
Designing an eHealth Well-Being Program: A Participatory Design Approach



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Participatory Design Process
3. Results
3.1. Step 1: Collecting Best Practices
3.2. Step 2: Participatory Design Sessions 1 and 2—July 2019
3.3. Step 3: First Design of Intervention Proof-of-Concept
3.4. Step 4: Participatory Design Sessions 3 and 4—September 2019
3.5. Step 5: Final Draft of Intervention Proof-of-Concept
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. The Impact of COVID-19 on Mental, Neurological and Substance Use Services. Available online: https://www.who.int/publications/i/item/978924012455 (accessed on 9 December 2020).
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLOS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef] [PubMed]
- Petzold, M.B.; Bendau, A.; Plag, J.; Pyrkosch, L.; Maricic, L.M.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.A.; Hoque, N.; Alif, S.M.; Salehin, M.; Islam, S.M.S.; Banik, B.; Sharif, A.; Nazim, N.B.; Sultana, F.; Cross, W. Factors associated with psychological distress, fear and coping strategies during the COVID-19 pandemic in Australia. Glob. Health 2020, 16, 1–15. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet. Res. 2001, 3, e20. [Google Scholar] [CrossRef] [PubMed]
- Rigby, M.; Ammenwerth, E. The Need for Evidence in Health Informatics. Stud. Health Technol. Inform. 2016, 222, 3–13. [Google Scholar]
- Enam, A.; Torres-Bonilla, J.; Eriksson, H. Evidence-Based Evaluation of eHealth Interventions: Systematic Literature Review. J. Med. Internet Res. 2018, 20, e10971. [Google Scholar] [CrossRef] [PubMed]
- Luecking, C.T.; Hennink-Kaminski, H.; Ihekweazu, C.; Vaughn, A.; Mazzucca, S.; Ward, D.S. Social marketing approaches to nutrition and physical activity interventions in early care and education centres: A systematic review. Obes. Rev. 2017, 18, 1425–1438. [Google Scholar] [CrossRef]
- Dietrich, T.; Trischler, J.; Schuster, L.; Rundle-Thiele, S. Co-designing services with vulnerable consumers. J. Serv. Theory Pract. 2017, 27, 663–688. [Google Scholar] [CrossRef] [Green Version]
- Lundkvist, A.; Yakhlef, A. Customer involvement in new service development: A conversational approach. Manag. Serv. Qual. Int. J. 2004, 14, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Witell, L.; Kristensson, P.O.; Gustafsson, A.; Löfgren, M. Idea generation: Customer co-creation versus traditional market research techniques. J. Serv. Manag. 2011, 22, 140–159. [Google Scholar] [CrossRef] [Green Version]
- Aceves-Martins, M.; Llauradó, E.; Tarro, L.; Moreno-García, C.F.; Trujillo Escobar, T.G.; Solà, R.; Giralt, M. Effectiveness of Social Marketing Strategies to Reduce Youth Obesity in European School-Based Interventions: A Systematic Review and Me-Ta-Analysis. Nutr. Rev. 2016, 74, 337–351. [Google Scholar] [CrossRef]
- Kubacki, K.; Rundle-Thiele, S. Formative Research in Social Marketing: Innovative Methods to Gain Consumer Insights; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Del Río-González, A.; Zea, M.; Calabrese, S.; Betancourt, F.; Pacheco-Cabrales, J.; Estrada-Santiago, Y.; Poppen, P. Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing Among Colombian Men Who Have Sex with Men (MSM). Int. J. Environ. Res. Public Health 2021, 18, 1811. [Google Scholar] [CrossRef]
- Costa, A.; Mourão, S.; Santos, O.; Alarcão, V.; Virgolino, A.; Nogueira, P.; Bettencourt, M.; Reis, S.; Graça, A.; Henriques, A. I-DECIDE: A Social Prescribing and Digital Intervention Protocol to Promote Sexual and Reproductive Health and Quality of Life among Young Cape Verdeans. Int. J. Environ. Res. Public Health 2021, 18, 850. [Google Scholar] [CrossRef]
