
Ageist Attitudes Are Associated with Will-to-Live and Moderated by Age, Medical Conditions and Attitudes toward Aging

Abstract
1. Introduction
2. Study 1
2.1. Method
2.1.1. Participants and Procedure
2.1.2. Measures
2.1.3. Data Analysis
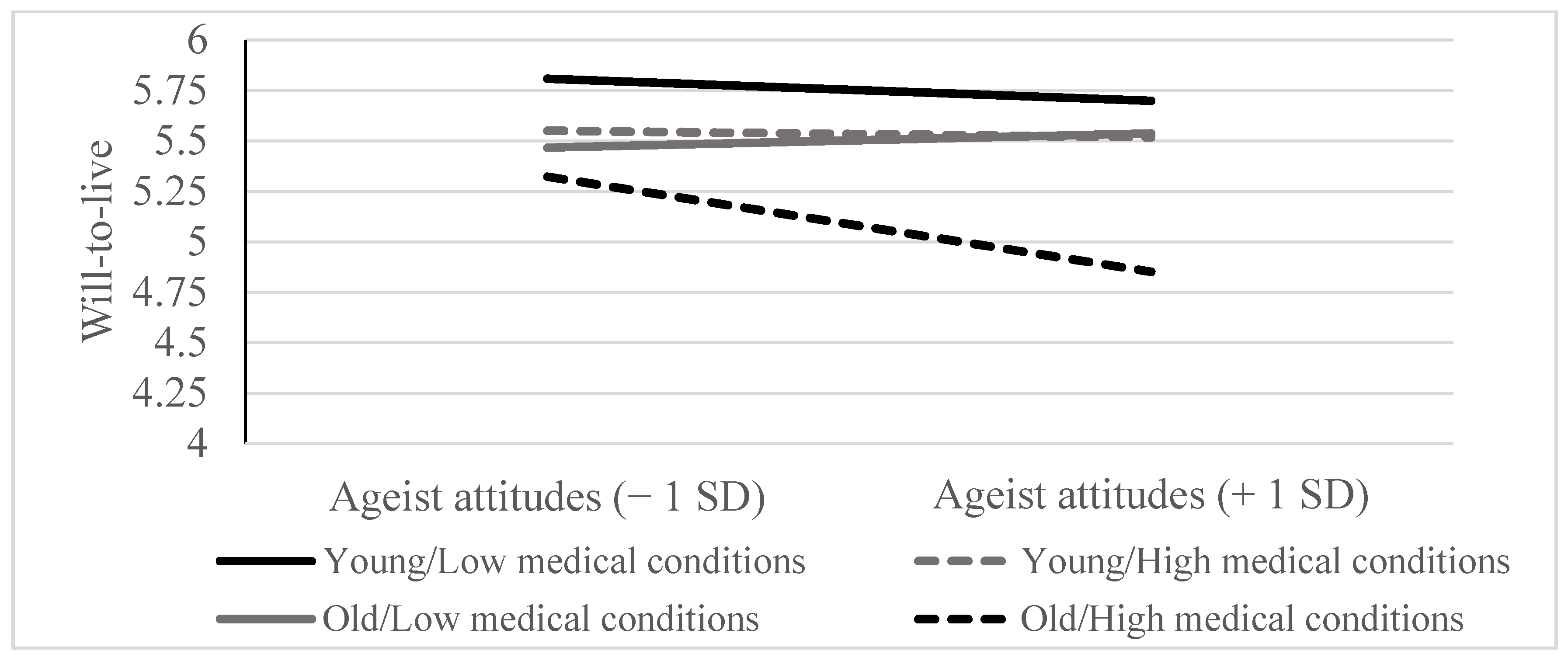
2.2. Results and Discussion
3. Study 2
3.1. Method
3.1.1. Participants and Procedure
3.1.2. Measures
3.1.3. Data Analysis
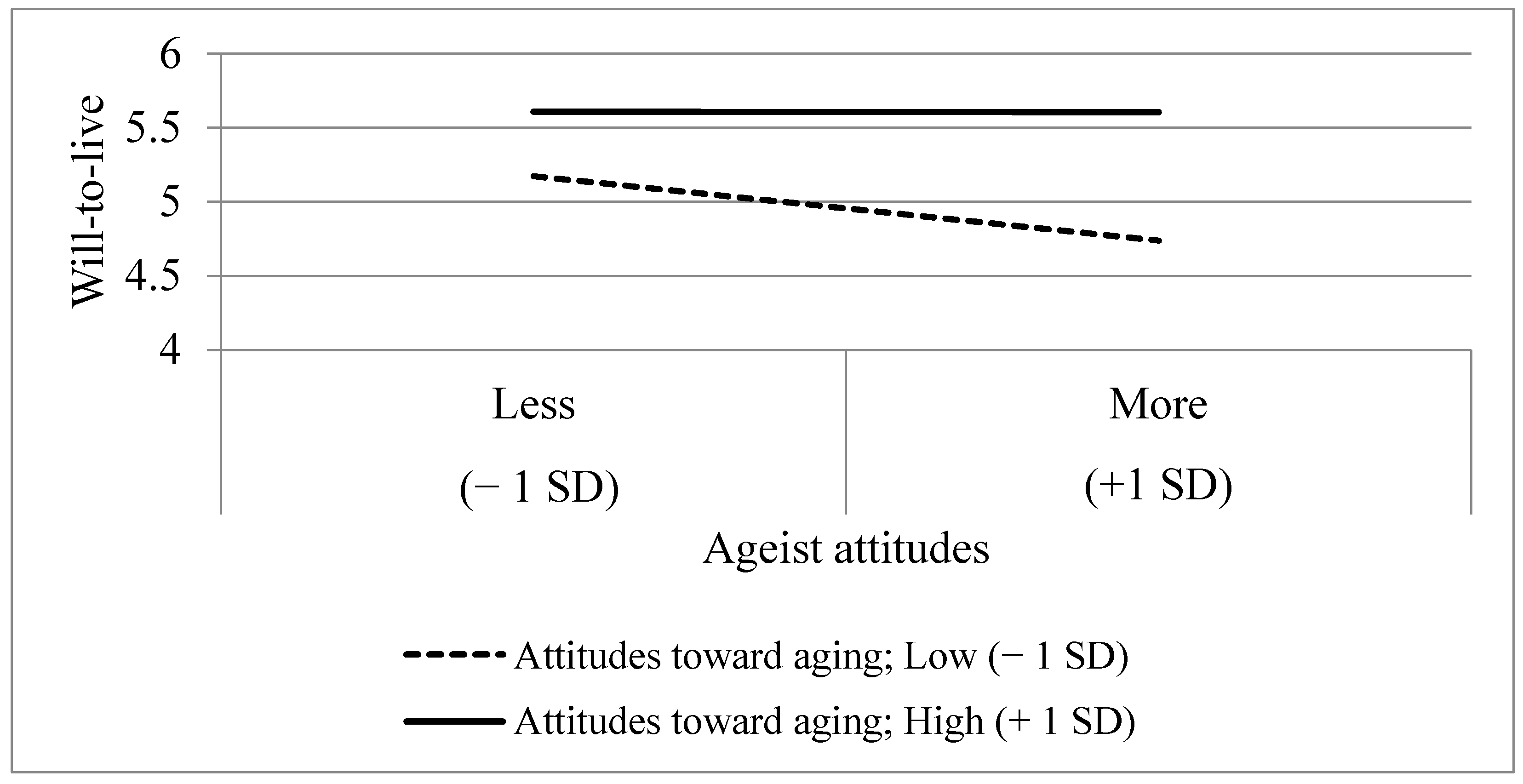
3.2. Results and Discussion
4. General Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carmel, S. The will to live: Gender differences among elderly persons. Soc. Sci. Med. 2001, 52, 949–958. [Google Scholar] [CrossRef]
- Izal, M.; Nuevo, R.; Montorio, I. Successful Aging and positive psychology: Two empirically related perspectives. OBM Geriatr. 2019, 3, 1–19. [Google Scholar] [CrossRef]
- Izal, M.; Bernabeu, S.; Martinez, H.; Bellot, A.; Montorio, I. Will to live as an expression of the well-being of older people. Rev. Esp. Geriatr. Gerontol. 2020, 55, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Shrira, A.; Carmel, S.; Tovel, H.; Raveis, V.H. Reciprocal relationships between the will-to-live and successful aging. Aging Ment. Health 2019, 23, 1350–1357. [Google Scholar] [CrossRef]
