1. Introduction
Limited research has been conducted to study the respiration behavior of tobacco use in the natural environment, in part due to the lack of suitable ambulatory monitoring techniques. Current commercially available Wearable Respiratory Monitors (WRM) may be leveraged to measure ambulatory respiration topography in the natural environment [
1], although little research [
2] has been done to utilize these devices for this application. In this paper, we demonstrate the feasibility of using one such WRM, the Hexoskin Smart Garment (Carré Technologies Inc., Montréal, PQ, Canada), to measure ambulatory respiration topography of cigarette and hookah smokers in their natural use environment.
To fully assess the health effects associated with tobacco use, both puffing and respiration behaviors must be considered. Traditionally, researchers have focused only on puffing behavior (puffing topography) quantified by puff flow rate, puff duration, puff volume, and inter puff gap, typically measured using a topography monitor [
3,
4,
5,
6]. However, puffing topography by itself is insufficient for understanding the distribution of toxic constituents in the respiratory tract beyond the oral cavity. The flow dynamics of the inhaled and exhaled volume, characterized by the flow rate, volume, duration, start and end time of each inhale and exhale, breath-hold period, and time between breaths, are necessary for accurate modeling of deposition of inhaled tobacco particles in the lungs [
7]. These parameters are collectively referred to as respiration topography.
Researchers have shown that users may alter their puffing and respiration behavior to compensate for the reduction in nicotine dose, typically by increasing puff and inhalation volume [
8,
9,
10,
11], but other compensatory mechanisms include regulating inhalation flow rate, increasing breath-hold duration, and extending the exhalation period to increase the retention of nicotine [
12]. Compensatory behavior has the potential to render alternative tobacco products, such as low-yield cigarettes, ineffective at reducing the risk of exposure or adverse health effects.
Respiration topography may also be used to study the effects of product characteristics on usage behavior due to variations in flow path restriction. Research has identified two main smoking patterns: mouth-to-lung (MTL) [
13] and direct-to-lung (DTL) [
14,
15]. MTL is typically associated with cigarette use. One possible reason for this is due to the restrictive nature of the cigarette flow path, which makes deep inhalations difficult. In contrast, we expect to see more DTL behavior in users of lower-resistance tobacco products, such as hookah and certain e-cigs, such as the JUUL. For any fixed inhaled volume, the concentration of nicotine is likely higher in DTL than in MTL since, in DTL, the volume is comprised entirely of emissions from the tobacco product, whereas in MTL, it is a smaller volume of puffed emissions that is then diluted in a larger volume of clean air during inhalation. Given this, it is conceivable that tobacco manufacturers are designing their products to have lower resistance, as is the trend from cig-a-likes, to sub-ohm, and finally to pod-style e-cigs, so as to facilitate DTL behavior and thereby increase nicotine consumption. This is, however, unverified, but with a method to measure respiratory topography, we may in the future be able to link product characteristics (e.g., flow path resistance) to product use behaviors (e.g., DTL vs. MTL) and their consequent health effects. By observing when inhalation occurs in relation to the puff, the full topographic smoking pattern can be obtained.
This paper aims to assess the feasibility of adapting the Hexoskin for ambulatory respiration topography observation and address some of the challenges, in particular, (1) calibration of the Hexoskin Smart Garment, (2) calculation of respiration topography parameters observed from smokers in their natural environment, and (3) acceptability of the Hexoskin by the participants.
