
Phase Angle and Bio-Impedance Values during the First Year after Delivery in Women with Previous Excessive Gestational Weight Gain: Innovative Data from the Belgian INTER-ACT Study

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
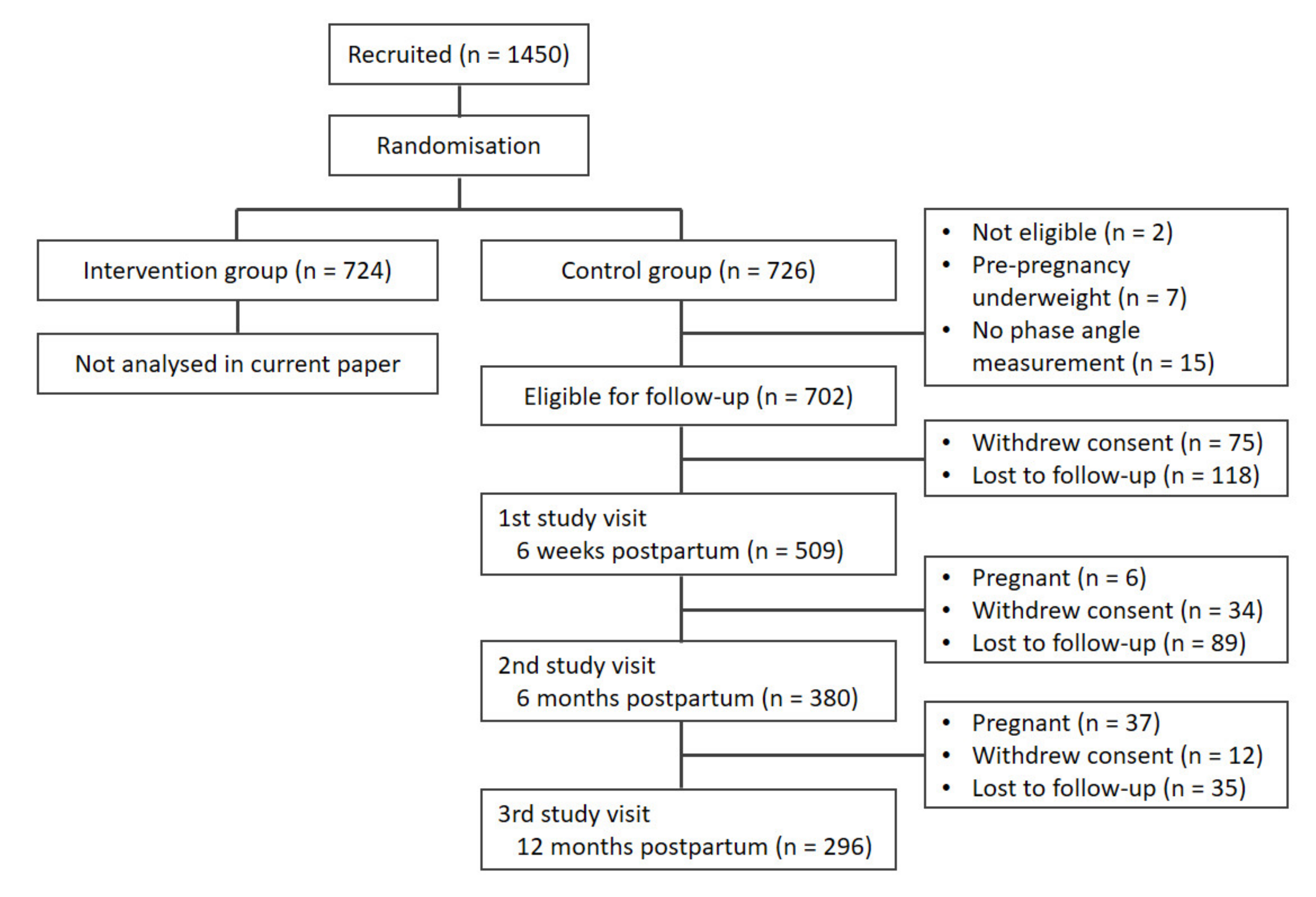
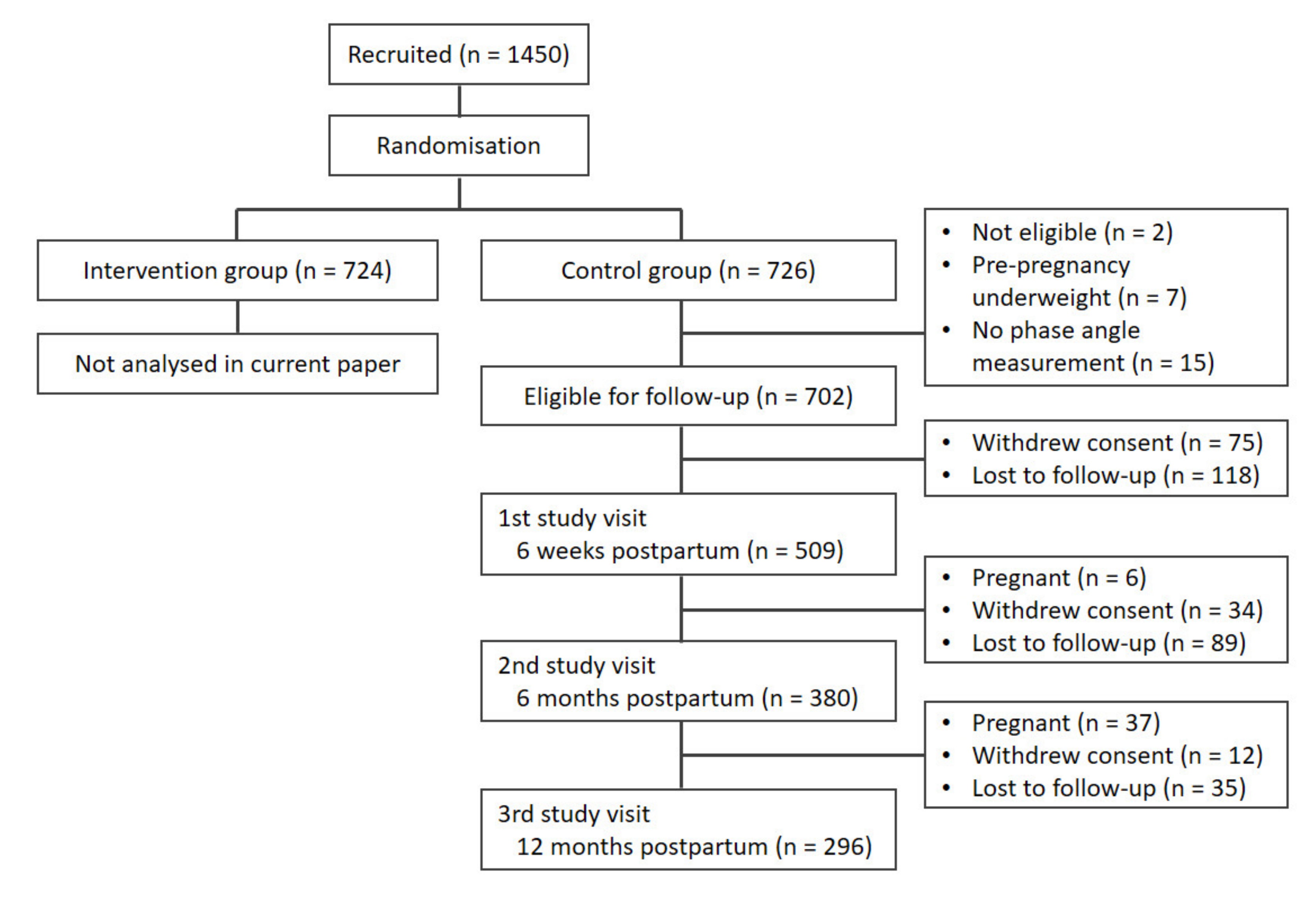
2.1. Recruitment
2.2. Anthropometric Measurements
2.3. Measurement of BIA and Calculation of Phase Angle
2.4. Questionnaire Data
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Phase Angle Values at 6 Weeks Postpartum
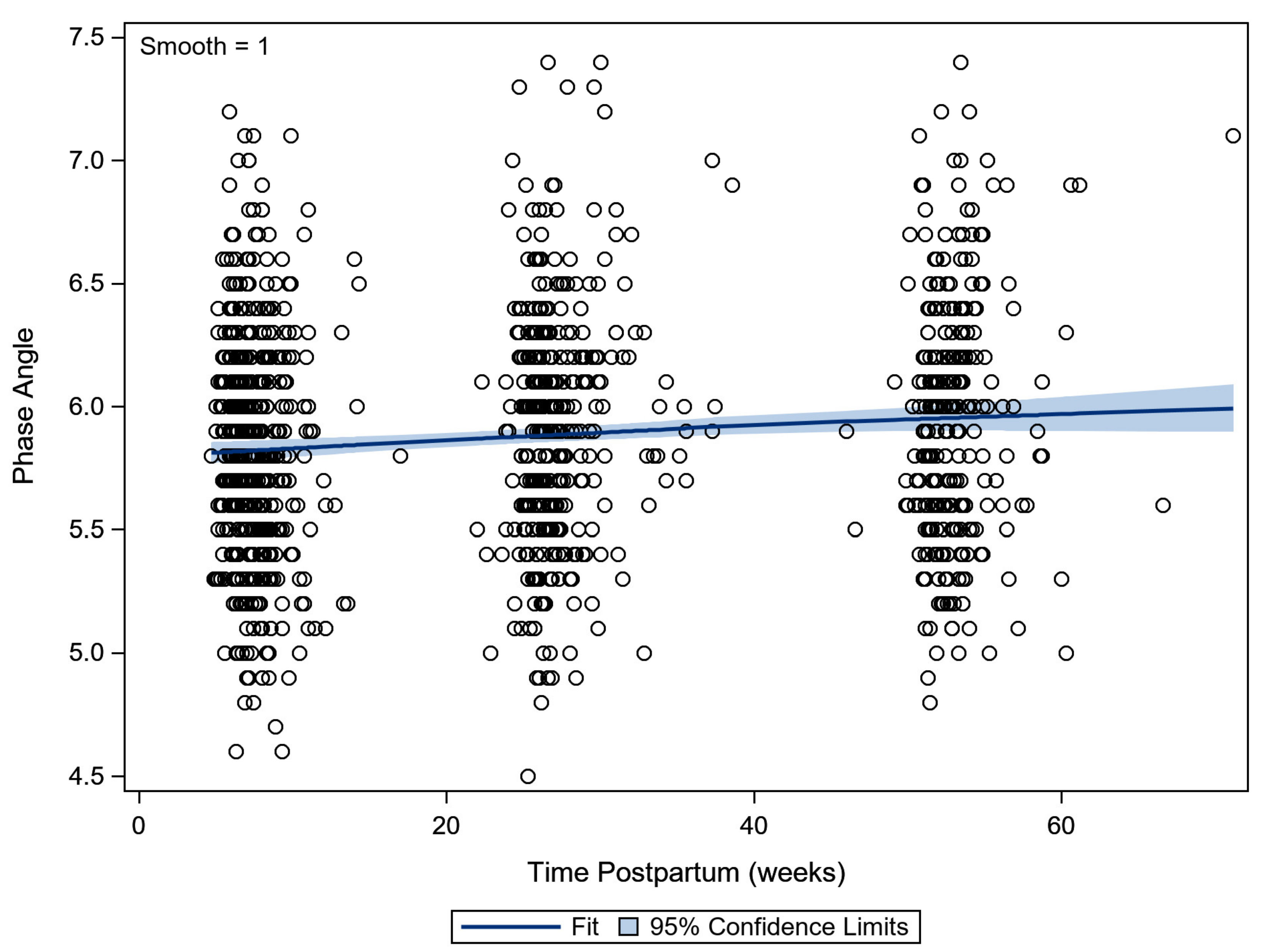
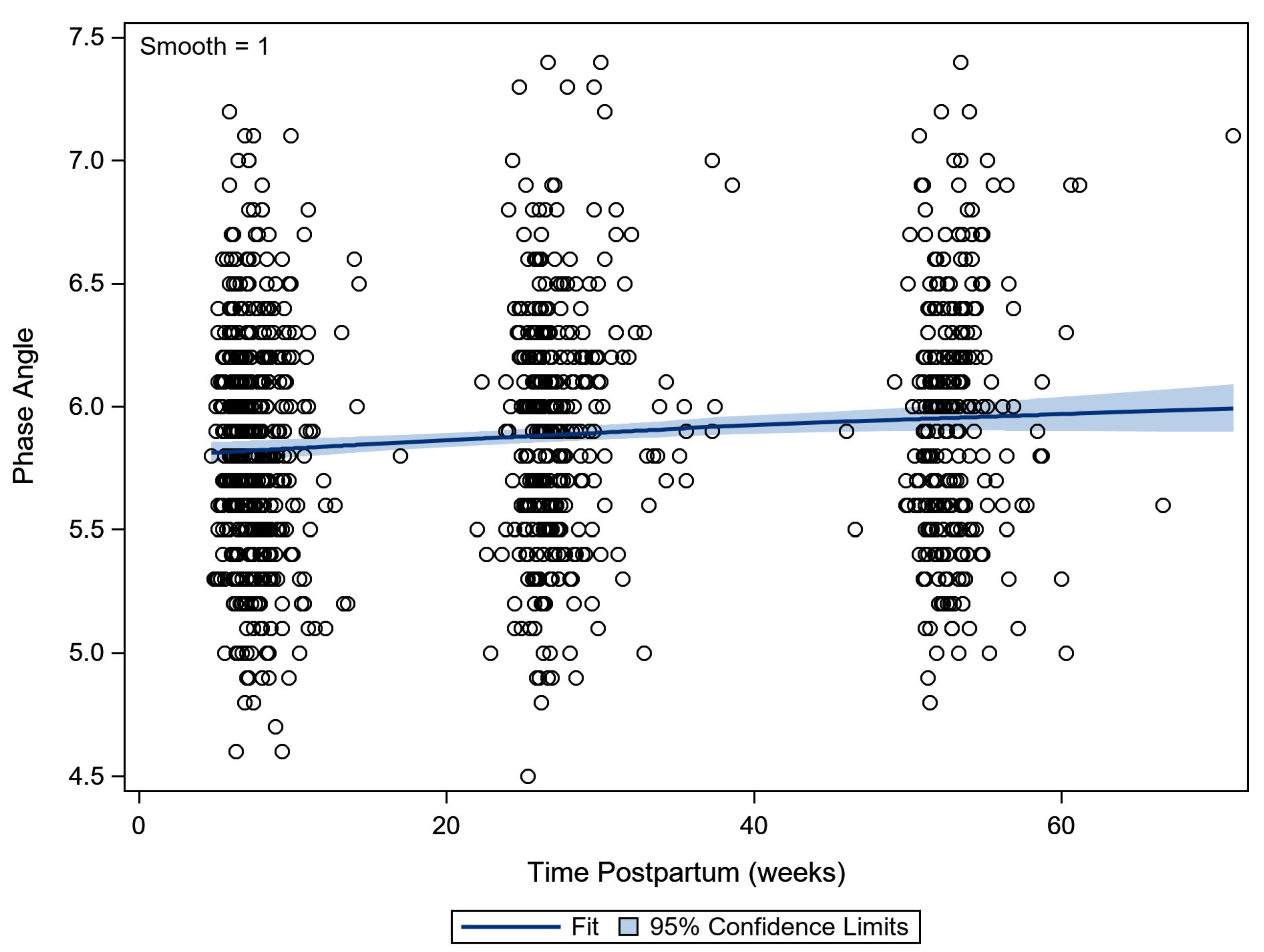
3.3. Evolution in Phase Angle in the First Year Postpartum
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berlit, S.; Tuschy, B.; Stojakowits, M.; Weiss, C.; Leweling, H.; Sutterlin, M.; Kehl, S. Bioelectrical impedance analysis in pregnancy: Reference ranges. In Vivo 2013, 27, 851–854. [Google Scholar] [PubMed]
- Institute of Medicine; National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.K.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Siminerio, L.L.; Himes, K.P.; Hutcheon, J.A.; Lash, T.L.; Parisi, S.M.; Abrams, B. Maternal obesity and gestational weight gain are risk factors for infant death. Obes. 2016, 24, 490–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogozinska, E.; Zamora, J.; Marlin, N.; Betran, A.P.; Astrup, A.; Bogaerts, A.; Cecatti, J.G.; Dodd, J.M.; Facchinetti, F.; Geiker, N.R.W.; et al. Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials. BMC Pregnancy Childb. 2019, 19, 322. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. AM. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef]