- Carmel, S.; Baron-Epel, O.; Shemy, G. The will-to-live and survival at old age: Gender differences. Soc. Sci. Med. 2007, 65, 518–523. [Google Scholar] [CrossRef]
- Karppinen, H.; Laakkonen, M.L.; Strandberg, T.E.; Tilvis, R.S.; Pitkälä, K.H. Will-to-live and survival in a 10-year follow-up among older people. Age Ageing 2012, 41, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Carmel, S. The will to live as an indicator of well-Being and predictor of survival in old age. In Understanding Well-Being in the Oldest Old; Poon, L.W., Cohen-Mansfield, J., Eds.; Cambridge University Press: New York, NY, USA, 2011; pp. 281–289. [Google Scholar] [CrossRef]
- Carmel, S.; Mutran, E. Wishes regarding the use of life-sustaining treatments among elderly persons in Israel: An explanatory model. Soc. Sci. Med. 1997, 45, 1715–1727. [Google Scholar] [CrossRef]
- Damron-Rodriguez, J.; Carmel, S. Exploring the will to live and distinguishing depression at end of life. Generations 2014, 38, 30–36. Available online: https://www.proquest.com/scholarly-journals/exploring-will-live-distinguishing-depression-at/docview/1640761956/se-2?accountid=44866 (accessed on 14 February 2021).