- Firestone, R.; Rowe, C.J.; Modi, S.N.; Sievers, D. The effectiveness of social marketing in global health: A systematic review. Health Policy Plan. 2017, 32, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Rothberg, A.E.; McEwen, L.N.; Kraftson, A.T.; Ajluni, N.; Fowler, C.E.; Miller, N.M.; Zurales, K.R.; Herman, W.H. Factors associated with participant retention in a clinical, intensive, behavioral weight management program. BMC Obes. 2015, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, B.; Broesskamp-Stone, U.; Ruckstuhl, B.; Ackermann, G.; Spoerri, A.; Cloetta, B. Modelling the results of health promotion activities in Switzerland: Development of the Swiss Model for Outcome Classification in Health Promotion and Prevention. Health Promot. Int. 2007, 23, 86–97. [Google Scholar] [CrossRef] [PubMed]
- King, D.K.; Glasgow, R.E.; Leeman-Castillo, B. Reaiming RE-AIM: Using the Model to Plan, Implement, and Evaluate the Effects of Environmental Change Approaches to Enhancing Population Health. Am. J. Public Health 2010, 100, 2076–2084. [Google Scholar] [CrossRef]
- Fernandez, M.E.; Ruiter, R.A.C.; Markham, C.M.; Kok, G. Intervention Mapping: Theory- and Evidence-Based Health Promotion Program Planning: Perspective and Examples. Front. Public Health 2019, 7, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebden, L.; Cook, A.; Van Der Ploeg, H.P.; King, L.; Bauman, A.; Allman-Farinelli, M. A mobile health intervention for weight management among young adults: A pilot randomised controlled trial. J. Hum. Nutr. Diet. 2013, 27, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, A.L.; Parasuraman, A.; Bowen, D.E.; Patricio, L.; Voss, C.A. Service Research Priorities in a Rapidly Changing Context. J. Serv. Res. 2015, 18, 127–159. [Google Scholar] [CrossRef]
- Dietrich, T.; Rundle-Thiele, S.; Schuster, L.; Connor, J. Co-designing social marketing programs. J. Soc. Mark. 2016, 6, 41–61. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, A.; Cosgrave, C.; Macdonald, J.; Gunn, K.; Dietrich, T.; Brumby, S. Translating Co-Design from Face-to-Face to Online: An Australian Primary Producer Project Conducted during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 4147. [Google Scholar] [CrossRef] [PubMed]
- Thabrew, H.; Fleming, T.; Hetrick, S.; Merry, S. Co-design of eHealth Interventions with Children and Young People. Front. Psychiatry 2018, 9, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babajanian, B. Promoting empowerment? The World Bank’s Village Investment Project in Kyrgyzstan. Cent. Asian Surv. 2015, 34, 1–17. [Google Scholar] [CrossRef]
- Narayanan, S.; Rajan, A.T.; Jebaraj, P.; Elayaraja, M. Delivering basic infrastructure services to the urban poor: A meta-analysis of the effectiveness of bottom-up approaches. Util. Policy 2017, 44, 50–62. [Google Scholar] [CrossRef]
- Ashton, L.M.; Morgan, P.J.; Hutchesson, M.J.; Rollo, M.E.; Collins, C.E. Feasibility and preliminary efficacy of the ‘HEYMAN’ healthy lifestyle program for young men: A pilot randomised controlled trial. Nutr. J. 2017, 16, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stead, M.; Arnott, L.; Dempsey, E. Healthy heroes, magic meals, and a visiting alien: Community-led assets-based social marketing. Soc. Mark. Q. 2013, 19, 26–39. [Google Scholar] [CrossRef]
- Ahmad, M.S.; Talib, N.B.A. Analysis of community empowerment on projects sustainability: Moderating role of sense of community. Soc. Indic. Res. 2016, 129, 1039–1056. [Google Scholar] [CrossRef]
- Andajani-Sutjahjo, S.; Liew, T.C.H.; Smith, J.F.; Esekielu, I.; Mason, G.; Tariu, I. Engaging community volunteers in participatory action research in Tāmaki community of Auckland, New Zealand. Health Promot. Int. 2016, 33, 219–228. [Google Scholar] [CrossRef]
