
Is Pollution a Cost to Health? Theoretical and Empirical Inquiry for the World’s Leading Polluting Economies



Abstract
1. Introduction
2. Literature Review
Research Gap and Objectives of the Study
3. Materials and Methods
3.1. Rationale of the Study
3.2. Theoretical Model
3.3. Data and Methodology for Empirical Verifications
3.4. Cointegration and Error Correction Mechanism
3.5. Granger Causality Test
4. Empirical Results
5. Discussion
6. Conclusions and Future Research Agenda
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agras, J.; Chapman, D. A Dynamic Approach to the Environmental Kuznets Curve hypothesis. Ecol. Econ. 1999, 28, 267–277. [Google Scholar] [CrossRef]
- Nemat, S. Economic development and environmental quality: An econometric analysis. Oxf. Econ. Pap. 1994, 46, 757–773. [Google Scholar]
- Dinda, S.; Coondoo, D.; Pal, M. Air Quality and Economic Growth: An Empirical Study. Ecol. Econ. 2000, 34, 409–423. [Google Scholar] [CrossRef]
- Narayan, P.K.; Narayan, S. Does environmental quality influence health expenditures? Empirical evidence from a panel of selected OECD countries. Ecol. Econ. 2008, 65, 367–374. [Google Scholar] [CrossRef]
- Balgati, B.H.; Moscone, F. Health care expenditure and income in the OECD reconsidered: Evidence from panel data. Econ. Model. 2010, 27, 804–811. [Google Scholar]
- Lieb, C.M. The Environmental Kuznets Curve and Flow versus Stock Pollution: The Neglect of Future Damages. Environ. Resour. Econ. 2004, 29, 483–506. [Google Scholar] [CrossRef]
- Bloom, D.E.; Canning, D. Policy forum: Public health. The health and wealth of nations. Science 2000, 287, 1207–1209. [Google Scholar] [CrossRef] [PubMed]
- WHO. Investing in Health for Economic Development. National Macroeconomics and Health (CMH) Reports. 2004. Available online: https://www.who.int/macrohealth/action/sintesis15novingles.pdf?ua=1 (accessed on 5 November 2020).
- Bleakley, H. Health, Human Capital, and Development. Annu. Rev. Econ. 2010, 2, 283–310. [Google Scholar] [CrossRef]
- Raghupathi, V.; Raghupathi, W. Healthcare Expenditure and Economic Performance: Insights from the United States Data. Front. Public Health 2020, 8, 156. [Google Scholar] [CrossRef]
- Mankiw, N.G.; Romer, D.; Weil, D.N. A contribution to the empirics of economic growth. Q. J. Econ. 1992, 107, 407–437. [Google Scholar] [CrossRef]
