
The Impact of Sedentary Behavior and Self-Rated Health on Cardiovascular Disease and Cancer among South Korean Elderly Persons Using the Korea National Health and Nutrition Examination Survey (KNHANES) 2014–2018 Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Database Information
2.2. Sedentary Behavior
2.3. Self-Rated Health
2.4. Cardiovascular Disease and Cancer
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heron, M. National Center for Health Statistics Deaths: Leading Causes for 2018. Deaths Lead. Causes 2018 2021, 68, 1–77. [Google Scholar] [CrossRef]
- Lee, D.H.; Nam, J.Y.; Kwon, S.; K+eum, N.; Lee, J.-T.; Shin, M.-J.; Oh, H. Lifestyle risk score and mortality in Korean adults: A population-based cohort study. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Cabanas-Sánchez, V.; Guallar-Castillón, P.; Higueras-Fresnillo, S.; Rodríguez-Artalejo, F.; Martínez-Gómez, D. Changes in Sitting Time and Cardiovascular Mortality in Older Adults. Am. J. Prev. Med. 2018, 54, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, E. The association between elderly people’s sedentary behaviors and their health-related quality of life: Focusing on comparing the young-old and the old-old. Health Qual. Life Outcomes 2019, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Kim, Y.; Wilkens, L.R.; Park, S.-Y.; Goodman, M.T.; Monroe, K.R.; Kolonel, L.N. Association between various sedentary behaviours and all-cause, cardiovascular disease and cancer mortality: The Multiethnic Cohort Study. Int. J. Epidemiol. 2013, 42, 1040–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, J.A.; Chastin, S.F.M.; Skelton, D.A. Prevalence of Sedentary Behavior in Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Jang, E. Low Self-Rated Health as A Risk Factor for Depression in South Korea: A Survey of Young Males and Fe-males. Healthcare 2021, 9, 452. [Google Scholar] [CrossRef]
