
Estimating the Burden of Alcohol on Ambulance Callouts through Development and Validation of an Algorithm Using Electronic Patient Records

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Dataset
2.2. Assessment of Callouts as Alcohol-Related
2.3. Algorithm Development
- (a)
- Cleaning the extracted sections of text in the dataset for both alcohol-related and misleading terms (e.g., removing extra spaces, removing punctuation and excluding the “stop words”).
- (b)
- Identifying words common to the callouts classified by alcohol-related based on their frequency (recurrence in more than 2.5% of alcohol-related callouts) and expert opinion (e.g., extra words identifying unambiguously alcohol-related callouts such as names of specific beverages appearing in some of the remaining records classified as alcohol-related).
- (c)
- Looking at the recurrence of words identified in (b) within the misleading terms. Focusing on the combination of one word before and one word after the words in (b) within the misleading terms. Identifying the most frequent combinations.
- (d)
- Identifying and correcting the most common spelling errors in ePRFs of words identified in (b) and (c).
- (e)
- Identifying every callout as “alcohol-related” whenever there was at least one of the “alcohol-related terms”, except those excluded by the combinations in point (c).
2.4. Assesment of Algorithm Performances
2.5. Algorithm Application to Full SAS Dataset
3. Results
3.1. Algorithm Performance
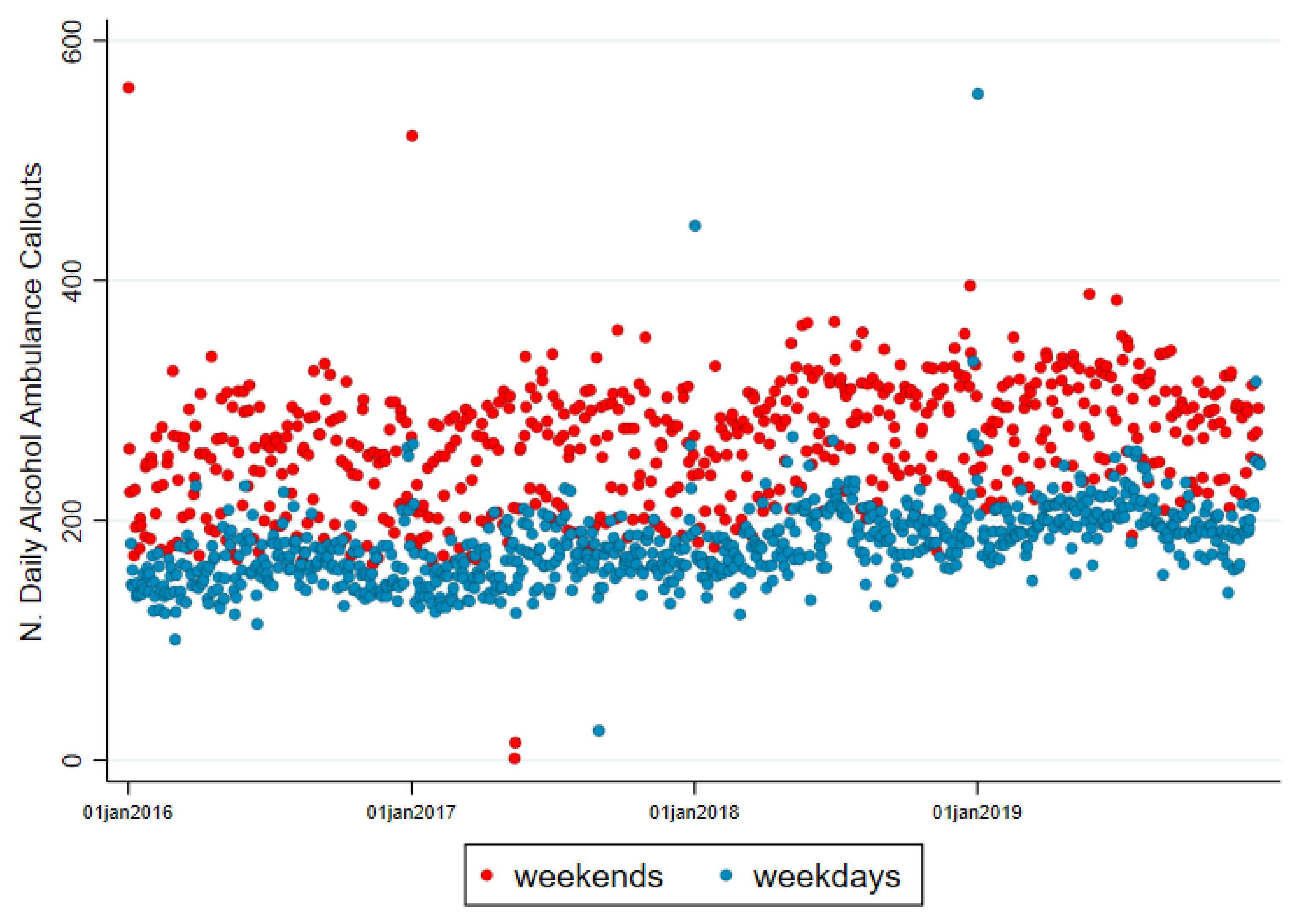
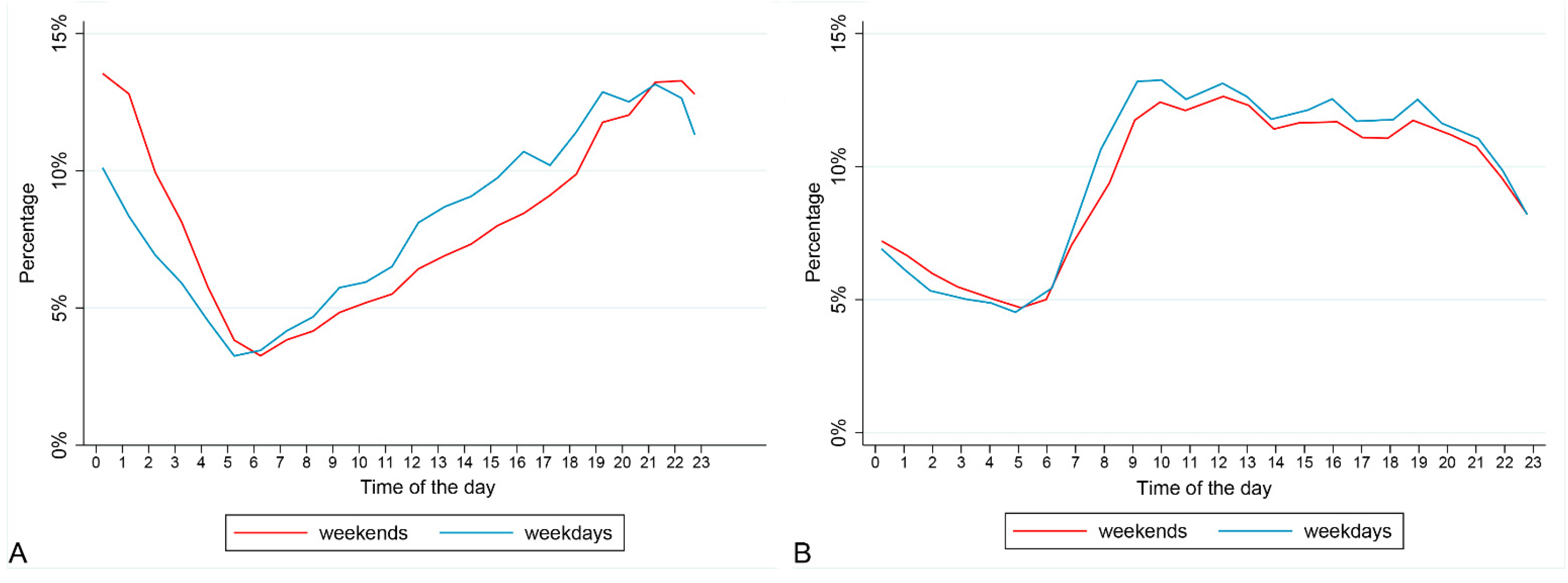
3.2. Alcohol-Related Callouts
4. Discussion
4.1. Alcohol-Related Ambulance Callouts
4.2. Strengths and Limitations of the Algorithm
4.3. Further Opportunities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| List of Stop Words: |
|---|
