
Factors Influencing Unmet Healthcare Needs among Older Korean Women


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Samples
2.2. Instruments
2.2.1. Baseline Characteristics
2.2.2. Unmet Healthcare Needs
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistics Korea. Statistics of Elderly Population. 2019. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/1/index.board?bmode=read&aSeq=377701 (accessed on 20 May 2020).
- Ministry of Health and Welfare. 2017 The Survey of the Elderly Population; Report No.: 2017-53; Ministry of Health and Welfare: Sejong, Korea, 2017; 881p.
- Joo, J.H.; Kim, H.J.; Jang, J.; Park, E.; Jang, S. Unmet healthcare needs status and trend of Korea in 2018. Health Policy Manag. 2020, 30, 120–125. [Google Scholar] [CrossRef]
- Shin, S.; Hwang, E. Gender differences in the cognitive function and nutritional status in older age: A representative nationwide data of Korean elders. J. Korean Public Health Nurs. 2017, 31, 209–219. [Google Scholar] [CrossRef]
- Lee, H.S. The factors influencing health-related quality of life in the elderly: Focused on the general characteristics, health habits, mental health, chronic diseases, and nutrient intake status: Data from the fifth Korea national health and nutrition examination survey (KNHANES V), 2010~ 2012. Korean J. Community Nutr. 2014, 19, 479–489. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K.; Heidari, B.; Hajian-Tilaki, A. Health related quality of life and its socio-demographic determinants among Iranian elderly people: A population based cross-sectional study. J. Caring Sci. 2017, 6, 39–47. [Google Scholar] [CrossRef]
- Sim, S. Basic Study on the Life Satisfaction of the Elderly. In 2018 National Statistical Development Institute Research Report; 2018; pp. 60–115. Available online: http://kostat.go.kr/sri/srikor/srikor_pbl/2/index.board?bmode=read&aSeq=371290&pageNo=4&rowNum=10&amSeq=&sTarget=&sTxt= (accessed on 20 May 2020).
- Park, G.; Choi, B. A gender analysis of the association between self-rated health and disability of daily living among Korean elderly. Korean Public Health Res. 2018, 44, 25–34. [Google Scholar]
- Scheel-Hincke, L.L.; Möller, S.; Lindahl-Jacobsen, R.; Jeune, B.; Ahrenfeldt, L.J. Cross-national comparison of sex differences in ADL and IADL in Europe: Findings from share. Eur. J. Ageing 2020, 17, 69–79. [Google Scholar] [CrossRef]
- Kwon, J.O.; Lee, E.N.; Bae, S.H. Concept analysis of health inequalities. J. Korean Acad. Nurs. 2015, 21, 20–31. [Google Scholar] [CrossRef][Green Version]
- Herr, M.; Arvieu, J.J.; Aegerter, P.; Robine, J.; Ankri, J. Unmet health care needs of older people: Prevalence and predictors in a French cross-sectional survey. Eur. J. Public Health. 2014, 24, 808–813. [Google Scholar] [CrossRef]
- Pappa, E.; Kontodimopoulos, N.; Papadopoulos, A.; Tountas, Y.; Niakas, D. Investigating unmet health needs in primary health care services in a representative sample of the Greek population. Int. J. Environ. Res. Public Health 2013, 10, 2017–2027. [Google Scholar] [CrossRef]
- OECD. Unmet Needs for Healthcare; OECD, 2019; Available online: https://www.oecd.org/health/health-systems/Unmet-Needs-for-Health-Care-Brief-2020.pdf (accessed on 20 May 2020).
