
The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review

Abstract
1. Introduction
2. Material and Methods
2.1. Scoping Review Framework
2.2. Identifying the Research Question
- To raise hypotheses for the recent changes in the infant mortality rates in Brazil.
- Identifying gaps in terms of research concerning the determinants that may impact infant mortality in Brazil.
2.3. Identifying the Relevant Studies
2.3.1. Inclusion and Exclusion Criteria
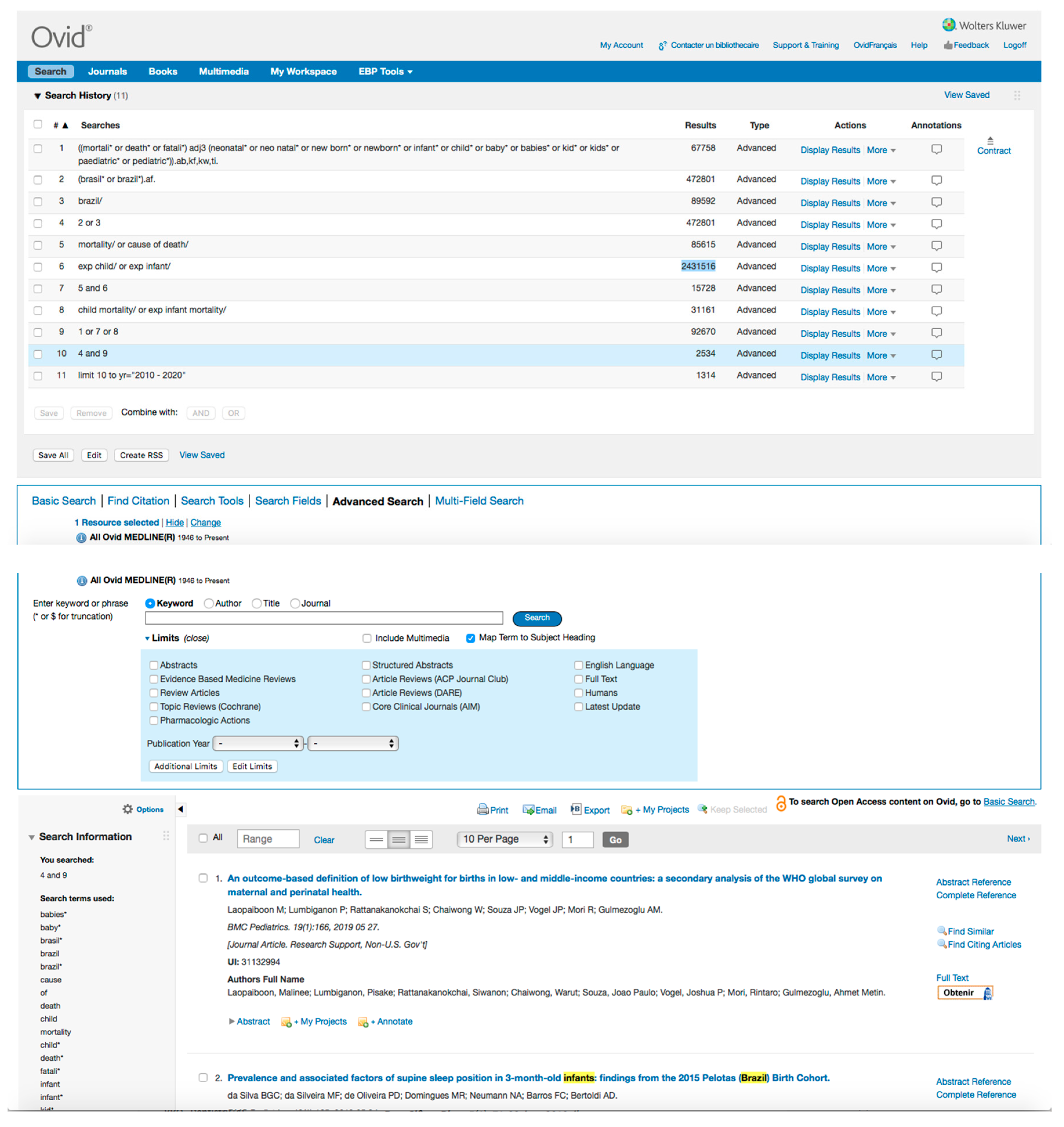
2.3.2. Search Criteria
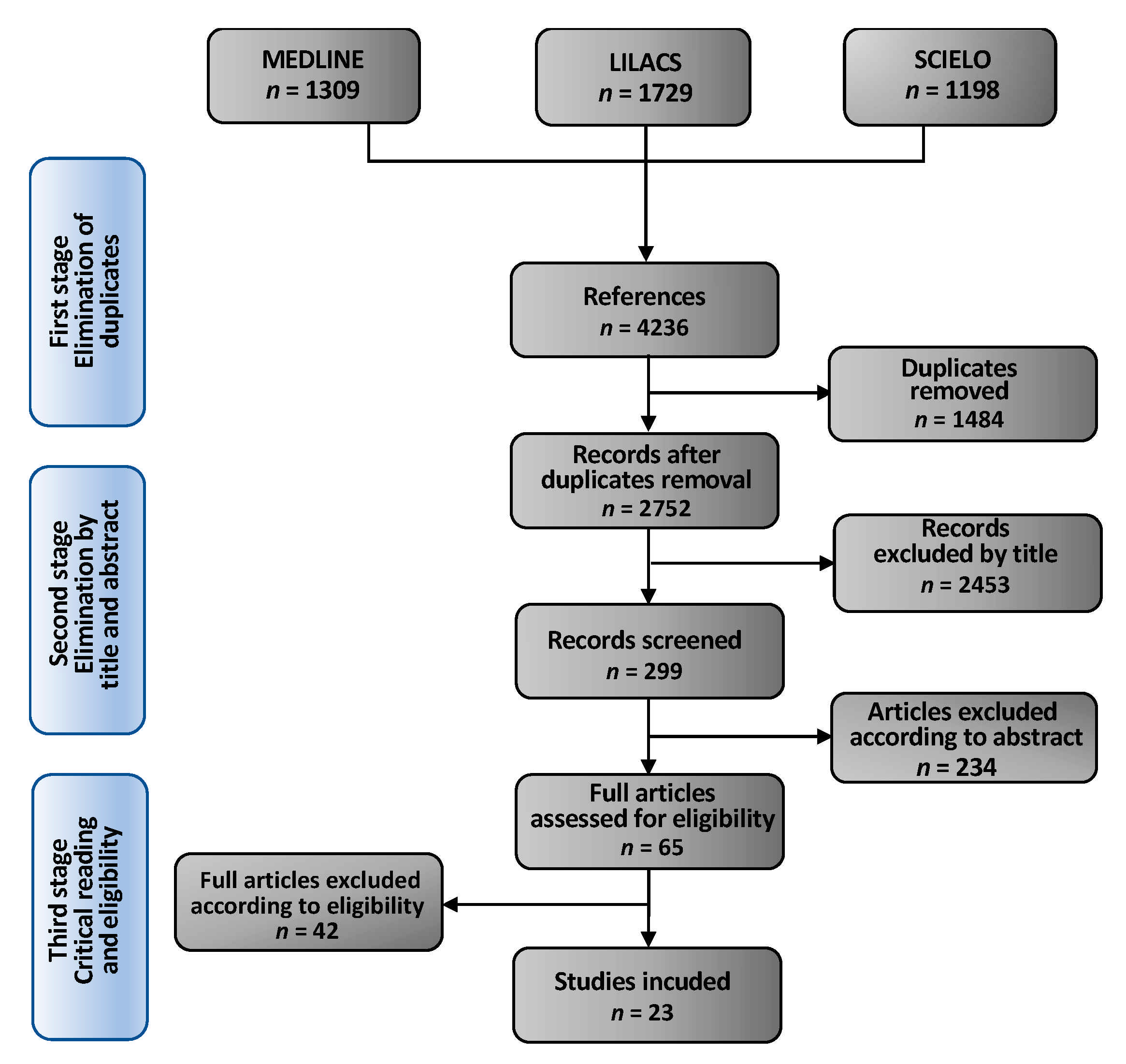
3. Study Selection
3.1. Selected Studies
3.2. Charting the Data, Summarizing and Reporting the Findings
4. Results
4.1. The Determinants of Infant Mortality in Brazil
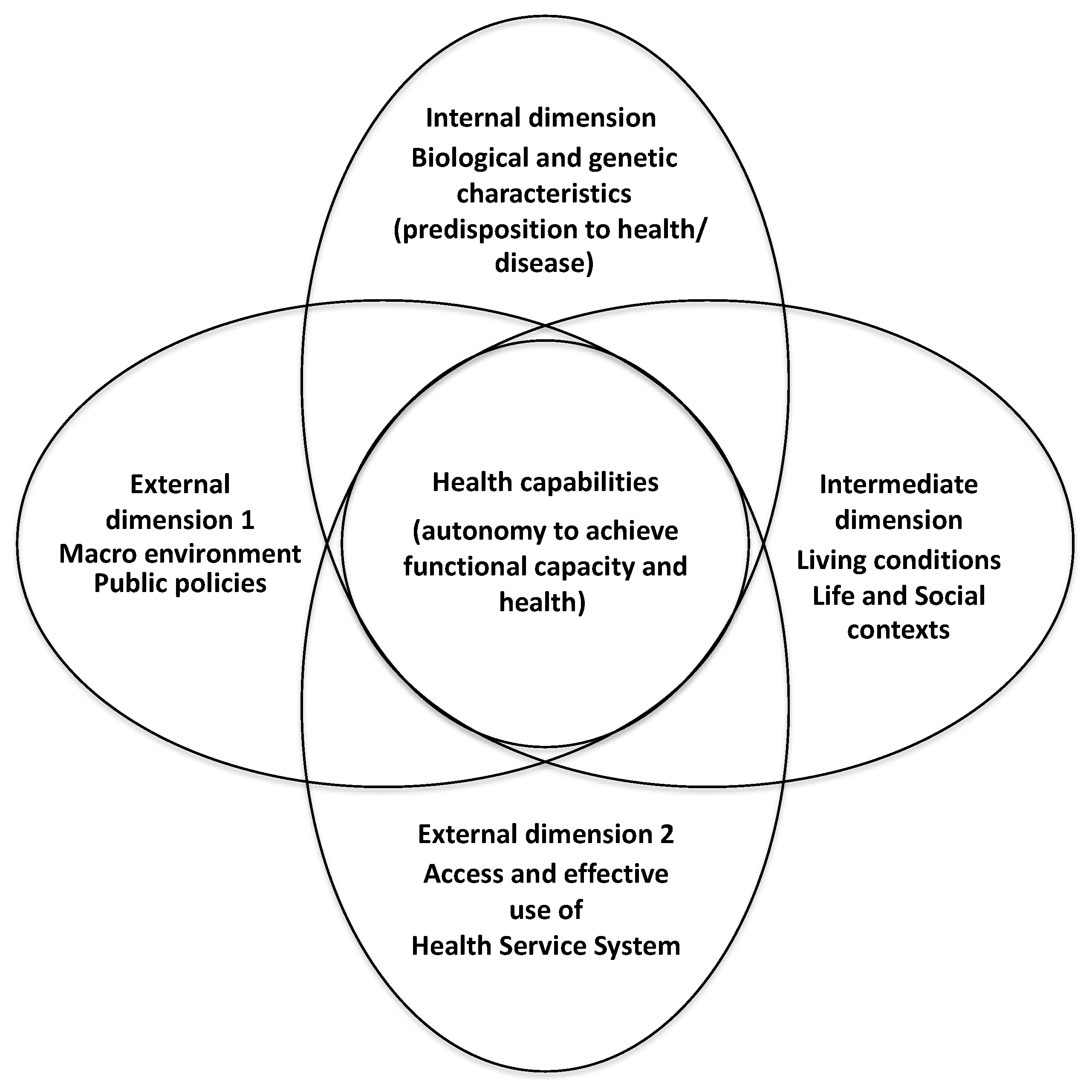
4.2. The Four Dimensions of CMHC
4.2.1. External Dimension 1—Macro-Environment/Outcome of Public Policies
Healthcare Policies and Actions
Policies Not Directly Related to Health
The Brazilian Conditional Cash Transfer Bolsa Família Program
4.2.2. External Dimension 2—Access and Effective Use of the Health Service System
Coverage, Reorganization and Access to Health Services
Quality of Services
4.2.3. Intermediate Dimension—Living Conditions, Social, and Life Contexts
Income, Poverty and Nutritional Status
Housing
Educational Attainment and Fertility
Living Conditions and Development Indexes
4.2.4. Internal Dimension—Individual Characteristics/Genetic and Biological Factors
Low Birth Weight, Maternal Age, and Congenital Malformations
5. Discussion
5.1. The Implementation of FHS and BFP and the CMHC
Strengths and Limits
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FHS | Family Health Strategy |
| BFP | Bolsa Família Program |
| WHO | World Health Organization |
| SUS | Brazilian Unified Health System (Sistema Único de Saúde) |
| NMR | Neonatal Mortality Rate |
| ENMR | Early Neonatal Mortality Rate |
| LNMR | Late Neonatal Mortality rate |
| IMR | Infant Mortality Rate |
| U5MR | Under-five Mortality Rate |
| PNMR | Post-neonatal mortality rate |
| MEDLINE | US National Library of Medicine |
| LILACS | Latin American and Caribbean Literature in Health Sciences |