- Han, K.-M.; Ko, Y.-H.; Yoon, H.-K.; Han, C.; Ham, B.-J.; Kim, Y.-K. Relationship of depression, chronic disease, self-rated health, and gender with health care utilization among community-living elderly. J. Affect. Disord. 2018, 241, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Schneider, T.; Faß, E.; Lochbaum, M. Personal social capital and self-rated health among middle-aged and older adults: A cross-sectional study exploring the roles of leisure-time physical activity and socioeconomic status. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Wilson, J.; Blackburn, N.E.; O’Reilly, R.; Kee, F.; Caserotti, P.; Tully, M.A. Association of objective sedentary behaviour and self-rated health in English older adults. BMC Res. Notes 2019, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Lim, S.; Lim, J.; Kim, K.; Han, M.; Yoon, I.Y.; Kim, J.; Chang, Y.; Chang, C.B.; Chin, H.J. An overview of the Ko-rean longitudinal study on health and aging. Psychiatry Investig. 2007, 4, 84. [Google Scholar]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Barnes, J.; Behrens, T.K.; Benden, M.E.; Biddle, S.; Bond, D.; Brassard, P.; Brown, H.; Carr, L.; Carson, V.; Chaput, J.-P. Letter to the Editor: Standardized use of the terms “sedentary” and “sedentary behaviours”. Mental Health Physical Act. 2013, 6, 55–56. [Google Scholar]
- An, S.Y.; Kang, H.E.; Kim, S.M.; Sok, S.A.; Yang, H.J.; Lee, G.N. Association between sitting time and diabetes mellitus, car-diovascular disease and metabolic syndrome in Korean: The sixth Korean National Health and Nutrition Examination Sur-vey 2013 and 2014. Korea J. Family Pract. 2017, 7, 558–595. [Google Scholar]
- Lee, J.; Lee, C.; Min, J.; Kang, D.-W.; Kim, J.-Y.; Yang, H.I.; Park, J.; Lee, M.-K.; Lee, M.-y.; Park, I. Development of the Kore-an Global Physical Activity Questionnaire: Reliability and validity study. Global Health Promot. 2020, 27, 44–55. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organizaion. The Asia-Pacific perspective: Redefining obesity and its treatment. Int. Obes. Task Force 2000, 2, 15–21. [Google Scholar]
