
Immunohistochemical Expression of Serine and Arginine-Rich Splicing Factor 1 (SRSF1) in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Study

 ,
,  ,
,  ,
,  ,
, 
 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement and Sample Collection
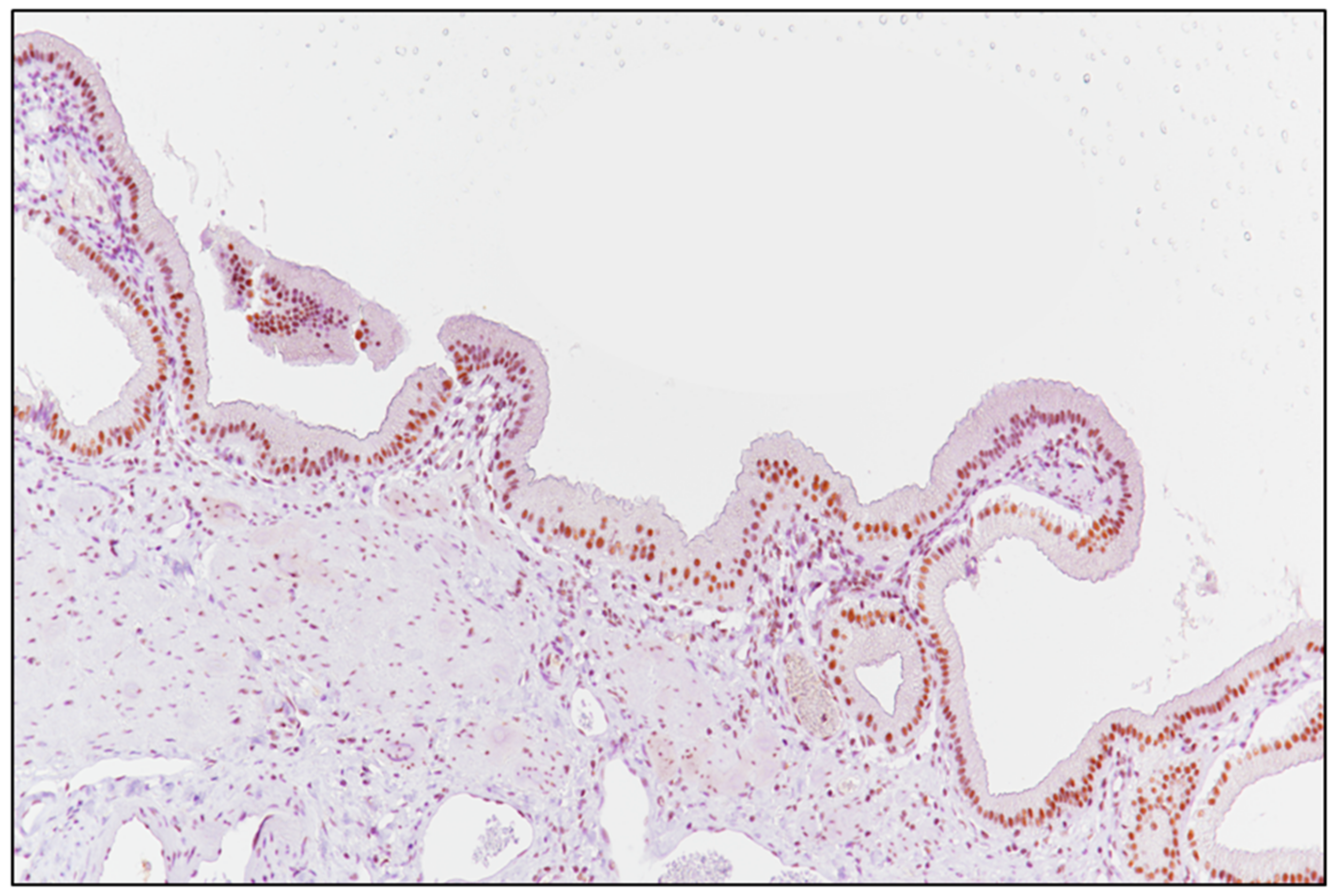
2.2. Laboratory Tests and Evaluation of SRSF1 Immunohistochemistry
2.3. Blood Vascular Microvessel Density (MVD)
2.4. Statistical Analysis
3. Results
3.1. Clinico-Pathological Features of the Patients Included in the Study
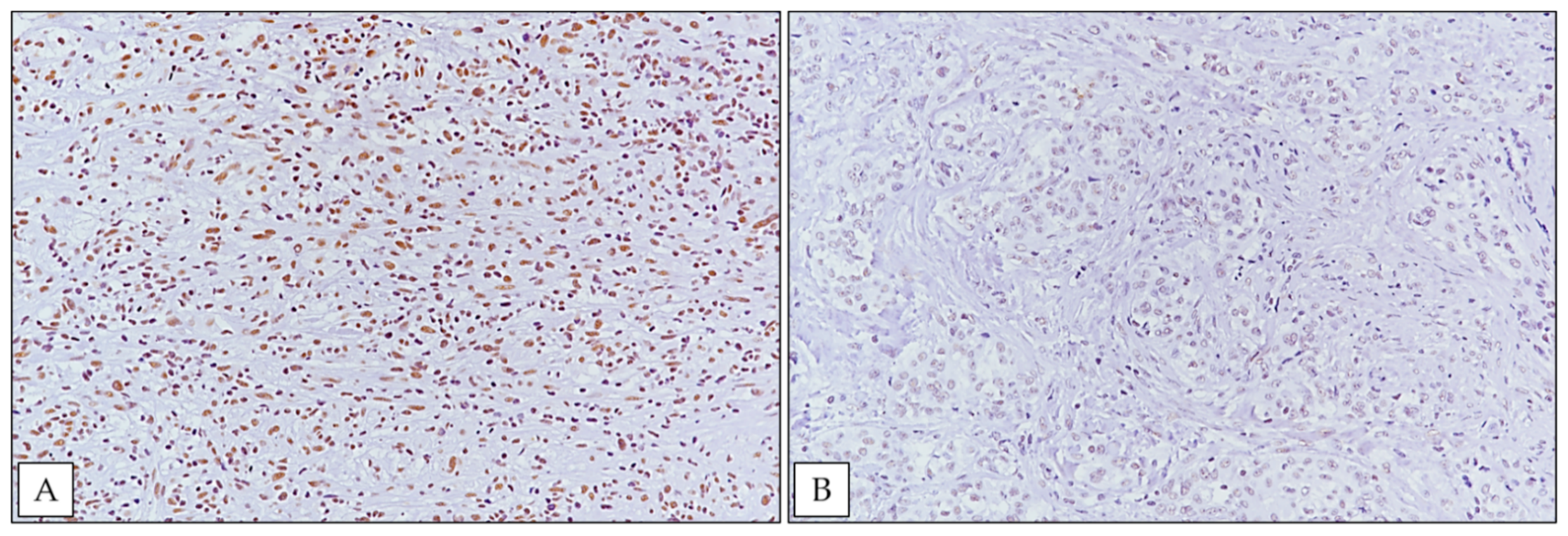
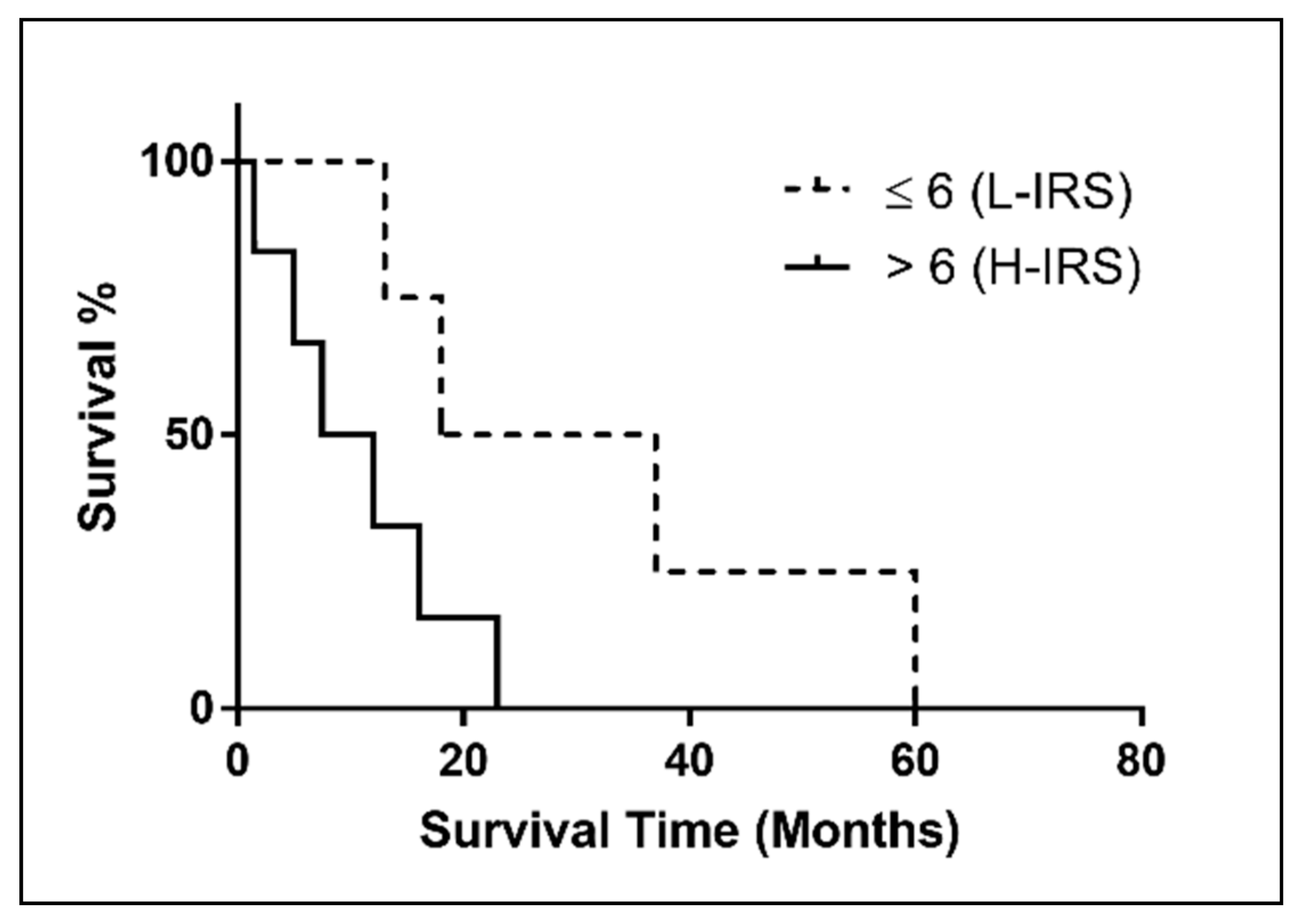
3.2. SRSF1 Immunohistochemical Expression and Its Correlation with Prognosis
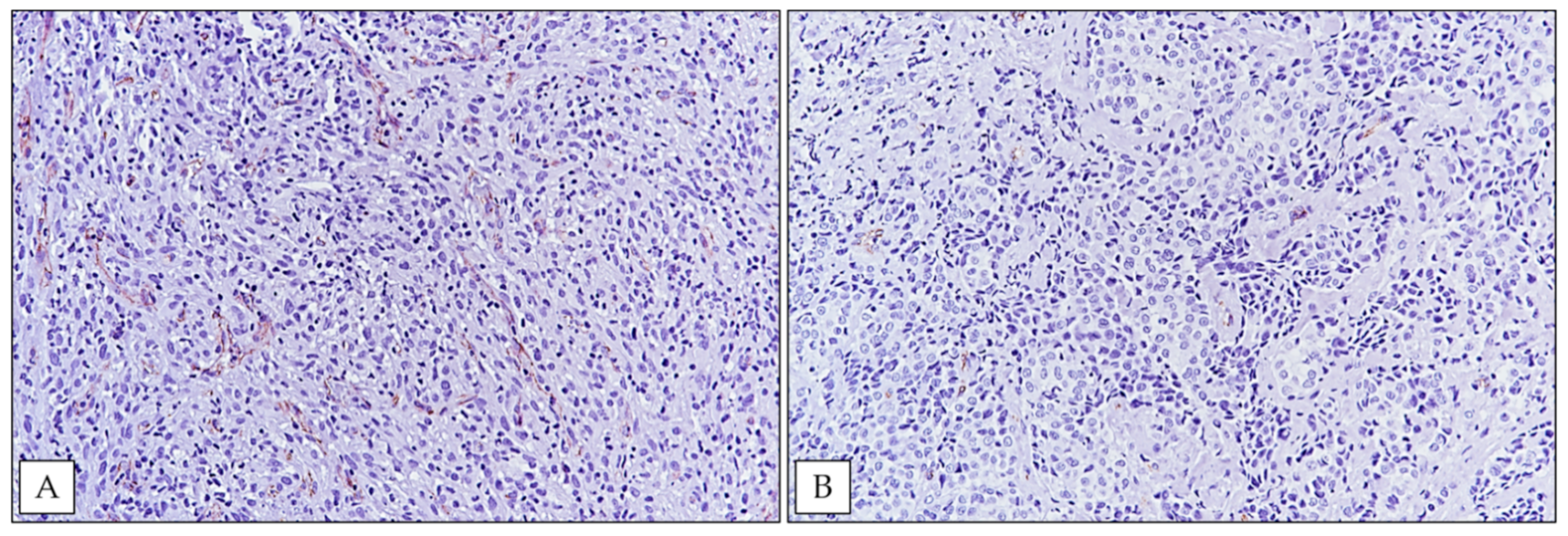
3.3. SRSF1 Immunoexpression Was Positively Associated with MVD Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tomasson, K.; Gudmundsson, G.; Briem, H.; Rafnsson, V. Malignant mesothelioma incidence by nation-wide cancer registry: A population-based study. J. Occup. Med. Toxicol. 2016, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Baas, P.; Fennell, D.; Kerr, K.M.; Van Schil, P.E.; Haas, R.L.; Peters, S.; ESMO Guidelines Committee. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. S5), v31–v39. [Google Scholar] [CrossRef]