- Blewitt, C.; Morris, H.; Jackson, K.; Barrett, H.; Bergmeier, H.; O’Connor, A.; Mousa, A.; Nolan, A.; Skouteris, H. Integrating Health and Educational Perspectives to Promote Preschoolers’ Social and Emotional Learning: Development of a Multi-Faceted Program Using an Intervention Mapping Approach. Int. J. Environ. Res. Public Health 2020, 17, 575. [Google Scholar] [CrossRef] [Green Version]
- Thorsen, A.V.; Lassen, A.D.; Tetens, I.; Hels, O.; E Mikkelsen, B. Long-term sustainability of a worksite canteen intervention of serving more fruit and vegetables. Public Health Nutr. 2010, 13, 1647–1652. [Google Scholar] [CrossRef]
- Hoyer, W.D.; Chandy, R.; Dorotic, M.; Krafft, M.; Singh, S.S. Consumer Cocreation in New Product Development. J. Serv. Res. 2010, 13, 283–296. [Google Scholar] [CrossRef]
- Buchanan, R. Wicked Problems in Design Thinking. Des. Issues 1992, 8, 5–21. [Google Scholar] [CrossRef]
- Sanders, E.B.-N.; Stappers, P.J. Co-creation and the new landscapes of design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Vallentin-Holbech, L.; Guldager, J.D.; Dietrich, T.; Rundle-Thiele, S.; Majgaard, G.; Lyk, P.; Stock, C. Co-Creating a Virtual Alcohol Prevention Simulation with Young People. Int. J. Environ. Res. Public Health 2020, 17, 1097. [Google Scholar] [CrossRef] [Green Version]
- Giacomin, J. What Is Human Centred Design? Des. J. 2014, 17, 606–623. [Google Scholar] [CrossRef] [Green Version]
- Kairy, D.; Mostafavi, M.A.; Blanchette-Dallaire, C.; Belanger, E.; Corbeil, A.; Kandiah, M.; Wu, T.Q.; Mazer, B. A Mobile App to Optimize Social Participation for Individuals with Physical Disabilities: Content Validation and Usability Testing. Int. J. Environ. Res. Public Health 2021, 18, 1753. [Google Scholar] [CrossRef]
- Spinuzzi, C. The methodology of participatory design. Tech. Commun. 2005, 52, 163–174. [Google Scholar]
- Saad-Sulonen, J.; Eriksson, E.; Halskov, K.; Karasti, H.; Vines, J. Unfolding participation over time: Temporal lenses in participatory design. CoDesign 2018, 14, 4–16. [Google Scholar] [CrossRef] [Green Version]
- Springer, M.V.; Skolarus, L.E. Community-Based Participatory Research. Stroke 2019, 50, 48–50. [Google Scholar] [CrossRef]
- Corrado, A.M.; Benjamin-Thomas, T.E.; McGrath, C.; Hand, C.; Rudman, D.L. Participatory Action Research With Older Adults: A Critical Interpretive Synthesis. Gerontol. 2019, 60, e413–e427. [Google Scholar] [CrossRef]
- Höltinger, S.; Salak, B.; Schauppenlehner, T.; Scherhaufer, P.; Schmidt, J. Austria’s wind energy potential – A participatory modeling approach to assess socio-political and market acceptance. Energy Policy 2016, 98, 49–61. [Google Scholar] [CrossRef]
- Borger, M.; van Hoof, A.; Sanders, J. Exploring participatory journalistic content: Objectivity and diversity in five examples of participatory journalism. Journalism 2016, 20, 444–466. [Google Scholar] [CrossRef] [Green Version]
- Heller, K.; Price, R.; Reinharz, S.; Riger, S.; Wandersman, A. Psychology and Community Change: Challenges of the Future; Brooks Cole Publishing Company: Pacific Grove, CA, USA, 1977. [Google Scholar]
- Schuler, D.; Namioka, A. Participatory Design: Principles and Practices; L. Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1993. [Google Scholar]
- Zhang, M.W.; Ying, J. Incorporating Participatory Action Research in Attention Bias Modification Interventions for Addictive Disorders: Perspectives. Int. J. Environ. Res. Public Health 2019, 16, 822. [Google Scholar] [CrossRef] [Green Version]
