
Emotional Intelligence and Social Support: Two Key Factors in Preventing Occupational Stress during COVID-19



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Demographics
2.3.2. Emotional Intelligence
2.3.3. Social Support
2.3.4. Occupational Stress
2.4. Statistical Analyses
3. Results
3.1. Preliminary Analyses
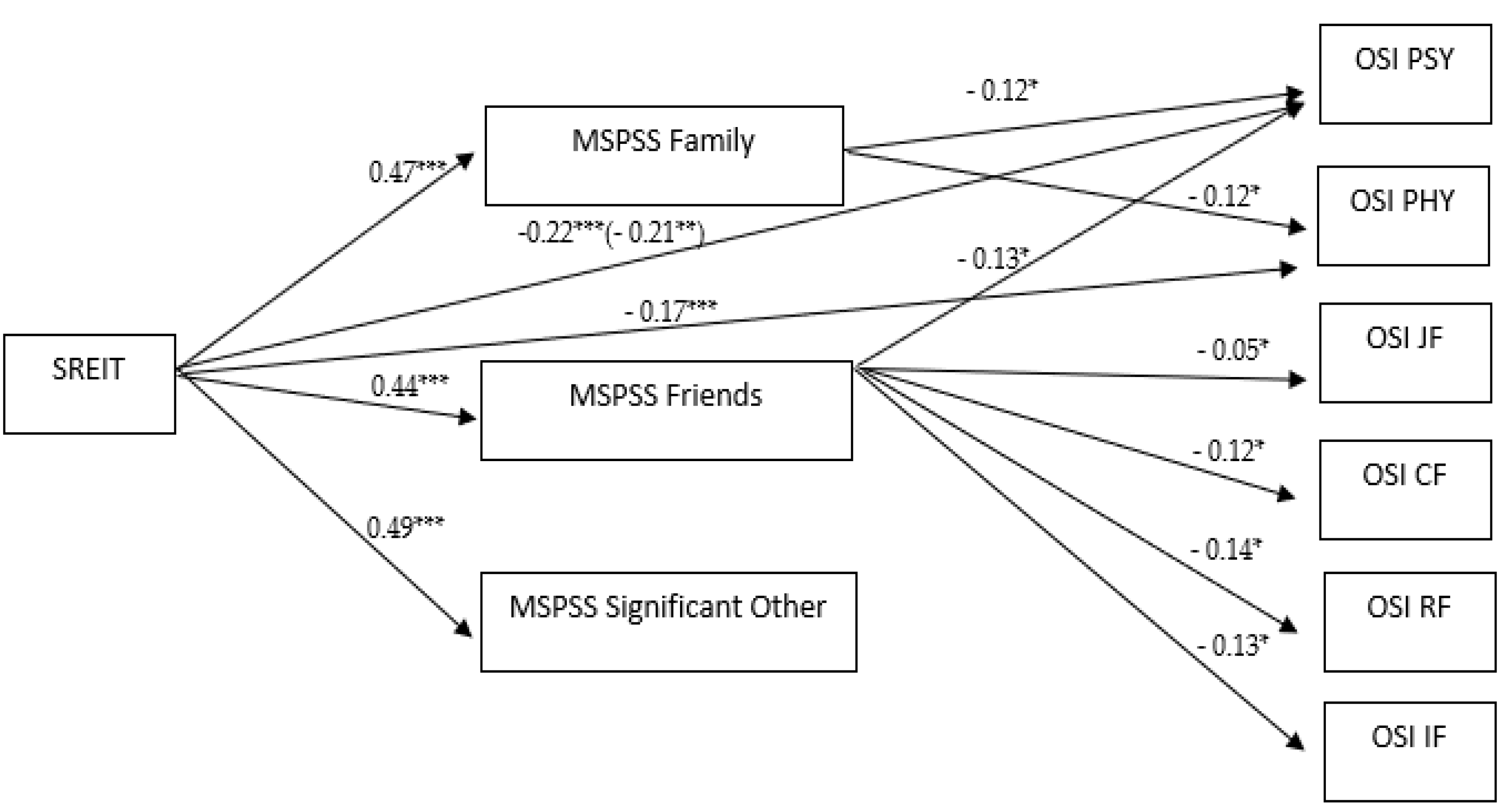
3.2. Mediation Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ganster, D.C.; Rosen, C.C. Work stress and employee health: A multidisciplinary review. J. Manag. 2013, 39, 1085–1122. [Google Scholar] [CrossRef]
- Clarke, S.G.; Cooper, C.L. The risk management of occupational stress. Health Risk Soc. 2000, 2, 173–187. [Google Scholar] [CrossRef]
- van der Ploeg, E.; Kleber, R.J. Acute and chronic job stressors among ambulance personnel: Predictors of health symptoms. Occup. Environ. Med. 2003, 60, 40–46. [Google Scholar] [CrossRef] [Green Version]
- King, K.A.; Vidourek, R.; Schwiebert, M. Disordered eating and job stress among nurses. J. Nurs. Manag. 2009, 17, 861–869. [Google Scholar] [CrossRef]
- Espnes, G.A.; Byrne, D.G. Occupational stress and cardiovascular disease. Stress Health 2008, 24, 231–238. [Google Scholar]
- Bhui, K.S.; Dinos, S.; Stansfeld, S.A.; White, P.D. A Synthesis of the Evidence for Managing Stress at Work: A review of the reviews reporting on Anxiety, Depression, and Absenteeism. J. Environ. Public Health 2012, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, H.; Nakao, H.; Tsuchiya, M.; Kuroda, Y.; Katoh, T. Burnout and work environments of public health nurses involved in mental health care. Occup. Environ. Med. 2004, 61, 764–768. [Google Scholar] [CrossRef]
- Mosaredaghrad, A.M. Occupational stress and its consequences: Implications for health policy and management. Leadersh. Health Serv. 2014, 3, 224–239. [Google Scholar] [CrossRef]
- Lambert, E.; Paoline, E.A. The influence of individual, job and organizational characteristics on correctional staff job stress, job satisfaction and organizational commitment. Crim. Justice Rev. 2008, 33, 541–564. [Google Scholar] [CrossRef]
- Kenny, D.T.; Cooper, C.L. Introduction: Occupational stress and its management. Int. J. Stress Manag. 2003, 10, 275–279. [Google Scholar] [CrossRef]
- Beehr, T.A.; Farmer, S.; Glazer, S.; Gudanowski, D.M.; Nair, V.N. The enigma of social support and occupational stress: Source of congruence and gender tole effects. J. Occup. Health Psych. 2003, 8, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Biron, C.; Brun, J.P.; Ivers, H. Extend and sources of occupational stress in university staff. Work 2008, 30, 511–522. [Google Scholar] [PubMed]
- Cheng, Y.; Guo, Y.L.; Yeh, W.Y. A national survey of psychosocial job stressors and their implications for health among working people in Taiwan. Int. Arch. Occup. Environ. Health 2001, 74, 495–504. [Google Scholar] [CrossRef]