2. Materials and Methods
2.1. Human Subject Study Protocol
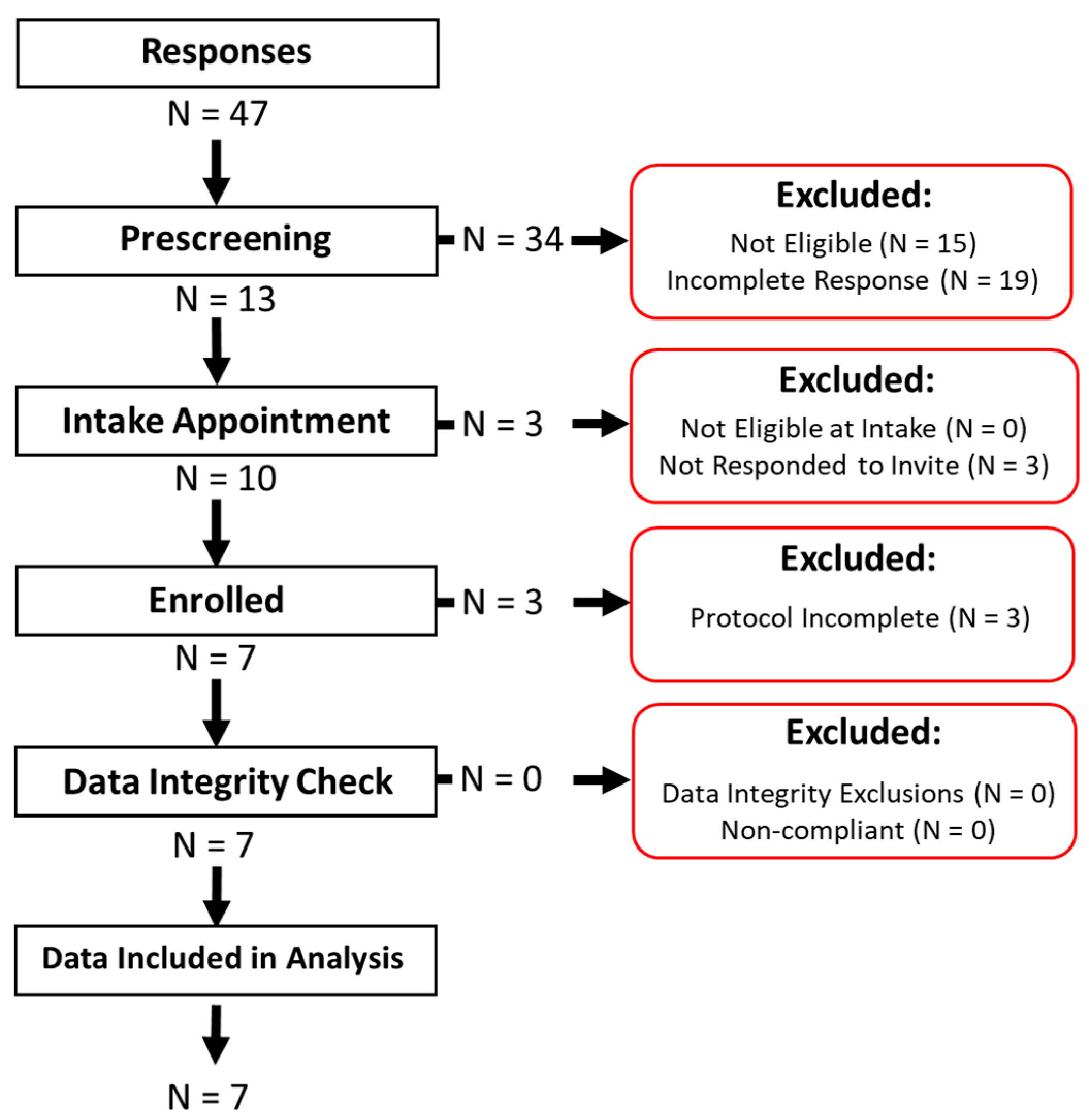
The study protocol consisted of an online participant recruitment and pre-screening survey (
Table 1) prior to the intake meeting, a final screening and verification of eligibility according to the Inclusion/Exclusion Criteria during the intake meeting, the review and signing of the informed consent form, the deployment of the WRM for a 3-day observation period with an in-lab WRM calibration on each observation day, an exit questionnaire assessing the acceptability of the monitor and the study protocol, and finally the incentives. The study protocol was reviewed and approved by the Rochester Institute of Technology (RIT) Human Subjects Research Office Institutional Review Board (IRB).
Cigarette and hookah users were recruited from the RIT community via mass email and flyers between July 2019 to March 2020, when the study was halted due to the COVID-19 pandemic. To satisfy the Inclusion Criteria, the participant must: (1) Be of legal smoking age, (2) Answer “Some days” or “Everyday” to the question Q1 or Q2 in
Table 1, and (3) Indicate that they had their own tobacco product since the study would not provide them with a product to use. We complied with the change in legal smoking age from 18 to 21 on 20 December 2019 due to the “Tobacco 21” legislation [
16]. The Exclusion Criteria excluded the following participants from being eligible: those with underlying cardiovascular and pulmonary diseases, pregnant women, or women intending to become pregnant.
The observation period spanned three days. On the first day, prospective participants were invited to the laboratory for a final eligibility screening and were enrolled once they reviewed and signed the informed consent form. Enrolled participants were provided with the WRM along with instructions on how to use it. The participants were informed that they must wear the WRM whenever they were using the tobacco product type they were enrolled to use and were not required to wear the WRM when not smoking. The participants were also provided with a daily study log to self-report their use behavior and compliance to the study protocol. At the end of the intake meeting, a WRM calibration was conducted on the participant, and then they were allowed to leave and use their tobacco product freely. On the second day, the participants returned to the laboratory at a pre-scheduled time for another WRM calibration. The participants were free to use their desired product prior to and after the scheduled meeting. On the third day, the participants returned to the laboratory and performed a final calibration. The participants were asked about the acceptability of the WRM and the study protocol in a structured interview. Finally, participants were provided a $25 incentive upon successful completion of the study protocol. Participants who dropped out of the study prematurely were provided with a $5 incentive.