- Meneguci, J.; Sasaki, J.E.; Santos, Á.D.S.; Scatena, L.M.; Damião, R. Socio-demographic, clinical and health behavior correlates of sitting time in older adults. BMC Public Health 2015, 15, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansah, J.P.; Inn, R.L.H.; Ahmad, S. An evaluation of the impact of aggressive hypertension, diabetes and smoking cessation management on CVD outcomes at the population level: A dynamic simulation analysis. BMC Public Health. 2019, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Shrivastava, U.; Misra, A.; Mohan, V.; Unnikrishnan, R.; Bachani, D. Obesity, Diabetes and Cardiovascular Diseases in India: Public Health Challenges. Curr. Diabetes Rev. 2016, 13, 65–80. [Google Scholar] [CrossRef]
- Kostis, J.B. The Importance of Managing Hypertension and Dyslipidemia to Decrease Cardiovascular Disease. Cardiovasc. Drugs Ther. 2007, 21, 297–309. [Google Scholar] [CrossRef]
- Ryou, I.; Cho, Y.; Yoon, H.-J.; Park, M. Gender differences in the effect of self-rated health (SRH) on all-cause mortality and specific causes of mortality among individuals aged 50 years and older. PLoS ONE 2019, 14, e0225732. [Google Scholar] [CrossRef] [PubMed]
- Sasco, A.; Lauby-Secretan, B.; Straif, K. Tobacco smoking and cancer: A brief review of recent epidemiological evidence. Lung Cancer 2004, 45, S3–S9. [Google Scholar] [CrossRef]
- Nagai, H.; Kim, Y.H. Cancer prevention from the perspective of global cancer burden patterns. J. Thorac. Dis. 2017, 9, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.P.; Ki, M.; Power, C. Sedentary Behaviour and Biomarkers for Cardiovascular Disease and Diabetes in Mid-Life: The Role of Television-Viewing and Sitting at Work. PLoS ONE 2012, 7, e31132. [Google Scholar] [CrossRef] [PubMed]
- Sperlich, S.; Tetzlaff, J.; Geyer, S. Trends in good self-rated health in Germany between 1995 and 2014: Do age and gender matter. Int. J. Public Health 2019, 64, 921–933. [Google Scholar] [CrossRef]