- Islam, M.I.; Alam, K.M.W.; Keramat, S.A. Working conditions and occupational stress among nurses in Bangladesh: A cross-sectional pilot study. J. Public Health 2021. [CrossRef]
- Marinaccio, A.; Ferrante, P.; Corfiati, M.; Di Tecco, C.; Rondinone, B.M.; Bonafede, M.; Ronchetti, M.; Persechino, B.; Iavicoli, S. The relevance of socio-demographic and occupational variables for the assessment of work-related stress risk. BMC Public Health 2013, 13, 1157. [Google Scholar] [CrossRef] [Green Version]
- Ryu, G.W.; Yang, Y.S.; Choi, M. Mediating role of coping style on the relationship between job stress and subjective well-being among Korean police officers. BMC Public Health 2020, 20, 470. [Google Scholar] [CrossRef]
- Mensah, A. Job stress and mental well-being among working men and women in Europe: The mediating role of social support. Int. J. Environ. Res. Public Health 2021, 18, 2494. [Google Scholar] [CrossRef]
- Leon, R.D.; Tănăsescu, R.I. Emotional intelligence and occupational stress in Romanian organizations. Manag. Dyn. Knowl. Econ. 2018, 1, 52–65. [Google Scholar] [CrossRef] [Green Version]
- Ogińska-Bulik, N. Emotional intelligence in the workplace: Exploring its effects on occupational stress and health outcomes in human service workers. Int. J. Occup. Med. 2005, 18, 167–175. [Google Scholar]
- Petrides, K.V.; Pita, R.; Kokkinaki, F. The location of trait emotional intelligence in personality factor space. Br. J. Psychol. 2007, 98, 273–289. [Google Scholar] [CrossRef] [Green Version]
- Goleman, D. Working with Emotional Intelligence; Bantam: Bloomsbury, London, 1998. [Google Scholar]
- Hong, E.; Lee, Y.S. The mediating effect of emotional intelligence between emotional labour, job stress, burnout and nurses’ turnover intention. Int. J. Nurs. Pract. 2016, 22, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Krishnakumar, R.; Lalitha, S. A study on emotional intelligence and occupational stress. IJMCR 2014, 2, 633–636. [Google Scholar]
- O’Connor, P.; Nguyen, J.; Anglim, J. Effectively coping with task stress: A study of the validity of the Trait Emotional Intelligence Questionnaire–Short Form (TEIQue–SF). J. Personal. Assess. 2017, 99, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Srivastava, R. Examine the relationship between emotional intelligence with Demographic profile, job stress, job satisfaction and turnover intention. Int. J. Appl. Bus. Econ. Res. 2016, 14, 4887–4900. [Google Scholar]
- Anand, P.V. Occupational stress: Relationship with emotional intelligence and coping self-efficacy. J. Organ. Hum. Behav. 2019, 8, 33–39. [Google Scholar]
- Lee, J.H.; Sim, I.-O. Analysis of the relationship between the psychological wellbeing, emotional intelligence, willpower, and job-efficacy of clinical nurses: A structural model application. Int. J. Environ. Res. Public. Health 2021, 18, 5582. [Google Scholar] [CrossRef]