2.2. Wearable Respiratory Monitor
The WRM used in this study is the Hexoskin Smart Garment with the Hexoskin Smart Device (datalogger). The Hexoskin has been used in a number of applications, including sports and fitness tracking [
17,
18], patient monitoring [
19], and assessing obesity risk [
20]. The use of the Hexoskin for ambulatory measurement of respiration topography was previously qualitatively assessed [
1]. The Smart Garment is a shirt-type WRM, made from a tight form-fitting material and can be worn on its own or as an undergarment. The shirt has two embedded respiratory inductance plethysmograph (RIP) sensors, one at the thorax (right below the pectoral muscle) and one on the abdomen. These sensors measure chest motion by measuring the changes in cross-sectional area at each location on the torso. The datalogger provides power to these sensors and collects data from them at a fixed rate of 128 Hz and stores the data internally. Data collection begins immediately once the datalogger is attached to the shirt and continues until it is detached from the shirt or the datalogger runs out of battery. Each time the datalogger is attached to the shirt, a new data record is created, without overwriting previous records. At the end of the observation period, the data was extracted from the datalogger to a computer via USB.
2.3. Calibration Theory and Process
The two chest motion waveforms, measured at the thorax (TC) and the abdomen (AB), are related to the lung volume waveform as per the model (reproduced in Equation (1)) introduced by Konno and Mead [
21]. The lung volume waveform calculated using this model is an estimate of the actual lung volume and is denoted by
. The parameters in curly braces denote vectors with a length of N elements. The Volume–Motion (V-M) parameters, Ktc and Kab, convert the TC and AB waveforms from arbitrary units (i.e., counts) to volume units (i.e., (mL)). These V-M parameters were obtained via calibration of the WRM, which must be done on the person wearing the WRM to account for variations in physiology and breathing style across participants and variations in respiratory sensor response across shirts. Although calibration is not necessary for deriving the inhalation duration, exhalation duration, and breath-hold, since these can be obtained directly from the chest motion waveform, it is necessary for deriving the inhalation and exhalation volumes and flow rates.
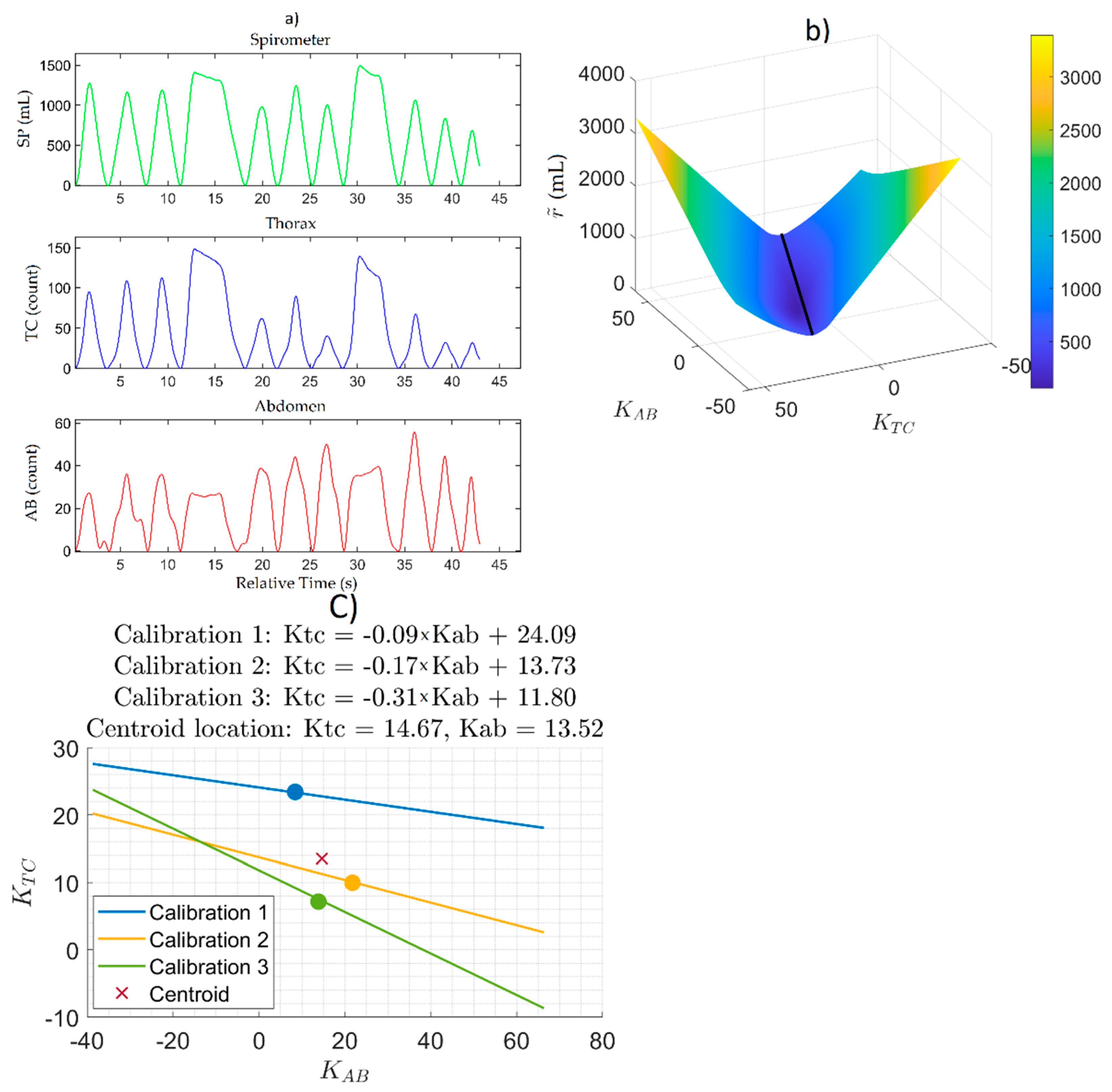
During calibration, participants were instructed to breathe exclusively through a spirometer (Vernier, Beaverton, OR, USA) while wearing the WRM and a nose clip and perform the following breathing exercise while seated: 5 normal breaths, followed by a deep inhale, a breath-hold, then an exhale, followed by 5 more normal breaths. This was repeated 3 times without pausing in between. Participants were instructed to abort the breathing exercise at any time if they experienced any discomfort.
The spirometer measures the actual lung volume waveform (SP) and is considered the true condition. By using Equation (1), the
waveform can be calculated from the TC and AB waveforms and an arbitrary set of Ktc and Kab. The difference between
and SP is defined as the residual (
, Equation (2)).
The residual is calculated at each value of the SP, TC, and AB waveforms and is therefore itself a waveform with a length of N elements. For a given set of SP, TC, and AB waveforms,
is a function of Ktc and Kab. The objective of the calibration is to find a pair of Ktc and Kab that minimizes
