
Prevalence of SARS-CoV-2 Infection at the University of Barcelona during the Third COVID-19 Pandemic Wave in Spain

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
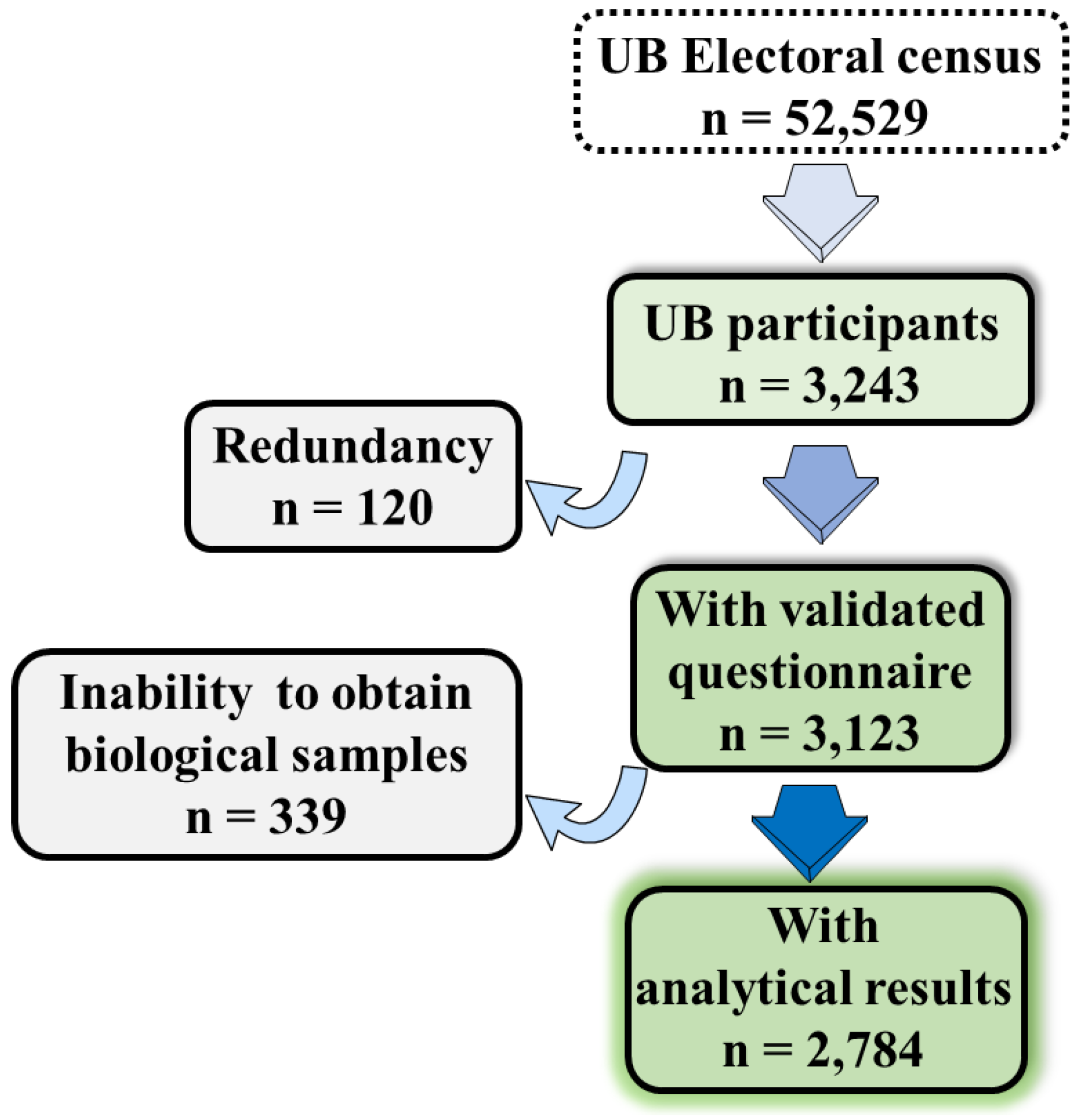
2.1. Study Design and Participants
2.2. Logistics Procedure
2.3. Sample Collection
2.4. SARS-CoV-2 Detection by RT-PCR
2.5. Detection of SARS-CoV-2 Antibodies
2.6. Statistical Analysis
2.7. Role of the Funding Source
3. Results
3.1. Baseline Characteristics
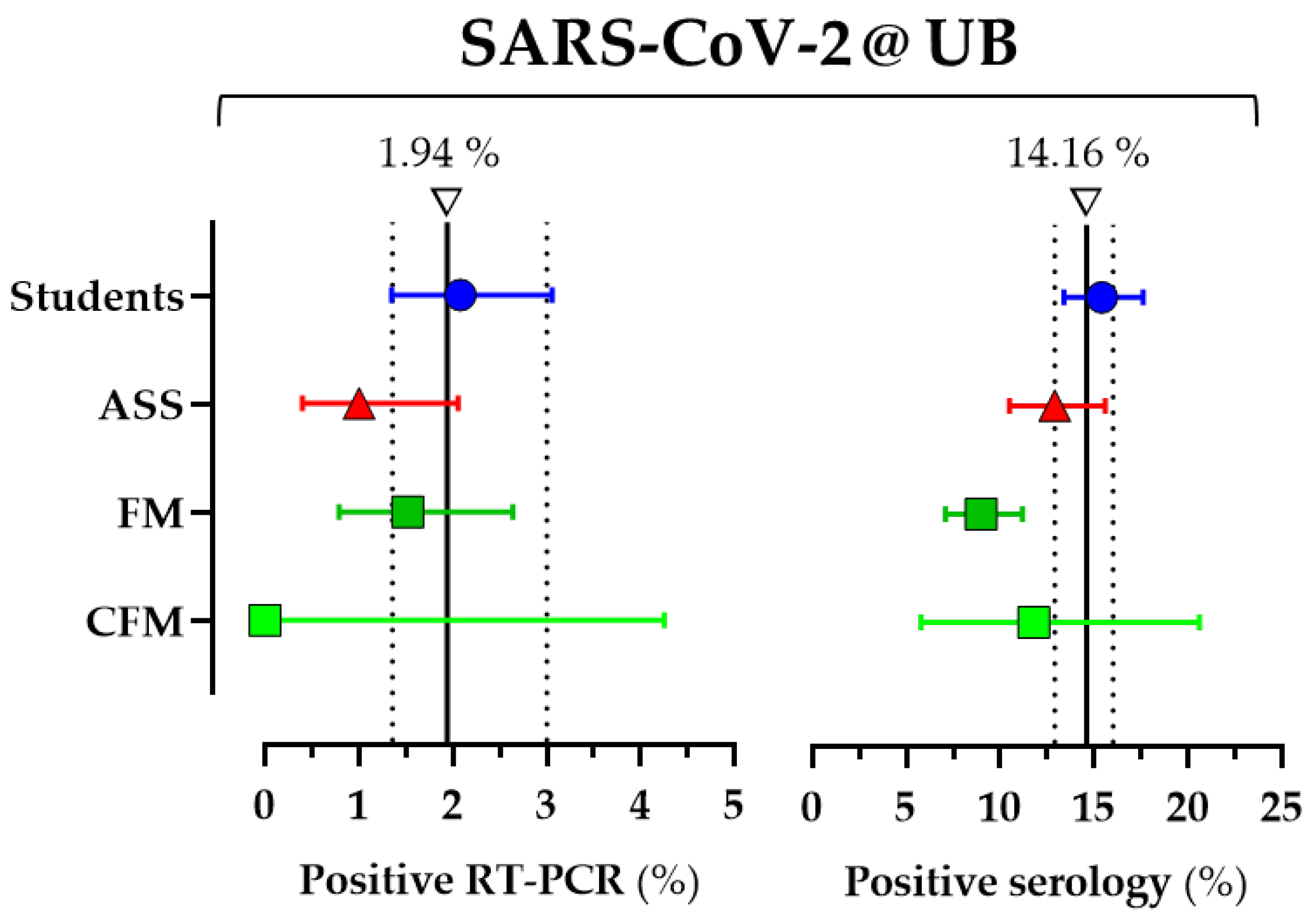
3.2. SARS-CoV-2 Infection Prevalence
3.3. Asymptomatic COVID Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Sociodemographic | •Age |
| •Gender | |
| •Collective UB (student, faculty, administrative) | |
| •Weight | |
| •Height | |
| •Level of studies | |
| Clinical background | •Cancer |
| •Cardiovascular disease (includes hypertension) | |
| •Endocrine disease (includes diabetes) | |
| •Immunocompromised | |
| •Liver diseases | |
| •Pulmonary disease | |
| •Renal disease | |
| Background SARS-CoV-2 infection | •No / suspected / confirmed |
| In case of suspected or confirmed: | |
| •Date of first symptom | |
| •Symptoms (fever, chills, severe tiredness, sore throat, cough, arthralgia, shortness of breath, heada che, anosmia or ageusia, and nausea, vomiting, or diarrhoea) sore throat, cough, arthralgia, shortness | |
| Previous screening for SARS-CoV-2 | •Previous screening for SARS-CoV-2 |
| •PCR (date, positive/negative) | |
| •Serology (date, positive/negative) | |
| Risk of SARS-CoV-2 infection | Direct contact/s with people with COVID |
| Lifestyles | •Alcohol (previous / during pandemic) |
| •Smoke tobacco (previous / during pandemic) | |
| •Other drugs |
| University of Barcelona: |
| Amparo Asensi, Montse Bachs, Maria Dolors Baena, Silvia Costa Abós, Cristina Cruz Gómez, Antoni Forés, Ester Fusté Domínguez, Rocio Escobar Miranda, Antonio Gar-cía-Honrubia, Anna Gargallo, Eva Garrido, Isabella Gastalgo, Miquel Lizandra, José López López, Maria Antonia Martínez Momblan, Vinyet Robles, Xavier Roca, José L. Rosa-López, Josep Maria Sierra Artigosa, Gonzalo Silva-Robledo, Avelina Tortosa, An-toni Trilla-García, Marta Valle, |
