
Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. COVID-19 VL
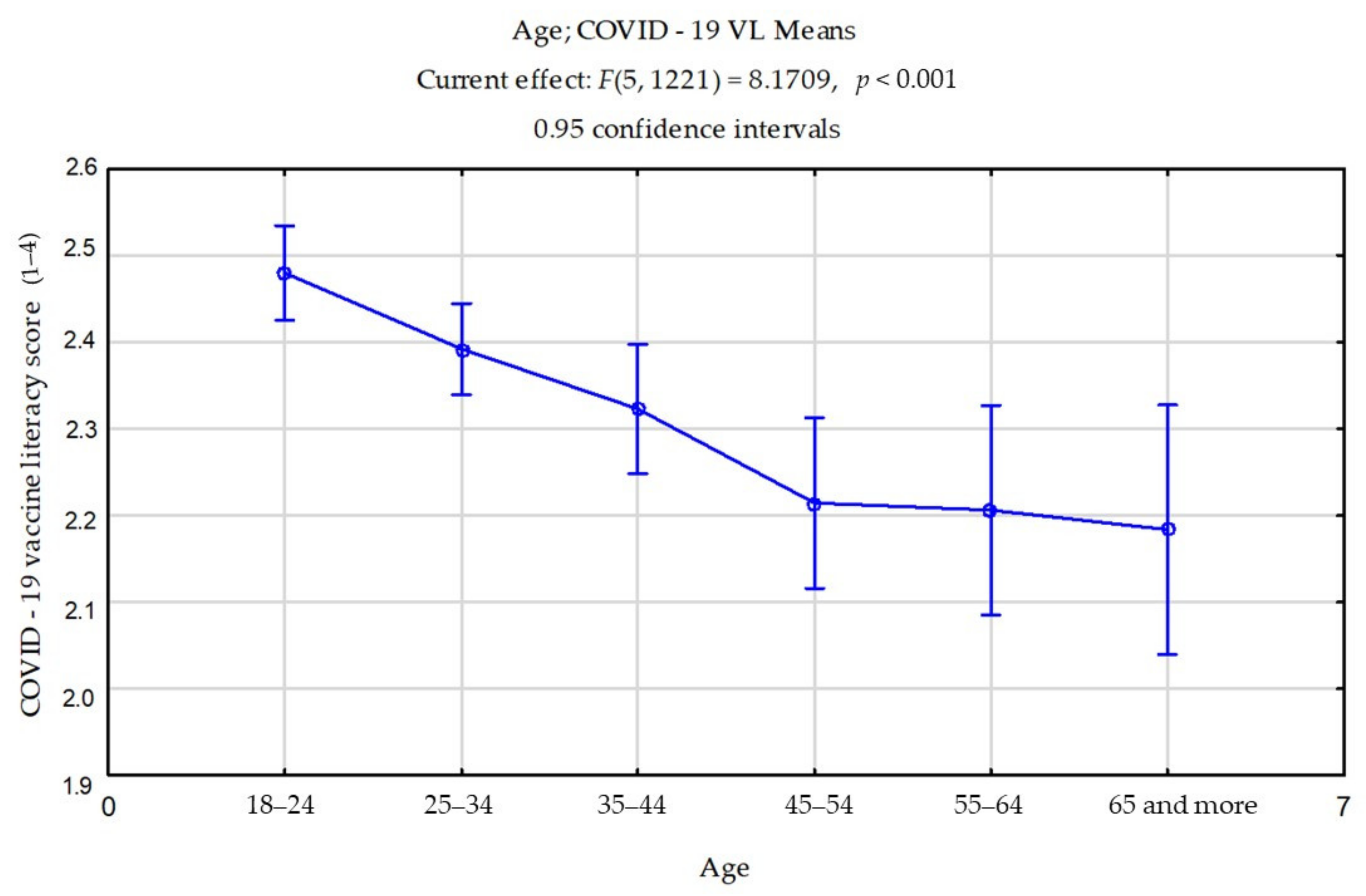
3.2. COVID-19 VL Considering Socio-Demographic Characteristics
3.3. Attitudes and Perceptions about Future COVID-19 Vaccines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCaffery, K.; Dodd, R.H.; Cvejic, E.; Ayre, J.; Batcup, C.; Isautier, J.M.J.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Disparities in COVID-19 related knowledge, attitudes, beliefs and behaviours by health literacy. Med. Rxiv. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Spring, H. Health literacy and COVID-19. Health Info. Libr. J. 2020, 37, 171–172. [Google Scholar] [CrossRef]
- Levin-Zamir, D. Communication, Health Literacy and a Systems Approach for Mitigating the COVID-19 Pandemic: The Case for Massive Vaccine Roll-out in Israel. J. Health Commun. 2020, 25, 816–818. [Google Scholar] [CrossRef]
- Official Government Website for Accurate and Verified Information on Coronavirus. Available online: https://www.koronavirus.hr/ (accessed on 15 March 2021).