- Brookfield, K.; Scott, I.; Tinker, A.; Thompson, C.W. Perspectives on “Novel” Techniques for Designing Age-Friendly Homes and Neighborhoods with Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, C.; De Angeli, A. Applying user centred and participatory design approaches to commercial product development. Des. Stud. 2014, 35, 614–631. [Google Scholar] [CrossRef]
- Kandusová, V.; Vácha, T. Rethinking Public Buildings’ Functions: The Case for Participatory Design Methodology. IOP Conf. Ser. Earth Environ. Sci. 2019, 290, 012158. [Google Scholar] [CrossRef]
- Sharma, V.; Simpson, R.C.; Lopresti, E.F.; Mostowy, C.; Olson, J.; Puhlman, J.; Hayashi, S.; A Cooper, R.; Konarski, E.; Kerley, B. Participatory design in the development of the wheelchair convoy system. J. Neuroeng. Rehabil. 2008, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Sanders, E.B.-N.; Brandt, E.; Binder, T. A framework for organizing the tools and techniques of participatory design. In Proceedings of the 11th Biennial Participatory Design Conference on-PDC ’10, Sydney, Australia, 29 November–3 December 2010; Association for Computing Machinery: New York, NY, USA, 2010; pp. 195–198. [Google Scholar]
- Lindgaard, G.; Dillon, R.; Trbovich, P.; White, R.; Fernandes, G.; Lundahl, S.; Pinnamaneni, A. User Needs Analysis and requirements engineering: Theory and practice. Interact. Comput. 2006, 18, 47–70. [Google Scholar] [CrossRef]
- Muller, M.J. Participatory Design: The Third Space in Hci. In The Human-Computer Interaction Handbook; Informa UK Limited: London, UK, 2007; pp. 1087–1108. [Google Scholar]
- Akoglu, C.; Dankl, K. Co-creation for empathy and mutual learning: A framework for design in health and social care. CoDesign 2019, 1–17. [Google Scholar] [CrossRef]
- Kim, J.; Rundle-Thiele, S.; Knox, K.; Burke, K.; Bogomolova, S. Consumer perspectives on household food waste reduction campaigns. J. Clean. Prod. 2020, 243, 118608. [Google Scholar] [CrossRef]
- Ballantyne, D.; Varey, R.J. The service-dominant logic and the future of marketing. J. Acad. Mark. Sci. 2008, 36, 11–14. [Google Scholar] [CrossRef]
- Lusch, R.F.; Vargo, S.L. Service-dominant logic: Reactions, reflections and refinements. Mark. Theory 2006, 6, 281–288. [Google Scholar] [CrossRef]
- McColl-Kennedy, J.R.; Vargo, S.; Dagger, T.S.; Sweeney, J.; Van Kasteren, Y. Health Care Customer Value Cocreation Practice Styles. J. Serv. Res. 2012, 15, 370–389. [Google Scholar] [CrossRef]
- Waterman, A.S.; Schwartz, S.J.; Zamboanga, B.L.; Ravert, R.D.; Williams, M.K.; Agocha, V.B.; Kim, S.Y.; Donnellan, M.B. The Questionnaire for Eudaimonic Well-Being: Psychometric properties, demographic comparisons, and evidence of validity. J. Posit. Psychol. 2010, 5, 41–61. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.M.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Aadahl, M.; Jørgensen, T. Validation of a New Self-Report Instrument for Measuring Physical Activity. Med. Sci. Sports Exerc. 2003, 35, 1196–1202. [Google Scholar] [CrossRef]
- Räsänen, P.; Lappalainen, P.; Muotka, J.; Tolvanen, A.; Lappalainen, R. An online guided ACT intervention for enhancing the psychological wellbeing of university students: A randomized controlled clinical trial. Behav. Res. Ther. 2016, 78, 30–42. [Google Scholar] [CrossRef]
- Wong, Y.J.; Blackwell, N.M.; Mitts, N.G.; Gabana, N.T.; Li, Y. Giving thanks together: A preliminary evaluation of the Gratitude Group Program. Pract. Innov. 2017, 2, 243–257. [Google Scholar] [CrossRef]
- D’Raven, L.T.L.; Moliver, N.; Thompson, D. Happiness intervention decreases pain and depression, boosts happiness among primary care patients. Prim. Health Care Res. Dev. 2015, 16, 114–126. [Google Scholar] [CrossRef] [Green Version]