| Gerència Territorial Metropolitana Sud (GTMS): |
| Encarna Grifell-Martín |
| Clinical Research Support Unit-[HUB·IDIBELL]: |
| Thiago Carnaval |
| Information and Communication Technologies Department-Catalan Institute of Health: |
| Pau Casals-Villena, Manel Domingo-Rodríguez, Nacho Nieto |
| Bellvitge University Hospital: |
| Anna Carrera-Salinas, Aida González-Díaz, Daniel Vázquez-Sánchez |
| UICEC-Bellvitge University Hospital: |
| Ana Gainza, Angela Garrido, Pilar Hereu, Nadia Llavero, Eva Llosa, Mireia Santllorente |
| Nursing-University of Barcelona: |
| Sonia Aguirre Álvarez, Sergio Alonso, Mónica Tania Anguita Amador, Sonia Ayuso Margañón, Nadia Azzouz Balich, Núria Campanera Moliné, Carmen Cañas Aranda, Jessica Castaño Camuñez, Paloma Castillo, Alba Cuartero, Joan Maria Estrada Masllorens, Anabelen Fernández-Cervilla, Daniela C. de Freitas-Vieira, Elvira García Carulla, Verónica Gimenez Villa, Julia González Vaca, Marta González Martínez, Eva M. Guix-Comellas, Ana Lanau Roig, Cristina Laserna-Jiménez, Nerea Latorre Feliu, Mireia Lopez-Poyato, Laura Manzano-Benito, Laura Martin-Moreno, Eugenia Mellado-Pau, Paloma Pifarre Montaner, José M. Montero, Sabah L. el Morabiti, Marta del Moral, Yolanda Martos, M. Carmen Olmos Palenzuela, Marc Pañero, Celine Primiceri-Sánchez, Angela Puchercos Ferrer, Andrea Roman-Martinez, Andrea Recacha Robredo, Carlota Riba, Marta Romero García, Samuel Romero Martínez, Antonio Rosa Castillo, Anabelen Rubio, José Luis Sánchez-Ceba, José A. Sarria-Guerrero, Cristina Sanz Mellado, Angeles Saz Roy, Sara Tejero Bernardo, Gloria Timoneda-Gracia, Andrea Urbina Moral |
| Oficina de Seguretat, Salut i Medi Ambient (OSSMA)—University of Barcelona: |