| SciELO | Scientific Electronic Library Online |
| MMAT | Mixed Method Appraisal Toll |
| CMHC | Conceptual Model of Health Capability |
| LBW | Low Birth Weight |
| LBWP | Low Birth Weight Paradox |
| GDP | Gross Domestic Growth |
| GBD | Global Burden Disease |
| NIP | National Immunization Program |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concepts | Mortality | Infant | Brazil |
|---|---|---|---|
| Keywords | Mortality Mortalities Morte Mortalidade Death * Death rate Death rates Fatality rates | Neonatal Infant Child Neonatal Neonatal Newborn Newborn Perinatal Baby Babies Kid Paediatric Pediatric | Brasil Brazil |
| Descriptors | Mortality (exp) Cause of death | Child Infant | Brazil |
| Descriptors | Child mortality Infant mortality | ||
| # Research | Equations | Results |
|---|---|---|
| 1 | ((mortali* or death* or fatali*) adj3 (neonatal* or neo natal* or new born* or newborn* or infant* or child* or baby* or babies* or kid* or kids* or paediatric* or pediatric*)). ab,kf,kw,ti. | 67,758 |
| 2 | (brasil* OR brazil*). af. | 472,801 |
| 3 | Brazil/ | 89,592 |
| 4 | 3 OR 4 | 472,801 |
| 5 | mortality/OR cause of death/ | 85,615 |
| 6 | Exp child/OR exp infant/ | 2,431,516 |
| 7 | 5 AND 6 | 15,728 |
| 8 | child mortality/OR exp infant mortality/ | 31,161 |
| 9 | 1 OR 7 OR 8 | 92,670 |
| 10 | 4 AND 9 | 2534 |
| 11 | limit 10 to year = ”2010–2020” | 1314 |


| Concepts | Concept 1 | Concept 2 |
|---|---|---|
| Keywords | Mortalidade Infantil no Brasil | Mortalidade Neonatal no Brasil |
| Descriptors base SCIELO | mortalidade, infantil, brasil | mortalidade, neonatal, brasil |
| Concept 1 (research equation with keywords) | w:((mortali* OR death* OR fatali*) AND (neonat* OR “neo nat*” OR newborn* OR “new born*” OR “recém nascido*” OR infant* OR child* OR crianca*) AND (brasil* OR brazil*)) AND (db:(“LILACS”)) AND (year_cluster:[2010 TO 2020]) AND (db:(“LILACS”)) | |
| Concept 2 (research equation with descriptors) | mh:(mh:(((((mortality OR death OR “cause of death”) AND (child OR infant OR “infant, newborn”)) OR (“child mortality” OR “infant mortality” OR “perinatal mortality”)) AND (brazil))) AND (db:(“LILACS”)) AND (year_cluster:[2010 TO 2020])) | |