- Bar-On, R.; Brown, J.M.; Kirkcaldy, B.D.; Thorne, E.P. Emotional expression and implications for occupational stress: An application of the Emotional Quotient Inventory (EQ-I). Personal. Individ. Differ. 2000, 28, 1107–1118. [Google Scholar] [CrossRef]
- King, M.; Gardner, D. Emotional intelligence and occupational stress among professional staff in New Zeland. Int. J. Organ. Anal. 2006, 14, 186–203. [Google Scholar] [CrossRef]
- Augusto Landa, J.M.; López-Zafra, E.; Berrios Martos, M.P.; Aguilar-Luzón, M. The relationship between emotional intelligence, occupational stress and health in nurses: A questionnaire survey. Int. J. Nurs. Stud. 2008, 45, 888–901. [Google Scholar] [CrossRef]
- Walia, P.; Tulsi, P.K. Emotional intelligence and occupational stress of college teachers. J. Organ. Hum. Behav. 2014, 3, 33–39. [Google Scholar]
- Lartey, J.K.S.; Amponsah-Tawiah, K.; Osafo, J. Emotional intelligence and perceived organizational support as predictors of emotional exhaustion among nurses and midwives. Int. J. Worplace Health Manag. ahead-of-print. [CrossRef]
- Dinicola, G.; Julian, L.; Gregorich, S.E. The role of social support in anxiety for persons with COPD. J. Psychosom. Res. 2013, 74, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.Q.; Chen, W.Q.; Lin, J.X. Effect of social support on psychological-stress-induced anxiety and depressive symptoms in patients receiving peritoneal dialysis. J. Psychol. Res. 2008, 65, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Kafetsios, K.; Sideridis, G.D. Attachment, social support and well-being in young and older adults. J. Health Psychol. 2006, 11, 863–875. [Google Scholar] [CrossRef]
- Gallagher, E.N.; Vella-Brodrick, D.A. Social support and emotional intelligence as predictors of subjective well-being. Personal. Individ. Differ. 2008, 44, 1551–1561. [Google Scholar] [CrossRef]
- Koydemir, S.; Simsek, Ö.F.; Schütz, A.; Tipandjan, A. Differences in how trait emotional intelligence predicts life satisfaction: The role of affect balance versus social support in India and Germany. J. Happiness Stud. 2013, 14, 51–66. [Google Scholar] [CrossRef]
- Kong, F.; Zhao, J.; You, X. Social support mediates the impact of emotional intelligence on mental distress and life satisfaction in Chinese young adults. Personal. Individ. Differ. 2012, 53, 513–517. [Google Scholar] [CrossRef]
- Kong, F.; Gong, X.; Sajjad, S.; Yang, K.; Zhao, J. How is emotional intelligence linked to life satisfaction? The mediating role of social support, positive affect and negative affect. J. Happiness Stud. 2019, 20, 2733–2745. [Google Scholar]
- Yousaf, S.; Rasheed, M.I.; Hameed, Z.; Luqman, A. Occupational stress and its outcomes: The role of work-social support in the hospitality industry. Personal. Rev. 2019, 49, 755–773. [Google Scholar] [CrossRef]
- Beehr, T.A.; Bowling, N.A.; Bennett, M.M. Occupational stress and failures of social support: When helping hurts. J. Occup. Health Phychol. 2010, 15, 45–59. [Google Scholar] [CrossRef]