- Benhabib, J.; Spiegel, M.M. The role of human capital in economic development evidence from aggregate cross-country data. J. Monet. Econ. 1994, 34, 143–173. [Google Scholar] [CrossRef]
- Chang, K.; Ying, Y. Economic Growth, Human Capital Investment, and Health Expenditure: A Study of OECD Countries. Hitotsubashi J. Econ. 2006, 47, 1–16. [Google Scholar]
- Baldacci, E.; Clements, B.; Gupta, S.; Cui, Q. Social spending, human capital, and growth in developing countries. World Dev. 2008, 36, 1317–1341. [Google Scholar] [CrossRef]
- Pelinescu, E. The Impact of Human Capital on Economic Growth. Procedia Econ. Financ. 2015, 22, 184–190. [Google Scholar] [CrossRef]
- Grossman, G.M.; Krueger, A.B. Environmental Impacts of a North American Free Trade Agreement; Working Paper 3914; National Bureau of Economic Research (NBER): Cambridge, MA, USA, 1991. [Google Scholar] [CrossRef]
- Lago-Peñas, S.; Cantarero-Prieto, D.; Blázquez-Fernández, C. On the relationship between GDP and health care expenditure: A new look. Econ. Model. 2013, 32, 124–129. [Google Scholar] [CrossRef]
- Chaabouni, S.; Zghidi, N.; Mbarek, M.B. On the causal dynamics between CO 2 emissions, health expenditures and economic growth. Sustain. Cities Soc. 2016, 22, 184–191. [Google Scholar] [CrossRef]
- Yu, Y.; Zhang, L.; Zheng, X. On the nexus of environmental quality and public spending on health care in China: A panel cointegration analysis. Econ. Political Stud. 2016, 4, 319–331. [Google Scholar] [CrossRef]
- Lu, W.-C. Greenhouse Gas Emissions, Energy Consumption and Economic Growth: A Panel Cointegration Analysis for 16 Asian Countries. Int. J. Environ. Res. Public Health 2017, 14, 1436. [Google Scholar] [CrossRef] [PubMed]
- Sterpu, M.; Soava, G.; Mehedintu, A. Impact of Economic Growth and Energy Consumption on Greenhouse Gas Emissions: Testing Environmental Curves Hypotheses on EU Countries. Sustainability 2018, 10, 3327. [Google Scholar] [CrossRef]
- Usman, M.; Ma, Z.; Wasif Zafar, M.; Haseeb, A.; Ashraf, R.U. Are Air Pollution, Economic and Non-Economic Factors Associated with Per Capita Health Expenditures? Evidence from Emerging Economies. Int. J. Env. Res. Public Health 2019, 16, 1967. [Google Scholar] [CrossRef]
- Pi, T.; Wu, H.; Li, X. Does Air Pollution Affect Health and Medical Insurance Cost in the Elderly: An Empirical Evidence from China. Sustainability 2019, 11, 1526. [Google Scholar] [CrossRef]
