
Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Antibody Testing
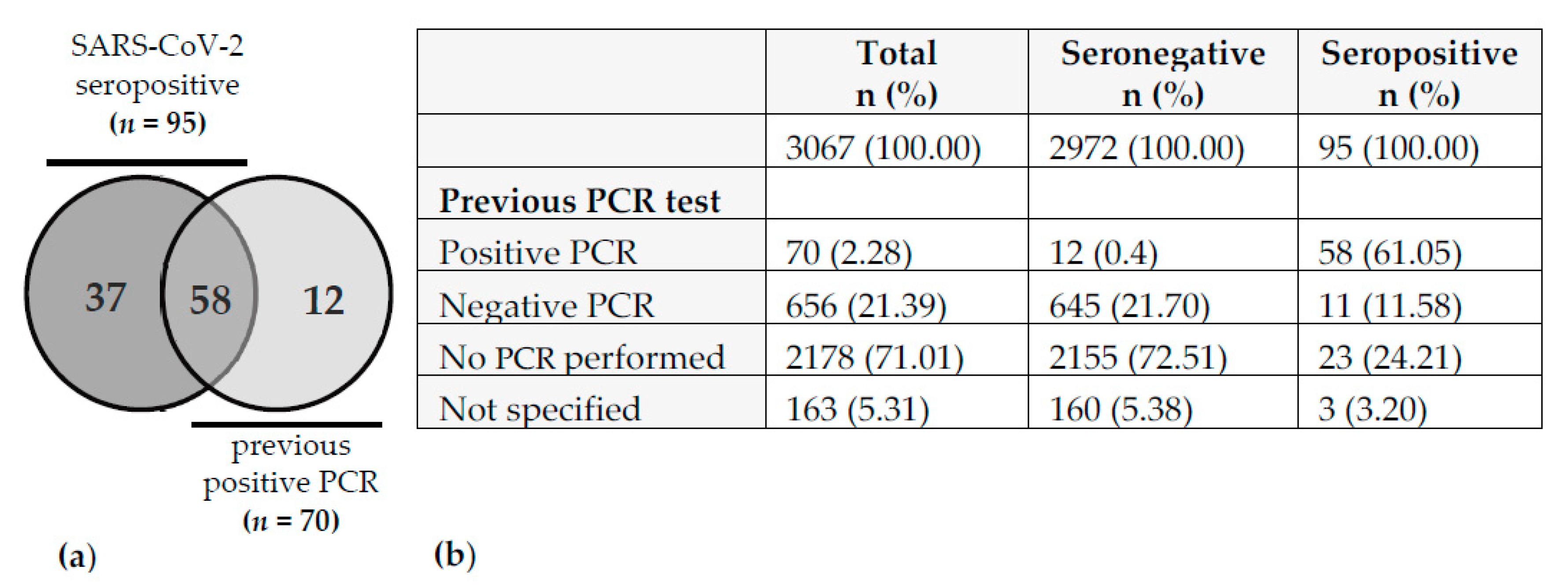
2.3. Definition of SARS-CoV-2 History
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. Available online: https://covid19.who.int/ (accessed on 28 June 2021).
- RKI Coronavirus Disease 2019 (COVID-19) Daily Situation Report from the Robert Koch Institute. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Mai_2021/2021-05-15-de.pdf?__blob=publicationFile (accessed on 28 June 2021).
- Dalewski, B.; Palka, L.; Kiczmer, P.; Sobolewska, E. The impact of SARS-CoV-2 outbreak on the Polish dental community’s standards of care—A six-month retrospective survey-based study. Int. J. Environ. Res. Public Health 2021, 18, 1281. [Google Scholar] [CrossRef]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in health care workers during the covid-19 epidemic. A cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef]
- Croghan, I.T.; Chesak, S.S.; Adusumalli, J.; Fischer, K.M.; Beck, E.W.; Patel, S.R.; Ghosh, K.; Schroeder, D.R.; Bhagra, A. Stress, Resilience, and Coping of Healthcare Workers during the COVID-19 Pandemic. J. Prim. Care Community Health 2021, 12, 21501327211008448. [Google Scholar] [CrossRef]
- Weissman, D.N.; De Perio, M.A.; Radonovich, L.J. COVID-19 and Risks Posed to Personnel during Endotracheal Intubation. JAMA J. Am. Med. Assoc. 2020, 323, 2027–2028. [Google Scholar] [CrossRef]
- Laursen, J.; Petersen, J.; Didriksen, M.; Iversen, K.; Ullum, H. Prevalence of SARS-CoV-2 igg/igm antibodies among danish and swedish falck emergency and non-emergency healthcare workers. Int. J. Environ. Res. Public Health 2021, 18, 923. [Google Scholar] [CrossRef]
- Weinberger, T.; Steffen, J.; Osterman, A. Prospective Longitudinal Serosurvey of Health Care Workers in the First Wave of the SARS-CoV-2 Pandemic in a Quaternary Care Hospital in Munich, Germany. Clin. Infect Dis. 2021, 26, 1–15. [Google Scholar]
- WHO. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. Available online: https://www.who.int/news/item/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 28 June 2021).