- Christo, F.; Kirti, T. Organizational role stress: Impact of manager and peer support. J. Knowl. Glob. 2012, 5, 1–28. [Google Scholar]
- Woodhead, E.L.; Northrop, L.; Edelstein, B. Stress, social support, and burnout among long-term care nursing staff. J. Appl. Gerontol. 2016, 35, 84–105. [Google Scholar] [CrossRef] [PubMed]
- Slaski, M.; Cartwright, S. Health, performance and emotional intelligence: An exploratory study of retail managers. Stress Health 2002, 18, 63–68. [Google Scholar] [CrossRef]
- Jordan, D.J.; Ashkanasy, N.M.; Hartel, C.E.J. Emotional intelligence as a moderator of emotional and behavioral reactions to job insecurity. Acad. Manag. Rev. 2002, 27, 361–372. [Google Scholar] [CrossRef] [Green Version]
- Salovey, P.; Rothman, A.J.; Detweiler, J.B.; Steward, W.T. Emotional states and physical health. Am. Psychol. 2000, 55, 276–285. [Google Scholar] [CrossRef]
- Montes-Berges, B.; Augusto, J.M. Exploring the relationship between perceived emotional intelligence, coping, social support and mental health in nursing students. J. Psychiatr. Ment. Health Nurs. 2007, 14, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Yeung, D.Y.; Liu, E.S.C.; Rochelle, T.L. Sequential mediating effects of provided and received social support on trait emotional intelligence and subjective happiness: A longitudinal examination in Hong Kong Chinese university students. Int. J. Psychol. 2019, 54, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Jia, H.; Zhang, J.; Li, Y.; Song, F.; Yu, X. Nurses’ occupational stress and presenteeism: The mediating role of public service motivation and the moderating role of health. Int. J. Environ. Res. Public Health 2021, 18, 3523. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Ricciardi, W.; Antonelli, M. Occupational stress and mental health among anestetists during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8245. [Google Scholar] [CrossRef]
- Al-Mansour, K.; Alfuzan, A.; Alsarheed, D.; Alenexi, M.; Abogazalah, F. Work-related challenges among primary health centers workers during COVID-19 in Saudi Arabia. Int. J. Environ. Res. Public. Health 2021, 18, 1898. [Google Scholar] [CrossRef]
- Soto-Rubio, A.; Giménez-Espert, M.; Prado_Gascó, V. Effect of emotional intelligence and psychological risks of burnout, job satisfaction, and nurses’ health during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7998. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Lee, S.-Y.; Cho, J.-H. A study on the job retention intention of nurses based on social support in the COVID-19 Situation. Sustainability 2020, 12, 7276. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Hall, L.E.; Haggerty, D.J.; Cooper, J.T.; Golden, C.J.; Dornheim, L. Development and validation of a measure of emotional intelligence. Personal. Individ. Differ. 1998, 25, 167–177. [Google Scholar] [CrossRef]