- Liao, Q.; Jin, W.; Tao, Y.; Qu, J.; Li, Y.; Niu, Y. Health and Economic Loss Assessment of PM2.5 Pollution during 2015–2017 in Gansu Province, China. Int. J. Environ. Res. Public Health 2020, 17, 3253. [Google Scholar] [CrossRef]
- To, A.H.; Ha, D.T.-T.; Nguyen, H.M.; Vo, D.H. The Impact of Foreign Direct Investment on Environment Degradation: Evidence from Emerging Markets in Asia. Int. J. Env. Res. Public Health 2019, 16, 1636. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Shi, J.; Wu, Q. Environmental Kuznets Curve: Empirical Relationship between Energy Consumption and Economic Growth in Upper-Middle-Income Regions of China. Int. J. Env. Res. Public Health 2020, 17, 6971. [Google Scholar] [CrossRef]
- An, J.; Heshmati, A. The relationship between air pollutants and healthcare expenditure: Empirical evidence from South Korea. Environ. Sci. Pollut. Res. 2019, 26, 31730–31751. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Ding, L.; Zhang, Q.; Na, J.; Cheng, J. Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities. Int. J. Env. Res. Public Health 2020, 17, 990. [Google Scholar] [CrossRef]
- Lucas, R.E., Jr. On the mechanics of economic development. J. Monet. Econ. 1988, 22, 3–42. [Google Scholar] [CrossRef]
- Romer, P. Human Capital and Growth: Theory and Evidence; NBER Working Paper No. 3173; National Bureau of Economic Research: Cambridge, MA, USA, 1989. [Google Scholar]
- Barro, J.R. Human capital and growth in cross-country regressions. Q. J. Econ. 1991, 106, 407–443. [Google Scholar] [CrossRef]
- Ramsey, F.P. A Mathematical Theory of Saving. Econ. J. 1928, 38, 543–559. [Google Scholar] [CrossRef]
- Cass, D. Optimum Growth in an Aggregative Model of Capital Accumulation. Rev. Econ. Stud. 1965, 32, 233–240. [Google Scholar] [CrossRef]
- Koopmans, T.C. On the Concept of Optimal Economic Growth. In The Economic Approach to Development Planning; Rand McNally: Chicago, IL, USA, 1965; pp. 225–287. [Google Scholar]
- Dickey, D.A.; Fuller, W.A. Distribution of the estimators of autoregressive time series with a unit root. J. Am. Stat. Assoc. 1979, 74, 427–431. [Google Scholar]
- Engle, R.F.; Granger, C.W. Co-integrationand error correction: Representation, estimationand testing. Econometrica 1987, 55, 251–276. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating causal relations by econometric models and cross spectral-methods. Econometrica 1969, 37, 424–438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
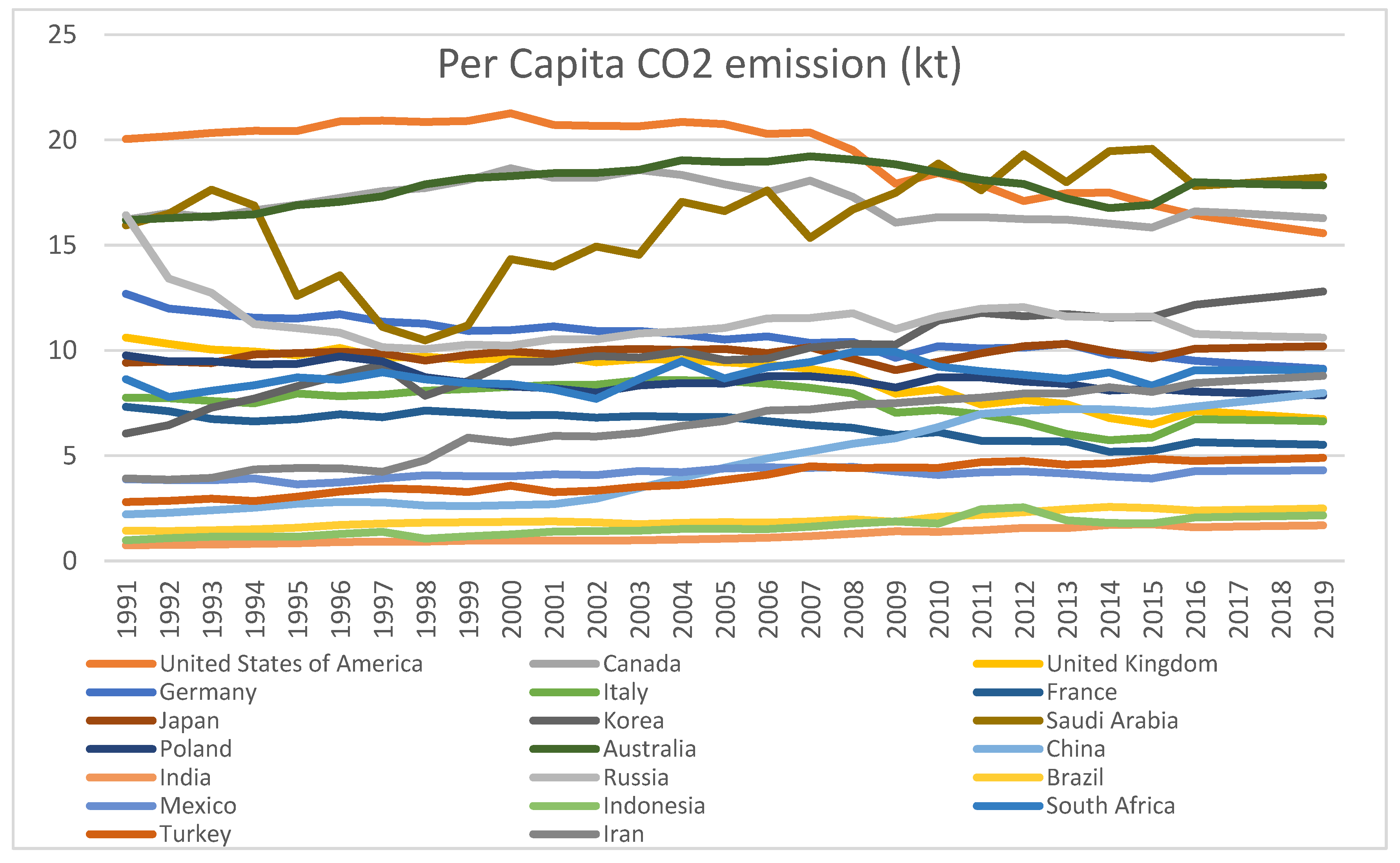
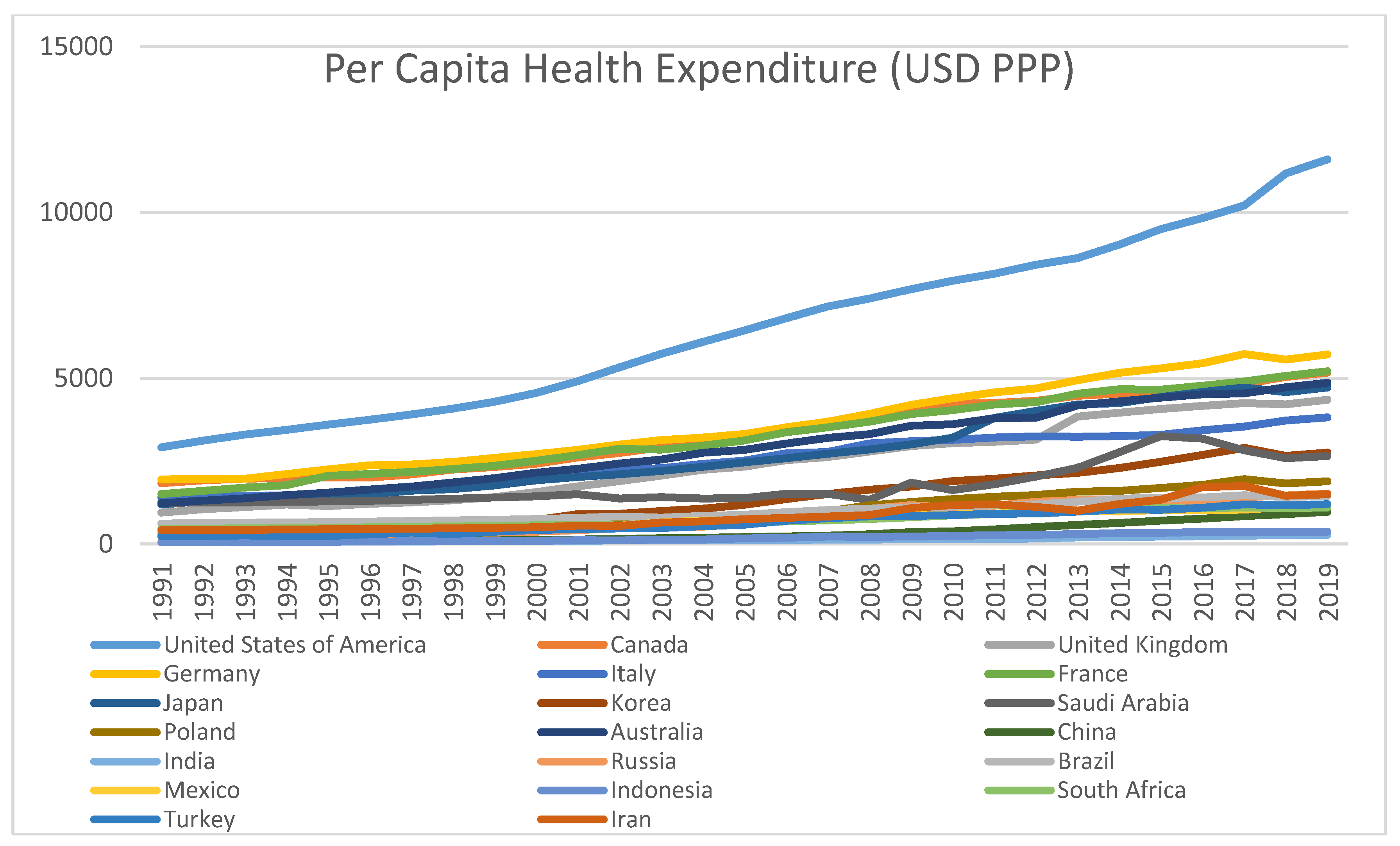