- Jang, J.; Yoon, H.J.; Park, E.; Jang, S. Unmet healthcare needs status and trend of Korea in 2016. Health Policy Manag. 2018, 28, 91–94. [Google Scholar] [CrossRef]
- Socias, M.E.; Koehoorn, M.; Shoveller, J. Gender inequalities in access to health care among adults living in British Columbia, Canada. Womens Health Issues 2016, 26, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J. Understanding reasons for unmet health care needs in Korea: What are health policy implications? BMC Health Serv. Res. 2018, 18, 557. [Google Scholar] [CrossRef]
- Lee, S.E.; Yeon, M.; Kim, C.; Yoon, T. The association among individual and contextual factors and unmet healthcare needs in South Korea: A multilevel study using national data. J. Prev. Med. Public Health. 2016, 49, 308. [Google Scholar] [CrossRef]
- Tumin, D.; Menegay, M.; Shrider, E.A.; Nau, M.; Tumin, R. Local income inequality, individual socioeconomic status, and unmet healthcare needs in Ohio, USA. Health Equity 2018, 2, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Hoebel, J.; Rommel, A.; Schröder, S.L.; Fuchs, J.; Nowossadeck, E.; Lampert, T. Socioeconomic inequalities in health and perceived unmet needs for healthcare among the elderly in Germany. Int J. Environ. Res. Public Health 2017, 14, 1127. [Google Scholar] [CrossRef]
- Zavras, D.; Zavras, A.I.; Kyriopoulos, I.I.; Kyriopoulos, J. Economic crisis, austerity and unmet healthcare needs: The case of Greece. BMC Health Serv. Res. 2016, 16, 309. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, J.; Moon, Y.; Kim, K.J.; Lee, K.; Choi, J.; Han, S. Unmet healthcare needs of elderly people in Korea. BMC Geriatr. 2018, 18, 98. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Ouyang, W.; Tian, L.; Song, Y.; Miao, W. Elderly health inequality in China and its determinants: A geographical perspective. Int. J. Environ. Res. Public Health 2019, 16, 2953. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, D.I.; Park, H.Y.; Pak, Y.; Tran, P.N.H.; Thai, T.T.; Thuy, M.T.T.; Dung, D.V. Unmet healthcare needs and associated factors in rural and suburban Vietnam: A cross-sectional study. Int. J. Environ. Res. Public Health. 2020, 17, 6320. [Google Scholar] [CrossRef]