- Teulings, N.; Masconi, K.L.; Ozanne, S.E.; Aiken, C.E.; Wood, A.M. Effect of interpregnancy weight change on perinatal outcomes: Systematic review and meta-analysis. BMC Pregnancy Childb. 2019, 19, 386. [Google Scholar] [CrossRef] [Green Version]
- Timmermans, Y.E.G.; van de Kant, K.D.G.; Oosterman, E.O.; Spaanderman, M.E.A.; Villamor-Martinez, E.; Kleijnen, J.; Vreugdenhil, A.C.E. The impact of interpregnancy weight change on perinatal outcomes in women and their children: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e12974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogaerts, A.; Van den Bergh, B.R.; Ameye, L.; Witters, I.; Martens, E.; Timmerman, D.; Devlieger, R. Interpregnancy weight change and risk for adverse perinatal outcome. Obstet. Gynecol. 2013, 122, 999–1009. [Google Scholar] [CrossRef]
- Marshall, N.E.; Murphy, E.J.; King, J.C.; Haas, E.K.; Lim, J.Y.; Wiedrick, J.; Thornburg, K.L.; Purnell, J.Q. Comparison of multiple methods to measure maternal fat mass in late gestation. Am. J. Clin. Nutr. 2016, 103, 1055–1063. [Google Scholar] [CrossRef] [Green Version]
- Most, J.; Marlatt, K.L.; Altazan, A.D.; Redman, L.M. Advances in assessing body composition during pregnancy. Eur. J. Clin. Nutr. 2018, 72, 645–656. [Google Scholar] [CrossRef]
- Norman, K.; Stobaus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis--clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Danielzik, S.; Dörhöfer, R.P.; Later, W.; Wiese, S.; Müller, M.J. Phase angle from bioelectrical impedance analysis: Population reference values by age, sex, and body mass index. JPEN J. Parenter Enteral. Nutr. 2006, 30, 309–316. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Hall, C.B.; Siders, W.A. Assessment of change in hydration in women during pregnancy and postpartum with bioelectrical impedance vectors. Nutr. 2007, 23, 543–550. [Google Scholar] [CrossRef]