| Country | Average (PCCO2) | SD (PCCO2) | Average (PHEXP) | SD (PHEXP) | Correlation Coefficient | t Values (p) |
|---|---|---|---|---|---|---|
| United States of America | 6516 | 2601.632 | 19.21363 | 1.861279 | −0.89415 | −10.37 (0.01) |
| Canada | 3334 | 1126.657 | 17.06334 | 0.88801 | −0.46232 | −2.709 (0.05) |
| United Kingdom | 2464 | 1161.124 | 8.758151 | 1.289833 | −0.96192 | −18.28 (0.01) |
| Germany | 3625 | 1284.053 | 10.64438 | 0.88965 | −0.9453 | −15.05 (0.01) |
| Italy | 2534 | 785.431 | 7.514357 | 0.856867 | −0.63267 | −4.245 (0.01) |
| France | 3287 | 1170.555 | 6.38005 | 0.649456 | −0.91989 | −12.18 (0.01) |
| Japan | 2760 | 1219.106 | 9.850593 | 0.298101 | 0.432676 | 2.493 (0.05) |
| Korea | 1382 | 848.6826 | 9.933926 | 1.83271 | 0.936752 | 13.907 (0.01) |
| Saudi Arabia | 1772 | 632.222 | 16.18668 | 2.54894 | 0.595657 | 3.853 (0.05) |
| Poland | 989 | 557.6097 | 8.631876 | 0.572912 | −0.72773 | −5.513 (0.01) |
| Australia | 2930 | 1178.464 | 17.84431 | 0.920926 | 0.317275 | 1.738 (0.06) |
| China | 331 | 284.2651 | 4.727953 | 2.112316 | 0.931261 | 13.281 (0.01) |
| India | 134 | 66.95031 | 1.190575 | 0.338213 | 0.949835 | 15.780 (0.01) |
| Russia | 772 | 468.893 | 11.35594 | 1.238982 | −0.12432 | −0.651 (0.2) |
| Brazil | 976 | 294.9416 | 1.961122 | 0.353308 | 0.94661 | 15.257 (0.01) |
| Mexico | 705 | 275.2264 | 4.112457 | 0.219916 | 0.650419 | 4.449 (0.01) |
| Indonesia | 186 | 112.3897 | 1.601843 | 0.428217 | 0.877965 | 9.529 (0.01) |
| South Africa | 730 | 234.0077 | 8.793801 | 0.542375 | 0.410325 | 2.337 (0.05) |
| Turkey | 656 | 336.5572 | 3.920033 | 0.734984 | 0.973712 | 22.212 (0.01) |
| Iran | 853 | 419.4096 | 6.472487 | 1.658229 | 0.909682 | 11.381 (0.01) |
| Developed Countries | Developing Countries | ||||||
|---|---|---|---|---|---|---|---|
| Country | ADF(Prob) PCHEXP | ADF(Prob) PCCO2 | Remarks | Country | ADF(Prob) PCHEXP | ADF(Prob) PCCO2 | Remarks |
| United States of America | −3.8 (0.01) | −4.9 (0.00) | S at 1st ∆ | China | −4.2 (0.00) | −4.7 (0.00) | S at 2nd ∆ |
| Canada | −3.0 (0.05) | −4.8 (0.00) | S at 1st ∆ | India | −3.3 (0.02) | −4.9 (0.00) | S at 1st ∆ |
| United Kingdom | −4.9 (0.00) | −6.8 (0.00) | S at 1st ∆ | Russia | −3.7 (0.00) | −6.6 (0.00) | S at 1st ∆ |
| Germany | −4.7 (0.00) | −8.4 (0.00) | S at 1st ∆ | Brazil | −4.9 (0.00) | −4.7 (0.00) | S at 1st ∆ |
| Italy | −4.5 (0.00) | −4.0 (0.00) | S at 1st ∆ | Mexico | −4.5 (0.00) | −5.4 (0.00) | S at 1st ∆ |