. For this, the mean absolute residual (
Equation (3)) is considered and is plotted as a function of Ktc and Kab to form a mean absolute residual surface. The
is a scalar with units of [mL] and represents the mean of the absolute difference between the volume estimate and the true condition.
2.4. Obtaining V-M Parameters from Multiple Calibrations
Section 2.3 described the theory and process for obtaining the V-M parameters from a single calibration. As per the study protocol, each participant performed 3 calibrations, one on each day of observation. As a result, there were 3 mean absolute residual surfaces for each participant. To find the set of Ktc and Kab that yields comparable
when applied to all 3 calibrations, we proposed finding the centroid to the polygon formed by connecting the minimum point of each surface. The values of Ktc and Kab at the centroid were then used to estimate the lung volume waveform (Equation (1)) from TC and AB obtained while the participant used their tobacco product in the natural environment. This method of obtaining the values of Ktc and Kab is broadly applicable for N
cal ≥ 3 calibrations.
2.5. Respiration Topography Analysis
The data analysis was conducted using an added feature in RIT’s previously described Topography Analysis Program (TAP) [
22]. First, the TC and AB time-series waveforms collected from the WRM were segmented into data for calibration, obtained during the calibration process, and data for calculating respiration topography, obtained during the natural environment observation. Both TC and AB waveforms were smoothed using a Savitzky–Golay 128-sample rolling-average filter. TAP then identified the minima in each waveform and then performed baseline compensation by first generating the baseline trend waveform for both TC and AB by piecewise interpolation between the minima on each waveform. The baseline trend waveform of each chest motion waveform was then subtracted from the original waveforms. The resultant baseline compensated waveform would then nominally have minima at 0. The algorithm then identified the maxima locations in each of the baseline compensated waveforms. The Ktc and Kab parameters were then obtained from the calibration data segment using the method described above. These parameters were then applied to Equation (1) along with the TC and AB from the natural environment data segment to obtain the volume estimate waveform.
The volume waveform was then segmented into individual breathing cycles by using the previously found extrema locations. The minimum at the start of a rising wave is the start of an inhale (and the start of the cycle), and the minimum at the end of a falling wave is the end of an exhale (and the end of the cycle). By considering the maxima, each breathing cycle could then be further segmented into an inhale, breath-hold, and exhale. Between any two minima there is one maximum, which corresponds to the end of the inhale. The segment of the waveform from the preceding minimum to this maximum was considered the inhale portion of the cycle. Subsequently, the period from the end of the inhale to the following minima was considered the exhale portion of the cycle. If a period of stable volume (neither rising nor falling significantly) is present following the end of an inhale before the start of the exhale, then this is considered the breath-hold period. During normal breathing, the breath-hold period is typically negligible; however, breath-holding is likely present following smoke/vapor inhalation during tobacco use.
