
Testing the Structural Validity of the Self-Stigma Scale in Relatives of People with Autism in the Spanish Context

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Measurements
“Las siguientes preguntas hacen mención a cómo se siente actualmente acerca de la enfermedad de su hijo. Aunque usamos el término "enfermedad", piense en esto de cualquier manera que se sienta más cómodo. Marque si está totalmente en desacuerdo, en desacuerdo, se siente neutral, de acuerdo o muy de acuerdo con las siguientes afirmaciones.”
2.3. Procedure
2.4. Data Analysis
3. Results
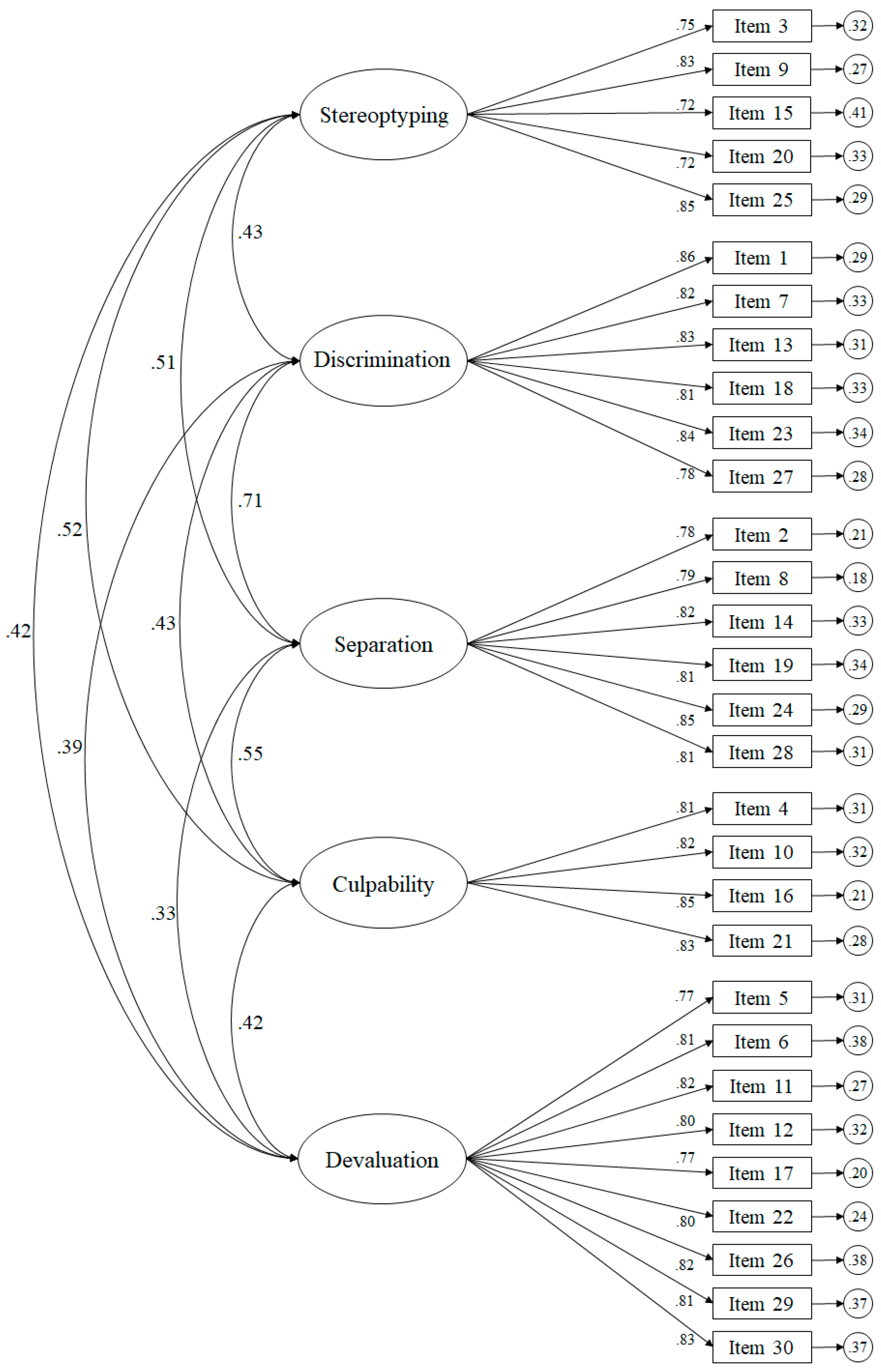
3.1. Confirmatory Factorial Analysis
3.2. Gender Invariance Analysis
3.3. Descriptive Statistics, Correlation and Reliability Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Me sentiría cómodo diciéndole a mis amistades que mi hijo/a tiene TEA.I would feel comfortable telling my friends that my child has ASD.