- Wurm, S.; Diehl, M.; Kornadt, A.E.; Westerhof, G.J.; Wahl, H.W. How do views on aging affect health outcomes in adulthood and late life? Explanations for an established connection. Dev. Rev. 2017, 46, 27–43. [Google Scholar] [CrossRef]
- Carmel, S. The will-to-live scale: Development, validation, and significance for elderly people. Aging Ment. Health 2017, 21, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.N. Age-ism: Another form of bigotry. Gerontologist 1969, 9, 243–246. [Google Scholar] [CrossRef]
- North, M.S.; Fiske, S.T. Resource scarcity and prescriptive attitudes generate subtle, intergenerational older-worker exclusion. J. Soc. Issues 2016, 72, 122–145. [Google Scholar] [CrossRef]
- June, A.; Segal, D.L.; Coolidge, F.L.; Klebe, K. Religiousness, social support and reasons for living in African American and European American older adults: An exploratory study. Aging Ment. Health 2009, 13, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.D.; Joiner, T.E. The interpersonal-psychological theory of suicidal behavior: Current status and future directions. J. Clin. Psychol. 2009, 65, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Ashman, O.; Dror, I. To be or not to be: The effects of aging stereotypes on the will to live. OMEGA-J. Death Dying 2000, 40, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.; Lima, M.L.; Abrams, D.; Swift, H. Will to live in older people’s medical decisions: Immediate and delayed effects of aging stereotypes. J. Appl. Soc. Psychol. 2014, 44, 399–408. [Google Scholar] [CrossRef]
- Zamir, A.; Granek, L.; Carmel, S. Factors affecting the will to live among elderly Jews living in Israel. Aging Ment. Health 2020, 24, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Brothers, A.; Kornadt, A.E.; Nehrkorn-Bailey, A.; Wahl, H.W.; Diehl, M. The Effects of Age Stereotypes on Physical and Mental Health are Mediated by Self-Perceptions of Aging. J. Gerontol. Ser. B 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.R.; Moffat, S.; Resnick, S.M.; Slade, M.D.; Ferrucci, L. Buffer against cumulative stress. GeroPsych 2016, 29, 141–146. [Google Scholar] [CrossRef]
- Levy, B.R.; Myers, L.M. Preventive health behaviors influenced by self-perceptions of aging. Prev. Med. 2004, 39, 625–629. [Google Scholar] [CrossRef]
- Levy, B.R.; Slade, M.D.; Chung, P.H.; Gill, T.M. Resiliency over time of elders’ age stereotypes after encountering stressful events. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 70, 886–890. [Google Scholar] [CrossRef]
- Officer, A.; Thiyagarajan, J.A.; Schneiders, M.L.; Nash, P.; de la Fuente-Núñez, V. Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related? Int. J. Environ. Res. Public Health 2020, 17, 3159. [Google Scholar] [CrossRef] [PubMed]
- Carmel, S. Gender differences and the will-to-live in old age. Przeglądlekarski 2012, 69, 49–53. [Google Scholar] [CrossRef]
- Levy, B. Stereotype embodiment: A psychosocial approach to aging. Curr. Dir. Psychol. Sci. 2009, 18, 332–336. [Google Scholar] [CrossRef]
- Levy, B.R. Eradication of ageism requires addressing the enemy within. Gerontologist 2001, 41, 578–579. [Google Scholar] [CrossRef]
- Levy, B.R.; Banaji, M.R. Implicit ageism. In Ageism: Stereotyping and Prejudice against Older Persons; Nelson, T.D., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 49–75. [Google Scholar]