| Concept (Research equation with keywords) | (mortali* OR death* OR fatalit*) AND (neonatal* OR “neo natal*” OR “new born*” OR newborn* OR infant* OR child* OR crianca OR “recém nascido”) AND (brasil* OR brazil*) AND year_cluster:(“2013” OR “2014” OR “2019” OR “2017” OR “2011” OR “2018” OR “2010” OR “2016” OR “2012” OR “2015”) |



Appendix B


References
- Duarte, C.M.R. Health policy effects on infant mortality trends in Brazil: A literature review from the last decade. Cadernos Saúde Publica 2007, 23, 1511–1528. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Reidpath, D.D.; Allotey, P. Infant mortality rate as an indicator of population health. J. Epidemiol. Community Health 2003, 57, 344–346. [Google Scholar] [CrossRef] [PubMed]
- WHO. Principaux concepts relatifs aux déterminants sociaux de la santé. In Commission des Déterminants Sociaux de la Santé 2005–2008, Raport Final; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Gomes, T.G.A.C.B.; Ferreira, L.D.S.; Queiroz, M.N.D.; Reis Netto, P.B.D.; Bezerra, V.N.; Costa, A.M. Mortalidade na infância no Brasil e regiões no período de 2000 a 2011: O impacto da atenção básica. Comun. Ciênc. Saúde 2016, 27, 259–266. [Google Scholar] [CrossRef]
- Observatório de Saúde da Região Metropolitana de São Paulo. Evolução da Mortalidade Infantil na Região Metropolitana de São Paulo-RMSP-Mortalidade Infantil no Brasil e no Estado de São Paulo, Almeida, M.F., Mortalidade Infantil na RMSP, Silva, Z.P., Mortalidade Infantil na Cidade de São Paulo, Equipe CEInfo-SMS-SP, Coord. Júnior, A.E., Observatório de Saúde da RMSP and Sala, A. SES-SP and team GVEs-RMS; Observatório de Saúde da Região Metropolitana de São Paulo, Faculdade de Saúde Pública da Universidade de São Paulo, FSP-USP Mortalidade Infantil na RMSP, Silva, Z.P.; Faculdade de Saúde Pública da Universidade de São Paulo, FSP-USP: São Paulo, Brazil, 2018; p. 18. [Google Scholar]
- UNICEF. Levels & Trends in Child Mortality, UN Interagency Group for Child Mortality Estimation; UNICEF: New York, NY, USA, 2015.