| France | −5.5 (0.00) | −5.5 (0.00) | S at 1st ∆ | Indonesia | −5.5 (0.00) | −5.3 (0.00) | S at 1st ∆ |
| Japan | −3.8 (0.00) | −4.7 (0.00) | S at 1st ∆ | South Africa | −3.5 (0.04) | −6.4 (0.00) | S at 1st ∆ |
| Korea | −4.8 (0.00) | −4.9 (0.00) | S at 1st ∆ | Turkey | −5.0 (0.00) | −5.7 (0.00) | S at 1st ∆ |
| Saudi Arabia | −4.2 (0.00) | −3.1 (0.04) | S at 1st ∆ | Iran | −9.1 (0.00) | −6.2 (0.00) | S at 1st ∆ |
| Poland | −5.2 (0.00) | −4.6 (0.00) | S at 1st ∆ | ||||
| Australia | −7.3 (0.00) | −3.3 (0.02) | S at 1st ∆ | ||||
| Developed Countries | Developing Countries | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Country | LR Reg. Coef. (Prob) | ADF of Error (Prob) | EC Terms | Remarks on Whether Cointegration Exists | Country | LR Reg. Coef. (Prob) | ADF of Error (Prob) | EC Terms | Remarks on Whether Cointegration Exists |
| United States of America | −1249 (0.00) | −3.3 (0.01) | 0.04 (0.1) Errors not corrected | Yes | China | - | - | - | - |
| Canada | −586 (0.01) | −1.6 (0.46) | - | No | India | 230 (0.00) | −3.4 (0.01) | −0.05 (0.4) Errors not corrected | Yes |
| United Kingdom | −865 (0.00) | −2.9 (0.05) | −0.1 (0.3) Errors not corrected | Yes | Russia | −47 (0.56) | 0.79 (0.9) | - | No |
| Germany | −1364 (0.00) | −3.8 (0.00) | −0.14 (0.07) Errors are corrected | Yes | Brazil | 790 (0.00) | −2.98 (0.05) | −0.1 (0.2) Errors not corrected | Yes |
| Italy | −579 (0.00) | −4.8 (0.00) | 0.03 (0.3) Errors not corrected | Yes | Mexico | 814 (0.00) | −1.2 (0.6) | - | No |
| France | −1657 (0.00) | −2.86 (0.06) | −0.02 (0.7) Errors not corrected | Yes | Indonesia | 230 (0.00) | −3.6 (0.01) | −0.05 (0.4) Errors not corrected | Yes |
| Japan | 1769 (0.01) | −0.88 (0.7) | - | No | South Africa | 177 (0.02) | −0.85 (0.7) Errors not corrected | - | No |
| Korea | 433 (0.00) | −2.9 (0.06) | −0.10 (0.2) Errors not corrected | Yes | Turkey | 446 (0.00) | −2.99 (0.05) | −0.27 (0.02) Errors corrected | Yes |
| Saudi Arabia | 147 (0.00) | −2.9 (0.05) | −0.11 (0.1) Errors not corrected | Yes | Iran | 230 (0.00) | −2.98 (0.05) | −0.23 (0.05) Errors corrected | Yes |
| Poland | −708 (0.00) | −1.1 (0.7) | - | No | |||||
| Australia | 406 (0.05) | 0.99 (0.9) | - | No | |||||
| Developed Countries H0: Pollution Doesn’t Cause Health Exp H1: Health Exp Doesn’t Cause Pollution | Developing Countries H0: Pollution Doesn’t Cause Health Exp H1: Health Exp Doesn’t Cause Pollution | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Country | F Stat | Prob. | Lag | Remarks | Country | F Stat | Prob. | Lag | Remarks |