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 1–8. [Google Scholar]
- Vanderpool, R.C.; Gaysynsky, A.; Chou, W.Y.S. Using a global pandemic as a teachable moment to promote vaccine literacy and build resilience to misinformation. Am. J. Public Health 2020, 110, 284–285. [Google Scholar] [CrossRef] [PubMed]
- Biasio, L.R. Vaccine literacy is undervalued. Hum. Vaccines Immunother. 2019, 15, 2552–2553. [Google Scholar] [CrossRef] [PubMed]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; van der Linden, S. Susceptibility to misinformation about COVID-19 around the world: Susceptibility to COVID misinformation. R. Soc. Open Sci. 2020, 7, 1–15. [Google Scholar] [CrossRef]
- Ashkenazi, S.; Livni, G.; Klein, A.; Kremer, N.; Havlin, A.; Berkowitz, O. The relationship between parental source of information and knowledge about measles/measles vaccine and vaccine hesitancy. Vaccine 2020, 38, 7292–7298. [Google Scholar] [CrossRef] [PubMed]
- Lazcano-Ponce, E.; Alpuche-Aranda, C. Public health literacy in the face of the COVID-19 pandemic emergency. Salud Publica Mex. 2020, 62, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Ratzan, S.C.; Parker, R.M.; Selden, C.R.; Zorn, M. National Library of Medicine Current Bibliographies in Medicine: Health Literacy; National Institutes of Health, US Department of Health and Human Services: Bethesda, MD, USA, 2000.
- Biasio, L.R.; Giambi, C.; Fadda, G.; Lorini, C.; Bonaccorsi, G.; D’Ancona, F. Validation of an Italian tool to assess vaccine literacy in adulthood vaccination: A pilot study. Ann. Ig. 2020, 32, 205–222. [Google Scholar] [CrossRef]
- Sorensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef]
- Bauer, A.; Tiefengraber, D.; Wiedermann, U. Towards Understanding Vaccine Hesitancy and Vaccination Refusal in Austria. Wien Klin Wochenschr. 2020. [Google Scholar] [CrossRef]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 478–488. [Google Scholar] [CrossRef]
- Regmi, P.R.; Waithaka, E.; Paudyal, A.; Simkhada, P.; van Teijlingen, E. Guide to the design and application of online questionnaire surveys. Nepal. J. Epidemiol. 2016, 6, 640–644. [Google Scholar] [CrossRef]
- Petersen, R.S.; Tennant, A.; Nakagawa, T.H.; Marziale, M.H.P. Translation, adaptation and validation of the nurse-work instability scale to brazilian Portuguese. Rev. Latino-Am. Enfermagem. 2019, 27, e3170. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Pozza, A.; Di Giuseppe, M.; Conversano, C. The psychosocial impact of COVID-19 pandemic in Italy: A lesson for mental health prevention in the first severely hit European country. Psychol. Trauma. 2020, 12, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Espanha, R.; Ávila, P. Health Literacy Survey Portugal: A Contribution for the Knowledge on Health and Communications. Procedia Comput. Sci. 2016, 100, 1033–1041. [Google Scholar] [CrossRef]