- Necesito esconder el trastorno de mi hijo/a.I need to hide my child’s disorder.
- El TEA de hijo/a se refleja negativamente en mí.My child’s ASD reflects negatively on me.
- Me siento culpable porque mi hijo/a tenga TEA.I feel guilty about my child having ASD.
- El TEA de mi hijo/a, me hace sentir incómodo cuando estamos en situaciones sociales.My child’s ASD makes me feel uncomfortable when we are in social situations.
- Me siento abochornado por tener un hijo/a con TEA.I feel embarrassed about having a child with ASD.
- No puedo vivir mi vida de la manera que quiero porque tengo un hijo/a con TEA.I can’t live my life the way I want to because I have a child with ASD.
- Tengo que ser selectivo con quien le cuente que tengo un hijo/a con TEA.I have to be selective about who I tell that I have a child with ASD.
- Las personas con TEA no deberían de tener hijos.People with ASD should not have children.
- 1Me siento responsable de causar el trastorno de mi hijo/a.I feel responsible for causing my child’s disorder.
- Mi vida es más plena porque tengo un hijo/a con TEA.My life is fuller because I have a child with ASD.
- Me siento avergonzado por tener un hijo/a con TEA.I feel ashamed that I have a child with ASD.
- Tener un hijo/a con TEA me ha hecho preocuparme más por mí.Having a child with ASD has made me care more about myself.
- La gente no quiere hablar conmigo debido al TEA de mi hijo/a.People don’t want to talk to me because of my child’s ASD.
- Me preocupa ser etiquetado como alguien que tiene un hijo/a con TEA.I worry about being labelled as someone who has a child with ASD.
- La gente me culpa de la enfermedad de mi hijo/a.People blame me for my child’s condition.
- Mi identidad se ha visto negativamente afectada por la trastorno de mi hijo/a.My identity has been negatively affected by my child’s condition.
- Tengo la esperanza de que algún día el trastorno del espectro autista serán tratadas con carácter normalizado.I am hopeful that one day the autistic spectrum disorder will be treated as normalised.
- Me siento fuera de lugar en el mundo porque tengo un hijo/a con TEA.I feel out of place in the world because I have a child with ASD.
- Sigo buscando señales de que mi familiar no tiene realmente TEA.I keep looking for signs that my family member does not really have ASD.
- Me culpo por el trastorno de mi hijo/a.I blame myself for my child’s disorder.
- Cuando mi hijo/a con TEA es juzgado, me siento juzgado también.When my child with ASD is judged, I feel judged too.
- Me siento discriminado/a porque tengo un hijo/a con TEA.I feel discriminated against because I have a child with an ASD.
- Me siento aislado/a porque tengo un hijo/a con TEA.I feel isolated because I have a child with an ASD.
- Minimizo la gravedad del TEA de mi hijo/a cuando lo describo a las personas.I minimise the severity of my child’s ASD when I describe it to people.
- Soy una persona más fuerte porque tengo un hijo/a con TEA.I am a stronger person because I have a child with ASD.
- Los profesionales que trabajan con mi hijo/a valoran mi conocimiento acerca del TEA.The professionals who work with my child value my knowledge about ASD.
- Puedo hablar abiertamente sobre TEA con otros miembros de mi familia.I am able to talk openly about ASD with other members of my family.
- Me siento devastado/a de que mi hijo/a tenga TEA.I feel devastated that my child has ASD.
- Mi autoestima se ha visto deteriorada debido al trastorno de mi hijo/a.My self-esteem has deteriorated because of my child’s disorder.