- Ellegard, L.; Bertz, F.; Winkvist, A.; Bosaeus, I.; Brekke, H.K. Body composition in overweight and obese women postpartum: Bioimpedance methods validated by dual energy X-ray absorptiometry and doubly labeled water. Eur. J. Clin. Nutr. 2016, 70, 1181–1188. [Google Scholar] [CrossRef]
- Shaikh, S.; Schulze, K.J.; Ali, H.; Labrique, A.B.; Shamim, A.A.; Rashid, M.; Mehra, S.; Christian, P.; West, K.P. Bioelectrical impedance among rural Bangladeshi Women during pregnancy and in the postpartum period. J. Health Popul. Nutr. 2011, 29, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Bogaerts, A.; Bijlholt, M.; Mertens, L.; Braeken, M.; Jacobs, B.; Vandenberghe, B.; Ameye, L.; Devlieger, R. Development and Field Evaluation of the INTER-ACT App, a Pregnancy and Interpregnancy Coaching App to Reduce Maternal Overweight and Obesity: Mixed Methods Design. JMIR Form Res. 2020, 4, e16090. [Google Scholar] [CrossRef]
- Bogaerts, A.; Ameye, L.; Bijlholt, M.; Amuli, K.; Heynickx, D.; Devlieger, R. INTER-ACT: Prevention of pregnancy complications through an e-health driven interpregnancy lifestyle intervention—Study protocol of a multicentre randomised controlled trial. BMC Pregnancy Childb. 2017, 17, 154. [Google Scholar] [CrossRef] [Green Version]
- Matthys, C.; Meulemans, A.; Van der Schueren, B. Development and validation of general FFQ for use in clinical practice. Ann. Nutr. Metab. 2015, 67, 239. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Streb, A.R.; Hansen, F.; Gabiatti, M.P.; Tozetto, W.R.; Del Duca, G.F. Phase angle associated with different indicators of health-related physical fitness in adults with obesity. Physiol. Behav. 2020, 225, 113104. [Google Scholar] [CrossRef] [PubMed]