| Begoña Castillejos, Oriol Grasas-Llorens, Mariona Mas-Calderer, Pedro Moreno Arribas, Susana Sánchez Redondo, Xavi Trullàs Escoda, |
References
- Qian, G.; Yang, N.; Yan Ma, A.H.; Wang, L.; Li, G.; Chen, X.; Chen, X. COVID-19 transmission within a family cluster by presymptomatic carriers in China. Clin. Infect. Dis. 2020, 71, 861–862. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID. JAMA J. Am. Med. Assoc. 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Zhu, J.; Zhang, Z.; Han, Y. A familial cluster of infection associated with the 2019 novel coronavirus indicating possible person-to-person transmission during the incubation period. J. Infect. Dis. 2020, 221, 1757–1761. [Google Scholar] [CrossRef] [PubMed]
- Lennon, N.J.; Bhattacharyya, R.P.; Mina, M.J.; Rehm, H.L.; Hung, D.T.; Smole, S.; Woolley, A.; Lander, E.S.; Gabriel, S.B. Comparison of viral levels in individuals with or without symptoms at time of COVID-19 testing among 32,480 residents and staff of nursing homes and assisted living facilities in Massachusetts. medRxiv 2020. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed]
- DePietro, A. Here’s a Look at the Impact of Coronavirus (COVID-19) on Colleges and Universities in the U.S. Forbes. 2020. Available online: https://www.forbes.com/sites/andrewdepietro/2020/04/30/impact-coronavirus-covid-19-colleges-universities/?sh=3cec556161a6 (accessed on 5 April 2021).
- Cupertino, F.; Spataro, S.; Spinelli, G.; Schirinzi, A.; Bianchi, F.P.; Stefanizzi, P.; Di Serio, F.; Tafuri, S. The university as a safe environment during the SARS-COV-2 pandemic: The experience of Bari Politecnico. Ann. Ig. 2021, 33, 201–202. [Google Scholar] [PubMed]
- Rankings—Universitat de Barcelona. Available online: https://www.ub.edu/web/ub/en/universitat/la_ub_avui/ranquings/index.html? (accessed on 5 April 2021).
- The University of Barcelona in Figures. Available online: http://www.ub.edu/gtr/documents/xifres/UBenXifres_ANG.pdf (accessed on 5 April 2021).