- Craparo, G.; Magnano, P.; Faraci, P. Psychometric properties of the Italian version of the Self-Report Emotional Intelligence Test (SREIT). TPM Test. Psychom. 2014, 21, 121–133. [Google Scholar]
- Di Fabio, A.; Busoni, L. Misurare il supporto sociale percepito: Proprietà psicometriche della Multidimensional Scale of Perceived Social Support (MSPSS) in un campione di studenti universitari. Risorsa Uomo 2008, 14, 339–350. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.L.; Sloan, S.J.; Williams, S. Occupational Stress Indicator; NFERNelson: Windsor, UK, 1988. [Google Scholar]
- Sirigatti, S.M.; Stefanile, C. OSI: Occupational Stress Indicator; Giunti OS-Organizzazioni Speciali: Florence, Italy, 2002. [Google Scholar]
- Carríon, G.C.; Nitzl, C.; Roldán, J.L. Mediation Analyses in Partial Least Squares Structural Equation Modeling: Guidelines and Empirical Examples; Springer: New York, NY, USA, 2017. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Demographics | Options | N | % |
|---|---|---|---|
| Gender | Males | 197 | 53.7% |
| Females | 170 | 46.7% | |
| Marital status | Unmarried | 127 | 34.6% |
| Married | 177 | 48.2% | |
| Divorced | 20 | 5.4% | |
| Widower | 1 | 0.3% | |
| Cohabitant | 42 | 11.4% | |
| Parental status | No children | 172 | 47.1% |
| 1 child | 76 | 20.8% | |
| 2 children | 96 | 26.3% | |
| 3 children | 18 | 4.9% | |
| 4 children | 1 | 0.3% | |
| 5 children | 2 | 0.5% | |
| Educational | Junior high school | 42 | 11.6% |
| High school | 116 | 32% | |
| Degree (Bachelor/Master) | 127 | 35% | |
| Post-degree | 78 | 21.5% | |
| Employment status | Private sector | 240 | 65.8% |
| Public sector | 100 | 27.4% | |
| Tertiary sector | 25 | 6.8% | |
| Way of working during COVID-19 | work remotely only | 80 | 21.8% |
| work remotely, but also at the workplace | 99 | 27% | |
| work at the workplace, but also remotely, | 63 | 17.2% | |
| work at the workplace only | 120 | 32.7% | |
| Amount of changes in working conditions during COVID-19 | Not at all | 51 | 13.9% |
| A little | 135 | 13.9% | |
| Somewhat | 101 | 27.5% | |
| Very much | 64 | 17.4% | |
| Working conditions changed during COVID-19 | Salary increase | 29 | 5% |
| Salary decrease | 78 | 13.4% | |
| Working hours increase | 126 | 21.6% | |
| Working hours decrease | 69 | 11.8% | |
| Kind of job activity | 69 | 11.8% | |
| Layoff | 26 | 4.5% | |
| Relationships with coworkers | 118 | 20.2% | |
| Relationships with supervisors | 49 | 8.4% | |
| Other | 19 | 3.3% |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. SREIT | - | |||||||||||
| 2. MSPSS Family | 0.47 ** | - | ||||||||||
| 3. MSPSS Friends | 0.44 ** | 0.48 ** | - | |||||||||
| 4. MSPSS Significant Other | 0.49 ** | 0.51 ** | 0.52 ** | - | ||||||||
| 5. OSI PSY | −0.22 ** | −0.17 ** | −0.12 * | 0.03 | - | |||||||
| 6. OSI PHY | −0.17 ** | −0.19 ** | −0.08 | 0.09 | 0.65 ** | - | ||||||