- Arnold, D.T.; Maskell, N.A. Biomarkers in mesothelioma. Ann. Clin. Biochem. 2018, 55, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Filetti, V.; Vitale, E.; Broggi, G.; Hagnäs, M.P.; Candido, S.; Spina, A.; Lombardo, C. Update of in vitro, in vivo and ex vivo fluoro-edenite effects on malignant mesothelioma: A systematic review (Review). Biomed. Rep. 2020, 13, 60. [Google Scholar] [CrossRef]
- Comba, P.; Gianfagna, A.; Paoletti, L. Pleural mesothelioma cases in Biancavilla are related to a new fluoro-edenite fibrous amphibole. Arch. Environ. Health 2003, 58, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Paoletti, L.; Batisti, D.; Bruno, C.; Di Paola, M.; Gianfagna, A.; Mastrantonio, M.; Nesti, M.; Comba, P. Unusually high incidence of malignant pleural mesothelioma in a town of eastern Sicily: An epidemiological and environmental study. Arch. Environ. Health 2000, 55, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Grosse, Y.; Loomis, D.; Guyton, K.Z.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Scoccianti, C.; Mattock, H.; et al. International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of fluoro-edenite, silicon carbide fibres and whiskers, and carbon nanotubes. Lancet Oncol. 2014, 15, 1427–1428. [Google Scholar] [CrossRef]