References
- López, S.; Rivas, R.; Taboada, E. Revisiones sobre el autismo. Rev. Latinoam. De Psicol. 2009, 41, 555–570. [Google Scholar]
- Mottron, L.; Bzdok, D. Autism spectrum heterogeneity: Fact or artifact? Mol. Psychiatry 2020, 12, 3178–3185. [Google Scholar] [CrossRef]
- Grove, J.; Ripke, S.; Als, T.D.; Mattheisen, M.; Walters, R.K.; Won, H.; Pallesen, J.; Agerbo, E.; Andreassen, O.A.; Anney, R.; et al. Identification of common genetic risk variants for autism spectrum disorder. Nat. Genet. 2019, 51, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [Green Version]
- van‘t Hof, M.; van Berckelaer-Onnes, I.; Deen, M.; Neukerk, M.C.; Bannink, R.; Daniels, A.M.; Hoek, H.W.; Ester, W.A. Novel insights into autism knowledge and stigmatizing attitudes toward mental illness in Dutch youth and family center physicians. Community Ment. Health J. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbajosa, A.B.; Pérez, F.B.; Bertina, A.; Quintana, Y.C.; Sánchez, M.B.M.; Galán, S.P. La dinámica estigmatizante: Generación y mantenimiento del estigma y el autoestigma asociado al trastorno mental en la vida cotidiana. Clínica Contemp. 2018, 9, E1. [Google Scholar]
- Corrigan, P.W.; Nieweglowski, K. How does familiarity impact the stigma of mental illness? Clin. Psychol. Rev. 2019, 70, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Midence, K.; O’neill, M. The experience of parents in the diagnosis of autism: A pilot study. Autism 1999, 3, 273–285. [Google Scholar] [CrossRef]
- Woodgate, R.L.; Ateah, C.; Secco, L. Living in a world of our own: The experience of parents who have a child with autism. Qual. Health Res. 2008, 18, 1075–1083. [Google Scholar] [CrossRef]
- Plotkin, S.; Gerber, J.S.; Offit, P.A. Vaccines and autism: A tale of shifting hypotheses. Clin. Infect. Dis. 2009, 48, 456–461. [Google Scholar]
- Kelly, A.B.; Garnett, M.S.; Attwood, T.; Peterson, C. Autism spectrum symptomatology in children: The impact of family and peer relationships. J. Abnorm. Child Psychol. 2008, 36, 1069–1081. [Google Scholar] [CrossRef]
- Gross, L. A Broken Trust: Lessons from the Vaccine–Autism Wars: Researchers long ago rejected the theory that vaccines cause autism, yet many parents don’t believe them. Can scientists bridge the gap between evidence and doubt? PLoS Biology 2009, 7, e1000114. [Google Scholar] [CrossRef] [Green Version]
- Ludlow, A.; Skelly, C.; Rohleder, P. Challenges faced by parents of children diagnosed with autism spectrum disorder. J. Health Psychol. 2012, 17, 702–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tárraga-Mínguez, R.; Gómez-Marí, I.; Sanz-Cervera, P. What Motivates Internet Users to Search for Asperger Syndrome and Autism on Google? Int. J. Environ. Res. Public Health 2020, 17, 9386. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Haller, B. Consuming image: How mass media impact the identity of people with disabilities. Commun. Q. 2013, 61, 319–334. [Google Scholar] [CrossRef]
- Bergold, S.; Hastall, M.R.; Steinmayr, R. Do Mass Media Shape Stereotypes About Intellectually Gifted Individuals? Two Experiments on Stigmatization Effects from Biased Newspaper Reports. Gift. Child Q. 2021, 65, 75–94. [Google Scholar] [CrossRef]
- Alshaigi, K.; Albraheem, R.; Alsaleem, K.; Zakaria, M.; Jobeir, A.; Aldhalaan, H. Stigmatization among parents of autism spectrum disorder children in Riyadh, Saudi Arabia. Int. J. Pediatrics Adolesc. Med. 2020, 7, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.K.S.; Lam, C.B. Self-stigma among parents of children with autism spectrum disorder. Res. Autism Spectr. Disord. 2018, 48, 44–52. [Google Scholar] [CrossRef]
- Morris, E.; Hippman, C.; Murray, G.; Michalak, E.E.; Boyd, J.E.; Livingston, J.; Inglis, A.; Carrion, P.; Austin, J. Self-stigma in relatives of people with mental illness scale: Development and validation. Br. J. Psychiatry 2018, 212, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Trigueros, R.; Aguilar-Parra, J.M.; Cangas, A.J.; Ortiz, L.; Navarro, N. Adaptation and validation to the spanish context of the scale of self-stigma in relatives of people with mental illness. Ann. Psychol. 2019, 35, 371–377. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Byrne, B.M. Structural equation modeling with AMOS, EQS, and LISREL: Comparative approaches to testing for the factorial validity of a measuring instrument. Int. J. Test. 2001, 1, 55–86. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Pearson: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Byrne, B.M.; Shavelson, R.J.; Muthén, B. Testing for the equivalence of factor covariance and mean structures: The issue of partial measurement invariance. Psychol. Bull. 1989, 105, 456. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Modeling 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Mills, L.; Meiser, B.; Ahmad, R.; Schofield, P.R.; Peate, M.; Levitan, C.; Mills, L.; Meiser, B.; Ahmad, R.; Schofield, P.R.; et al. A cluster randomized controlled trial of an online psychoeducational intervention for people with a family history of depression. BMC Psychiatry 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trigueros, R.; Navarro, N.; Cangas, A.J.; Mercader, I.; Aguilar-Parra, J.M.; González-Santos, J.; González-Bernal, J.J.; Soto-Cámara, R. The Protective Role of Emotional Intelligence in Self-Stigma and Emotional Exhaustion of Family Members of People with Mental Disorders. Sustainability 2020, 12, 4862. [Google Scholar] [CrossRef]
- Navarro-Bayón, D.; García-Heras, S.; Carrasco, O.; Casas, A. Calidad de vida, apoyo social y deterioro en una muestra de personas con trastorno mental grave. Psychosoc. Interv. 2008, 17, 321–336. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Full Version (30 items) | ||||||||||
| Models | χ2 | df | χ2/df | Δχ2 | Δdf | CFI | TLI | IFI | RMSEA (IC 90%) | SRMSR |
| Model 1 | 1761.71 | 790 | 2.23 | - | - | 0.97 | 0.97 | 0.97 | 0.052 (0.049–0.060) | 0.042 |
| Model 2 | 1882.66 | 815 | 2.31 | 31.26 | 25 | 0.97 | 0.97 | 0.97 | 0.054 (0.050–0.060) | 0.043 |
| Model 3 | 2044.91 | 845 | 2.42 | 90.66 ** | 55 | 0.96 | 0.96 | 0.96 | 0.058 (0.051–0.062) | 0.046 |
| Model 4 | 2218.81 | 860 | 2.58 | 134.67 *** | 70 | 0.95 | 0.95 | 0.95 | 0.056 (0.054–0.061) | 0.047 |
| Short Version (10 items) | ||||||||||
| Models | χ2 | df | χ2/df | Δχ2 | Δdf | CFI | TLI | IFI | RMSEA (IC 90%) | SRMSR |
| Model 1 | 188.82 | 79 | 2.39 | - | - | 0.95 | 0.95 | 0.95 | 0.059 (0.055–0.063) | 0.053 |
| Model 2 | 231.41 | 89 | 2.60 | 14.29 | 9 | 0.95 | 0.95 | 0.95 | 0.060 (0.055–0.068) | 0.052 |
| Model 3 | 241.20 | 90 | 2.68 | 26.44 | 20 | 0.94 | 0.94 | 0.94 | 0.063 (0.065–0.070) | 0.058 |
| Model 4 | 293.88 | 100 | 2.94 | 57.33 ** | 30 | 0.94 | 0.94 | 0.94 | 0.062 (0.059–0.071) | 0.054 |
| Factors | M | SD | α | ω | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Stereotyping | 1.81 | 0.80 | 0.80 | 0.83 | 0.66 *** | 0.53 ** | 0.64 *** | 0.54 *** | |
| 2. Culpability | 2.12 | 1.33 | 0.83 | 0.85 | 0.31 ** | 0.45 ** | 0.61 *** | ||
| 3. Devaluation | 1.67 | 0.80 | 0.85 | 0.87 | 0.43 *** | 0.63 *** | |||
| 4. Discrimination | 1.23 | 1.34 | 0.81 | 0.82 | 0.40 *** | ||||
| 5. Separation | 2.11 | 1.05 | 0.79 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilar-Parra, J.M.; Megias, M.M.; Trigueros, R.; Mercader, I.; Fernández-Jiménez, C.; Fernández-Campoy, J.M. Testing the Structural Validity of the Self-Stigma Scale in Relatives of People with Autism in the Spanish Context. Int. J. Environ. Res. Public Health 2021, 18, 7384. https://doi.org/10.3390/ijerph18147384
Aguilar-Parra JM, Megias MM, Trigueros R, Mercader I, Fernández-Jiménez C, Fernández-Campoy JM. Testing the Structural Validity of the Self-Stigma Scale in Relatives of People with Autism in the Spanish Context. International Journal of Environmental Research and Public Health. 2021; 18(14):7384. https://doi.org/10.3390/ijerph18147384
Chicago/Turabian StyleAguilar-Parra, José M., Maria M. Megias, Rubén Trigueros, Isabel Mercader, Carolina Fernández-Jiménez, and Juan M. Fernández-Campoy. 2021. "Testing the Structural Validity of the Self-Stigma Scale in Relatives of People with Autism in the Spanish Context" International Journal of Environmental Research and Public Health 18, no. 14: 7384. https://doi.org/10.3390/ijerph18147384
APA StyleAguilar-Parra, J. M., Megias, M. M., Trigueros, R., Mercader, I., Fernández-Jiménez, C., & Fernández-Campoy, J. M. (2021). Testing the Structural Validity of the Self-Stigma Scale in Relatives of People with Autism in the Spanish Context. International Journal of Environmental Research and Public Health, 18(14), 7384. https://doi.org/10.3390/ijerph18147384