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; d’Aloja, E. COVID-19 and Italian Healthcare Workers From the Initial Sacrifice to the mRNA Vaccine: Pandemic Chrono-History, Epidemiological Data, Ethical Dilemmas, and Future Challenges. Front. Public Health 2021, 8, 591900. [Google Scholar] [CrossRef]
- Grant, J.; Wilmore, S.; McCann, N.; Donnelly, O.; Lai, R.; Kinsella, M.; Rochford, H.; Patel, T.; Kelsey, M.; Andrews, J. Seroprevalence of SARS-CoV-2 antibodies in healthcare workers at a London NHS Trust. Infect. Control Hosp. Epidemiol. 2020, 1–3. [Google Scholar] [CrossRef]
- Brant-Zawadzki, M.; Fridman, D.; Robinson, P.A.; Zahn, M.; Chau, C.; German, R.; Breit, M.; Bock, J.R.; Hara, J. SARS-CoV-2 antibody prevalence in health care workers: Preliminary report of a single center study. PLoS ONE 2020, 15, 6–11. [Google Scholar] [CrossRef]
- Hunter, B.R.; Dbeibo, L.; Weaver, C.S.; Beeler, C.; Saysana, M.; Zimmerman, M.K.; Weaver, L. Seroprevalence of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) antibodies among healthcare workers with differing levels of coronavirus disease 2019 (COVID-19) patient exposure. Infect. Control Hosp. Epidemiol. 2020, 41, 1441–1442. [Google Scholar] [CrossRef] [PubMed]
- RKI COVID-19 Germany Dashboard. Available online: https://experience.arcgis.com/experience/478220a4c454480e823b17327b2bf1d4 (accessed on 28 June 2021).
- The PostgreSQL Global Development Group. PostgreSQL: The World’s Most Advanced Open Source Relational Database. Available online: https://www.postgresql.org/ (accessed on 28 June 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 28 June 2021).
- McKelvey, R.D.; Zavoina, W. A statistical model for the analysis of ordinal level dependent variables. J. Math. Sociol. 1975, 4, 103–120. [Google Scholar] [CrossRef]
- Signorell, A.; Aho, K.; Alfons, A.; Anderegg, N.; Aragon, T.; Arachchige, C.; Arppe, A.; Baddeley, A.; Barton, K.; Bolker, B.; et al. DescTools: Tools for Descriptive Statistics. 2021. Available online: https://CRAN.R-project.org/package=DescTools (accessed on 28 June 2021).