- Caltabiano, R.; Loreto, C.; Vitale, E.; Matera, S.; Miozzi, E.; Migliore, M.; Angelico, G.; Tumino, R.; Ledda, C.; Rapisarda, V. Fibulin-3 immunoexpression in malignantmesothelioma due to fluoro-edenite: A preliminary report. Future Oncol. 2018, 14, 53–57. [Google Scholar] [CrossRef]
- Rapisarda, V.; Ledda, C.; Ricceri, V.; Arena, F.; Musumeci, A.; Marconi, A.; Fago, L.; Bracci, M.; Santarelli, L.; Ferrante, M. Detection of pleural plaques in workers exposed to inhalation of natural fluoro-edenite fibres. Oncol. Lett. 2015, 9, 2046–2052. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, V.; Ledda, C.; Migliore, M.; Salemi, R.; Musumeci, A.; Bracci, M.; Marconi, A.; Loreto, C.; Libra, M. FBLN-3 as a biomarker of pleural plaques in workers occupationally exposed to carcinogenic fibers: A pilot study. Future Oncol. 2015, 11, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Loreto, C.; Pomara, C.; Rapisarda, G.; Fiore, M.; Ferrante, M.; Bracci, M.; Santarelli, L.; Fenga, C.; Rapisarda, V. Sheep lymph-nodes as a biological indicator of environmental exposure to fluoro-edenite. Environ. Res. 2016, 147, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Pomara, C.; Bracci, M.; Mangano, D.; Ricceri, V.; Musumeci, A.; Ferrante, M.; Musumeci, G.; Loreto, C.; Fenga, C.; et