- Mak, W.W.; Chan, A.T.; Cheung, E.Y.; Lin, C.L.; Ngai, K.C.; Wong, S.Y.-S.; Kilpatrick, L.; Langrial, S. Enhancing Web-Based Mindfulness Training for Mental Health Promotion With the Health Action Process Approach: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e8. [Google Scholar] [CrossRef] [Green Version]
- Harvey-Berino, J.; Pope, L.; Gold, B.C.; Leonard, H.; Belliveau, C. Undergrad and Overweight: An Online Behavioral Weight Management Program for College Students. J. Nutr. Educ. Behav. 2012, 44, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Marcus, B.H.; Lewis, B.A.; Williams, D.; Dunsiger, S.; Jakicic, J.M.; Whiteley, J.A.; Albrecht, A.E.; Napolitano, M.A.; Bock, B.C.; Tate, D.F.; et al. A Comparison of Internet and Print-Based Physical Activity Interventions. Arch. Intern. Med. 2007, 167, 944–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweitzer, A.L.; Ross, J.T.; Klein, C.J.; Lei, K.Y.; Mackey, E.R.; Kapoukranidou, D.; Mouzakidis, C.; Merchant, G. An Electronic Wellness Program to Improve Diet and Exercise in College Students: A Pilot Study. JMIR Res. Protoc. 2016, 5, e29. [Google Scholar] [CrossRef] [PubMed]
- Howells, A.; Ivtzan, I.; Eiroa-Orosa, F.J. Putting the ‘app’ in Happiness: A Randomised Controlled Trial of a Smartphone-Based Mindfulness Intervention to Enhance Wellbeing. J. Happiness Stud. 2016, 17, 163–185. [Google Scholar] [CrossRef] [Green Version]
- Keeman, A.; Näswall, K.; Malinen, S.; Kuntz, J. Employee Wellbeing: Evaluating a Wellbeing Intervention in Two Settings. Front. Psychol. 2017, 8, 505. [Google Scholar] [CrossRef] [Green Version]
- Jerath, R.; Edry, J.W.; Barnes, V.A.; Jerath, V. Physiology of long pranayamic breathing: Neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Med. Hypotheses 2006, 67, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Kozasa, E.H.; Balardin, J.B.; Sato, J.R.; Chaim, K.T.; Lacerda, S.S.; Radvany, J.; Mello, L.E.A.M.; Amaro, E., Jr. Effects of a 7-Day Meditation Retreat on the Brain Function of Meditators and Non-Meditators During an Attention Task. Front. Hum. Neurosci. 2018, 12. [Google Scholar] [CrossRef] [PubMed]
- Howell, A.J.; Digdon, N.L.; Buro, K.; Sheptycki, A.R. Relations among mindfulness, well-being, and sleep. Pers. Individ. Differ. 2008, 45, 773–777. [Google Scholar] [CrossRef]
- Curry, O.S.; Rowland, L.A.; Van Lissa, C.J.; Zlotowitz, S.; McAlaney, J.; Whitehouse, H. Happy to help? A systematic review and meta-analysis of the effects of performing acts of kindness on the well-being of the actor. J. Exp. Soc. Psychol. 2018, 76, 320–329. [Google Scholar] [CrossRef]
- Bluethmann, S.M.; Bartholomew, L.K.; Murphy, C.C.; Vernon, S.W. Use of Theory in Behavior Change Interventions. Health Educ. Behav. 2017, 44, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willmott, M.T.; Pang, B.; Rundle-Thiele, P.S.; Badejo, A. Reported theory use in electronic health weight management interventions targeting young adults: A systematic review. Health Psychol. Rev. 2019, 13, 295–317. [Google Scholar] [CrossRef]
- Massey, S.H.; Decety, J.; Wisner, K.L.; Wakschlag, L.S. Specification of Change Mechanisms in Pregnant Smokers for Malleable Target Identification: A Novel Approach to a Tenacious Public Health Problem. Front. Public Health 2017, 5, 239. [Google Scholar] [CrossRef] [Green Version]
- Hurley, E.; Dietrich, T.; Rundle-Thiele, S. A systematic review of parent based programs to prevent or reduce alcohol consumption in adolescents. BMC Public Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465–474. [Google Scholar] [CrossRef]
- Newport, C. Digital Minimalism: On Living Better with Less Technology; Penguin UK: London, UK, 2019. [Google Scholar]
- Actions for Happiness. Our Vision for A Happier Society. Available online: https://www.actionforhappiness.org/about-us/our-vision (accessed on 2 May 2019).