- Lee, Y.J. Elderly healthy level of regional disparities compare. J. Korea Contents Assoc. 2015, 15, 347–358. [Google Scholar] [CrossRef]
- Meemon, N.; Paek, S.C. Factors associated with unmet need for healthcare among older adults in Thailand. Asia Pac. Soc. Sci. Rev. 2019, 19, 180–191. [Google Scholar]
- OECD. Unmet Needs Health Care Due Cost. Health Glance 2017. [Google Scholar] [CrossRef]
- Lee, H.J.; Huh, S.I. Unmet health care needs and impact of type of household among the elderly in Korea. Korean J. Health Econ. Policy 2017, 23, 85–108. [Google Scholar]
- Moon, J.; Kang, M. The prevalence and predictors of unmet medical needs among the elderly living alone in Korea: An application of the behavioral model for vulnerable populations. Health Soc. Welf. Rev. 2016, 36, 480–510. [Google Scholar] [CrossRef]
- Shin, H.E.; Ko, J.I.; Sim, E.H.; Kim, H.S. Unmet health care needs of elderly in South Korea: Systematic review. Health Econ. Policy Res. 2019, 25, 29–52. [Google Scholar]
- Syed, S.T.; Gerber, B.S.; Sharp, L.K. Traveling towards disease: Transportation barriers to healthcare access. J. Community Health 2013, 38, 976–993. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | n (%) | Unmet Healthcare Needs | χ2 | p | |
|---|---|---|---|---|---|
| Yes (n = 4151) | No (n = 38,547) | ||||
| n (%) | n (%) | ||||
| Age | |||||
| 65~74 | 21,135(49.5) | 1715(41.3) | 19,420(50.4) | 154.64 | <0.001 |
| 75~84 | 17,618(41.5) | 1896(45.7) | 15,722(40.8) | ||
| ≥85 | 3945(9.2) | 540(13.0) | 3405(8.8) | ||
| Residential area | |||||
| Metropolitan | 13,846(32.4) | 1025(24.7) | 12,821(33.3) | 127.12 | <0.001 |
| Urban | 8786(20.6) | 981(23.6) | 7805(20.2) | ||
| Rural | 20,066(47.0) | 2145(51.7) | 17,921(46.5) | ||
| Living arrangement | |||||
