-life care in the patient’s own home | Qualitative study | To gain a deeper understanding of community nurses’ experiences of ethical problems in end-of-life care in the patient′s own home | 10 nurses | Inteviews | “In the first step of interpretation, two themes emerged: Uncomfortable feelings and Lack of cooperation and in the second step, one theme Lack of security emerged. Finally, the overall interpretation revealed the theme Feelings of loss of control in end-of-life care in the patient’s own home.” |
| Kadioǧlu, F.G.; Can, R.; Nazik, S.; Kadioǧlu, S. (2013) | Ethical problems in geriatrics: Views of Turkish primary healthcare professionals | Quantitative study | To determine the frequency rates of various geriatric ethical problems and to evaluate the importance given to these problems in primary healthcare. | 36 nurse | Questionnaire | “Based on the results, the most frequently encountered ethical issues were on “decision-making competency” and these issues respectively were “decision-making with relatives instead of elder patients”, “not informing elders due to the lack of tolerance” and “not informing elders due to the lack of comprehending”. The most important geriatric ethical issues were “ignoring respect for privacy”, “ignoring patient’s complaints” and “rejecting detailed examination or treatment because of age”. |
| De Veer, A.J.E.; Francke, A.L.; Struijs, A.; Willems, D.L. (2013) | Determinants of moral distress in daily nursing practice: A cross sectional correlational questionnaire survey | Quantitative study | To identify individual and job characteristics associated with moral distress in nursing staff | 365 nurses | Moral distress questionnaire and MAS-GZ | “Nursing staff in nursing homes had the highest scores and this was statistically significantly higher than those in home care, which had the lowest mean. |
| Kayser, J.W.; Nault, D.; Ostiguy, G. (2012) | Resolving moral distress when caring for patients who smoke while using home oxygen therapy | Case study | To describe this distress, then to propose a 3-step process of taking concrete actions to resolve the distress | - | - | “Three steps to resolve the moral distress described in this case scenario are proposed. Step 1 entails better understanding the competing moral principles that cause the distress. Step 2 entails better understanding what care options are available for the patient in question. And Step 3 involves taking action.” |
| Karlsson, M.; Roxberg, A.; Da Silva, A.B.; Berggren, I. (2010) | Community nurses’ experiences of ethical dilemmas in palliative care: A Swedish study | Qualitative study | To highlight community nurses’ experiences of ethical dilemmas in palliative care | 7 nurses | Inteviews | “The core themes that emerged were: powerlessness, frustration, and concern in relation to ethical dilemmas in palliative care. The nurses were motivated and felt responsibility for their patients’ end of life, and their relatives, and took their duties seriously. They wanted to satisfy all parties; the patient, the relatives and other palliative care professionals.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giannetta, N.; Villa, G.; Pennestrì, F.; Sala, R.; Mordacci, R.; Manara, D.F. Ethical Problems and Moral Distress in Primary Care: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7565. https://doi.org/10.3390/ijerph18147565
Giannetta N, Villa G, Pennestrì F, Sala R, Mordacci R, Manara DF. Ethical Problems and Moral Distress in Primary Care: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7565. https://doi.org/10.3390/ijerph18147565
Chicago/Turabian StyleGiannetta, Noemi, Giulia Villa, Federico Pennestrì, Roberta Sala, Roberto Mordacci, and Duilio Fiorenzo Manara. 2021. "Ethical Problems and Moral Distress in Primary Care: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 14: 7565. https://doi.org/10.3390/ijerph18147565
APA StyleGiannetta, N., Villa, G., Pennestrì, F., Sala, R., Mordacci, R., & Manara, D. F. (2021). Ethical Problems and Moral Distress in Primary Care: A Scoping Review. International Journal of Environmental Research and Public Health, 18(14), 7565. https://doi.org/10.3390/ijerph18147565