- Tönshoff, B.; Müller, B.; Elling, R.; Renk, H.; Meissner, P.; Hengel, H.; Garbade, S.F.; Kieser, M.; Jeltsch, K.; Grulich-Henn, J.; et al. Prevalence of SARS-CoV-2 Infection in Children and Their Parents in Southwest Germany. JAMA Pediatr. 2021. [Google Scholar] [CrossRef]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.K.; Sahly, H.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Prospective Sero-epidemiological Evaluation of SARS-CoV-2 among Health Care Workers in a German Secondary Care Hospital. Int. J. Infect. Dis. 2021, 102, 136–143. [Google Scholar] [CrossRef]
- Schmidt, S.B.; Grüter, L.; Boltzmann, M.; Rollnik, J.D. Prevalence of serum igg antibodies against sars-cov-2 among clinic staff. PLoS ONE 2020, 15, 4–11. [Google Scholar] [CrossRef]
- Behrens, G.M.N.; Cossmann, A.; Stankov, M.V.; Witte, T.; Ernst, D.; Happle, C.; Jablonka, A. Perceived versus proven SARS-CoV-2-specific immune responses in health-care professionals. Infection 2020, 48, 631–634. [Google Scholar] [CrossRef]
- Müller, K.; Girl, P.; Ruhnke, M.; Spranger, M.; Kaier, K.; von Buttlar, H.; Dobler, G.; Borde, J.P. Sars-cov-2 seroprevalence among health care workers—a voluntary screening study in a regional medical center in southern germany. Int. J. Environ. Res. Public Health 2021, 18, 3910. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Frisch, J.; Jahn, M.; Krawczyk, A.; Trilling, M.; Schipper, L.; Cordes, S.; Ross, B.; et al. SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 4540. [Google Scholar] [CrossRef]
- Santos-Hövener, C.; Neuhauser, H.K.; Rosario, A.S.; Busch, M.; Schlaud, M.; Hoffmann, R.; Gößwald, A.; Koschollek, C.; Hoebel, J.; Allen, J.; et al. Serology- And PCR-based cumulative incidence of SARS-cov-2 infection in adults in a successfully contained early hotspot (CoMoLo study), Germany, May to June 2020. Eurosurveillance 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Tesoriero, J.M.; Rosenthal, E.M.; Chung, R.; Barranco, M.A.; Styer, L.M.; Parker, M.M.; Leung, S.J.; Morne, J.E.; Greene, D.; et al. Cumulative incidence and diagnosis of SARS-CoV-2 infection in New York. Ann. Epidemiol. 2020, 48, 23–29. [Google Scholar] [CrossRef]
- De Donno, A.; Lobreglio, G.; Panico, A.; Grassi, T.; Bagordo, F.; Bozzetti, M.P.; Massari, S.; Siculella, L.; Damiano, F.; Guerra, F.; et al. Igm and igg profiles reveal peculiar features of humoral immunity response to sars-cov-2 infection. Int. J. Environ. Res. Public Health 2021, 18, 1318. [Google Scholar] [CrossRef]
- Ainsworth, M.; Andersson, M.; Auckland, K.; Baillie, J.K.; Barnes, E.; Beer, S.; Beveridge, A.; Bibi, S.; Blackwell, L.; Borak, M.; et al. Performance characteristics of five immunoassays for SARS-CoV-2: A head-to-head benchmark comparison. Lancet Infect. Dis. 2020, 20, 1390–1400. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild Covid-19. N. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Stubblefield, W.B.; Feldstein, L.R.; Steingrub, J.S.; Shapiro, N.I.; Ginde, A.A.; Prekker, M.E.; Brown, S.M.; Peltan, I.D.; et al. Decline in SARS-CoV-2 Antibodies After Mild Infection Among Frontline Health Care Personnel in a Multistate Hospital Network—12 States, April–August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1762–1766. [Google Scholar] [CrossRef]
- Heidt, A. Studies Report Rapid Loss of COVID-19 Antibodies|The Scientist Magazine. Available online: https://www.the-scientist.com/news-opinion/studies-report-rapid-loss-of-covid-19-antibodies-67650 (accessed on 28 June 2021).
- Röltgen, K.; Powell, A.E.; Wirz, O.F.; Stevens, B.A.; Hogan, C.A.; Najeeb, J.; Hunter, M.; Wang, H.; Sahoo, M.K.; Huang, C.H.; et al. Defining the features and duration of antibody responses to SARS-CoV-2 infection associated with disease severity and outcome. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Aqel, F. Antibodies, Immunity Low after COVID-19 Recovery. Available online: https://www.dw.com/en/coronavirus-antibodies-immunity/a-54159332 (accessed on 28 June 2021).