- Svendsen, I.W.; Damgaard, M.B.; Bak, C.K.; Bøggild, H.; Torp-Pedersen, C.; Svendsen, M.T.; Berg-Beckhoff, G. Employment Status and Health Literacy in Denmark: A Population-Based Study. Int. J. Public Health 2021, 66, 1–8. [Google Scholar] [CrossRef]
- Khoshravesh, S.; Moeini, B.; Rezapur-Shahkolai, F.; Taheri-Kharameh, Z.; Bandehelahi, K. Health Literacy of Employees of Hamadan University of Medical Sciences and Related Demographic Factors. J. Educ. Community Health 2018, 5, 19–26. [Google Scholar] [CrossRef][Green Version]
- Alharbi, B.A.; Masud, N.; Alajlan, F.A.; Alkhanein, N.I.; Alzahrani, F.T.; Almajed, Z.M.; Alessa, R.K.M.; Al-Farhan, A.I. Association of elderly age and chronic illnesses: Role of gender as a risk factor. J. Family Med. Prim. Care 2020, 9, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Lal, R.; Pattanayak, R. Alcohol use among the elderly: Issues and considerations. J. Geriatr. Ment. Health 2017, 4, 4–10. [Google Scholar] [CrossRef]
- Gao, L.; Maidment, I.; Matthews, F.E.; Robinson, L.; Brayne, C. Medication usage change in older people (65+) in England over 20 years: Findings from CFAS I and CFAS II. Age Ageing 2018, 47, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Aharon, A.A.; Nehama, H.; Rishpon, S.; Baron-Epel, O. Parents with high levels of communicative and critical health literacy are less likely to vaccinate their children. Patient Educ. Couns. 2017, 100, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Number (n) | Percentage (%) | |
|---|---|---|---|
| Gender | Males | 292 | 23.8 |
| Females | 935 | 76.2 | |
| Age | 18–24 | 374 | 30.5 |
| 25–34 | 406 | 33.1 | |
| 35–44 | 202 | 16.5 | |
| 45–54 | 115 | 9.4 | |
| 55–64 | 76 | 6.2 | |
| ≥65 | 54 | 4.4 | |
| Education | Elementary school | 30 | 2.4 |
| High school | 517 | 42.1 | |
| Undergraduate | 277 | 22.6 | |
| Graduate | 331 | 27 | |
| Master | 62 | 5.1 | |
| Doctorate | 10 | 0.8 | |
| Occupational status | Employed | 767 | 62.5 |
| Non-employed | 386 | 31.5 | |
| Retired | 74 | 6 | |
| I suffer from a chronic illness. | Yes | 227 | 18.5 |
| No | 1000 | 81.5 | |
| I use medication daily as recommended by my doctor. | Yes | 551 | 44.9 |
| No | 676 | 55.1 | |
| I consume tobacco products daily. | Yes | 387 | 31.5 |
| No | 840 | 68.5 | |
| I consume alcohol products daily. | Yes | 49 | 4 |
| No | 1178 | 96 | |
| I have been properly vaccinated so far. | Yes | 1128 | 91.9 |
| No | 99 | 8.1 | |
| I have had COVID-19. | Yes | 219 | 17.8 |
| No | 702 | 57.2 | |
| I do not know | 306 | 25 | |
| I have been in self-isolation. | Yes | 364 | 29.7 |
| No | 794 | 64.7 | |
| Yes, multiple times | 69 | 5.6 |
| Items | Factor 1 | Factor 2 |
|---|---|---|
| 1 | 0.142463 | −0.829147 |
| 2 | 0.118460 | −0.879581 |
| 3 | 0.168398 | −0.853559 |
| 4 | 0.134923 | −0.813179 |