2.6. Assessing Compliance and Acceptability
A daily paper study log was given to each participant that allowed them to self-report their product use during the study. The participant was instructed to report the number of cigarettes or hookah sessions they had each day along with the number of times they used their assigned product without wearing the WRM. By using this information, the participant’s compliance was assessed. The study log also allowed the participant to track whether they charged the WRM daily, which is necessary to prevent loss of data from the WRM discharging fully the following day.
During the exit appointment, each participant was given a questionnaire that assessed the acceptability of the study and the WRM. The questionnaire was administered as an interview, with the research administrator asking the questions and noting down the verbal responses from the participant.
4. Discussion
Many calibration techniques have been introduced in the literature [
21,
23,
24,
25]. We extended upon previous methods by analyzing the sensitivity of the residual to each V-M parameter. We saw that the mean absolute residual surface (
Figure 2b) showed a significantly stronger sensitivity to Ktc than to Kab. This feature was present in all participants. A simple linear regression algorithm would have just returned a single pair of Ktc and Kab that was the “good fit”, but we see that there is potentially an infinite number of combinations of Ktc and Kab with residuals within close proximity of each other (as illustrated by the valley in the mean absolute residual surface in
Figure 2b). In the absence of more information, it was not possible to determine the pair of Ktc and Kab that would qualify as a “good fit” beyond just a value judgment on the part of the analyst. One potential way to facilitate this is by obtaining more information about the physiology and the breathing style of the participant, such as by calibrating under different body postures or breathing maneuvers and patterns. We believe that the method presented here is a reasonable first step towards a more robust way to derive Ktc and Kab than the linear regression method presented in the past.
Additionally, we prototyped the logic to derive a single pair of Ktc and Kab from multiple calibrations (Ncal = 3 in this paper) using the centroid method. Other approaches considered included: (i) taking the mean Ktc and the mean Kab of the Ncal calibrations, (ii) only use a pair of Ktc and Kab from one of the Ncal calibrations, (iii) applying the pair of Ktc and Kab from the most recent calibration for the data collected following the calibration leading up to the next calibration, (iv) Combining all Ncal calibrations into a single data set to determine a single pair of Ktc and Kab. It is presently unclear what the best method is from these, but we plan on investigating this further.