| 7. OSI JF | −0.01 | −0.04 | 0.07 | 0.01 | 0.55 ** | 0.55 ** | - | |||||
| 8. OSI MF | 0.10 | 0.07 | −0.08 | −0.09 | 0.38 ** | 0.40 ** | 0.81 ** | - | ||||
| 9. OSI RF | 0.01 | 0.02 | −0.10 * | −0.01 | 0.47 ** | 0.50 ** | 0.83 ** | 0.84 ** | - | |||
| 10. OS CF | 0.03 | 0.01 | −0.10 * | 0.04 | 0.44 ** | 0.46 ** | 0.80 ** | 0.83 ** | 0.82 ** | - | ||
| 11. OSI IF | 0.09 | 0.10 | −0.15 * | 0.07 | 0.41 ** | 0.40 ** | 0.80 ** | 0.85 ** | 0.80 ** | 0.80 ** | - | |
| 12. OSI SF | 0.10 | 0.07 | 0.09 | 0.09 | 0.32 ** | 0.37 ** | 0.77 ** | 0.89 ** | 0.81 ** | 0.81 ** | 0.83 ** | - |
| Gender | M | SD | F | Sig | Partial η2 | |
|---|---|---|---|---|---|---|
| STREIT | M | 116.63 | 16.32 | |||
| F | 116.41 | 15.85 | ||||
| Tot | 116.53 | 16.08 | 0.018 | 0.895 | 0.000 | |
| MPSS Family | M | 22.86 | 5.73 | |||
| F | 23.49 | 5.01 | ||||
| Tot | 23.15 | 5.41 | 1.21 | 0.272 | 0.003 | |
| MPSS Friends | M | 21.49 | 5.71 | |||
| F | 21.57 | 5.85 | ||||
| Tot | 21.53 | 5.77 | 0.017 | 0.896 | 0.000 | |
| MPSS Significant Other | M | 23.29 | 5.24 | |||
| F | 23.33 | 5.63 | ||||
| Tot | 23.31 | 5.42 | 0.005 | 0.946 | 0.000 | |
| OSI PSY | M | 55.52 | 15.32 | |||
| F | 56.33 | 12.41 | ||||
| Tot | 55.89 | 14.04 | 0.301 | 0.584 | 0.001 | |
| OSY PHY | M | 32.80 | 14.79 | |||
| F | 33.63 | 12.45 | ||||
| Tot | 33.18 | 13.75 | 0.333 | 0.564 | 0.001 | |
| OSI JF | M | 30.45 | 9.63 | |||
| F | 30.60 | 7.97 | ||||
| Tot | 30.52 | 8.89 | 0.026 | 0.873 | 0.000 | |
| OSI MF | M | 39.32 | 11.82 | |||
| F | 40.34 | 11.23 | ||||
| Tot | 39.79 | 11.55 | 0.706 | 0.401 | 0.002 | |
| OSI RF | M | 34.28 | 10.38 | |||
| F | 33.76 | 9.15 | ||||
| Tot | 34.04 | 9.82 | 0.251 | 0.617 | 0.001 | |
| OSI CF | M | 32.50 | 9.56 | |||
| F | 32.43 | 8.81 | ||||
| Tot | 32.47 | 9.21 | 0.006 | 0.939 | 0.000 | |
| OSI IF | M | 39.86 | 11.03 | |||
| F | 40.30 | 11.02 | ||||
| Tot | 40.06 | 11.01 | 0.141 | 0.708 | 0.000 | |
| OSI SF | M | 40.56 | 11.70 | |||
| F | 40.73 | 11.81 | ||||
| Tot | 40.64 | 11.74 | 0.020 | 0.888 | 0.000 |
| 95% CI | |||||
|---|---|---|---|---|---|
| Type | Effect | LL | UP | β | p |
Indirect | SREIT → MSPSS Family → OSI PSY SREIT → MSPSS Friends → OSI PSY SREIT → MSPSS Significant Other → OSI PSY | −0.097 0.005 −0.055 | −0.003 0.091 0.042 | −0.06 −0.05 0.00 | 0.036 0.027 0.800 |
| Direct | SREIT → OSI PSY | −0.305 | −0.070 | −0.21 | 0.002 |
| Total | SREIT → OSI PSY | −0.283 | −0.108 | −0.22 | <0.001 |
Indirect | SREIT → MSPSS Family → OSI PHY SREIT → MSPSS Friends → OSI PHY SREIT → MSPSS Significant Other → OSI PHY | −0.094 −0.026 −0.083 | −0.002 0.056 0.014 | −0.06 0.01 −0.04 | 0.041 0.474 0.163 |
| Direct | SREIT → OSI PHY | −0.195 | 0.036 | −0.09 | 0.177 |
| Total | SREIT → OSI PHY | −0.233 | −0.061 | −0.17 | <0.001 |
Indirect | SREIT → MSPSS Family → OSI MF SREIT → MSPSS Friends → OSI MF SREIT → MSPSS Significant Other → OSI MF | −0.047 −0.011 −0.014 | 0.029 0.059 0.068 | −0.01 0.03 0.04 | 0.643 0.175 0.192 |