| a about above after again against all am an and are aren’t as at be because been before being below between both but by can’t cannot could couldn’t did didn’t do does doesn’t doing don’t down during each few for from further had hadn’t has hasn’t have haven’t having he he’d he’ll he’s her here here’s hers herself him himself his how how’s i i’d i’ll i’m i’ve if in into is isn’t it it’s its itself let’s me more most mustn’t my myself nor notof off on once only or other ought our ours out over own same shan’t she she’d she’ll she’s should shouldn’t so some such than that that’s the their theirs them themselves then there there’s these they they’d they’ll they’re they’ve this those through to too under until up very was wasn’t we we’d we’ll we’re we’ve were weren’t what what’s when when’s where where’s which while who who’s whom why why’s with won’t would wouldn’t you you’d you’ll you’re you’ve your yours yourself yourselves |
| Main Word | Spelling Errors and Word Declination, Changed into Main Word |
|---|---|
| alcohol | alco alcoholpt alcoholic nalcohol alchol alcoh alccohol alcoholism alcohn alcohohol alcohhol |
| drink | drinks drinking drinkin pdrink rdrink drin drinkn drinker drinknig drinkingpt drinki drank |
| intox | intoxicated intoxication intoxicted intoxicat intoxicate intoxication |
| vodka | vodca vodkapt vodkas |
| bottle | bottles bottl bott |
| drunk | ndrunk |
| buckfast | backfats bukfast bakfast buckfasts |
| whisky | whiskey wiski whiskei whiskys whiskes whiskeys whiskies |
| denies | deny deniese deni denied |
| since | ince sinc |
| cider | ciders |
| gin | gins |
| beer | beers |
References
- Institute of Alcohol Studies. Alcohol’s Impact on Emergency Services. 2015. Available online: https://www.ias.org.uk/wp-content/uploads/2020/09/rp18102015.pdf (accessed on 2 June 2021).
- London Ambulance Service. Alcohol-Related 999 Incidents. 2020. Available online: https://www.londonambulance.nhs.uk/news-2/alcohol-related-999-incidents/#:~:text=Alcohol%2Drelated%20incidents%20make%20up,cent%20of%20our%20total%20workload (accessed on 2 June 2021).
- Martin, N.; Newbury-Birch, D.; Duckett, J.; Mason, H.; Shen, J.; Shevills, C.; Kaner, E. A retrospective analysis of the nature, extent and cost of alcohol-related emergency calls to the ambulance service in an English region. Alcohol Alcohol. 2012, 47, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Scottish Ambualnce Service. The Impact of Alcohol on the Scottish Ambulance Service Summary of a Survey of Frontline Staff in 2015; Scottish Ambualnce Service: Glasgow, UK, 2015. [Google Scholar]