The calibrations were conducted while the participants were seated only, with their torso perpendicular to the ground, which we deemed to be the posture the participants would most likely use during their tobacco use sessions. Some prior research suggests that a participant’s V-M parameters may vary based on their body position [
26]. Hence, it is possible that the inhalation and exhalation volumes measured by the WRM calibrated while seated may not be accurate if the participants were not seated while smoking. In a future study, we plan to investigate the impact of calibration posture on the accuracy of the volume measurements. The duration-based respiration topography parameters, such as inhale and exhale duration, were not impacted by the magnitude of the volume waveform and, therefore not impacted by the calibration since they were calculated from the temporal locations of the extrema on the lung volume waveform.
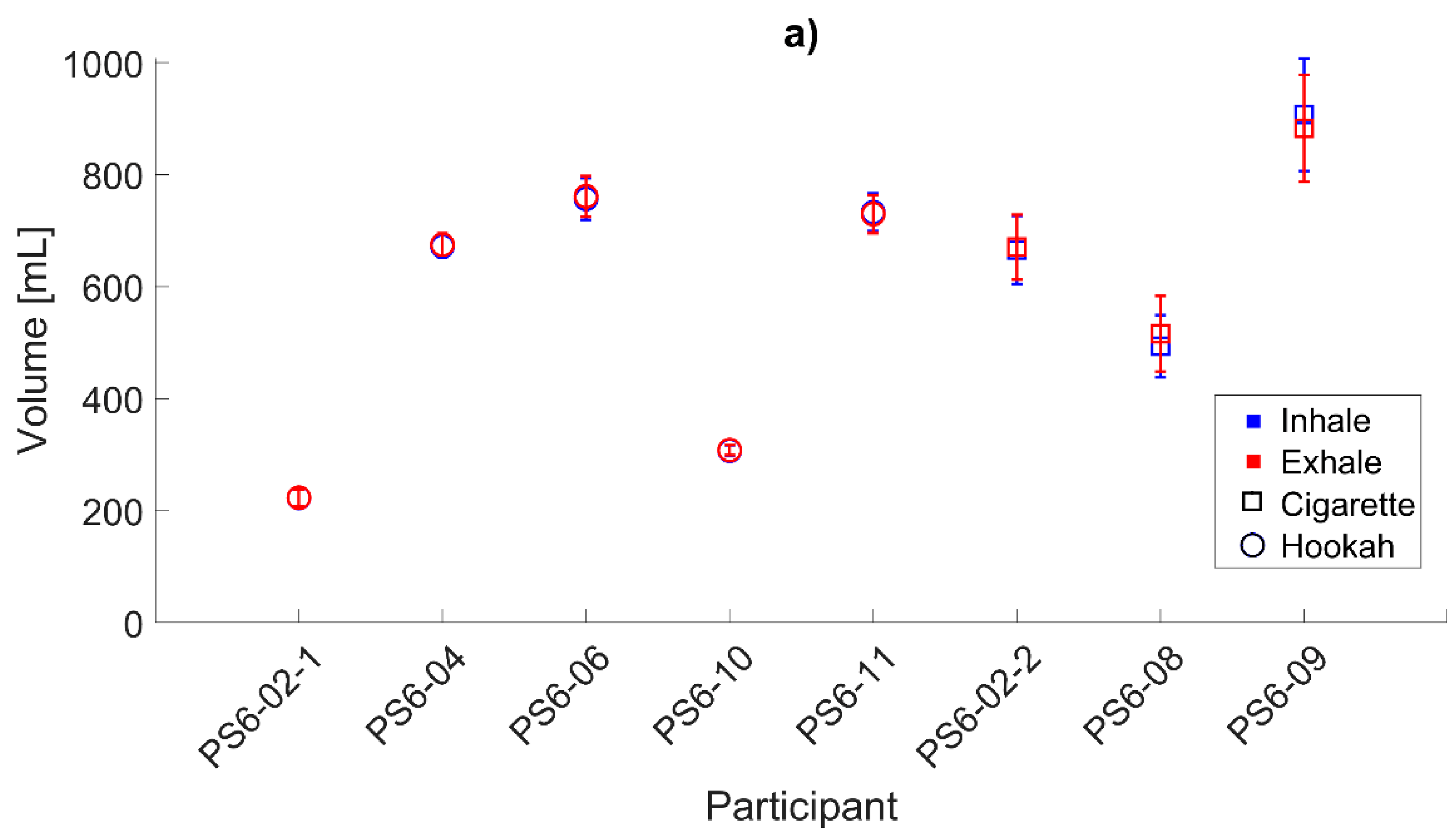
We were able to deploy the monitor for a 3-day observation study, which covered at least one full 24-h period. We were also able to analyze all the data collected from this period of observation and obtain both lung volume waveform and respiration topography for all seven participants. For this, we developed a computer algorithm to: (i) pre-process the data from the Hexoskin, (ii) perform the calibration and apply it to the measured TC and AB waveforms to obtain the lung volume waveform, and (iii) derive the respiration topography. This was necessary because the Hexoskin did not come with the necessary software to obtain either lung volume or respiration topography [
1]. We did not modify the Hexoskin hardware in any way for this study.
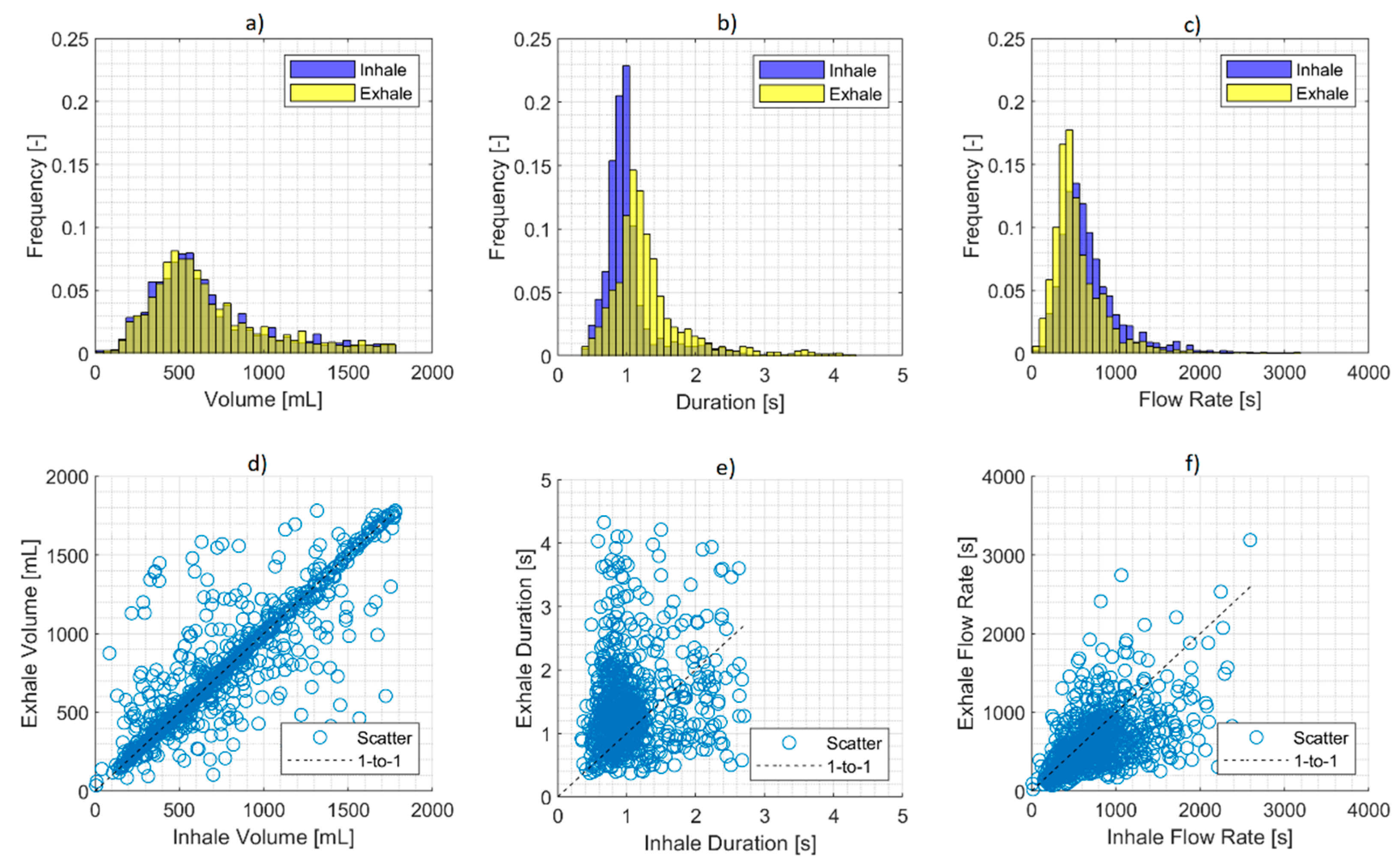
The data presented here were from participant’s smoking sessions and comprised two predominant underlying behaviors: natural tidal breathing and smoking-related ventilation, i.e., inhalation of tobacco emissions post puffing with potential breath-holding prior to exhalation. Although we did not attempt to discriminate between the two behaviors in this paper, the distribution (