- Popiołek-Kalisz, J.; Teter, M.; Kozak, G.; Powrózek, T.; Mlak, R.; Sobieszek, G.; Karakuła-Juchnowicz, H.; Małecka-Massalska, T. Potential bioelectrical impedance analysis (BIA) parameters in prediction muscle strength in women with anorexia nervosa. World J. Biol. Psychia. 2020, 1–11. [Google Scholar] [CrossRef]
- Bittencourt, D.C.D.; Schieferdecker, M.E.M.; Macedo, D.S.; Biesek, S.; Silveira Gomes, A.R.; Rabito, E.I. Phase Angle Reflects Loss of Functionality in Older Women. J. Nutr. Health Aging. 2020, 24, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Gerken, A.L.H.; Rohr-Kräutle, K.K.; Weiss, C.; Seyfried, S.; Reissfelder, C.; Vassilev, G.; Otto, M. Handgrip Strength and Phase Angle Predict Outcome After Bariatric Surgery. Obes. Surg. 2021, 31, 200–206. [Google Scholar] [CrossRef] [PubMed]
- D’Ettorre, M.; Bracaglia, R.; Gentileschi, S.; Tambasco, D. Micro-and macroscopic tissue modifications after bariatric surgery: Effects of different procedures—A pilot study. Aesthetic Plast. Surg. 2013, 37, 846–848. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.; Schoenfeld, B.J.; Dos Santos, L.; Nunes, J.P.; Tomeleri, C.M.; Cunha, P.M.; Sardinha, L.B.; Cyrino, E.S. Resistance Training Improves a Cellular Health Parameter in Obese Older Women: A Randomized Controlled Trial. J. Strength Cond. Res. 2020, 34, 2996–3002. [Google Scholar] [CrossRef]
- Piuri, G.; Ferrazzi, E.; Bulfoni, C.; Mastricci, L.; Di Martino, D.; Speciani, A.F. Longitudinal changes and correlations of bioimpedance and anthropometric measurements in pregnancy: Simple possible bed-side tools to assess pregnancy evolution. J. Matern Fetal Neonatal Med. 2017, 30, 2824–2830. [Google Scholar] [CrossRef]