- Beyhl, T.; Giese, H.; Plattner, H.; Meinel, C.; Leifer, L. The Design Thinking Methodology at Work: Capturing and Understanding the Interplay of Methods and Techniques. In Understanding Innovation; Springer Science: Berlin/Heidelberg, Germany, 2016; pp. 49–65. [Google Scholar]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Downe-Wamboldt, B. Content analysis: Method, applications, and issues. Health Care Women Int. 1992, 13, 313–321. [Google Scholar] [CrossRef]
- Ranjan, K.R.; Read, S. Value co-creation: Concept and measurement. J. Acad. Mark. Sci. 2016, 44, 290–315. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall PD Phases (Figure 1) | Spinuzzi’s Three-Step PD Process | Five-Step PD Process for eHealth Interventions | Rationale for a New PD Step |
|---|---|---|---|
| Phase 1: Gathering insights | 1. Initial exploration: explore workplace to assess current work processes. | 1. Collecting best practices: exploring best practice well-being activities through secondary research. | The objective of this study was to design a new eHealth intervention. Hence, insights could be collected beyond existing workplaces. This step was necessary to inform the second step. |
| 2. Discovery process: review existing work processes and envision a future workplace. | 2. Participatory discovery: elicit people’s preferences regarding well-being best practices and gain ideas for the design of a new intervention. | Given that the focus was on designing a new intervention, PD sessions (with 30 participants) could identify people’s preferences regarding effective well-being activities. | |
| Phase 2: Prototype development | 3. Prototyping: iteratively shaping artefacts | 3. Initial proof-of-concept: using people’s preferences to inform an initial proof-of-concept for PD sessions | Because we had utilised the first PD sessions as a means to elicit preferences and ideas for a prototype, we were able to use that information to suggest an initial proof-of-concept for the second round of PD sessions. |
| – | 4. Participatory prototyping: collecting feedback on proof-of-concept and the cocreation of new intervention designs according to people’s personal preferences | This extra step with two PD sessions was deemed necessary to ensure the emergence of a cocreated, user-friendly proof-of-concept. | |