- Zhao, J.; The Thai Cohort Study Team; Yiengprugsawan, V.; Seubsman, S.-A.; Kelly, M.; Bain, C.; Sleigh, A. Self-reported health and subsequent mortality: An analysis of 767 deaths from a large Thai cohort study. BMC Public Health 2014, 14, 860. [Google Scholar] [CrossRef] [Green Version]
- Bellettiere, J.; LaMonte, M.J.; Evenson, K.R.; Rillamas-Sun, E.; Kerr, J.; Lee, I.-M.; Di, C.; Rosenberg, D.E.; Stefanick, M.L.; Buchner, D.M. Sedentary behavior and cardiovascular disease in older women: The OPACH study. Circulation 2019, 139, 1036–1046. [Google Scholar] [CrossRef]
- Santiago, L.M.; Mercante, D.R.; Mattos, I.E. Self-rated health and associated factors in elderly patients with non-Hodgkin lymphoma. Cancer Epidemiol. 2017, 51, 30–34. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Murphy, M.H.; Murphy, N.M.; Woods, C.; Nevill, A.M.; Lane, A. Prevalence and correlates of physical inac-tivity in community-dwelling older adults in Ireland. PLoS ONE 2015, 10, e0118293. [Google Scholar] [CrossRef] [Green Version]
- Nabulsi, N.A.; Alobaidi, A.; Talon, B.; Asfaw, A.A.; Zhou, J.; Sharp, L.K.; Sweiss, K.; Patel, P.R.; Ko, N.Y.; Chiu, B.C.-H.; et al. Self-reported health and survival in older patients diagnosed with multiple myeloma. Cancer Causes Control. 2020, 31, 641–650. [Google Scholar] [CrossRef]
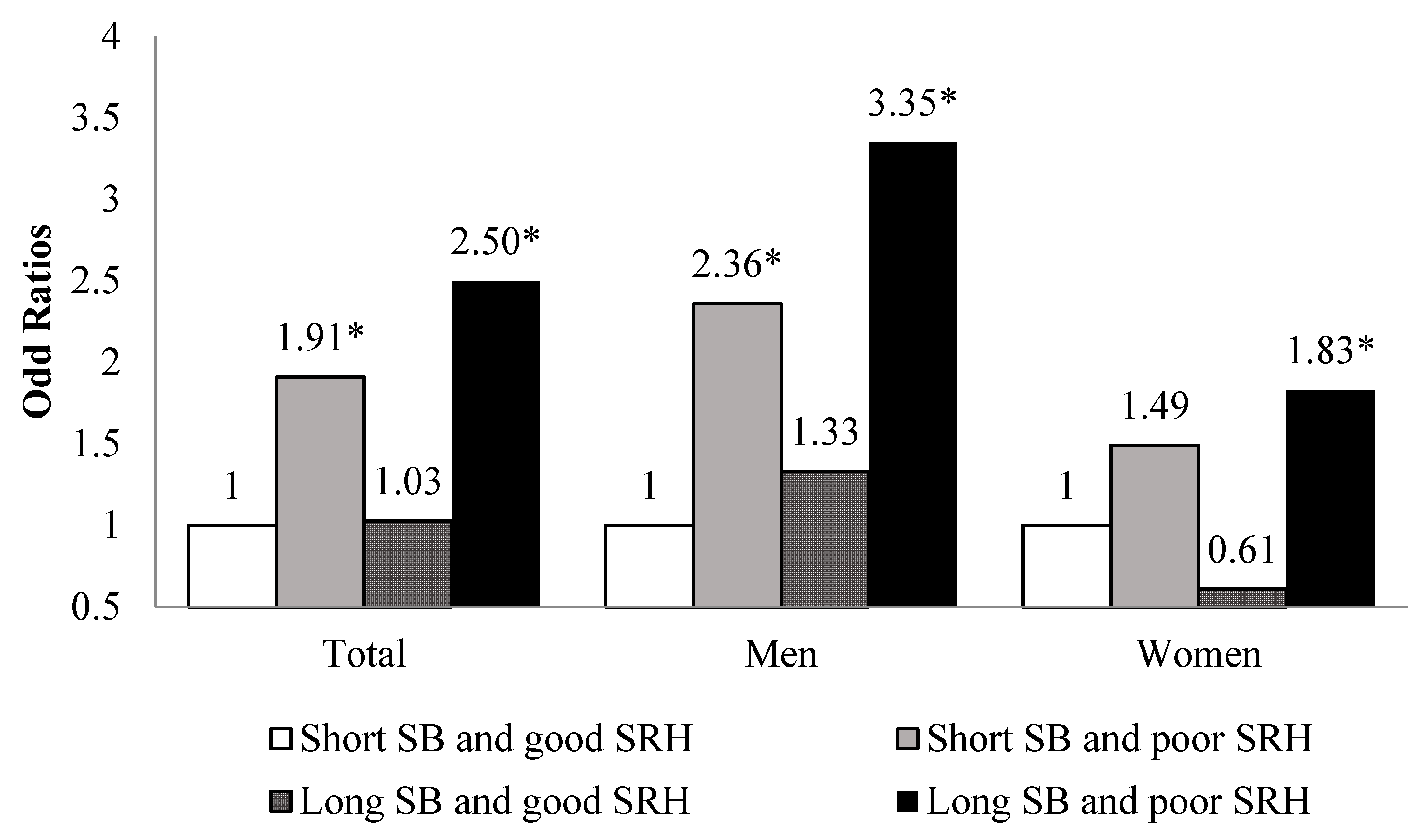

{kind=link}
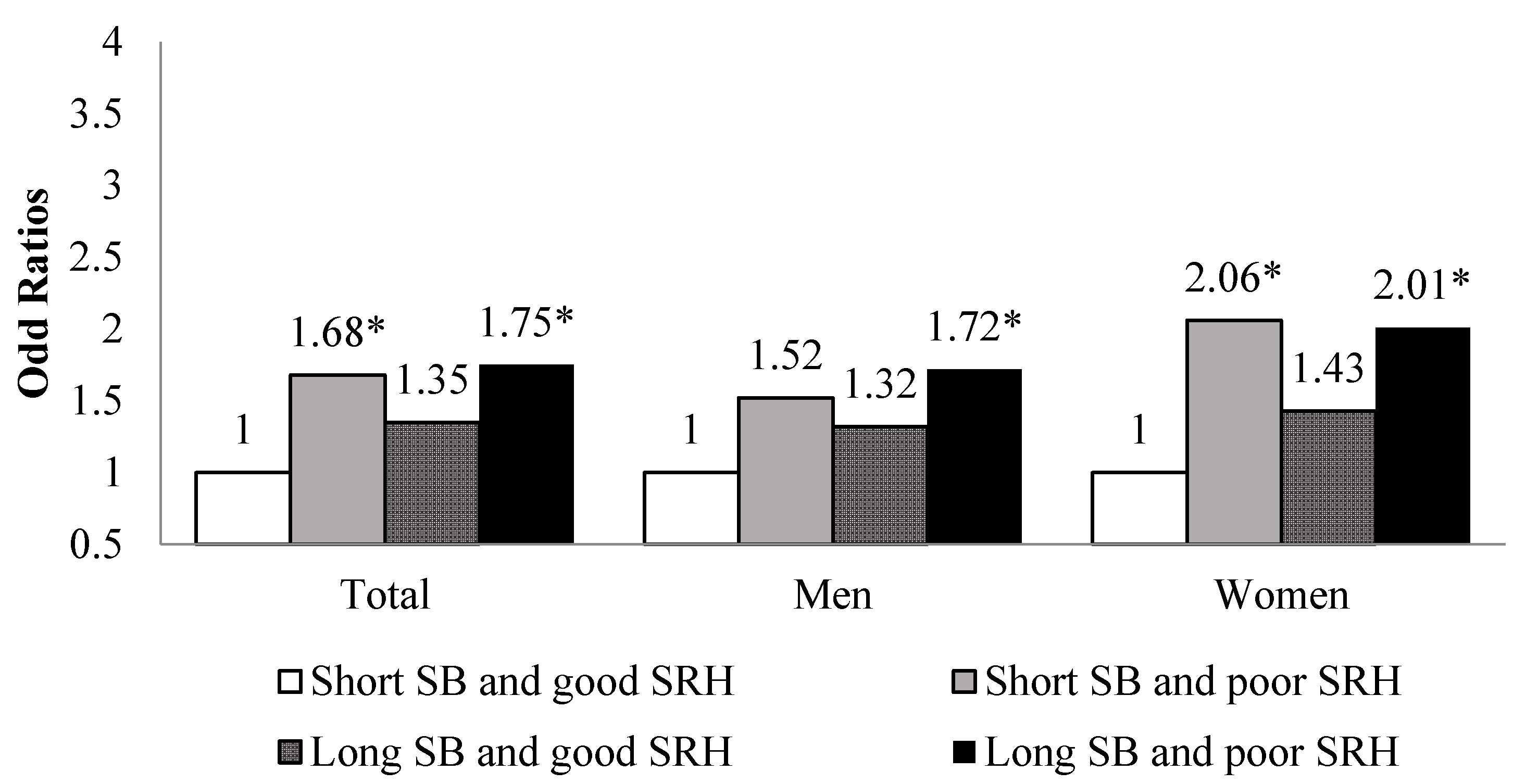
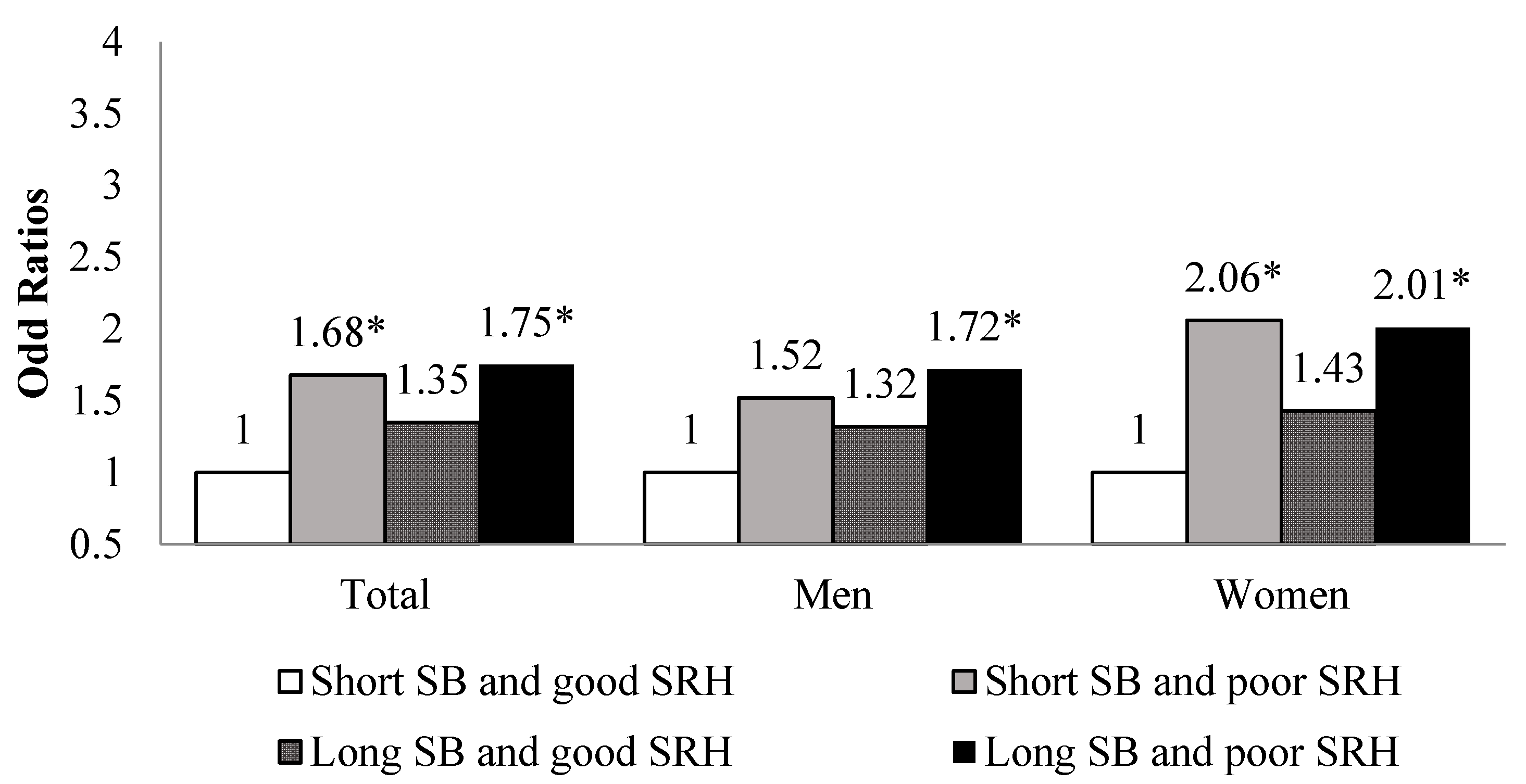{kind=link}
| Variables | Cardiovascular Disease (CVD) | Cancer | |||||
|---|---|---|---|---|---|---|---|
| Total | Yes (n = 914) | No (n = 5871) | p-Value | Yes (n = 663) | No (n = 6122) | p-Value | |
| N (%) | N (%) | N (%) | N (%) | ||||
| Sedentary behavior (hours) | |||||||
| 0–6 | 2629 | 305 (11.6) | 2324 (88.4) | 0.0003 | 243 (9.2) | 2386 (90.8) | 0.2436 |
| ≥7 | 4156 | 609 (14.7) | 3547 (85.3) | 420 (10.1) | 3736 (89.9) | ||
| Self-rated health | |||||||