| USA | 0.00 2.31 | 0.99 0.13 | 2,2 | No way causality | China | 0.21 1.18 | 0.88 0.34 | 3,3 | No way causality |
| Canada | 5.38 3.61 | 0.01 0.04 | 2,2 | Bidirectional causality | India | 0.16 3.49 | 0.91 0.03 | 3,3 | d(HExp) → d(CO2) |
| UK | 4.41 1.01 | 0.04 0.32 | 1,1 | d(HExp) → d(CO2) | Russia | 1.71 1.00 | 0.20 0.38 | 2,2 | No way causality |
| Germany | 0.03 0.66 | 0.58 0.99 | 3,3 | No way causality | Brazil | 0.37 1.41 | 0.69 0.26 | 2,2 | No way causality |
| Italy | 3.32 1.67 | 0.05 0.21 | 2,2 | d(CO2) → d(HExp) | Mexico | 0.72 0.11 | 0.55 0.95 | 3,3 | No way causality |
| France | 1.90 1.74 | 0.16 0.19 | 3,3 | No way causality | Indonesia | 1.61 0.02 | 0.21 0.87 | 1,1 | No way causality |
| Japan | 6.65 0.73 | 0.00 0.49 | 2,2 | d(CO2) → d(HExp) | S Africa | 0.99 3.25 | 0.32 0.08 | 1,1 | d(HExp) → d(CO2) |
| S Korea | 2.92 0.42 | 0.07 0.73 | 3,3 | d(CO2) → d(HExp) | Turkey | 1.86 3.25 | 0.17 0.04 | 3,3 | d(HExp) → d(CO2) |
| S Arabia | 1.42 0.02 | 0.24 0.87 | 1,1 | No way causality | Iran | 1.04 0.07 | 0.36 0.93 | 2,2 | No way causality |
| Poland | 0.16 0.73 | 0.92 0.54 | 3,3 | No way causality | |||||
| Australia | 4.53 0.22 | 0.04 0.63 | 1,1 | d(CO2) → d(HExp) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, R.C.; Ivaldi, E. Is Pollution a Cost to Health? Theoretical and Empirical Inquiry for the World’s Leading Polluting Economies. Int. J. Environ. Res. Public Health 2021, 18, 6624. https://doi.org/10.3390/ijerph18126624
Das RC, Ivaldi E. Is Pollution a Cost to Health? Theoretical and Empirical Inquiry for the World’s Leading Polluting Economies. International Journal of Environmental Research and Public Health. 2021; 18(12):6624. https://doi.org/10.3390/ijerph18126624
Chicago/Turabian StyleDas, Ramesh Chandra, and Enrico Ivaldi. 2021. "Is Pollution a Cost to Health? Theoretical and Empirical Inquiry for the World’s Leading Polluting Economies" International Journal of Environmental Research and Public Health 18, no. 12: 6624. https://doi.org/10.3390/ijerph18126624
APA StyleDas, R. C., & Ivaldi, E. (2021). Is Pollution a Cost to Health? Theoretical and Empirical Inquiry for the World’s Leading Polluting Economies. International Journal of Environmental Research and Public Health, 18(12), 6624. https://doi.org/10.3390/ijerph18126624