| – | 5. Pilot intervention proof-of-concept finalisation: finalise an outcome proof-of-concept based on PD insights. | It is imperative to inform the intervention design on the basis of user preferences and their ideas; however, program designers must carefully gauge available resources (e.g., time and budget) in the development of the proof-of-concept that prevent the uptake of some ideas proposed by users. Therefore, an extra step was added to finalise the outcome proof-of-concept. |
| Campaign/Year/ Author/Organisation | Targeted Health Behaviour | Outcome/Evaluation |
|---|---|---|
| The Student Compass [66] | Journaling, relaxation exercises | After a 7-week intervention, participants showed significantly higher gains in well-being, life satisfaction, and mindfulness skills. In addition, iACT participants’ self-reported stress and symptoms of depression were significantly reduced |
| Gratitude Group Program [67] | Gratitude journaling | After a 5-week intervention, participants showed a significant and clinically meaningful decrease in psychological distress and increase in state gratitude, satisfaction with life, and meaning in life |
| Happiness 101 [68] | Mindfulness, gratitude, goal setting | After a 6-week intervention, scores improved from baseline to 6-month follow-up for health, vitality, mental health, and the effects of mental and physical health on daily activities. Improvements in mental and physical health and functioning were shown over a 6-month period |
| HEYMAN [29] | Nutrition, physical activity | After a 3-month intervention, significant effects were found for daily improving vegetable servings; energy-dense, nutrient-poor foods; weight; BMI; fat mass; waist circumference; and cholesterol |
| Internet-based mindfulness training program [69] | Mindfulness | Both the basic and HAPA-enhanced mindfulness groups showed better mental well-being from pre-intervention to post-intervention, and improvement was sustained at 3-month follow-up |
| Online behavioural weight management program for college students [70] | Nutrition, Physical activity | Overweight/obese students lost an average of 5.1 ± 6.0 lbs. Those of healthy weight lost an average of 1.8 ± 3.2 lbs. Twenty-three percent of students lost >5% of their baseline weight |
| Print- and Internet-Based Physical Activity (PA) Promotion Intervention [71] | Physical activity | At 6 months, the tailored internet arm reported 120 min of PA/week, and the tailored print arm 112.5 min of PA/week. At 12 months, the physical activity minutes per week were 90 for both interventions |
| An Electronic Wellness Program to Improve Diet and Exercise in College Students [72] | Nutrition, physical activity | Mean change from baseline of saturated fat intake was marginally significant between the treatment groups at week 24. A significant difference in percent of snacks chosen that were fruit was detected |