- Losada-Baltar, A.; Jiménez-Gonzalo, L.; Gallego-Alberto, L.; Pedroso-Chaparro, M.D.S.; Fernandes-Pires, J.; Márquez-González, M. “We’re staying at home”. Association of self-perceptions of aging, personal and family resources and loneliness with psychological distress during the lock-down period of COVID-19. J. Gerontol. Ser. B 2020. [Google Scholar] [CrossRef]
- Marquet, M.; Chasteen, A.L.; Plaks, J.E.; Balasubramaniam, L. Understanding the mechanisms underlying the effects of negative age stereotypes and perceived age discrimination on older adults’ well-being. Aging Ment. Health 2019, 23, 1666–1673. [Google Scholar] [CrossRef]
- Westerhof, G.J.; Wurm, S. Subjective aging and health. In Oxford Research Encyclopedia of Psychology; Knight, B.G., Wahl, H.W., Eds.; Oxford University Press: Oxford, UK, 2018; pp. 1–30. [Google Scholar] [CrossRef]
- Bodner, E.; Bergman, Y.S.; Cohen-Fridel, S. Different dimensions of ageist attitudes among men and women: A multigenerational perspective. Int. Psychogeriatr. 2012, 24, 895–901. [Google Scholar] [CrossRef]
- Fraboni, M.; Saltstone, R.; Hughes, S. The Fraboni scale of ageism (FSA): An attempt at a more precise measure of ageism. Can. J. Aging 1990, 9, 55–56. [Google Scholar] [CrossRef]
- Bergman, Y.S.; Bodner, E. Ageist attitudes block young adults’ ability for compassion toward incapacitated older adults. Int. Psychogeriatr. 2015, 27, 1541–1550. [Google Scholar] [CrossRef]
- Bodner, E.; Shrira, A.; Hermesh, H.; Ben-Ezra, M.; Iancu, I. Psychiatrists’ fear of death is associated with negative emotions toward borderline personality disorder patients. Psychiatry Res. 2015, 228, 963–965. [Google Scholar] [CrossRef] [PubMed]
- Shrira, A.; Palgi, Y.; Ben-Ezra, M.; Spalter, T.; Kave, G.; Shmotkin, D. For better and for worse: The relationship between future expectations and functioning in the second half of life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2011, 66, 195–203. [Google Scholar] [CrossRef]
- Carmel, S.; Shrira, A.; Shmotkin, D. The will to live and death-related decline in life satisfaction. Psychol. Aging 2013, 28, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Nagi, S.Z. An epidemiology of disability among adults in the United States. Milbank Meml. Fund Q. 1976, 54, 439–467. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G.; Reno, R.R. Testing and probing three-way interactions. In Multiple Regression: Testing and Interpreting Interactions; Aiken, L.S., West, S.G., Reno, R.R., Eds.; Sage Publications: Newbury Park, CA, USA, 1991; pp. 49–61. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Janecková, H.; Dragomirecká, E.; Holmerová, I.; Vanková, H. The attitudes of older adults living in institutions and their caregivers to ageing. Cent. Eur. J. Public Health 2013, 21, 63–71. [Google Scholar] [CrossRef]
- Hayes, A.F. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- O’Brien, R.M. A caution regarding rules of thumb for variance inflation factors. Qual. Quant. 2007, 41, 673–690. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- North, M.S.; Fiske, S.T. A prescriptive intergenerational-tension ageism scale: Succession, identity, and consumption (SIC). Psychol. Assess. 2013, 25, 706–713. [Google Scholar] [CrossRef]
- Koren, E.; Shrira, A.; Bodner, E.; Bergman, Y.S. Subjective nearness-to-death and negative attitudes toward persons with disability: Attachment patterns moderate. Death Stud. 2020, 44, 312–318. [Google Scholar] [CrossRef]