- University of Barcelona Associated Hospitals. Available online: http://www.ub.edu/medicina/campus2/altres.htm (accessed on 5 April 2021).
- University of Barcelona Faculties and Centers. Available online: https://www.ub.edu/web/portal/en/the-ub/campus/faculties/ (accessed on 5 April 2021).
- Parc Científic de Barcelona. Available online: https://www.pcb.ub.edu/en/ (accessed on 5 April 2021).
- Research Institutes and Research Centres—Universitat de Barcelona. Available online: https://www.ub.edu/web/ub/en/recerca_innovacio/recerca_a_la_UB/instituts/instituts.html? (accessed on 5 April 2021).
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Interim Guidelines for Clinical Specimens for COVID-19. CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 4 May 2021).
- Risk Assessment: Risk Related to the Spread of New SARS-CoV-2 Variants of Concern in the EU/EEA—First Update. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-risk-assessment-spread-new-variants-concern-eueea-first-update (accessed on 30 April 2021).
- Rambaut, A.; Loman, N.; Pybus, O.; Barclay, W.; Barrett, J.; Carabelli, A.; Connor, T.; Peacock, T.; Robertson, D.L.; Volz, E.; et al. Preliminary Genomic Characterisation of an Emergent SARS-CoV-2 Lineage in the UK Defined by a Novel Set of Spike Mutations—SARS-CoV-2 Coronavirus/nCoV-2019 Genomic Epidemiology—Virological. Available online: https://virological.org/t/preliminary-genomic-characterisation-of-an-emergent-sars-cov-2-lineage-in-the-uk-defined-by-a-novel-set-of-spike-mutations/563 (accessed on 5 April 2021).
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.; Ostermann, P.N.; Walker, A.; Wienemann, T.; Mertens, A.; Adams, O.; Andree, M.; Hauka, S.; Lübke, N.; Keitel, V.; et al. Sensitivity of commercial Anti-SARS-CoV-2 serological assays in a high-prevalence setting. medRxiv 2020, 40, 1063–1071. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.r-project.org/ (accessed on 30 April 2021).