- Medoua, G.N.; Nana, E.S.; Essa’a, V.J.; Ntsama, P.M.; Matchawe, C.; Rikong, H.A.; Essame Oyono, J.L. Body composition of Cameroonian lactating women determined by anthropometry, bioelectrical impedance, and deuterium dilution. Nutrition 2011, 27, 414–419. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C.G.; Barros, A.J.; Wang, J.; Heymsfield, S.B.; Pierson, R.N., Jr. Bioelectrical impedance analysis: Population reference values for phase angle by age and sex. Am. J. Clin. Nutr. 2005, 82, 49–52. [Google Scholar] [CrossRef]
- Kyle, U.G.; Genton, L.; Slosman, D.O.; Pichard, C. Fat-free and fat mass percentiles in 5225 healthy subjects aged 15 to 98 years. Nutrition 2001, 17, 534–541. [Google Scholar] [CrossRef]
- Elia, M. Body composition by whole-body bioelectrical impedance and prediction of clinically relevant outcomes: Overvalued or underused? Eur. J. Clin. Nutr. 2013, 67 (Suppl. S1), S60–S70. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| n = 509 | ||
|---|---|---|
| Age at delivery, median (IQR) | 31.2 (28.9–33.8) | |
| Parity, n (%) | Primiparous | 287 (56.4) |
| Multiparous | 222 (43.6) | |
| Sex of infant, n (%) | Boy | 266 (52.3) |
| Girl | 243 (47.7) | |
| Education, n (%) | Up to 18 years of age | 146 (29.4) |
| Bachelor’s | 194 (39.1) | |
| Master’s or higher | 156 (31.5) | |
| Missing | 13 | |
| Ethnicity, n (%) | White European | 450 (90.7) |
| Other ethnicity | 46 (9.3) | |
| Missing | 13 | |
| Pre-pregnancy BMI, n (%) | Healthy weight | 251 (49.3) |
| Overweight | 179 (35.2) | |
| Obesity | 79 (15.5) | |
| Gestational weight gain in kg, median (IQR) | Overall | 17 (15–20) |
| Healthy weight pre-pregnancy | 19 (17–21) | |
| Overweight pre-pregnancy | 16 (13–19) | |
| Obese pre-pregnancy | 13.4 (12–17) | |