| Living alone | 15,748(36.9) | 1881(45.3) | 13,867(36.0) | 140.43 | <0.001 |
| Living with others | 26,950(63.1) | 2270(54.7) | 24,680(64.0) | ||
| Family income (monthly) (US dollars) | |||||
| <2000 | 30,062(70.4) | 3148(75.8) | 26,914(69.8) | 128.83 | <0.001 |
| 2000–4000 | 4512(10.6) | 284(6.8) | 4228(11.0) | ||
| 4001–6000 | 1646(3.9) | 76(1.8) | 1570(4.1) | ||
| >6000 | 6478(15.2) | 643(15.5) | 5835(15.1) | ||
| Education (n = 42,641) | |||||
| ≤Elementary school | 32,810(76.9) | 3554(85.7) | 29,256(76.0) | 208.69 | <0.001 |
| High school | 8590(20.2) | 547(13.2) | 8043(20.9) | ||
| ≥College | 1241(2.9) | 45(1.1) | 1196(3.1) | ||
| Basic livelihood subsidy (n = 42,656) | |||||
| Yes | 2947(6.9) | 523(12.6) | 2424(6.3) | 234.15 | <0.001 |
| No | 39,709(93.1) | 3614(87.4) | 36,095(93.7) | ||
| Activities of daily living (n = 42,696) | |||||
| Easy | 26,377(61.8) | 1679(40.5) | 24,698(64.1) | 1075.2 | <0.001 |
| A little difficult | 14,975(35.1) | 2124(51.2) | 12,851(33.3) | ||
| Difficult | 1344(3.1) | 347(8.4) | 997(2.6) | ||
| Diagnosed with hypertension (n = 42,675) | |||||
| Yes | 25,707(60.3) | 2534(61.1) | 23,173(60.1) | 1.34 | 0.249 |
| No/ | 16,968(39.7) | 1615(38.9) | 15,353(39.9) | ||
| Diagnosed with diabetes (n = 42,670) | |||||
| Yes | 8878(20.8) | 858(20.7) | 8020(20.8) | 0.04 | 0.855 |
| No | 33,792(79.2) | 3289(79.3) | 30,503(79.2) | ||
| Subjective health (n = 42,685) | |||||
| Good | 7287(17.1) | 354(8.5) | 6933(18.0) | 749.86 | <0.001 |
| Fair | 15,971(37.4) | 1084(26.1) | 14,887(38.6) | ||
| Poor | 19,427(45.5) | 2711(65.3) | 16,716(43.4) | ||
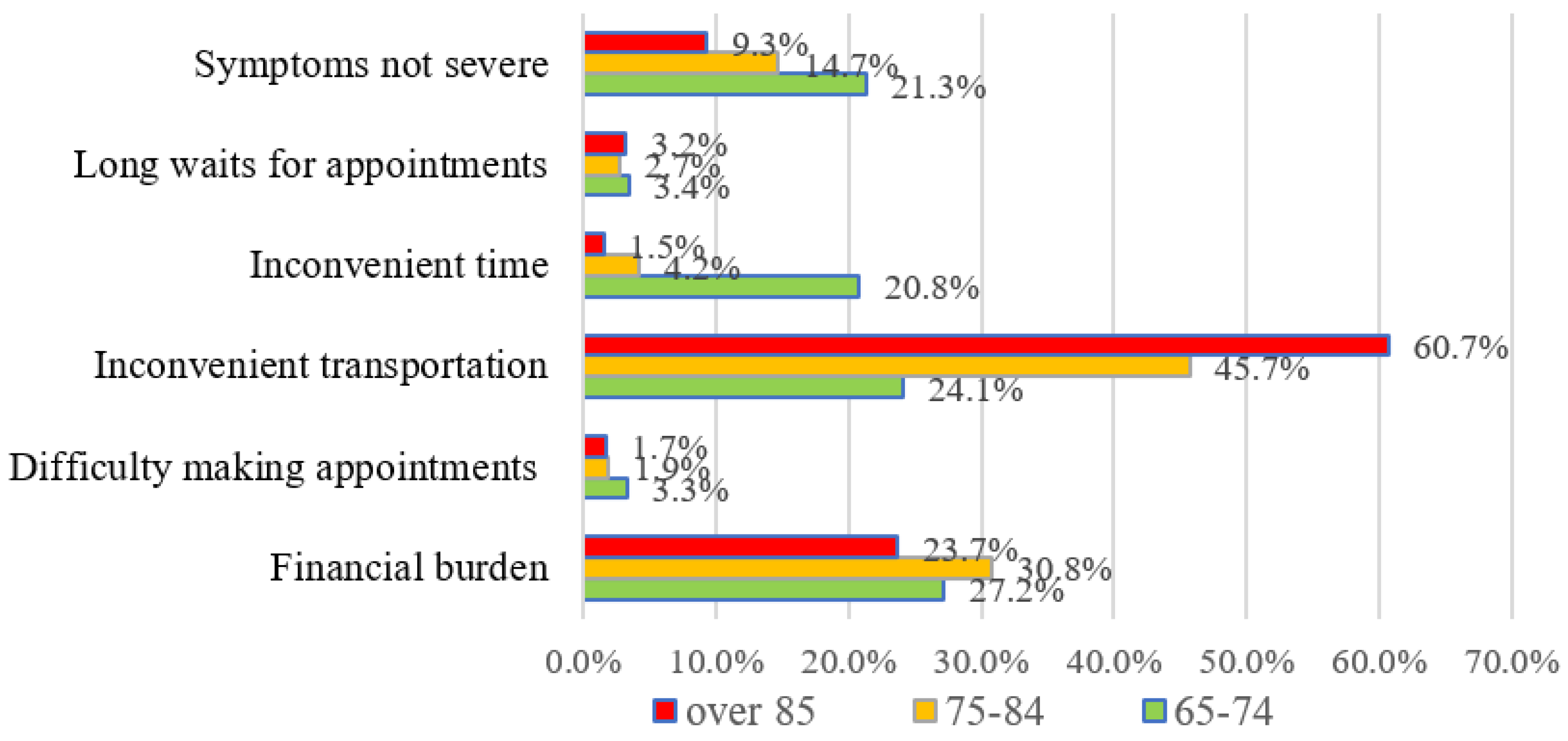
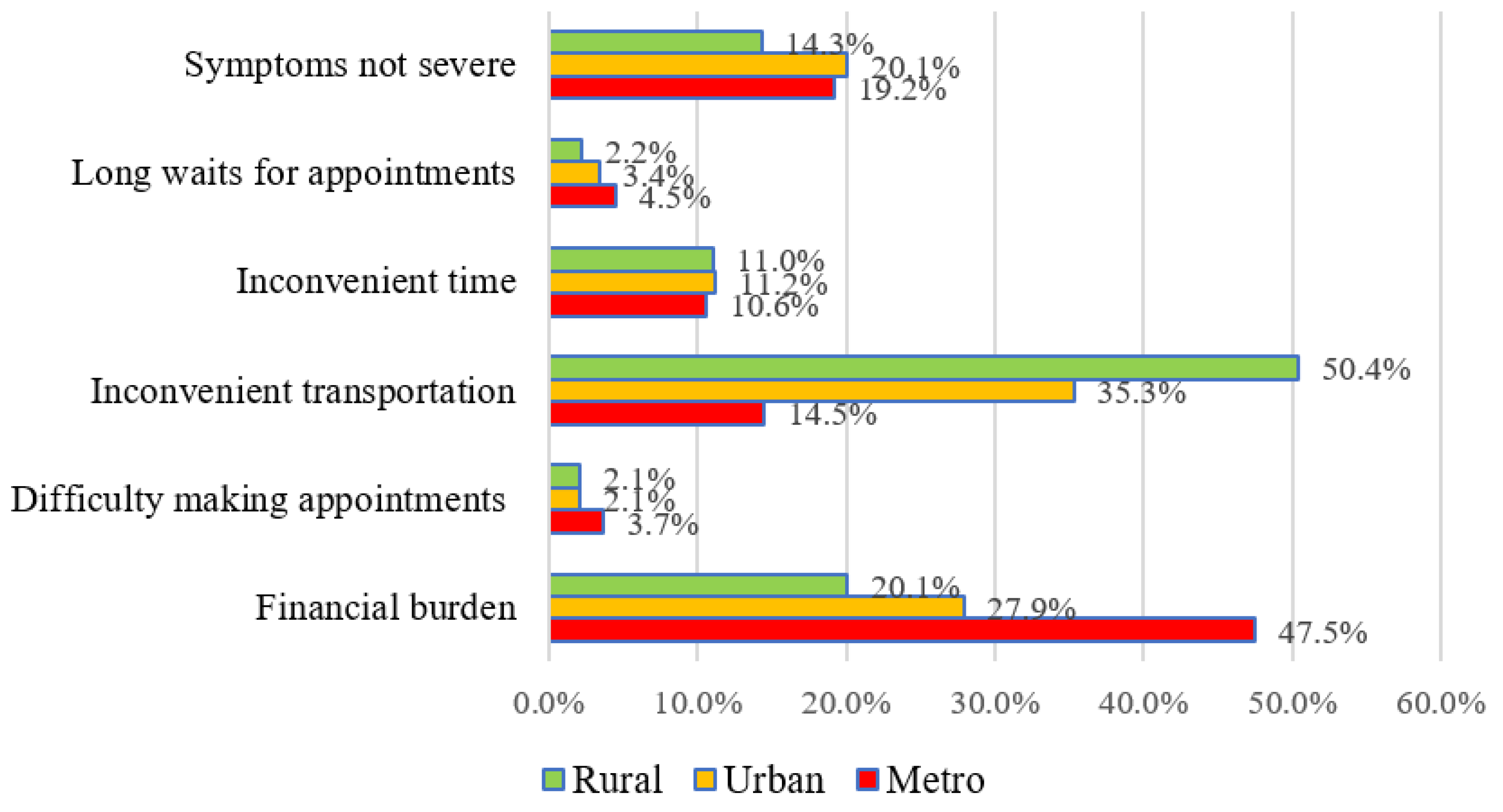
| Categories | n (%) | Age | χ2 (p) | Residential Area | χ2 (p) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 65~74 | 75~84 | ≥85 | Metropolitan | Urban | Rural | |||||
| (n = 1416) | (n = 1508) | (n = 410) | (n = 785) | (n = 796) | (n = 1753) | |||||
| n (%) | n (%) | |||||||||