| Good | 1448 | 96 (6.6) | 1352 (93.4) | <0.0001 | 111 (7.7) | 1337 (92.3) | 0.0023 |
| Poor | 5337 | 818 (23.0) | 4519 (77.0) | 552 (10.3) | 4785 (89.7) | ||
| Sex | |||||||
| Men | 3024 | 468 (15.5) | 2556 (84.5) | <0.0001 | 330 (11.0) | 2691 (89.0) | 0.0020 |
| Women | 3761 | 446 (11.9) | 3315 (88.1) | 333 (8.8) | 3431 (91.2) | ||
| Age | |||||||
| Young-old | 4615 | 567 (12.3) | 4048 (87.7) | <0.0001 | 456 (9.9) | 4159 (90.1) | 0.6585 |
| Old-old | 2170 | 347 (16.0) | 1823 (84.0) | 207 (9.5) | 1963 (90.5) | ||
| Household income | |||||||
| Quartile1 | 3107 | 435 (14.0) | 2672 (86.0) | 0.0739 | 281 (9.0) | 2826 (91.0) | 0.1254 |
| Quartile2 | 1875 | 254 (13.6) | 1621 (86.4) | 207 (11.0) | 1668 (89.0) | ||
| Quartile3 | 1042 | 148 (14.2) | 894 (85.8) | 106 (10.2) | 936 (89.8) | ||
| Quartile4 | 728 | 76 (10.4) | 652 (89.6) | 67 (9.2) | 661 (90.8) | ||
| Missing | 33 | ||||||
| Education level | |||||||
| Under middle school | 4932 | 678 (13.7) | 4254 (86.3) | 0.2408 | 440 (8.9) | 4492 (91.1) | 0.0001 |
| High schooland above | 1826 | 231 (12.7) | 1595 (87.3) | 220 (12.0) | 1606 (88.0) | ||
| Missing | 27 | ||||||
| Marital status | |||||||
| Yes | 4565 | 637 (14.0) | 3925 (86.0) | 0.0964 | 456 (10.0) | 4106 (90.0) | 0.2831 |
| No | 2171 | 271 (12.5) | 1900 (87.5) | 199 (9.2) | 1972 (90.8) | ||
| Missing | 52 | ||||||
| Physical activity | |||||||
| Yes | 2079 | 256 (12.3) | 1823 (87.7) | 0.0624 | 189 (9.1) | 1890 (90.9) | 0.2041 |
| No | 4660 | 652 (14.0) | 4008 (86.0) | 470 (10.1) | 4190 (89.9) | ||
| Missing | 46 | ||||||
| Current smoking | |||||||
| Yes | 649 | 98 (15.1) | 551 (84.9) | 0.2110 | 47 (7.2) | 602 (92.8) | 0.0252 |
| No | 6052 | 807 (13.3) | 5245 (86.7) | 604 (10.0) | 5448 (90.0) | ||
| Missing | 84 | ||||||
| High-risk alcohol drinking | |||||||
| Yes | 272 | 27 (9.9) | 245 (90.1) | 0.0777 | 20 (7.3) | 252 (92.7) | 0.1807 |
| No | 6435 | 879 (13.7) | 5556 (86.3) | 631 (9.8) | 5804 (90.2) | ||
| Missing | 78 | ||||||
| Waist circumference | |||||||