| RCT of a Smartphone-Based Mindfulness Intervention [73] | Mindfulness | Positive affect with a medium effect size and reduced depressive symptoms with a small effect size |
| The Well-being Game [74] | Journaling, physical activity | Students reported a significant positive change in well-being levels; employees reported lower stress levels and higher well-being levels |
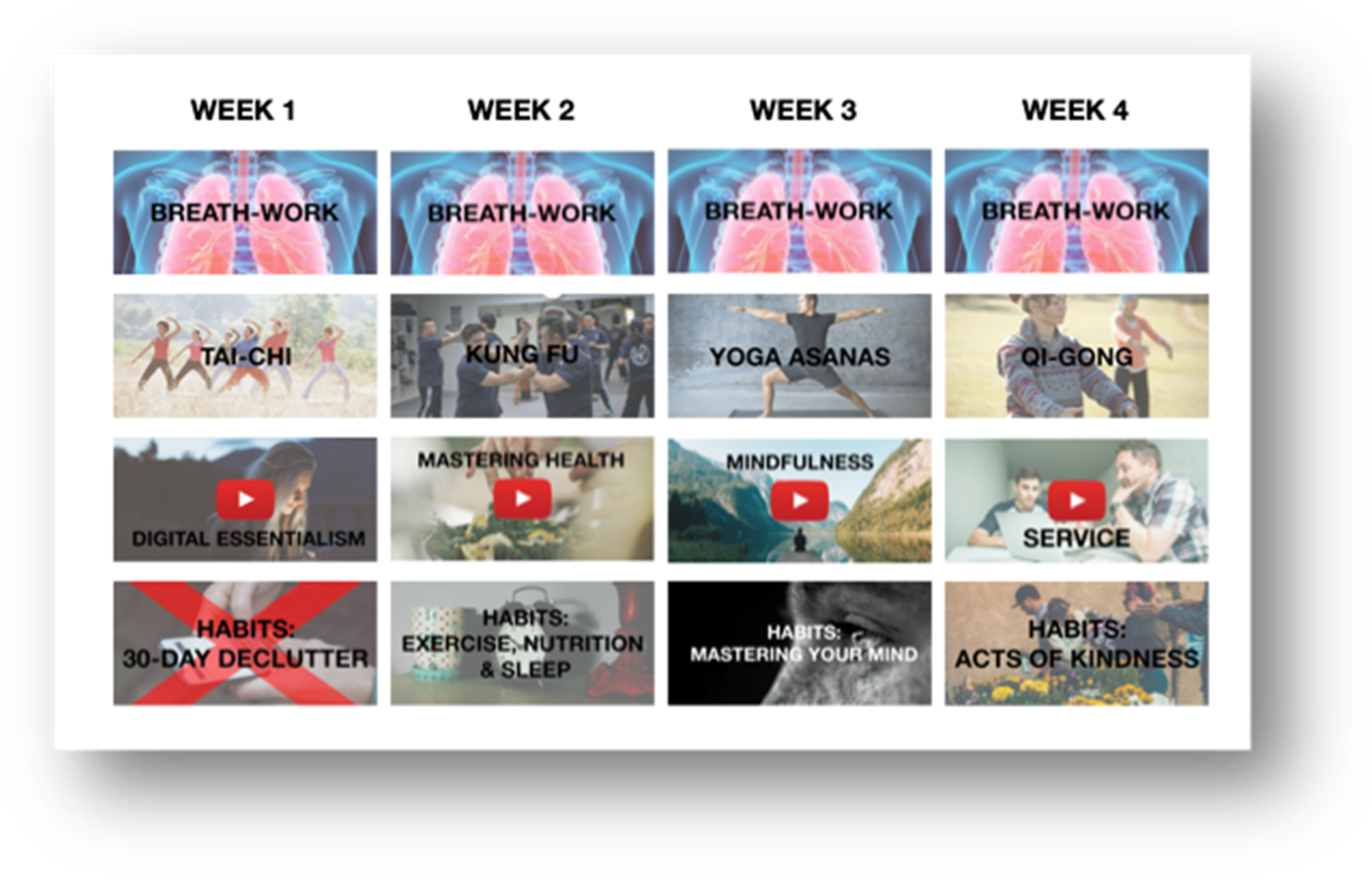
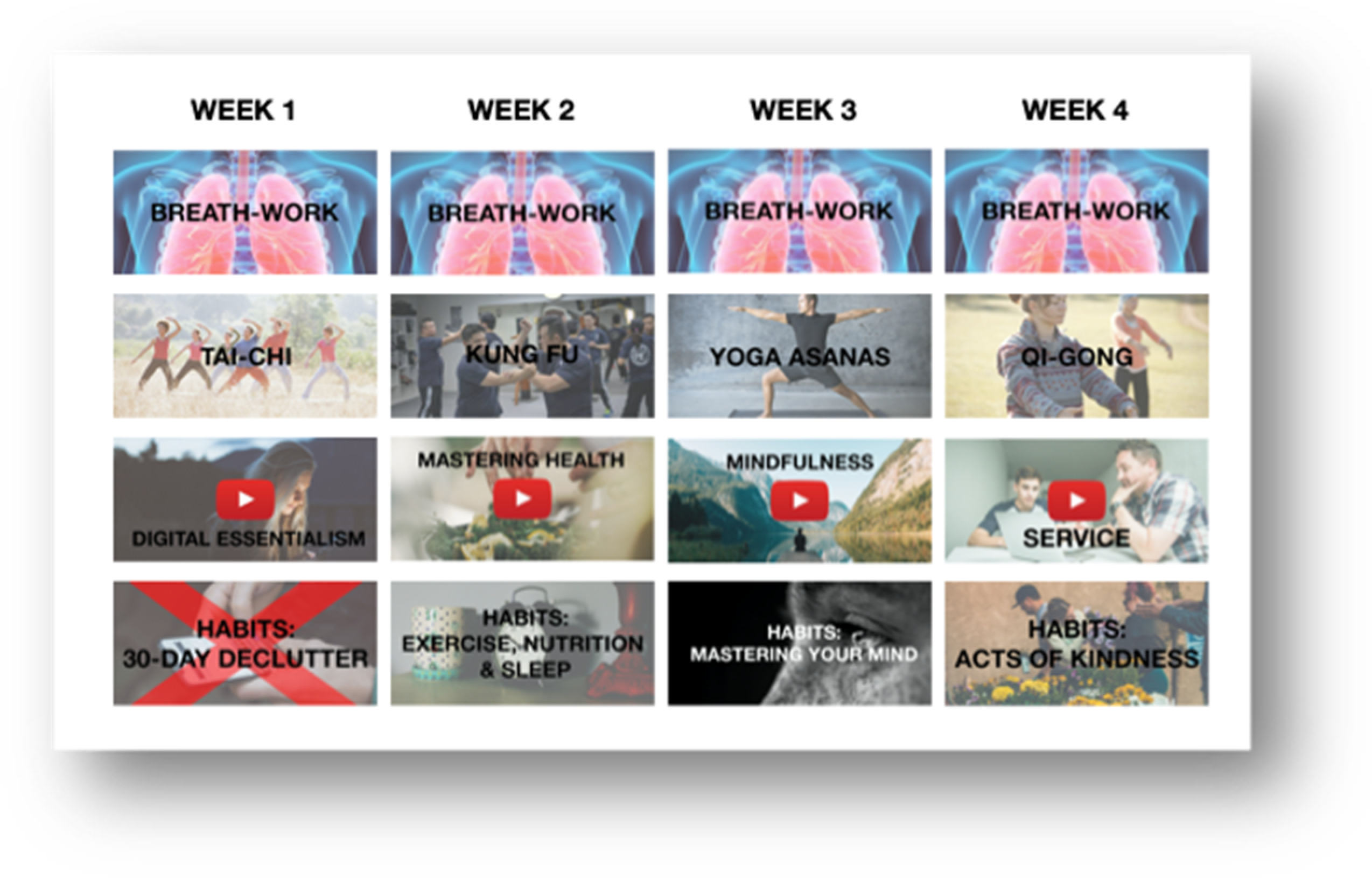
| Session 1 | Session 2 | |
|---|---|---|
| Part 1: Participation | Experiencing activities | Experiencing activities |
| Breathing exercises | 7 min breathing exercise | 7 min breathing exercise |
| Physical activity | 10 min physical activity routine | 10 min physical activity routine |
| Video viewing | Digital minimalism | Service |
| Action habits | Digital declutter | Acts of kindness, journaling |
| Part 2: Feedback capture | Feedback Capture Grid | Feedback Capture Grid |
| Part 3: Promotion campaign design | Campaign design | Campaign design |
| Session 3 and 4 | |
|---|---|
| Part 1: Questionnaire | 10 min questionnaire related to psychological well-being, mindfulness and resilience, and physical activity |
| Part 2: Breathing exercise | 7–10 min breathing exercise |
| Part 3: Feedback capture grid | Feedback capture grid based on presented design |
| Part 4: Program design | Individual design of most preferred program |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Hierden, Y.; Dietrich, T.; Rundle-Thiele, S. Designing an eHealth Well-Being Program: A Participatory Design Approach. Int. J. Environ. Res. Public Health 2021, 18, 7250. https://doi.org/10.3390/ijerph18147250
van Hierden Y, Dietrich T, Rundle-Thiele S. Designing an eHealth Well-Being Program: A Participatory Design Approach. International Journal of Environmental Research and Public Health. 2021; 18(14):7250. https://doi.org/10.3390/ijerph18147250
Chicago/Turabian Stylevan Hierden, Yannick, Timo Dietrich, and Sharyn Rundle-Thiele. 2021. "Designing an eHealth Well-Being Program: A Participatory Design Approach" International Journal of Environmental Research and Public Health 18, no. 14: 7250. https://doi.org/10.3390/ijerph18147250
APA Stylevan Hierden, Y., Dietrich, T., & Rundle-Thiele, S. (2021). Designing an eHealth Well-Being Program: A Participatory Design Approach. International Journal of Environmental Research and Public Health, 18(14), 7250. https://doi.org/10.3390/ijerph18147250