- Shei, A. Brazil’s Conditional Cash Transfer Program Associated with Declines in Infant Mortality Rates. Health Aff. 2013, 32, 1274–1281. [Google Scholar] [CrossRef]
- Souza, M.D.F.M.D.; Malta, D.C.; França, E.B.; Barreto, M.L. Changes in health and disease in Brazil and its States in the 30 years since the Unified Healthcare System (SUS) was created. Cienc. Saude Coletiva 2018, 23, 1737–1750. [Google Scholar] [CrossRef]
- Abrasco. Especial Abrasco Sobre o Aumento da Mortalidade Infantil e Materna no Brasil; Abrasco: Rio de Janeiro, Brazil, 2018. [Google Scholar]
- Fiocruz, Política e Ação em Saúde Pública: Conjuntura Política. Abrasco Alerta Para o Aumento da Mortalidade Infantil e Materna no Brasil. CEE—Centro de Estudos Estratégicos da Fiocruz. Pesquisa, Política e Ação em Saúde Pública: Conjuntura Política; Fiocruz: Rio de Janeiro, Brazil, 2019. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Santos, H.G.D.; Andrade, S.M.D.; Silva, A.M.R.; Mathias, T.A.D.F.; Ferrari, L.L.; Mesas, A.E. Mortes infantis evitáveis por intervenções do Sistema Único de Saúde: Comparação de duas coortes de nascimentos. Ciênc. Saúde Coletiva 2014, 19, 907–916. Available online: http://www.scielo.br/scielo.php?script=sci_arttextpid=S1413-81232014000300907lng=en (accessed on 7 September 2020). [CrossRef]
- Malta, D.C.; Prado, R.R.D.; Saltarelli, R.M.F.; Monteiro, R.A.; Souza, M.D.F.M.D.; Almeida, M.F.D. Preventable deaths in childhood, according to actions of the Unified Health System, Brazil. Rev. Bras. Epidemiol. 2019, 22, e190014. [Google Scholar] [CrossRef]
- Armstrong, R.; Hall, B.J.; Doyle, J.; Waters, E. Scoping the scope’ of a cochrane review. J. Public Health 2011, 33, 147–150. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. Interdiscip. J. Inf. Stud. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT) VERSION 2018/User Guide. 1 August 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 6 August 2020).
- Ruger, J.P. Health Capability: Conceptualization and Operationalization. Am. J. Public Health 2010, 100, 41–49. [Google Scholar] [CrossRef]
- Sen, A. Inequality of What? The Tanner Lecture on Huan Values, Delivered at Stanford University, 22 May 1979; Stanford University: Stanford, CA, USA, 1979. [Google Scholar]
- Sen, A. Health: Perception versus observation. Br. Med. J. 2002, 324, 860–861. [Google Scholar] [CrossRef]
- Nussbaum, M.C. Creating Capabilities: The Human Development Approach in Creating Capabilities: The Human Development Approach; Harvard University Press: Cambridge, MA, USA, 2013. [Google Scholar]
- López Barreda, R.; Robertson-Preidler, J.; Bedregal García, P. Health assessment and the capability approach. Glob. Bioeth. 2019, 30, 19–27. [Google Scholar] [CrossRef]
- Hamal, M.; Dieleman, M.; De Brouwere, V.; de Cock Buning, T. Social determinants of maternal health: A scoping review of factors influencing maternal mortality and maternal health service use in India. Public Health Rev. 2020, 41, 13. [Google Scholar] [CrossRef]
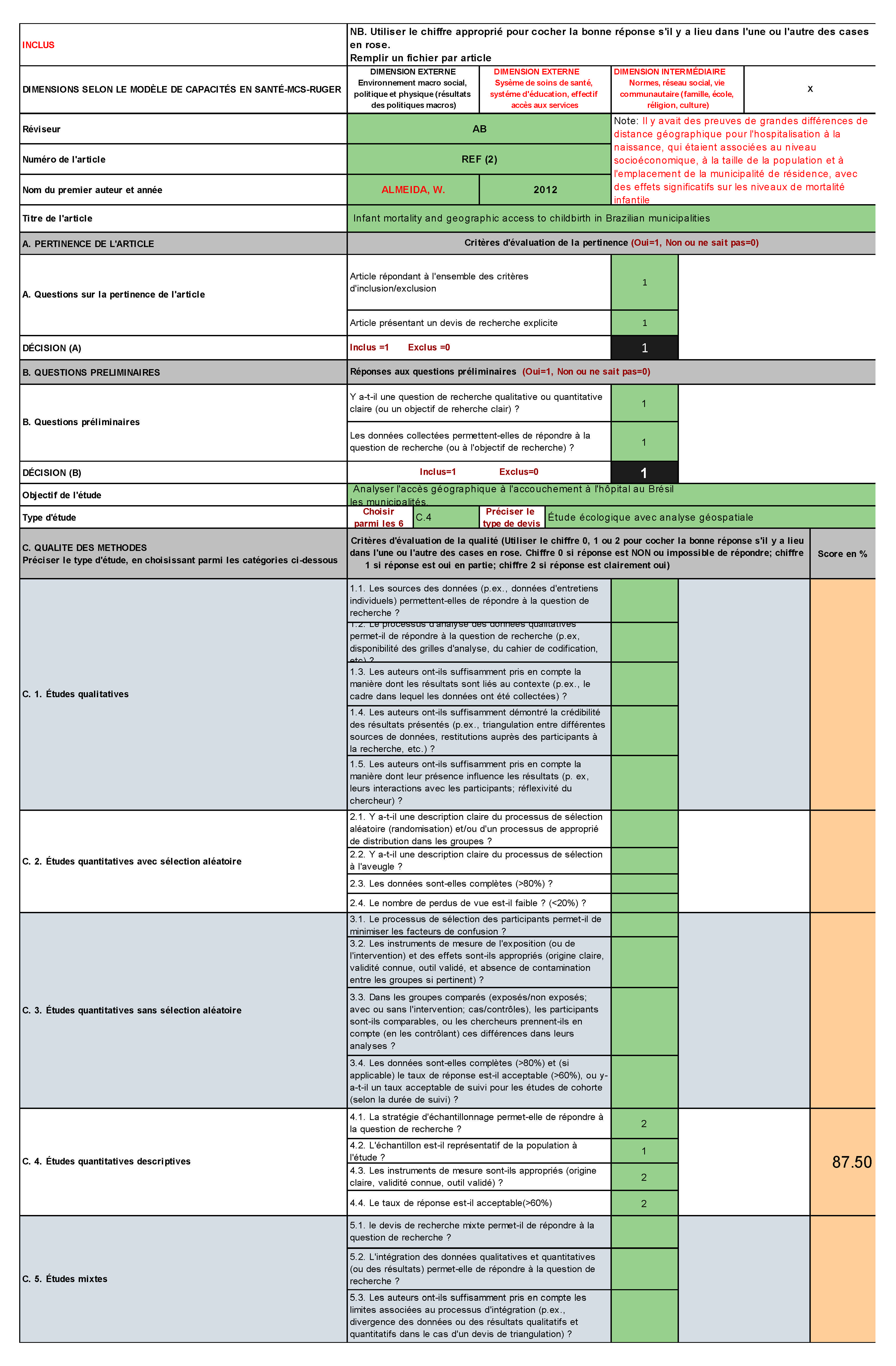
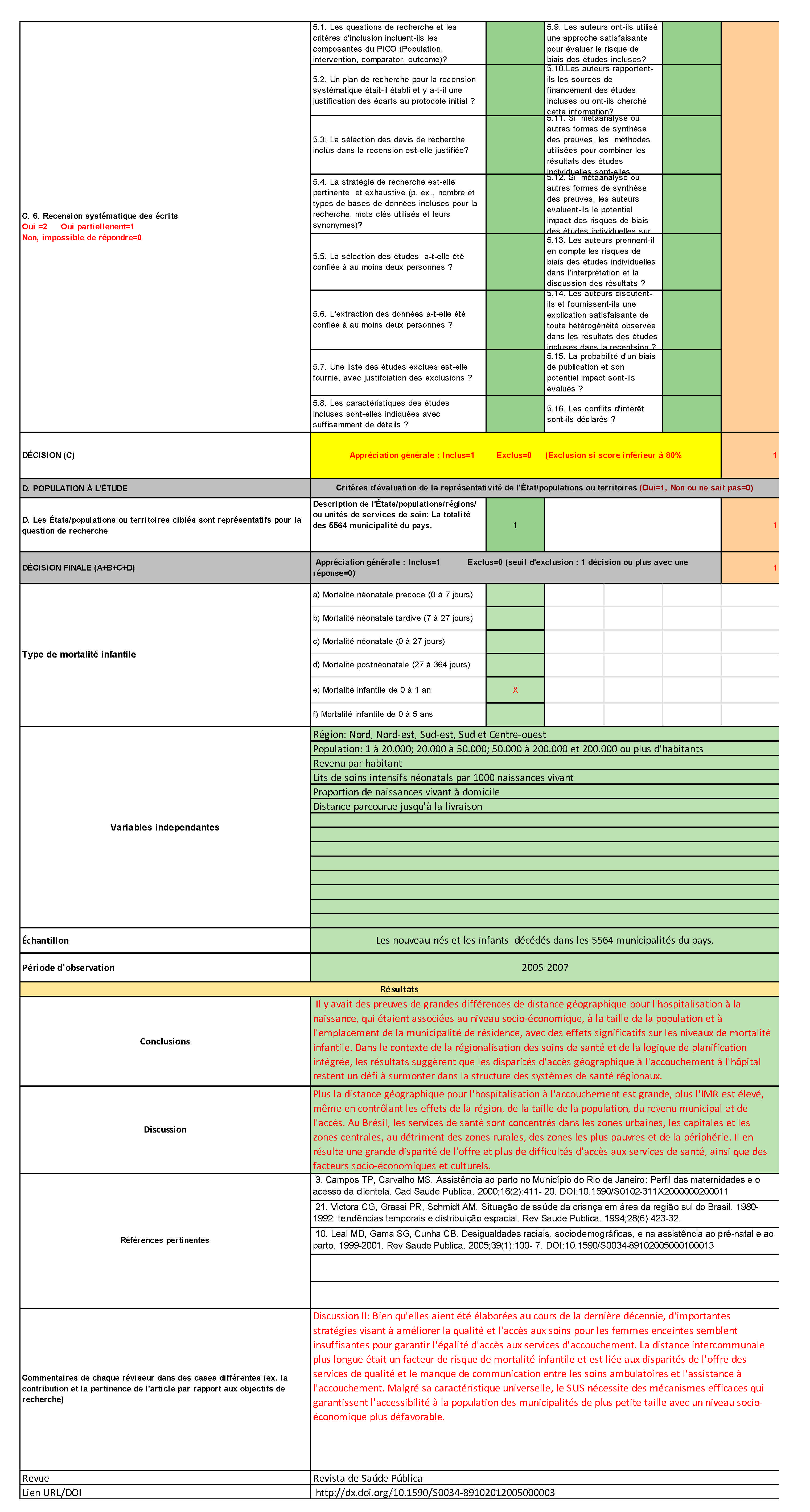
- Almeida, W.D.S.D.; Szwarcwald, C.L. Infant mortality and geographic access to childbirth in Brazilian municipalities. Rev. Saude Publica 2012, 46, 68–76. [Google Scholar] [CrossRef]
- Araújo, C.E.L.; Gonçalves, G.Q.; Machado, J.A. Brazilian municipalities and their own expenditures on health: Some associations. Cienc. Saude Coletiva 2017, 22, 953–963. [Google Scholar] [CrossRef]
- Boschi-Pinto, C.; Dilip, T.R.; Costello, A. Association between community management of pneumonia and diarrhoea in high-burden countries and the decline in under-five mortality rates: An ecological analysis. BMJ Open 2017, 7, e012639. [Google Scholar] [CrossRef]
- Buehler, H.F.; Ignotti, E.; Neves, S.M. Spatial analysis of integrated health and environmental indicators for morbidity and mortality due to infant diarrhea in Brazil, 2010. Cadernos Saude Publica 2014, 30, 1921–1934. [Google Scholar]
- França, E.B.; Lansky, S.; Rego, M.A.S.; Malta, D.C.; França, J.S.; Teixeira, R.; Porto, D.; Almeida, M.F.D.; Souza, M.D.F.M.D.; Szwarcwald, C.L.; et al. Leading causes of child mortality in Brazil, in 1990 and 2015: Estimates from the Global Burden of Disease study. Rev. Bras. Epidemiol. 2017, 20 (Suppl. 1), 46–60. [Google Scholar] [CrossRef]