- Steensels, D.; Oris, E.; Coninx, L.; Nuyens, D.; Delforge, M.L.; Vermeersch, P.; Heylen, L. Hospital-Wide SARS-CoV-2 Antibody Screening in 3056 Staff in a Tertiary Center in Belgium. J. Am. Med. Assoc. 2020, 324, 195–197. [Google Scholar] [CrossRef]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jiménez, A.; Santano, R.; Sanz, S.; Méndez, S.; Llupià, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef]
- Venugopal, U.; Jilani, N.; Rabah, S.; Shariff, M.A.; Jawed, M.; Batres, A.M.; Abubacker, M.; Menon, S.; Pillai, A.; Shabarek, N.; et al. SARS-CoV-2 seroprevalence among health care workers in a New York City hospital: A cross-sectional analysis during the COVID-19 pandemic. Int. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Shields, A.; Faustini, S.E.; Perez-Toledo, M.; Jossi, S.; Aldera, E.; Allen, J.D.; Al-Taei, S.; Backhouse, C.; Bosworth, A.; Dunbar, L.A.; et al. SARS-CoV-2 seroprevalence and asymptomatic viral carriage in healthcare workers: A cross-sectional study. Thorax 2020, 75, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Marcella Vaselli, N.; Hungerford ORCID, D.; Shenton, B.; Khashkhusha, A.; Cunliffe, N.A.; French, N. The Seroprevalence of SARS-CoV-2 in Europe: A Systematic Review. bioRxiv 2021. [Google Scholar] [CrossRef]
- Braun, K.M.; Moreno, G.K.; Buys, A.; Somsen, E.D.; Bobholz, M.; Accola, M.A.; Anderson, L.; Rehrauer, W.M.; Baker, D.A.; Safdar, N.; et al. Viral sequencing reveals US healthcare personnel rarely become infected with SARS-CoV-2 through patient contact. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Streeck, H.; Schulte, B.; Kümmerer, B.M.; Richter, E.; Höller, T.; Fuhrmann, C.; Bartok, E.; Dolscheid, R.; Berger, M.; Wessendorf, L.; et al. Infection fatality rate of SARS-CoV-2 infection in a German community with a super-spreading event. medRxiv 2020. [Google Scholar] [CrossRef]
- Madewell, Z.J.; Yang, Y.; Longini, I.M.; Halloran, M.E.; Dean, N.E. Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2031756. [Google Scholar] [CrossRef]
- Çelebi, G.; Pişkin, N.; Çelik Bekleviç, A.; Altunay, Y.; Salcı Keleş, A.; Tüz, M.A.; Altınsoy, B.; Hacıseyitoğlu, D. Specific risk factors for SARS-CoV-2 transmission among health care workers in a university hospital. Am. J. Infect. Control 2020, 48, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.C.; Pau, S.; Salinas, A.B.; Oladapo-Shittu, O.; Cosgrove, S.E.; Lewis-Cherry, R.; Vecchio-Pagan, B.; Osei, P.; Gurses, A.P.; Rock, C.; et al. Barriers to physical distancing among healthcare workers on an academic hospital unit during the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2021, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Piening, B.; Nouri-Pasovsky, P.A.; Krüger, A.C.; Gastmeier, P.; Aghdassi, S.J.S. SARS-Coronavirus-2 cases in healthcare workers may not regularly originate from patient care: Lessons from a university hospital on the underestimated risk of healthcare worker to healthcare worker transmission. Antimicrob. Resist. Infect. Control 2020, 9. [Google Scholar] [CrossRef]
- Napolitano, F.; Di Giuseppe, G.; Montemurro, M.V.; Molinari, A.M.; Donnarumma, G.; Arnese, A.; Pavia, M.; Angelillo, I.F. Seroprevalence of SARS-CoV-2 Antibodies in Adults and Healthcare Workers in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 4761. [Google Scholar] [CrossRef]
- Haehner, A.; Draf, J.; Dräger, S.; De With, K.; Hummel, T. Predictive Value of Sudden Olfactory Loss in the Diagnosis of COVID-19. ORL 2020, 82, 175–180. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Marinosci, A.; Landis, B.N.; Calmy, A. Possible link between anosmia and COVID-19: Sniffing out the truth. Eur. Arch. Oto-Rhino-Laryngology 2020, 277, 2149–2150. [Google Scholar] [CrossRef] [PubMed]
- Schmithausen, R.M.; Döhla, M.; Schößler, H.; Diegmann, C.; Schulte, B.; Richter, E.; Eis-Hübinger, A.M.; Streeck, H. Characteristic temporary loss of taste and olfactory senses in SARS-CoV-2-positive-individuals with mild symptoms. Pathog. Immun. 2020, 5, 117–120. [Google Scholar] [CrossRef] [PubMed]
- de Haro-Licer, J.; Roura-Moreno, J.; Vizitiu, A.; González-Fernández, A.; González-Ares, J.A. Long Term Serious Olfactory Loss in Colds and/or Flu. Available online: https://pubmed.ncbi.nlm.nih.gov/23948436/ (accessed on 28 June 2021).