- Lavezzo, E.; Franchin, E.; Ciavarella, C.; Cuomo-Dannenburg, G.; Barzon, L.; Del Vecchio, C.; Rossi, L.; Manganelli, R.; Loregian, A.; Navarin, N.; et al. Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’. Nature 2020, 584, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, C.J.E.; Farrar, J.; Cutts, F.T.; Basta, N.E.; Graham, A.L.; Lessler, J.; Ferguson, N.M.; Burke, D.S.; Grenfell, B.T. Use of serological surveys to generate key insights into the changing global landscape of infectious disease. Lancet 2016, 388, 728–730. [Google Scholar] [CrossRef]
- Vusirikala, A.; Whitaker, H.; Jones, S.; Tessier, E.; Borrow, R.; Linley, E.; Hoschler, K.; Baawuah, F.; Ahmad, S.; Andrews, N.; et al. Seroprevalence of SARS-CoV-2 Antibodies in University Students: Cross-sectional study, December 2020, England. J. Infect. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Losina, E.; Leifer, V.; Millham, L.; Panella, C.; Hyle, E.P.; Mohareb, A.M.; Neilan, A.M.; Ciaranello, A.L.; Kazemian, P.; Freedberg, K.A. College Campuses and COVID-19 Mitigation: Clinical and Economic Value. Ann. Intern. Med. 2021, 174, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Thakur, A.; Soklaridis, S.; Crawford, A.; Mulsant, B.; Sockalingam, S. Using Rapid Design Thinking to Overcome COVID-19 Challenges in Medical Education. Acad. Med. 2021, 96, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Screening and Seroepidemiology of SARS-CoV-2 Infection at the University of Barcelona: A Cross-Sectional Study. Available online: https://clinicaltrials.gov/ct2/show/NCT04784403 (accessed on 6 April 2021).


| Students n = 1206 | ASS n = 699 | FM n = 793 | CFM n = 86 | ||
|---|---|---|---|---|---|
| Age, years | mean (sd) | 23.1 (6.3) | 49.3 (9.4) | 48.8 (11.3) | 50.4 (10.8) |
| Gender, Male/Female | n (%)/n (%) | 334 (28)/872 (72) | 222 (32)/477 (68) | 369 (46.5)/424 (53.5) | 40 (46.5)/46 (53.5) |
| BMI, kg/m² | |||||
| Underweight, < 18 | n (%) | 62 (5) | 5 (1) | 14 (2) | 1 (1) |
| Normal weight, 18 < 25 | n (%) | 937 (78) | 346 (50) | 452 (57) | 52 (61) |
| Overweight, 25 < 30 | n (%) | 172 (14) | 238 (34) | 266 (34) | 27 (31) |
| Obesity, ≥ 30 | n (%) | 34 (3) | 108 (16) | 59 (7) | 6 (7) |
| Clinical background (yes): | n (%) | ||||
| Cancer | n (%) | 2 (0) | 3 (0) | 1 (0) | 0 (0) |
| Cardiovascular disease (includes hypertension) | n (%) | 9 (1) | 73 (10) | 89 (11) | 13 (15) |
| Endocrine disease (diabetes) | n (%) | 2 (0) | 15 (2) | 8 (1) | 0 (0) |
| Immunocompromised | n (%) | 3 (0) | 12 (2) | 9 (1) | 1 (1) |
| Liver diseases | n (%) | 2 (0) | 6 (1) | 2 (0) | 0 (0) |
| Pulmonary disease | n (%) | 38 (3) | 44 (6) | 26 (3) | 2 (2) |
| Renal disease | n (%) | 0 (0) | 2 (0) | 6 (1) | 1 (1) |
| Lifestyle habits: | |||||
| Alcohol consumption, yes | n (%) | 502 (42) | 397 (57) | 560 (71) | 52 (61) |
| Increased during pandemic, yes | n(%) | 57 (11) | 47 (12) | 59 (10) | 8 (15) |
| Smoke tobacco, yes | n (%) | 147 (12) | 123 (18) | 82 (10) | 9 (11) |
| Increased during pandemic, yes | n (%) | 71 (6) | 47 (7) | 35 (4) | 1 (1) |