- Lubman, D.I.; Matthews, S.; Heilbronn, C.; Killian, J.J.; Ogeil, R.P.; Lloyd, B.; Witt, K.; Crossin, R.; Smith, K.; Bosley, E. The National Ambulance Surveillance System: A novel method for monitoring acute alcohol, illicit and pharmaceutical drug related-harms using coded Australian ambulance clinical records. PLoS ONE 2020, 15, e0228316. [Google Scholar] [CrossRef]
- Dietze, P.M.; Cvetkovski, S.; Rumbold, G.; Miller, P. Ambulance attendance at heroin overdose in Melbourne: The establishment of a database of ambulance service records. Drug Alcohol Rev. 2000, 19, 27–33. [Google Scholar] [CrossRef]
- Degenhardt, L.; Hall, W.; Adelstein, B.-A. Ambulance Calls to Suspected Drug Overdoses: Analysis of New South Wales Patterns July 1997 to June 1999; National Drug and Alcohol Research Centre Sydney: Randwick, Australia, 2000. [Google Scholar]
- Ogeil, R.P.; Room, R.; Matthews, S.; Lloyd, B. Alcohol and burden of disease in Australia: The challenge in assessing consumption. Aust. N. Z. J. Public Health 2015, 39, 121–123. [Google Scholar] [CrossRef]
- Morral, A.R.; McCaffrey, D.; Iguchi, M.Y. Hardcore drug users claim to be occasional users: Drug use frequency underreporting. Drug Alcohol Depend. 2000, 57, 193–202. [Google Scholar] [CrossRef]
- Monge, S.; Duijster, J.; Kommer, G.J.; van de Kassteele, J.; Donker, G.A.; Krafft, T.; Engelen, P.; Valk, J.P.; de Waard, J.; de Nooij, J. Use of ambulance dispatch calls for surveillance of severe acute respiratory infections. Emerg. Infect. Dis. 2020, 26, 148. [Google Scholar] [CrossRef] [PubMed]
- Mostashari, F.; Fine, A.; Das, D.; Adams, J.; Layton, M. Use of ambulance dispatch data as an early warning system for communitywide influenzalike illness, New York City. J. Urban Health 2003, 80, i43–i49. [Google Scholar] [PubMed]