- Potter, M.R.; Chen, J.H.; Lobban, N.S.; Doty, R.L. Olfactory dysfunction from acute upper respiratory infections: Relationship to season of onset. Int. Forum Allergy Rhinol. 2020, 10, 706–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Negative n (%) # | Positive n (%) # | OR [95% CI] | p-Value | SC | |
|---|---|---|---|---|---|
| Age | |||||
| 14–19 (Ref. Group) | 48 (1.6) | 1 (0.9) | |||
| 20–29 | 515 (17.4) | 19 (17.8) | 1.87 [0.36;34.29] | 0.55090 | |
| 30–39 | 660 (22.3) | 27 (25.2) | 2.12 [0.42;38.77] | 0.47152 | |
| 40–49 | 627 (21.2) | 21 (19.6) | 1.81 [0.36;33.20] | 0.56863 | |
| 50–59 | 830 (28.1) | 32 (29.9) | 2.26 [0.45;41.07] | 0.43346 | |
| ≥60 | 279 (9.4) | 7 (6.5) | 1.38 [0.23;26.47] | 0.76833 | |
| Gender | |||||
| Female (Ref. Group) | 2377 (80.3) | 76 (71.0) | |||
| Male | 562 (19.0) | 31 (29.0) | 1.77 [1.05;2.92] | 0.02735 | * |
| Not specified | 20 (0.7) | - | 0.00 [-] | 0.99133 | |
| Working from Home | |||||
| No (Ref. Group) | 2753 (93.0) | 95 (88.8) | |||
| Yes | 168 (5.7) | 9 (8.4) | 1.67 [0.75;3.29] | 0.16849 | |
| Not specified | 38 (1.3) | 3 (2.8) | 2.86 [0.65;8.77] | 0.10124 | |
| In-house Mobility | |||||
| <10% (Ref. Group) | 1297 (43.8) | 48 (44.9) | |||
| 10–50% | 294 (9.9) | 4 (3.7) | 0.73 [0.44;1.20] | 0.22103 | |
| >50% | 1958 (66.2) | 82 (76.6) | 1.00 [0.59;1.65] | 0.98574 | |
| Not specified | 40 (1.4) | - | 1.57 [0.24;5.69] | 0.55710 | |
| Patient Contact | |||||
| <10% (Ref. Group) | 667 (22.5) | 21 (19.6) | |||
| 10–50% | 294 (9.9) | 4 (3.7) | 0.37 [0.10;1.11] | 0.10087 | |
| >50% | 1958 (66.2) | 82 (76.6) | 1.08 [0.47;2.65] | 0.85662 | |
| Not specified | 40 (1.4) | - | 0.00 [-] | 0.98755 | |
| Work Area | |||||
| Physicians (Ref. Group) | 445 (15.0) | 17 (15.9) | |||
| Administration, patient management, reception | 356 (12.0) | 10 (9.3) | 0.81 [0.27;2.38] | 0.69788 | |
| Housekeeping and transport services | 186 (6.3) | 1 (0.9) | 0.17 [0.01;0.90] | 0.09369 | |
| IT and technical services | 73 (2.5) | 9 (8.4) | 3.10 [0.98;9.68] | 0.05174 | |
| Laboratory, pathology and pharmacy staff | 111 (3.8) | - | 0.00 [-] | 0.98017 | |
| Nursing staff, medical assistance and non-medical therapists | 1629 (55.1) | 69 (64.5) | 1.35 [0.74;2.57] | 0.33705 | |
| Others/not specified | 159 (5.4) | 1 (0.9) | 0.21 [0.01;1.16] | 0.14371 | |
| Contact COVID-19 Patients | |||||
| No (Ref. Group) | 1818 (61.4) | 67 (62.6) | |||
| Yes, COVID-19 suspect ward | 260 (8.8) | 12 (11.2) | 1.08 [0.54;2.00] | 0.80862 | |
| Yes, combinations of COVID-19 wards and ER | 353 (11.9) | 11 (10.3) | 0.66 [0.32;1.26] | 0.23625 | |
| Yes, COVID-19 ICU | 215 (7.3) | 5 (4.7) | 0.46 [0.16;1.08] | 0.10652 | |
| Yes, COVID-19 ward | 102 (3.4) | 2 (1.9) | 0.47 [0.08;1.55] | 0.29777 | |
| Yes, ER | 165 (5.6) | 10 (9.3) | 1.38 [0.64;2.73] | 0.37505 | |
| Not specified | 46 (1.6) | - | 0.00 [-] | 0.98642 | |
| Negative n (%) | Positive n (%) | OR [95% CI] | p-Value | SC | |
|---|---|---|---|---|---|
| Headache (Ref.Group) | 1298 (43.9) | 65 (60.7) | |||
| Fever ≥ 38 °C | 338 (11.4) | 51 (47.7) | 3.01 [2.04; 4.42] | 0.00000 | *** |