| Normal | 3889 | 481 (12.4) | 3408 (87.6) | 0.0008 | 245 (9.0) | 2508 (91.0) | 0.0318 |
| Obese | 2753 | 419 (15.2) | 2334 (84.8) | 408 (10.5) | 3481 (89.5) | ||
| Missing | 143 | ||||||
| Diabetes mellitus | |||||||
| Yes | 1501 | 268 (17.9) | 1233 (82.1) | <0.0001 | 149 (9.9) | 1352 (90.1) | 0.5555 |
| No | 4495 | 516 (11.5) | 3979 (88.5) | 423 (9.4) | 4072 (90.6) | ||
| Missing | 789 | ||||||
| Hypertension | |||||||
| Yes | 4247 | 660 (15.5) | 3587 (84.5) | <0.0001 | 389 (9.2) | 3858 (90.8) | 0.0251 |
| No | 2530 | 253 (10.0) | 2277 (90.0) | 274 (10.8) | 2256 (89.2) | ||
| Missing | 8 | ||||||
| Dyslipidemia | |||||||
| Yes | 2397 | 362 (15.1) | 2035 (84.9) | 0.0036 | 216 (9.1) | 2167 (90.9) | 0.1440 |
| No | 4388 | 552 (12.6) | 3836 (87.4) | 443 (10.2) | 3913 (89.8) | ||
| Cardiovascular Disease (CVD) | Cancer | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Sedentary behavior | ||||
| 0–6 | 1.00 | 1.00 | ||
| ≥7 | 1.28 | 1.08–1.51 | 1.10 | 0.91–1.33 |
| Self-rated health | ||||
| Good | 1.00 | 1.00 | ||
| Poor | 2.36 | 1.85–3.01 | 1.48 | 1.17–1.88 |
| Sex | ||||
| Women | 1.00 | 1.00 | ||
| Men | 1.73 | 1.43–2.09 | 1.36 | 1.10–1.69 |
| Age | ||||
| Young-old | 1.00 | 1.00 | ||
| Old-old | 1.37 | 1.15–1.63 | 1.00 | 0.81–1.23 |
| Household income | ||||
| Quartile1 | 1.25 | 0.93–1.70 | 1.12 | 0.81–1.56 |
| Quartile2 | 1.30 | 0.96–1.77 | 1.38 | 1.00–1.91 |
| Quartile3 | 1.40 | 1.00–1.95 | 1.25 | 0.88–1.78 |
| Quartile4 | 1.00 | 1.00 | ||
| Education level | ||||
| Under middle school | 1.10 | 0.90–1.33 | 0.71 | 0.57–0.87 |
| High school and above | 1.00 | 1.00 | ||
| Marital status | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.21 | 0.92–1.36 | 0.94 | 0.75–1.17 |
| Physical activity | ||||
| No | 1.08 | 0.91–1.29 | 1.18 | 0.97–1.44 |
| Yes | 1.00 | 1.00 | ||
| Current smoking | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.98 | 0.75–1.28 | 0.63 | 0.45–0.90 |
| High-risk alcohol drinking | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.52 | 0.33–0.84 | 0.64 | 0.37–1.10 |