- Duijster, J.W.; Doreleijers, S.D.; Pilot, E.; van der Hoek, W.; Kommer, G.J.; van der Sande, M.A.; Krafft, T.; van Asten, L.C. Utility of emergency call centre, dispatch and ambulance data for syndromic surveillance of infectious diseases: A scoping review. Eur. J. Public Health 2020, 30, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Bork, K.; Klein, B.; Molbak, K.; Trautner, S.; Pedersen, U.; Heegaard, E. Surveillance of ambulance dispatch data as a tool for early warning. Eurosurveillance 2006, 11, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Vergouwe, Y.; Royston, P.; Moons, K.G. Prognosis and prognostic research: Validating a prognostic model. BMJ 2009, 338, b605. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Desrosiers, M.; DeWerd, L.; Deye, J.; Lindsay, P.; Murphy, M.K.; Mitch, M.; Macchiarini, F.; Stojadinovic, S.; Stone, H. The importance of dosimetry standardization in radiobiology. J. Res. Natl. Inst. Stand. Technol. 2013, 118, 403. [Google Scholar] [CrossRef] [PubMed]
- Public Health Scotland. Scottish Ambulance Service, Expenditure and Statistics, by Board Area. Data and Intelligence/Previously ISD Scotland/Finance Data Files. 2021. Available online: https://beta.isdscotland.org/topics/finance/file-listings-fy-2019-to-2020/ (accessed on 2 June 2021).
- Martineau, F.; Tyner, E.; Lorenc, T.; Petticrew, M.; Lock, K. Population-level interventions to reduce alcohol-related harm: An overview of systematic reviews. Prev. Med. 2013, 57, 278–296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy to Reduce the Harmful Use of Alcohol; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Herald Scotland. Online Drinking a Factor in 90,000 Ambulance Call-Outs over Four Years. 2020. Available online: https://www.heraldscotland.com/news/18591698.drinking-factor-90-000-ambulance-call-outs-four-years/ (accessed on 2 June 2021).
- Elizabeth, A.; Richardson, N.K.S.; Jamie, P.; Richard, M. Alcohol-Related Illness and Death in Scottish Neighbourhoods: Is There a Relationship with the Number of Alcohol Outlets? 2014. Available online: https://www.alcohol-focus-scotland.org.uk/media/65042/Alcohol-outlet-density-and-harm-report.pdf (accessed on 2 June 2021).