- Laidlaw, K.; Kishita, N.; Shenkin, S.D.; Power, M.J. Development of a short form of the Attitudes to Ageing Questionnaire (AAQ). Int. J. Geriatr. Psychiatry 2018, 33, 113–121. [Google Scholar] [CrossRef]
- Shrira, A.; Ayalon, L.; Bensimon, M.; Bodner, E.; Rosenbloom, T.; Yadid, G. Parental post-traumatic stress disorder symptoms are related to successful aging in offspring of Holocaust survivors. Front. Psychol. 2017, 8, 1099. [Google Scholar] [CrossRef]
- Benyamini, Y.; Idler, E.L.; Leventhal, H.; Leventhal, E.A. Positive affect and function as influences on self-assessments of health expanding our view beyond illness and disability. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2000, 55, P107–P116. [Google Scholar] [CrossRef]
- Steele, C.M.; Aronson, J. Stereotype threat and the intellectual test performance of African Americans. J. Personal. Soc. Psychol. 1995, 69, 797–811. [Google Scholar] [CrossRef]
- Cuddy, A.J.; Fiske, S.T. Doddering but dear: Process, content, and function in stereotyping of older persons. In Ageism: Stereotyping and Prejudice against Older Persons; Nelson, T.D., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 3–26. [Google Scholar]
- Lamont, R.A.; Swift, H.J.; Abrams, D. A review and meta-analysis of age-based stereotype threat: Negative stereotypes, not facts, do the damage. Psychol. Aging 2015, 30, 180–193. [Google Scholar] [CrossRef]
- Steele, C.M. A threat in the air: How stereotypes shape intellectual identity and performance. Am. Psychol. 1997, 52, 613–629. [Google Scholar] [CrossRef]
- Barber, S.J.; Mather, M. Stereotype threat in older adults: When and why does it occur and who is most affected? In Oxford Library of Psychology. The Oxford Handbook of Emotion, Social Cognition, and Problem Solving in Adulthood; Verhaeghen, P., Hertzog, C., Eds.; Oxford University Press: Oxford, UK, 2014; pp. 302–319. [Google Scholar]
- Kang, S.K.; Chasteen, A.L. The moderating role of age-group identification and perceived threat on stereotype threat among older adults. Int. J. Aging Hum. Dev. 2009, 69, 201–220. [Google Scholar] [CrossRef]
- O’Brien, L.T.; Hummert, M.L. Memory performance of late middle–aged adults: Contrasting self–stereotyping and stereotype threat accounts of assimilation to age stereotypes. Soc. Cogn. 2006, 24, 338–358. [Google Scholar] [CrossRef]
- Bergman, Y.S.; Bodner, E.; Cohen-Fridel, S. Cross-cultural ageism: Ageism and attitudes toward aging among Jews and Arabs in Israel. Int. Psychogeriatr. 2013, 25, 6–15. [Google Scholar] [CrossRef]
- Beyer, A.K.; Wolff, J.K.; Freiberger, E.; Wurm, S. Are self-perceptions of ageing modifiable? Examination of an exercise programme with vs. without a self-perception of ageing-intervention for older adults. Psychol. Health 2019, 34, 661–676. [Google Scholar] [CrossRef]
- Wolff, J.K.; Schüz, B.; Ziegelmann, J.P.; Warner, L.M.; Wurm, S. Short-term buffers, but long-term suffers? Differential effects of negative self-perceptions of aging following serious health events. J. Gerontol. Ser. B 2017, 72, 408–414. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wolff, J.K.; Warner, L.M.; Ziegelmann, J.P.; Wurm, S. What do targeting positive views on ageing add to a physical activity intervention in older adults? Results from a randomised controlled trial. Psychol. Health 2014, 29, 915–932. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | M/% | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Ageism | 2.71 | 0.61 | - | |||||||
| 2. MC a | 1.76 | 1.53 | 0.08 * | - | ||||||