| Direct | SREIT → OSI MF | −0.072 | 0.123 | 0.04 | 0.609 |
| Total | SREIT → OSI MF | −0.004 | 0.141 | 0.09 | 0.066 |
Indirect | SREIT → MSPSS Family → OSI JB SREIT → MSPSS Friends → OSI JF SREIT → MSPSS Significant Other → OSI JF | −0.052 0.001 −0.034 | 0.007 0.056 0.029 | −0.04 −0.05 0.01 | 0.139 0.042 0.867 |
| Direct | SREIT → OSI JF | −0.079 | 0.071 | .01 | 0.913 |
| Total | SREIT → OSI JF | −0.057 | 0.056 | .01 | 0.980 |
Indirect | SREIT → MSPSS Family → OSI RF SREIT → MSPSS Friends → OSI RF SREIT → MSPSS Significant Other → OSI RF | −0.035 0.007 −0.055 | 0.029 0.069 0.015 | −0.01 −0.06 −0.03 | 0.862 0.015 0.254 |
| Direct | SREIT → OSI RF | −0.095 | 0.072 | −0.02 | 0.784 |
| Total | SREIT → OSI RF | −0.059 | 0.066 | 0.01 | 0.915 |
Indirect | SREIT → MSPSS Family → OSI CF SREIT → MSPSS Friends → OSI CF SREIT → MSPSS Significant Other → OSI CF | −0.046 0.001 −0.034 | 0.016 0.059 0.032 | −0.03 −0.06 −0.01 | 0.344 0.039 0.942 |
| Direct | SREIT → OSI CF | −0.075 | 0.082 | 0.01 | 0.922 |
| Total | SREIT → OSI CF | −0.040 | 0.077 | 0.03 | 0.543 |
Indirect | SREIT → MSPSS Family → OSI IF SREIT → MSPSS Friends → OSI IF SREIT → MSPSS Significant Other → OSI IF | −0.024 0.004 −0.049 | 0.049 0.073 0.029 | 0.02 −0.05 −0.01 | 0.491 0.026 0.607 |
| Direct | SREIT → OSI IF | −0.074 | 0.112 | 0.03 | 0.700 |
| Total | SREIT → OSI IF | −0.009 | 0.129 | 0.09 | 0.092 |
Indirect | SREIT → MSPSS Family → OSI SF SREIT → MSPSS Friends → OSI SF SREIT → MSPSS Significant Other → OSI SF | −0.043 −0.062 −0.034 | 0.035 0.056 0.049 | −0.01 0.02 0.01 | 0.837 0.278 0.738 |
| Direct | SREIT → OSI SF | −0.029 | 0.170 | 0.09 | 0.167 |
| Total | SREIT → OSI SF | −0.019 | 0.167 | 0.01 | 0.233 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenti, G.D.; Faraci, P.; Magnano, P. Emotional Intelligence and Social Support: Two Key Factors in Preventing Occupational Stress during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 6918. https://doi.org/10.3390/ijerph18136918
Valenti GD, Faraci P, Magnano P. Emotional Intelligence and Social Support: Two Key Factors in Preventing Occupational Stress during COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(13):6918. https://doi.org/10.3390/ijerph18136918
Chicago/Turabian StyleValenti, Giusy Danila, Palmira Faraci, and Paola Magnano. 2021. "Emotional Intelligence and Social Support: Two Key Factors in Preventing Occupational Stress during COVID-19" International Journal of Environmental Research and Public Health 18, no. 13: 6918. https://doi.org/10.3390/ijerph18136918
APA StyleValenti, G. D., Faraci, P., & Magnano, P. (2021). Emotional Intelligence and Social Support: Two Key Factors in Preventing Occupational Stress during COVID-19. International Journal of Environmental Research and Public Health, 18(13), 6918. https://doi.org/10.3390/ijerph18136918