| Financial burden | 947 (28.4) | Y | 385 | 465 | 97 | 9.95 (0.007) | 373 | 222 | 352 | 200.83 (<0.001) |
| (40.7) | (49.1) | (10.2) | (39.4) | (23.4) | (37.2) | |||||
| N | 1031 | 1043 | 313 | 412 | 574 | 1401 | ||||
| (43.2) | (43.7) | (13.1) | (17.3) | (24.0) | (58.7) | |||||
| Difficulty making appointments | 82 (2.5) | Y | 47 | 28 | 7 | 7.61 (0.022) | 29 | 17 | 36 | 6.54 (0.038) |
| (57.3) | (34.1) | (8.5) | (35.4) | (20.7) | (43.9) | |||||
| N | 1369 | 1480 | 403 | 756 | 779 | 1717 | ||||
| (42.1) | (45.5) | (12.4) | (23.2) | (24.0) | (52.8) | |||||
| Inconvenient transportation | 1279 (38.4) | Y | 341 | 689 | 249 | 243.12 (<0.001) | 114 | 281 | 884 | 299.76 (<0.001) |
| (26.7) | (53.9) | (19.5) | (8.9) | (22.0) | (69.1) | |||||
| N | 1075 | 819 | 161 | 671 | 515 | 869 | ||||
| (52.3) | (39.9) | (7.8) | (32.7) | (25.1) | (42.3) | |||||
| Inconvenient time | 364 (10.9) | Y | 294 | 64 | 6 | 247.85 (<0.001) | 83 | 89 | 192 | 0.15 (0.926) |
| (80.8) | (17.6) | (1.6) | (22.8) | (24.5) | (52.7) | |||||
| N | 1122 | 1444 | 404 | 702 | 707 | 1561 | ||||
| (37.8) | (48.6) | (13.6) | (23.6) | (23.8) | (52.6) | |||||
| Long waits for appointments | 101 (3.0) | Y | 48 | 40 | 13 | 1.38 (0.501) | 35 | 27 | 39 | 9.67 (0.008) |
| (47.5) | (39.6) | (12.9) | (34.7) | (26.7) | (38.6) | |||||
| N | 1368 | 1468 | 397 | 750 | 769 | 1714 | ||||
| (42.3) | (45.4) | (12.3) | (23.2) | (23.8) | (53.0) | |||||
| Symptoms not severe | 561 (16.8) | Y | 301 | 222 | 38 | 41.37 (<0.001) | 151 | 160 | 250 | 17.59 (<0.001) |
| (53.7) | (39.6) | (6.8) | (26.9) | (28.5) | (44.6) | |||||
| N | 1115 | 1286 | 372 | 634 | 636 | 1503 | ||||
| (40.2) | (46.4) | (13.4) | (22.9) | (22.9) | (54.2) | |||||
| Variables | B | OR | 95% CI | p |
|---|---|---|---|---|
| Age | ||||
| ≥85 | 0.01 | 1.01 | 0.90~1.13 | 0.839 |
| 75~84 | −0.07 | 0.93 | 0.83~1.03 | 0.2 |
| 65~74 (reference) | ||||
| Residential area | ||||
| Rural | 0.29 | 1.34 | 1.21~1.47 | <0.001 |
| Urban | 0.16 | 1.18 | 10.08~1.28 | <0.001 |
| Metropolitan (reference) | ||||