- Garcia, L.P.; Santana, L.R. Evolution of socioeconomic inequalities in infant and child mortality in Brazil, 1993–2008. Cienc. Saude Coletiva 2011, 16, 3717–3728. [Google Scholar] [CrossRef]
- Guanais, F.C. The combined effects of the expansion of primary health care and conditional cash transfers on infant mortality in Brazil, 1998–2010. Am. J. Public Health 2013, 103, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Martins, P.C.R.; Pontes, E.R.J.C.; Higa, L.T. Convergência entre as Taxas de Mortalidade Infantil e os Índices de Desenvolvimento Humano no Brasil no período de 2000 a 2010. Interações 2018, 19, 291–303. [Google Scholar] [CrossRef]
- Mendes, P.S.; Ribeiro JR, H.C.; Mendes, C.M. Temporal trends of overall mortality and hospital morbidity due to diarrheal disease in Brazilian children younger than 5 years from 2000 to 2010. J. Pediatr. 2013, 89, 315–325. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Oliveira, G.S.; Lima, M.C.B.D.; Lyra, C.D.; da Costa Oliveira, A.G.R.; Ferreira, M.A.F. The spatial inequality of neonatal mortality in Brazil: 2006 to 2010. Cienc. Saude Coletiva 2013, 18, 2431–2441. [Google Scholar] [CrossRef]
- Ramalho, W.M.; Sardinha, L.M.V.; Rodrigues, I.P.; Duarte, E.C. Inequalities in infant mortality among municipalities in Brazil according to the Family Development Index, 2006–2008. Pan Am. J. Public Health 2013, 33, 205–212. [Google Scholar] [CrossRef]
- Rasella, D.; Aquino, R.; Barreto, M.L. Reducing childhood mortality from diarrhea and lower respiratory tract infections in Brazil. Pediatrics 2010, 126, e534–e540. [Google Scholar] [CrossRef]
- Rasella, D.; Aquino, R.; Santos, C.A.; Paes-Sousa, R.; Barreto, M.L. Effect of a conditional cash transfer programme on childhood mortality: A nationwide analysis of Brazilian municipalities. Lancet 2013, 382, 57–64. [Google Scholar] [CrossRef]
- Rodrigues, N.C.P.; Monteiro, D.L.M.; Almeida, A.S.D.; Barros, M.B.D.L.; Pereira Neto, A.; O’Dwyer, G.; Andrade, M.K.D.N.; Flynn, M.B.; Lino, V.T.S. Temporal and spatial evolution of maternal and neonatal mortality rates in Brazil, 1997–2012. J. Pediatr. 2016, 92, 567–573. [Google Scholar] [CrossRef]
- Russo, L.X.; Scott, A.; Sivey, P.; Dias, J. Primary care physicians and infant mortality: Evidence from Brazil. PLoS ONE 2019, 14, e0217614. [Google Scholar] [CrossRef]
- Schuck-Paim, C.; Taylor, R.J.; Alonso, W.J.; Weinberger, D.M.; Simonsen, L. Effect of pneumococcal conjugate vaccine introduction on childhood pneumonia mortality in Brazil: A retrospective observational study. Lancet Glob. Health 2019, 7, e249–e256. [Google Scholar] [CrossRef]
- Silva, A.A.M.D.; Silva, L.M.D.; Barbieri, M.A.; Bettiol, H.; Carvalho, L.M.D.; Ribeiro, V.S.; Goldani, M.Z. The epidemiologic paradox of low birth weight in Brazil. Rev. Saude Publica 2010, 44, 767–775. [Google Scholar] [CrossRef][Green Version]
- Silva, A.L.A.D.; Mendes, A.D.C.G.; Miranda, G.M.D.; Santos Neto, P.M.D. Childbirth care in Brazil: A critical situation has not yet been overcome. 1999–2013. Rev. Bras. Saúde Matern. Infant. 2016, 16, 129–137. [Google Scholar] [CrossRef]
- Verona, A.P.D.A.; Hummer, R.; Dias Júnior, C.S.; Lima, L.C.D. Infant mortality and mothers’ religious involvement in Brazil. Rev. Bras. Estud. Popul. 2010, 27, 59–74. [Google Scholar] [CrossRef]
- Vieira-Meyer, A.P.G.F.; de Araújo Dias, M.S.; Vasconcelos, M.I.O.; Rouberte, E.S.C.; de Almeida, A.M.B.; de Albuquerque Pinheiro, T.X.; de Lima Saintrain, M.V.; Machado, M.D.F.A.S.; Dufault, S.; Reynolds, S.A.; et al. What is the relative impact of primary health care quality and conditional cash transfer program in child mortality? Can. J. Public Health 2019, 110, 756–767. [Google Scholar] [CrossRef]
- Rodrigues, F.E.; Tatto, R.B.; Vauchinski, L.; Leães, L.M.; Rodrigues, M.M.; Rodrigues, V.B.; Catharino, A.; Cainelli, M.; Prates, G.P.; Cerqueira, T.M.; et al. Pneumonia mortality in Brazilian children aged 4 years and younger. J. Pediatr. 2011, 87, 111–114. [Google Scholar]
- Ferrari, R.A.P.; Bertolozzi, M.R. Mortalidade pós-neonatal no território brasileiro: Uma revisão da literatura. Rev. Esc. Enferm. USP 2012, 46, 1207–1214. [Google Scholar] [CrossRef][Green Version]
- Duarte, C.M.R. Reflexos das políticas de saúde sobre as tendências da mortalidade infantil no Brasil: Revisão da literatura sobre a última década. Cadernos Saúde Pública 2007, 23, 1511–1528. [Google Scholar] [CrossRef][Green Version]