- Sutherland, A.; Strang, L.; Stepanek, M.; Giacomantonio, C.; Boyle, A. Using Ambulance Data for Violence Prevention; RAND Corporation: Cambridge, UK, 2017. [Google Scholar]



| Main Word | Combination of Words to Exclude |
|---|---|
| Alcohol | “since alcohol” “any alcohol” “no alcohol” “or alcohol” “denies alcohol” “alcohol detox” “alcohol withdrawal” |
| Drink | “only drink” “any drink” “energy drink” “denies drink” “drink water” “not drink” |
| Intox | “appear intox” “not intox” |
| Bottle | “water bottle” “glass bottle” |
| Whisky | “one whisky” |
| Statistic | Manual Algorithm | ML Algorithm | Alcohol Flag |
|---|---|---|---|
| Sensitivity | 0.941 | 0.942 | 0.380 |
| Specificity | 0.996 | 0.996 | 1.000 |
| Accuracy | 0.986 | 0.987 | 0.890 |
| Alcohol flag = current flag used by SAS to record alcohol-related callouts | |||
| Alcohol-Related Callouts no. (%) | Non-Alcohol-Related Callouts no. (%) | Alcohol-Related Callouts as % of Total Callouts | |
|---|---|---|---|
| Total | 86,780 | 449,756 | 16.2% |
| Day of the week | |||
| Sunday | 15,663 (18.1) | 65,447 (14.6) | 19.3% |
| Monday | 10,746 (12.4) | 65,509 (14.6) | 14.1% |
| Tuesday | 10,657 (12.3) | 63,925 (14.2) | 14.3% |
| Wednesday | 10,250 (11.8) | 62,203 (13.8) | 14.1% |
| Thursday | 10,707 (12.3) | 63,349 (14.1) | 14.5% |
| Friday | 12,526 (14.4) | 63,806 (14.2) | 16.4% |
| Saturday | 16,231 (18.7) | 65,517 (14.6) | 19.9% |
| Month of the year | |||
| January | 7033 (8.1) | 39,054 (8.7) | 15.3% |
| February | 6586 (7.6) | 34,591 (7.7) | 16.0% |
| March | 7410 (8.5) | 36,851 (8.2) | 16.7% |
| April | 7297 (8.4) | 36,260 (8.1) | 16.8% |
| May | 7451 (8.6) | 37,463 (8.3) | 16.6% |
| June | 7622 (8.8) | 36,957 (8.2) | 17.1% |
| July | 7727 (8.9) | 37,258 (8.3) | 17.2% |
| August | 7527 (8.7) | 37,182 (8.3) | 16.8% |
| September | 7020 (8.1) | 37,329 (8.3) | 15.8% |
| October | 6889 (7.9) | 38,250 (8.5) | 15.3% |
| November | 6855 (7.9) | 38,129 (8.5) | 15.2% |
| December | 7363 (8.5) | 40,432 (9.0) | 15.4% |
| Emergency code1 | |||
| Green | 147 (0.2) | 965 (0.2) | 13.2% |
| Yellow | 48,250 (55.6) | 242,937 (54.0) | 16.6% |
| Amber | 19,819 (22.8) | 130,870 (29.1) | 13.2% |
| Red | 16,563 (19.1) | 63,362 (14.1) | 20.7% |
| Purple | 1976 (2.3) | 11,499 (2.6) | 14.7% |
| Unknown | 25 (0.03) | 123 (0.03) | 16.9% |
| Age group (years)2 | |||
| 0–24 | 12,758 (14.7) | 41,298 (10.4) | 23.6% |
| 25–39 | 16,863 (19.4) | 48,088 (12.1) | 26.0% |
| 40–54 | 19,632 (22.6) | 55,252 (13.9) | 26.2% |
| 55–69 | 16,834 (19.4) | 76,461 (19.2) | 18.0% |
| 70+ | 12,283 (14.2) | 176,228 (44.4) | 6.5% |
| Sex3 | |||
| Female | 31,612 (38.1) | 218,471 (52.3) | 12.6% |
| Male | 51,378 (61.9) | 199,634 (47.7) | 20.4% |
| Scottish Index of multiple deprivation decile for patient home address4 | |||
| 1 (most deprived) | 7284 (21.8) | 29,836 (15.4) | 19.6% |
| 2 | 5246 (15.6) | 25,681 (13.3) | 17.0% |