| Previous screening for SARS-CoV-2: | |||||
| At least one RT-PCR, yes | n (%) | 626 (52) | 263 (38) | 292 (37) | 44 (51) |
| At least one RT-PCR-positive, yes | n (%) | 68 (11) | 29 (11) | 19 (7) | 4 (9) |
| At least one serology study, yes | n (%) | 232 (19) | 78 (11) | 126 (16) | 16 (19) |
| At least one serology-positive study, yes | n (%) | 35 (13) | 15 (16) | 12 (9) | 4 (9) |
| Risk of SARS-CoV-2 infection: | |||||
| Direct contact with infected people, yes | n (%) | 154 (23) | 84 (13) | 79 (12) | 10 (13) |
| Students n = 626 | ASS n = 263 | FM n = 292 | CFM n = 44 | ||
|---|---|---|---|---|---|
| Fever (yes) | n (%) | 102 (16.3%) | 38 (14.4%) | 33 (11.3%) | 4 (9.1%) |
| Cough (yes) | n (%) | 77 (12.3%) | 35 (13.3%) | 26 (8.9%) | 4 (9.1%) |
| Anosmia (yes) | n (%) | 35 (5.6%) | 10 (3.8%) | 5 (1.7%) | 1 (2.3%) |
| Ageusia (yes) | n (%) | 26 (4.2%) | 5 (1.9%) | 2 (0.7%) | 1 (2.3%) |
| Shortness of breath (yes) | n (%) | 29 (4.6%) | 8 (3.0%) | 8 (2.7%) | 3 (6.8%) |
| Sore throat (yes) | n (%) | 54 (8.6%) | 21 (8.0%) | 12 (4.1%) | 0 (0.0%) |
| Fatigue (yes) | n (%) | 55 (8.8%) | 20 (7.6%) | 20 (6.8%) | 2 (4.6%) |
| Nausea (yes) | n (%) | 18 (2.9%) | 11 (4.2%) | 11 (3.8%) | 0 (0.0%) |
| Diarrhoea (yes) | n (%) | 50 (8.0%) | 29 (11.0%) | 15 (5.1%) | 1 (2.3%) |
| Arthralgia (yes) | n (%) | 56 (8.9%) | 24 (9.1%) | 12 (4.1%) | 1 (2.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Videla, S.; Otero, A.; Martí, S.; Domínguez, M.Á.; Fabrellas, N.; Delgado-Hito, M.P.; Cruz, I.; Tebé, C.; Vinuesa, T.; Ardila, F.; et al. Prevalence of SARS-CoV-2 Infection at the University of Barcelona during the Third COVID-19 Pandemic Wave in Spain. Int. J. Environ. Res. Public Health 2021, 18, 6526. https://doi.org/10.3390/ijerph18126526
Videla S, Otero A, Martí S, Domínguez MÁ, Fabrellas N, Delgado-Hito MP, Cruz I, Tebé C, Vinuesa T, Ardila F, et al. Prevalence of SARS-CoV-2 Infection at the University of Barcelona during the Third COVID-19 Pandemic Wave in Spain. International Journal of Environmental Research and Public Health. 2021; 18(12):6526. https://doi.org/10.3390/ijerph18126526
Chicago/Turabian StyleVidela, Sebastián, Aurema Otero, Sara Martí, M. Ángeles Domínguez, Nuria Fabrellas, M. Pilar Delgado-Hito, Imma Cruz, Cristian Tebé, Teresa Vinuesa, Fernando Ardila, and et al. 2021. "Prevalence of SARS-CoV-2 Infection at the University of Barcelona during the Third COVID-19 Pandemic Wave in Spain" International Journal of Environmental Research and Public Health 18, no. 12: 6526. https://doi.org/10.3390/ijerph18126526
APA StyleVidela, S., Otero, A., Martí, S., Domínguez, M. Á., Fabrellas, N., Delgado-Hito, M. P., Cruz, I., Tebé, C., Vinuesa, T., Ardila, F., Sancho, M., Fernández, E., Figuerola, M., & Ciruela, F. (2021). Prevalence of SARS-CoV-2 Infection at the University of Barcelona during the Third COVID-19 Pandemic Wave in Spain. International Journal of Environmental Research and Public Health, 18(12), 6526. https://doi.org/10.3390/ijerph18126526