- Santos, H.A.; de Andrade, S.M.; Birolim, M.; Carvalho, W.; Silva, A. Infant mortality in Brazil: A literature review before and after the unified health system implementation. Pediatria 2010, 32, 131–143. [Google Scholar]
- Tengland, P.-A. Health and capabilities: A conceptual clarification. Med. Health Care Philos. 2020, 23, 25–33. [Google Scholar] [CrossRef]


| MEDLINE | MeSh ** descriptors: ((mortali* or death* or fatali*) adj3 (neonatal* or neo natal* or new born* or newborn* or infant* or child* or baby* or babies* or kid* or kids* or paediatric* or pediatric*)). ab, kf, kw, ti. Keywords: “death” “fatality”, “neonatal”, “neo natal”, “newborn”, “new born”, “child”, “baby”, “babies”, “kid”, “kids”, “paediatric” and “pediatric” |
| LILACS | Descriptors: Concept 1: mh:(mh:(((((mortality OR death OR “cause of death”) AND (child OR infant OR “infant, newborn”)) OR (“child mortality” OR “infant mortality” OR “perinatal mortality”)) AND (brazil))) AND (db:(“LILACS”)) AND (year_cluster: [2010 TO 2020]))” Keywords: w:((mortali* OR death* OR fatali*) AND (neonat* OR “neonat*” OR newborn* OR “new born*” OR “recém nascido*” OR infant* OR child* OR crianca AND (brasil* OR brazil*)) AND (db:(“LILACS”)) AND (year_cluster:[2010 TO 2020]) AND (db:(“LILACS”)) |
| SCIELO | Keywords: (mortali* OR death* OR fatalit*) AND (neonatal* OR “neonatal*” OR “new born*” OR newborn* OR infant* OR child* OR crianca OR “recém nascido”) AND (brasil* OR brazil*) AND year_cluster:(“2013” OR “2014” OR “2019” OR “2017” OR “2011” OR “2018” OR “2010” OR “2016” OR “2012” OR “2015”) |
| Author | Period | Methods | Sample/Study Unit | Indicator | Objective |
|---|---|---|---|---|---|
| Almeida, W. [23] | 2005–2007 | Ecological study with geospatial analysis | Newborns and deceased infants in the 5564 municipalities | IMR | To analyze geographic access to childbirth in hospital in Brazil municipalities and IMR |
| Araújo, C. [24] | 2010 | Retrospective descriptive analysis | Deceased children of mothers living in 5526 municipalities | IMR | To evaluate the effect of municipal per capita spending on health on IMR |
| Boschi-Pinto, C. [25] | 1990–2015 | Ecological study | Populations and regions of 75 low and middle income countries with high burden of diarrhea and pneumonia, including Brazil | U5MR | To explore whether the adoption of national policies for the management of pneumonia and diarrhea is associated with the decline U5MR |
| Bühler, H. [26] | 2010 | Ecological study with geospatial analysis | Deceased children under-one year from mothers who lived in the 558 health micro-regions | IMR | To study environmental indicators for diarrhea in children under one year of age in Brazil and IMR |
| França, E. [27] | 1990–2015 | Ecological study and statistical analysis | Deceased children under-five and general population | U5MR | To analyze the leading causes of U5MR, using estimates from the Global Burden of Disease Study (GBD) 2015 |
| Garcia, L. [28] | 1993–2008 | Cross-sectional study | Macro-regions, units of the Federation and nine metropolitan regions | IMR/U5MR | To study the temporal evolution and the extent of inequalities in infant and child mortality |
| Gomes, T. [4] | 2000–2011 | Ecological study with time series | Under-five deceased children in Brazil and macro-regions | U5MR | To analyze the trends in childhood mortality in Brazil and regions study the correlation between acute diarrheal disease and acute respiratory infection and U5MR |
| Guanais, F. [29] | 1998–2010 | Panel data | Deceased children of families benefiting from the BFP and FHS living in 4853 municipalities | NMR/Post-neonatal mortality rate (PNMR) | To examine the combined effects of (FHS) and BFP on NMR and PNMR |
| Malta, D. [13] | 2000–2013 | Ecological study with time series | All under-five children deceased in Brazil and macro-regions | U5MR | To analyze the trend in U5MR according to the list of preventable causes of death |
| Martins, P. [30] | 2000–2010 | Ecological study | Children under-one deceased from mothers living in the states and macro-regions | IMR | To analyze the convergence between the decrease in IMR and the Municipal Human Development Index |
| Mendes, P. [31] | 2000–2010 | Ecological study with time series | Under-one and under-five deceased children in the 5 macro-regions | IIMR/U5MR | To analyze the temporal trends of indicators of IMR and U5MR related to hospital morbidity due to diarrheal diseases |