| PPWR at 6 weeks PP, median (IQR) | Overall | 6.5 (3.9–9.0) |
| Healthy weight pre-pregnancy | 7.4 (5.2–9.6) | |
| Overweight pre-pregnancy | 5.8 (3.2–8.4) | |
| Obese pre-pregnancy | 4.4 (1.2–8.0) | |
| BMI at 6 weeks PP, median (IQR) | Overall | 27.7 (25.1–30.9) |
| Fat percentage at 6 weeks PP, median (IQR) | Overall | 34.9 (31.9–38.6) |
| Muscle mass (in kg) at 6 weeks PP, median (IQR)) | Overall | 47.8 (44.8–51.0) |
| Waist–hip ratio at 6 weeks PP, median (IQR) | Overall | 0.78 (0.75–0.82) |
| Phase angle (in degrees) at 6 weeks PP, median (IQR) | Overall | 5.8 (5.5–6.1) |
| Energy intake (in kcal) at 6 weeks PP, median (IQR) | Overall | 1387 (1132–1646) |
| MET-minutes per day at 6 weeks PP, median (IQR) | Overall | 265 (127–487) |
| Sedentary time in minutes per day at 6 weeks PP, median (IQR) | Overall | 300 (217–411) |
| Exclusive breastfeeding at 6 weeks PP, n (%) | Yes | 274 (55.6) |
| No | 219 (44.4) | |
| Missing | 16 |
| Association with Phase Angle | p-Value | ||
|---|---|---|---|
| Age (correlation) | 0.03 | 0.45 | |
| Parity (median (IQR)) | Nulliparous | 5.8 (5.5–6.1) | 0.02 |
| Multiparous | 5.9 (5.6–6.2) | ||
| Sex of infant (median (IQR)) | Boy | 5.8 (5.5–6.1) | 0.40 |
| Girl | 5.8 (5.5–6.2) | ||
| Education (median (IQR)) | Up to 18 years of age | 5.8 (5.5–6.3) | 0.46 |
| Bachelor’s degree | 5.8 (5.5–6.1) | ||
| Master’s degree or higher | 5.8 (5.5–6.1) | ||
| Ethnicity (median (IQR)) | White European | 5.8 (5.5–6.1) | 0.87 |
| Other ethnicity | 5.8 (5.5–6.2) | ||
| Body composition (correlation) | BMI | 0.18 | <0.001 |
| Fat percentage | −0.04 | 0.36 | |
| Muscle mass | 0.13 | 0.004 | |
| Waist–hip ratio | 0.16 | <0.001 | |
| Lifestyle factors (correlation): | Energy intake (in kcal) | 0.07 | 0.13 |