| 3 | 4554 (13.6) | 24,504 (12.7) | 15.7% |
| 4 | 3919 (11.7) | 21,655 (11.2) | 15.3% |
| 5 | 3111 (9.3) | 19,167 (9.9) | 14.0% |
| 6 | 2491 (7.4) | 17,684 (9.1) | 12.4% |
| 7 | 2241 (6.7) | 16,236 (8.4) | 12.1% |
| 8 | 1699 (5.1) | 14,310 (7.4) | 10.6% |
| 9 | 1591 (4.8) | 13,094 (6.8) | 10.8% |
| 10 (least deprived) | 1306 (3.9) | 11,601 (6.0) | 10.1% |
| Scottish Index of multiple deprivation decile for callout location5 | |||
| 1 (most deprived) | 17,473 (20.1) | 66,680 (15.0) | 20.8% |
| 2 | 12,568 (14.5) | 57,671 (13.0) | 17.9% |
| 3 | 11,691 (13.5) | 54,405 (12.2) | 17.7% |
| 4 | 10,102 (11.6) | 49,029 (11.0) | 17.1% |
| 5 | 8715 (10.0) | 45,223 (10.2) | 16.2% |
| 6 | 7355 (8.5) | 44,378 (10.0) | 14.2% |
| 7 | 5795 (6.7) | 37,472 (8.4) | 13.4% |
| 8 | 5286 (6.1) | 34,927 (7.8) | 13.2% |
| 9 | 3695 (4.3) | 29,427 (6.6) | 11.2% |
| 10 (least deprived) | 3383 (3.9) | 26,248 (5.9) | 11.4% |
| Rural/urban areas classified by callout location6 | |||
| Large urban area | 36,107 (41.6) | 159,817 (36.0) | 18.4% |
| Other urban area | 32,514 (37.5) | 164,774 (37.2) | 16.5% |
| Accessible small town | 6154 (7.1) | 36,425 (8.2) | 14.5% |
| Remote small town | 3046 (3.5) | 17,292 (3.9) | 15.0% |
| Accessible rural area | 5360 (6.2) | 42,732 (0.1) | 11.1% |
| Remote rural area | 2555 (2.9) | 22,470 (0.05) | 10.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manca, F.; Lewsey, J.; Waterson, R.; Kernaghan, S.M.; Fitzpatrick, D.; Mackay, D.; Angus, C.; Fitzgerald, N. Estimating the Burden of Alcohol on Ambulance Callouts through Development and Validation of an Algorithm Using Electronic Patient Records. Int. J. Environ. Res. Public Health 2021, 18, 6363. https://doi.org/10.3390/ijerph18126363
Manca F, Lewsey J, Waterson R, Kernaghan SM, Fitzpatrick D, Mackay D, Angus C, Fitzgerald N. Estimating the Burden of Alcohol on Ambulance Callouts through Development and Validation of an Algorithm Using Electronic Patient Records. International Journal of Environmental Research and Public Health. 2021; 18(12):6363. https://doi.org/10.3390/ijerph18126363
Chicago/Turabian StyleManca, Francesco, Jim Lewsey, Ryan Waterson, Sarah M. Kernaghan, David Fitzpatrick, Daniel Mackay, Colin Angus, and Niamh Fitzgerald. 2021. "Estimating the Burden of Alcohol on Ambulance Callouts through Development and Validation of an Algorithm Using Electronic Patient Records" International Journal of Environmental Research and Public Health 18, no. 12: 6363. https://doi.org/10.3390/ijerph18126363
APA StyleManca, F., Lewsey, J., Waterson, R., Kernaghan, S. M., Fitzpatrick, D., Mackay, D., Angus, C., & Fitzgerald, N. (2021). Estimating the Burden of Alcohol on Ambulance Callouts through Development and Validation of an Algorithm Using Electronic Patient Records. International Journal of Environmental Research and Public Health, 18(12), 6363. https://doi.org/10.3390/ijerph18126363