| 3. WTL | 5.43 | 0.82 | −0.14 *** | −0.29 *** | - | |||||
| 4. Age | 68.30 | 11.81 | 0.13 *** | 0.40 *** | −0.33 *** | - | ||||
| 5. Gender b | 53.9% | - | 0.02 | 0.05 | 0.06 | 0.03 | - | |||
| 6. Marital status c | 74.1% | - | −0.02 | −0.17 *** | −0.13 ** | −0.26 *** | −0.26 *** | - | ||
| 7. Children | 3.00 | 1.53 | 0.003 | −0.01 | 0.06 *** | 0.06 | −0.07 | 0.17 *** | - | |
| 8. Employment d | 50.3% | - | 0.08 * | 0.34 *** | −0.24 *** | 0.66 *** | 0.17 *** | −0.22 *** | 0.09 * | |
| 9. FI e | 1.78 | 1.00 | 0.14 ** | 0.40 *** | −0.34 *** | 0.48 | 0.11 ** | −0.20 *** | 0.10 ** | −0.35 *** |
| B | Β | p | |
|---|---|---|---|
| Step 1: Covariates (∆R2 = 0.140) | |||
| Gender a | 0.049 | 0.028 | 0.511 |
| Marital status b | 0.132 | 0.070 | 0.115 |
| Children | −0.1 | −0.02 | 0.604 |
| Unemployment c | −0.12 | −0.07 | 0.121 |
| Functional impairment | −0.26 | −0.33 | 0.000 |
| Step 2: Main effects (∆R2 = 0.041) | |||
| Age | −0.013 | −0.138 | 0.011 |
| Medical conditions | −0.084 | −0.157 | 0.000 |
| Ageist attitudes | −0.128 | −0.089 | 0.027 |
| Step 3: Two-way interactions (∆R2 = 0.014) | |||
| Age X Medical conditions | −0.022 | −0.025 | 0.533 |
| Age X Ageist attitudes | −0.045 | −0.054 | 0.186 |
| Ageism X Medical conditions | −0.086 | −0.094 | 0.022 |
| Step 4: Three-way interaction (∆R2 = 0.013) | |||
| Age X Medical conditions X Ageist attitudes | −0.102 | −0.118 | 0.004 |
| R2= 0.207 | |||
| Variables | M/% | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Ageism | 2.49 | 0.74 | - | ||||||||
| 2. ATA a | 3.69 | 0.62 | −0.24 *** | - | |||||||
| 3. WTL | 5.24 | 0.79 | −0.25 *** | 0.46 *** | - | ||||||
| 4. Age | 72.11 | 10.12 | 0.12 * | −0.05 | −0.07 | - | |||||
| 5. Gender b | 53.6% | - | −0.04 | −0.09 | −0.06 | 0.12 * | - | ||||
| 6. Marital status c | 74.5% | - | −0.04 | 0.18 ** | 0.10 | −0.94 | −0.23 *** | - | |||
| 7. Children | 3.27 | 1.23 | 0.07 | 0.04 | 0.00 | −0.09 | −0.03 | 0.19 ** | - | ||
| 8. Subjective health | 3.82 | 0.87 | −0.30 *** | 0.44 *** | 0.39 *** | 0.033 | −0.04 | 0.17 ** | −0.04 | - | |
| 9. Unemployment d | 54.4% | - | 0.29 * | −0.17 ** | −0.20 *** | 0.09 | −0.11 * | −0.14 * | −0.03 | −0.31 *** | - |
| 10. FI e | 1.69 | 0.98 | 0.25 ** | −0.17 ** | −0.16 ** | 0.08 | −0.13 * | −0.16 ** | 0.05 | −0.39 *** | 0.15 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gvili, R.-L.; Bodner, E. Ageist Attitudes Are Associated with Will-to-Live and Moderated by Age, Medical Conditions and Attitudes toward Aging. Int. J. Environ. Res. Public Health 2021, 18, 6736. https://doi.org/10.3390/ijerph18136736
Gvili R-L, Bodner E. Ageist Attitudes Are Associated with Will-to-Live and Moderated by Age, Medical Conditions and Attitudes toward Aging. International Journal of Environmental Research and Public Health. 2021; 18(13):6736. https://doi.org/10.3390/ijerph18136736
Chicago/Turabian StyleGvili, Racheli-Lital, and Ehud Bodner. 2021. "Ageist Attitudes Are Associated with Will-to-Live and Moderated by Age, Medical Conditions and Attitudes toward Aging" International Journal of Environmental Research and Public Health 18, no. 13: 6736. https://doi.org/10.3390/ijerph18136736
APA StyleGvili, R.-L., & Bodner, E. (2021). Ageist Attitudes Are Associated with Will-to-Live and Moderated by Age, Medical Conditions and Attitudes toward Aging. International Journal of Environmental Research and Public Health, 18(13), 6736. https://doi.org/10.3390/ijerph18136736