| Living alone | ||||
| Yes | 0.19 | 1.21 | 1.13~1.31 | <0.001 |
| No (reference) | ||||
| Family income (monthly) | ||||
| (US dollars) | ||||
| <2000 | −0.03 | 0.92 | 0.84~1 | 0.12 |
| 2000–4000 | −0.29 | 0.71 | 0.62~0.81 | <0.001 |
| 4001–6000 | −0.60 | 0.54 | 0.42~0.70 | <0.001 |
| >6000 (reference) | ||||
| Education | ||||
| ≤Elementary school | 0.55 | 1.73 | 1.27~2.36 | <0.001 |
| High school | 0.34 | 1.4 | 1.02~1.92 | 0.034 |
| ≥College (reference) | ||||
| Basic livelihood subsidy | ||||
| Yes | 0.57 | 1.67 | 1.50~1.83 | <0.001 |
| No (reference) | ||||
| Activities of daily living | ||||
| A little difficult | 0.59 | 1.81 | 1.68~1.95 | <0.001 |
| Difficult | 1.23 | 3.43 | 2.97~3.96 | <0.001 |
| Easy (reference) | ||||
| Subjective health | ||||
| Good | −0.79 | 0.45 | 0.40~0.51 | <0.001 |
| Fair | −0.50 | 0.6 | 0.55~0.65 | <0.001 |
| Poor (reference) | ||||
| Diagnosed with hypertension | ||||
| Yes | −0.14 | 0.86 | 0.81–0.93 | <0.001 |
| No (reference) | ||||
| Diagnosed with diabetes | ||||
| Yes | −0.13 | 0.87 | 0.80~0.94 | 0.001 |
| No (reference) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.A.; Kim, O. Factors Influencing Unmet Healthcare Needs among Older Korean Women. Int. J. Environ. Res. Public Health 2021, 18, 6862. https://doi.org/10.3390/ijerph18136862
Choi JA, Kim O. Factors Influencing Unmet Healthcare Needs among Older Korean Women. International Journal of Environmental Research and Public Health. 2021; 18(13):6862. https://doi.org/10.3390/ijerph18136862
Chicago/Turabian StyleChoi, Jung A., and Oksoo Kim. 2021. "Factors Influencing Unmet Healthcare Needs among Older Korean Women" International Journal of Environmental Research and Public Health 18, no. 13: 6862. https://doi.org/10.3390/ijerph18136862
APA StyleChoi, J. A., & Kim, O. (2021). Factors Influencing Unmet Healthcare Needs among Older Korean Women. International Journal of Environmental Research and Public Health, 18(13), 6862. https://doi.org/10.3390/ijerph18136862