| 5 | −0.650464 | −0.224153 |
| 6 | −0.686086 | 0.031209 |
| 7 | −0.689637 | −0.028863 |
| 8 | −0.667444 | −0.145471 |
| 9 | −0.777003 | −0.142782 |
| 10 | −0.840424 | −0.063800 |
| 11 | −0.830299 | −0.065123 |
| 12 | −0.765684 | −0.020569 |
| Age | n (%) | Functional Mean Score * (SD) | p ** | Interactive-Critical Mean Score * (SD) | p ** | Vaccine Literacy Total Score * | p ** |
|---|---|---|---|---|---|---|---|
| 18–24 | 374 (30.5) | 2.95 (0.69) | 2.24 (0.78) | 2.47 (0.57) | |||
| 25–34 | 406 (33.1) | 2.98 (0.68) | 2.09 (0.78) | 2.39 (0.54) | |||
| 35–44 | 202 (16.5) | 2.77 (0.70) | <0.001 | 2.09 (0.69) | <0.001 | 2.32 (0.51) | <0.001 |
| 45–54 | 115 (9.4) | 2.74 (0.51) | 1.95 (0.61) | 2.21 (0.46) | |||
| 55–64 | 76 (6.2) | 2.69 (0.69) | 1.96 (0.68) | 2.20 (0.49) | |||
| ≥65 | 54 (4.4) | 2.21 (0.77) | 2.16 (0.78) | 2.18 (0.54) |
| Variable | VL Functional Score | VL Interactive-Critical Score | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| A * | Mean (SD) | t | df | p * | A* | Mean (SD) | t | df | p ** | |
| Will it be possible to produce safe and efficacious vaccines? | Yes | 2.86 (0.71) | 63.25 | 2452 | <0.01 | Yes | 2.12 (0.75) | 31.40 | 2452 | <0.01 |
| No | 1.32 (0.46) | No | 1.32 (0.46) | |||||||
| Will you get vaccinated, if possible? | Yes | 2.86 (0.71) | 53.67 | 2452 | <0.01 | Yes | 2.12 (0.75) | 22.82 | 2452 | <0.01 |
| No | 1.53 (0.49) | No | 1.53 (0.49) | |||||||
| Will authorities succeed in vaccinating the entire population? | Yes | 2.86 (0.71) | 44.83 | 2452 | <0.01 | Yes | 2.12 (0.75) | 11.82 | 2452 | <0.01 |
| No | 1.83 (0.36) | No | 1.83 (0.36) | |||||||
| Would you pay a fee to be vaccinated? | Yes | 2.86 (0.71) | 47.01 | 2452 | <0.01 | Yes | 2.12 (0.75) | 15.21 | 2452 | <0.01 |
| No | 1.74 (0.43) | No | 1.74 (0.43) | |||||||
| Should children be vaccinated too? | Yes | 2.86 (0.71) | 46.74 | 2452 | <0.01 | Yes | 2.12 (0.75) | 14.83 | 2452 | <0.01 |
| No | 1.75 (0.43) | No | 1.75 (0.43) | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gusar, I.; Konjevoda, S.; Babić, G.; Hnatešen, D.; Čebohin, M.; Orlandini, R.; Dželalija, B. Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7073. https://doi.org/10.3390/ijerph18137073
Gusar I, Konjevoda S, Babić G, Hnatešen D, Čebohin M, Orlandini R, Dželalija B. Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(13):7073. https://doi.org/10.3390/ijerph18137073
Chicago/Turabian StyleGusar, Ivana, Suzana Konjevoda, Grozdana Babić, Dijana Hnatešen, Maja Čebohin, Rahela Orlandini, and Boris Dželalija. 2021. "Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 13: 7073. https://doi.org/10.3390/ijerph18137073
APA StyleGusar, I., Konjevoda, S., Babić, G., Hnatešen, D., Čebohin, M., Orlandini, R., & Dželalija, B. (2021). Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(13), 7073. https://doi.org/10.3390/ijerph18137073