| Waist circumference | ||||
| Normal | 1.00 | 1.00 | ||
| Obesity | 1.40 | 1.41–1.92 | 0.88 | 0.73–1.19 |
| Diabetes mellitus | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.41 | 1.19–1.67 | 1.06 | 0.86–1.30 |
| Hypertension | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.45 | 1.21–1.73 | 0.94 | 0.78–1.14 |
| Dyslipidemia | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.32 | 1.12–1.56 | 0.99 | 0.82–1.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Nam, J.Y. The Impact of Sedentary Behavior and Self-Rated Health on Cardiovascular Disease and Cancer among South Korean Elderly Persons Using the Korea National Health and Nutrition Examination Survey (KNHANES) 2014–2018 Data. Int. J. Environ. Res. Public Health 2021, 18, 7426. https://doi.org/10.3390/ijerph18147426
Park S, Nam JY. The Impact of Sedentary Behavior and Self-Rated Health on Cardiovascular Disease and Cancer among South Korean Elderly Persons Using the Korea National Health and Nutrition Examination Survey (KNHANES) 2014–2018 Data. International Journal of Environmental Research and Public Health. 2021; 18(14):7426. https://doi.org/10.3390/ijerph18147426
Chicago/Turabian StylePark, Soojin, and Jin Young Nam. 2021. "The Impact of Sedentary Behavior and Self-Rated Health on Cardiovascular Disease and Cancer among South Korean Elderly Persons Using the Korea National Health and Nutrition Examination Survey (KNHANES) 2014–2018 Data" International Journal of Environmental Research and Public Health 18, no. 14: 7426. https://doi.org/10.3390/ijerph18147426
APA StylePark, S., & Nam, J. Y. (2021). The Impact of Sedentary Behavior and Self-Rated Health on Cardiovascular Disease and Cancer among South Korean Elderly Persons Using the Korea National Health and Nutrition Examination Survey (KNHANES) 2014–2018 Data. International Journal of Environmental Research and Public Health, 18(14), 7426. https://doi.org/10.3390/ijerph18147426