| Impairment of taste/smell | 100 (3.4) | 56 (52.3) | 11.18 [7.41; 16.89] | 0.00000 | *** |
| Congested/running nose | 1161 (39.2) | 51 (47.7) | 0.88 [0.60; 1.27] | 0.49358 | |
| Cough | 958 (32.4) | 52 (48.6) | 1.08 [0.74; 1.57] | 0.67286 | |
| Sore throat/hoarseness | 1204 (40.7) | 47 (43.9) | 0.78 [0.53; 1.14] | 0.20292 | |
| Shortness of breath | 296 (10.0) | 35 (32.7) | 2.36 [1.52; 3.61] | 0.00009 | *** |
| Respiratory distress | 88 (3.0) | 11 (10.3) | 2.50 [1.21; 4.72] | 0.00786 | ** |
| Abnormal sleepiness/drowsiness | 64 (2.2) | 10 (9.3) | 3.12 [1.45; 6.11] | 0.00172 | ** |
| Apathy | 31 (1.0) | 11 (10.3) | 7.09 [3.28; 14.35] | 0.00000 | *** |
| Loss of appetite | 130 (4.4) | 27 (25.2) | 4.15 [2.52; 6.66] | 0.00000 | *** |
| Weight loss | 53 (1.8) | 13 (12.1) | 4.90 [2.45; 9.20] | 0.00000 | *** |
| Stomach pain | 291 (9.8) | 6 (5.6) | 0.41 [0.16; 0.88] | 0.03977 | * |
| Diarrhea | 453 (15.3) | 19 (17.8) | 0.84 [0.48; 1.38] | 0.50587 | |
| Nausea/vomit | 230 (7.8) | 11 (10.3) | 0.96 [0.47; 1.76] | 0.89041 | |
| Joint pain | 508 (17.2) | 37 (34.6) | 1.45 [0.95; 2.19] | 0.07789 | |
| Muscle pain | 459 (15.5) | 40 (37.4) | 1.74 [1.15; 2.61] | 0.00778 | ** |
| Swollen lymph nodes | 135 (4.6) | 6 (5.6) | 0.89 [0.34; 1.93] | 0.78441 | |
| Conjunctivitis | 76 (2.6) | 7 (6.5) | 1.84 [0.75; 3.89] | 0.14194 | |
| Skin rash | 106 (3.6) | 7 (6.5) | 1.32 [0.54; 2.76] | 0.50025 | |
| Malaise/weakness | 634 (21.4) | 61 (57.0) | 1.92 [1.34; 2.76] | 0.00041 | *** |
| Other symptoms | 51 (1.7) | 9 (8.4) | 3.52 [1.57; 7.15] | 0.00101 | ** |
| No symptoms since 1 January 2020 | 734 (24.8) | 5 (4.7) | 0.14 [0.05; 0.31] | 0.00002 | *** |
| Not specified | 111 (3.8) | 2 (1.9) | 0.36 [0.06; 1.17] | 0.15838 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larribère, L.; Gordejeva, J.; Kuhnhenn, L.; Kurscheidt, M.; Pobiruchin, M.; Vladimirova, D.; Martin, M.; Roser, M.; Schramm, W.; Martens, U.M.; et al. Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center. Int. J. Environ. Res. Public Health 2021, 18, 7057. https://doi.org/10.3390/ijerph18137057
Larribère L, Gordejeva J, Kuhnhenn L, Kurscheidt M, Pobiruchin M, Vladimirova D, Martin M, Roser M, Schramm W, Martens UM, et al. Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center. International Journal of Environmental Research and Public Health. 2021; 18(13):7057. https://doi.org/10.3390/ijerph18137057
Chicago/Turabian StyleLarribère, Lionel, Jelizaveta Gordejeva, Lisa Kuhnhenn, Maximilian Kurscheidt, Monika Pobiruchin, Dilyana Vladimirova, Maria Martin, Markus Roser, Wendelin Schramm, Uwe M. Martens, and et al. 2021. "Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center" International Journal of Environmental Research and Public Health 18, no. 13: 7057. https://doi.org/10.3390/ijerph18137057
APA StyleLarribère, L., Gordejeva, J., Kuhnhenn, L., Kurscheidt, M., Pobiruchin, M., Vladimirova, D., Martin, M., Roser, M., Schramm, W., Martens, U. M., & Eigenbrod, T. (2021). Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center. International Journal of Environmental Research and Public Health, 18(13), 7057. https://doi.org/10.3390/ijerph18137057