| MET-minutes/week | 0.07 | 0.16 | |
| Sedentary time/day | −0.08 | 0.12 | |
| Exclusive breastfeeding at 6 weeks (median (IQR)) | No | 5.8 (5.5–6.1) | 0.85 |
| Yes | 5.8 (5.5–6.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bijlholt, M.; Maslin, K.; Ameye, L.; Shawe, J.; Bogaerts, A.; Devlieger, R. Phase Angle and Bio-Impedance Values during the First Year after Delivery in Women with Previous Excessive Gestational Weight Gain: Innovative Data from the Belgian INTER-ACT Study. Int. J. Environ. Res. Public Health 2021, 18, 7482. https://doi.org/10.3390/ijerph18147482
Bijlholt M, Maslin K, Ameye L, Shawe J, Bogaerts A, Devlieger R. Phase Angle and Bio-Impedance Values during the First Year after Delivery in Women with Previous Excessive Gestational Weight Gain: Innovative Data from the Belgian INTER-ACT Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7482. https://doi.org/10.3390/ijerph18147482
Chicago/Turabian StyleBijlholt, Margriet, Kate Maslin, Lieveke Ameye, Jill Shawe, Annick Bogaerts, and Roland Devlieger. 2021. "Phase Angle and Bio-Impedance Values during the First Year after Delivery in Women with Previous Excessive Gestational Weight Gain: Innovative Data from the Belgian INTER-ACT Study" International Journal of Environmental Research and Public Health 18, no. 14: 7482. https://doi.org/10.3390/ijerph18147482
APA StyleBijlholt, M., Maslin, K., Ameye, L., Shawe, J., Bogaerts, A., & Devlieger, R. (2021). Phase Angle and Bio-Impedance Values during the First Year after Delivery in Women with Previous Excessive Gestational Weight Gain: Innovative Data from the Belgian INTER-ACT Study. International Journal of Environmental Research and Public Health, 18(14), 7482. https://doi.org/10.3390/ijerph18147482