Figure 4) of larger amounts of sub-1000 mL volumes and smaller amounts of volumes greater than 1000 mL is indicative of natural tidal breaths and smoking-related ventilation, respectively. The ability to discriminate between the two behaviors is necessary for identifying smoking-specific respiration topography. This is currently a focus of our future development. For this, we will leverage our wPUM topography monitors [
27] to identify the start and end of a puff relative to the lung volume waveform measured by the WRM. This will help in discriminating the breaths that are associated with smoking from the natural tidal breaths. Additionally, this will potentially allow us to discriminate between MTL and DTL. The characterization of these smoking patterns is also a topic for future research.
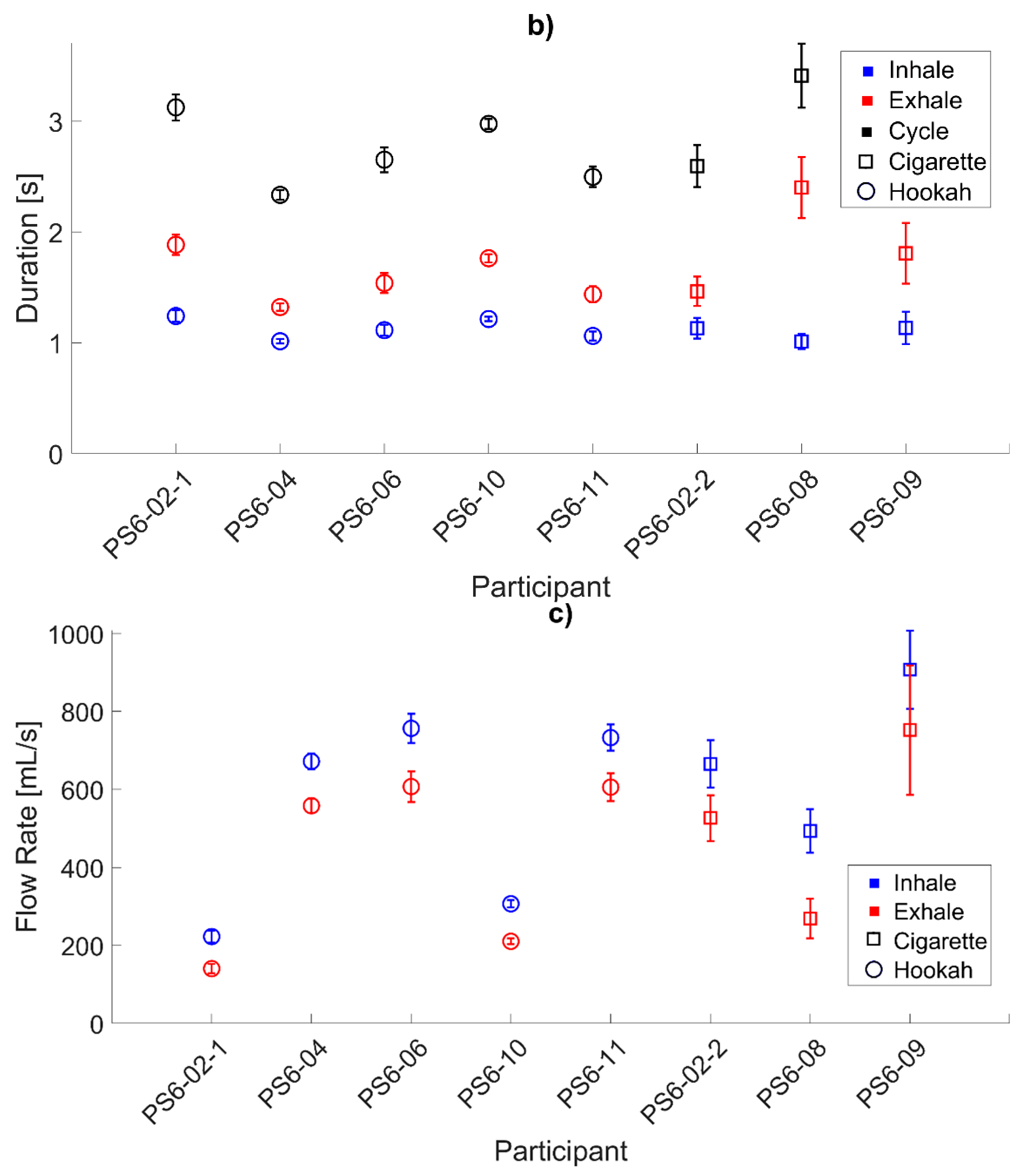
It was observed that in all participants, the mean exhale duration was longer than the mean inhale duration. This is consistent with the accepted pattern of tidal breathing in healthy adults. We predict that this phenomenon is also present in smoking-related ventilation cycles as a mechanism for increasing the nicotine uptake by extending the smoke retention time. Additionally, changes in the duration of either the inhale or the exhale or the ratio between the two may also be an effect of compensatory behavior. As expected from the relationship between the exhale duration and inhale duration and the consistent volume inhaled and exhaled, the data presented here indicate that the mean inhale flow rate was higher than the mean exhale flow rate.
The extrema locations in the volume waveform had a strong impact on the respiration topography since every respiration topography parameter was calculated based on the location of the extrema that prescribes each breathing cycle. Therefore, the algorithm used to find these extrema points had an impact since any misplaced extrema will affect the respiration topography of that breathing cycle and possibly those of the adjacent breathing cycles. The quality of the data and the nature of the behavior being observed also has an impact on the algorithm’s ability to obtain respiration topography, including irregularities in the volume waveform that may be a result of behaviors, such as walking, talking, and yawning, or sensor slippage on the body. More work still needs to be done to assess the sensitivity of respiration topography to these irregularities in the volume waveform. The current algorithm operated on the volume waveform directly and used the prominence values of the peaks and troughs of the breathing cycles to find the extrema, but alternative approaches exist that make use of frequency domain analysis or machine learning. More work must be done and presented to make a meaningful comparison between methods of obtaining respiration topography from lung waveform.