| Oliveira, G. [32] | 2006–2010 | Ecological study with geospatial analysis | Newborns deceased in the 26 states and the Federal District, Brasília | NMR | To analyze the spatial distribution of neonatal mortality and its correlation with biological, socioeconomic, maternal and child factors |
| Ramalho, W. [33] | 2006–2008 | Ecological study | Children deceased between 27th and the 364th day of life in the 5227 | NMR/ENMR/LNMR/PNMR | To describe the inequalities in infant mortality according to socio-economic indicators between geographic areas and municipalities in Brazil |
| Rasella, D. [34] | 2000–2005 | Panel data | Children under-five who died in Brazilian municipalities | NMR/IMR/PNMR/U5MR | To assess the effects of the FHS on the U5MR du to diarrhea diarrheal diseases and lower respiratory tract infections |
| Rasella, D. [35] | 2004–2009 | Panel data | Children under-five who died in 2853 municipalities. | U5MR | To assess the effect of BFP on deaths of children under-five, associated with to poverty, diarrhea, lower respiratory tract infections and malnutrition |
| Rodrigues, N. [36] | 1997–2000/ 2001–2004/ 2005–2008/ 2009–2012 | Ecological study with geospatial analysis | Deceased children from mothers living in the 5 macro-regions | ENMR/LNMR | To assess the spatial and temporal trends of maternaland neonatal mortality. |
| Russo, L. [37] | 2005–2012 | Panel data | Deceased children under-one year in 5563 municipalities | IMR | To study the effect of primary care physicians on IMR |
| Schuck-Paim, C. [38] | 1980–2010 | Retrospective descriptive analysis | Children under-five who died frompneumonia from mothers living in the 5570 municipalities | U5MR | To assess the effect of ten-valent pneumococcal conjugate vaccine (PCV10) on under-five mortality from pneumonia |
| Shei, A. [7] | 1998–2008 | Times series study | Infant deaths in the all municipalities in the country. | NMR/PNMR/IMR | To examine whether the implementation and expansion of the BFP Program, was associated with infant mortality |
| Silva, A.A. [39] | 1995–2007 | Correlational descriptive study | Deceased children in the five Macro-regions and the 26 states and the Federal District, Brasília | IMR | To examine whether the low birth weight (LBW) paradox exists in Brazil |
| Silva, A.L.D. [40] | 1999–2013 | Ecological time series | The country’s population (women of childbearing age, children born alive and deceased in the national territory | NMR/IMR | To analyze childbirth assistance according to birth profile, characteristics of live births and preventable infant deaths |
| Verona, A. [41] | 1996–2006 | Correlational analysis | Under-one children deceased from mothers aged 15 to 49 who had at least one child in the five years preceding the survey | IMR | To examine the relation between IMR and religious involvement of mothers |
| Vieira-Meyer, A. [42] | 2012 | Ecological study | Under-one deceased children from mothers living in 3441 municipalities | IMR | To access how the coverage and quality of FHS and BFP are associated with IMR |
| Outcome of Public Policies | Health Policies | Policies Not Directly Related to Health | Conditional Cash Transfer Program | Reorganization of Health Service System | Access and Effective Use of Healthcare | Access to Health Services | Quality of Healthcare | Primary Healthcare | Living Conditions | Income | Housing | Education | Nutritional Status and Poverty | Fertiliy Rate | Inividual Characteristics | Maternal Age | Low Birth Weight | Congenital Malformation | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| External Dimension 1 | 19 | 13 | 15 | 7 | |||||||||||||||
| External Dimension 2 | 18 | 14 | 5 | 5 | 7 | ||||||||||||||
| Intermediate Dimension | 18 | 8 | 7 | 7 | 5 | 5 | |||||||||||||
| Internal Dimension | 6 | 1 | 4 | 2 | |||||||||||||||
| Proportion | 83% | 57% | 65% | 30% | 78% | 61% | 22% | 22% | 30% | 78% | 35% | 30% | 30% | 22% | 22% | 27% | 4% | 17% | 9% |
| Main Author/Year | External Dimension 1 * | External Dimension 2 * | Intermediate Dimension * | Internal Dimension * |
|---|---|---|---|---|
| Almeida, W./2012 [23] | Socioeconomic conditions | Unequal access and quality of healthcare/organization of healthcare | Geographical distance and the difficult access to childbirth facility/socioeconomic and cultural factors | _ |