The participants’ acceptability of the Hexoskin is key to assessing its viability as a tool for ambulatory measurement of respiration topography. Prior to the start of the study, we were concerned that the participants would not be willing to wear the Hexoskin shirt for extended periods, i.e., to cover the whole day of observation. Therefore, we only required the participant to wear the shirt while they were using their tobacco product, and we expected that the participants would take the shirt off in between sessions. From the exit interview results, we can see that the majority did remove the shirt in between sessions but most indicated that they would be willing to wear it for extended periods. In a future study, we intend to recommend the participant wear the shirt for a full day of observation. Data collected outside of their smoking session will help establish the participant’s baseline tidal breathing behavior and help with identifying smoking-related ventilation. The downside to the requirement to wearing the shirt for an extended amount of time is that we would lose the natural indication of the start and end of a smoking session that came with the participant attaching and detaching the datalogger from the shirt. Another option is for the participant to wear the shirt throughout the day but detach the datalogger between sessions. The disadvantage here is that there is a risk that the participant would forget to reattach the datalogger prior to starting a session, causing the loss of valuable data. Alternatively, we can leverage our wPUM topography monitor to provide the start and end time of each puff and the start and end time of each session.
Another concern that we had was in the amount of data that would be collected if the shirt was worn for an extended time. The Hexoskin samples each chest motion sensor at 128 Hz, which after 12 h would result in over 5 million samples. In addition to the storage concerns, we anticipated computational difficulty with processing large vectors and finding extrema locations in large sets of data. In practice thus far, we have not encountered any issues with our algorithm in terms of the data size. We expect that the algorithm would be scalable to larger datasets obtained from longer observation periods.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}