| Araújo, C./2017 [24] | Per capita spending of municipality’s own resources on healthcare | Unequal access to healthcare | Living conditions | _ |
| Boschi-Pinto, C./2017 [25] | National policy of management for treating pneumonia and diarrhea/the Millennium Development Goal SDG-4 | _ | _ | _ |
| Bühler, H./2014 [26] | Socio-environmental policies | _ | Percentage of residents without garbage collection service and dependency ratio | _ |
| França, E./2017 [27] | BFP/National Immunization Program (NIP)/FHS | Primary healthcare/reorganization of prenatal and neonatal care | Improvements in nutrition/basic sanitation | Prematurity/congenital anomalies |
| Garcia, L./2011 [28] | Regional socioeconomic inequalities/household per capita income | _ | Maternal schooling/living conditions | _ |
| Gomes, T./2016 [4] | Expanding coverage rate of FHS/improvements in socioeconomic conditions | Increase in the population covered by primary care | _ | _ |
| Guanais, F./2013 [29] | The expansion and interaction between FHS and BFP programs | Quality of hospital birth care | Improvements in daily living Conditions/ fertility rate | _ |
| Malta, D./2019 [13] | SUS/healthcare promotion actions linked to healthcare actions | Adequate neonatal care/diagnostic/therapeutic actions and care during childbirth | _ | Short-term pregnancy/low birth weight (LBW) |
| Martins, P./2018 [30] | Regional socioeconomic disparities | _ | Living conditions expressed by Municipal Human Development Index (MHDI) | _ |
| Mendes, P./2013 [31] | Healthcare policies and socioeconomic inequalities | Limited access to healthcare | Socioeconomic and cultural disparities | _ |
| Oliveira, G./2013 [32] | Macroeconomic policies/BFP/socioeconomic and regional inequalities | Inequalities in accessing maternal/prenatal/birth care and caesarean sections | Living conditions/maternaleducation/Low Birth Weight Paradox (LBWP) | Maternal age/teenage pregnancy/LBW |
| Ramalho, W./2013 [33] | Socioeconomic conditions measured by Family Development Index (FDI) | Coverage of healthcare/healthcare information system | FDI/family vulnerability/social mobilization | Congenital malformation |
| Rasella, D./2010 [34] | FHS coverage rate | Reorganization of primary healthcare/early case diagnosis/antibiotic prescription | socioeconomic conditions | _ |
| Rasella, D./2013 [35] | BFP and FHS coverage rate | Increased primary care through BFP | Extreme poverty/undernutrition | _ |
| Rodrigues, N./2016 [36] | _ | Unequal distribution of healthcare among the macro-regions | _ | _ |
| Russo, L./2019 [37] | Gross Domestic Product per capita/FHS | Availability of primary care physician/private health insurance coverage | Gross Domestic Product (GDP) per capita/piped water/electricity/garbage collection | _ |
| Schuck-Paim, C./2019 [38] | National Immunization Program | Vaccination/improved education and healthcare | Improved nutrition and hygiene/maternal education | _ |
| Shei, A./2013 [7] | Expanding coverage rate of the PBF | Improved access to healthcare | Reduction of health inequalities | Congenital malformation |
| Silva, A.A./2010 [39] | _ | Healthcare during pregnancy/early medical interventions | Socioeconomic conditions/maternal education | LBWP |
| Silva, A.L.D./2016 [40] | _ | Hospital quality/increased use of health private sector | _ | LBW |
| Verona, A./2010 [41] | _ | _ | Maternal religious involvement, parity and region | _ |
| Vieira-Meyer, A./2019 [42] | FHS and PBF coverage rate | Quality and effectiveness of FHS | Socioeconomic conditions/Human Development Index/family attitude towards health | _ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bugelli, A.; Borgès Da Silva, R.; Dowbor, L.; Sicotte, C. The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 6464. https://doi.org/10.3390/ijerph18126464
Bugelli A, Borgès Da Silva R, Dowbor L, Sicotte C. The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(12):6464. https://doi.org/10.3390/ijerph18126464
Chicago/Turabian StyleBugelli, Alexandre, Roxane Borgès Da Silva, Ladislau Dowbor, and Claude Sicotte. 2021. "The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 12: 6464. https://doi.org/10.3390/ijerph18126464
APA StyleBugelli, A., Borgès Da Silva, R., Dowbor, L., & Sicotte, C. (2021). The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review. International Journal of Environmental Research and Public Health, 18(12), 6464. https://doi.org/10.3390/ijerph18126464