al. Natural carcinogenic fiber and pleural plaques assessment in a general population: A cross-sectional study. Environ. Res. 2016, 150, 23–29. [Google Scholar] [CrossRef]
- Rapisarda, V.; Caltabiano, R.; Musumeci, G.; Castrogiovanni, P.; Ferrante, M.; Ledda, C.; Lombardo, C.; Graziano, A.C.E.; Cardile, V.; Loreto, C. Analysis of fibulin-3 after exposure to asbestos-like fibers. Environ. Res. 2017, 156, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Costa, C.; Matera, S.; Puglisi, B.; Costanzo, V.; Bracci, M.; Fenga, C.; Rapisarda, V.; Loreto, C. Immunomodulatory effects in workers exposed to naturally occurring asbestos fibers. Mol. Med. Rep. 2017, 15, 3372–3378. [Google Scholar] [CrossRef] [PubMed]
- Putzu, M.G.; Bruno, C.; Zona, A.; Massiccio, M.; Pasetto, R.; Piolatto, P.G.; Comba, P. Fluoro-edenitic fibres in the sputum of subjects from Biancavilla (Sicily): A pilot study. Environ. Health 2006, 5, 20. [Google Scholar] [CrossRef][Green Version]
- Loreto, C.; Rapisarda, V.; Carnazza, M.L.; Musumeci, G.; Valentino, M.; Fenga, C.; Martinez, G. Fluoro-edenite fibres induce lungcellapoptosis: An in vivo study. Histol. Histopathol. 2008, 23, 319–326. [Google Scholar] [CrossRef]
- Angelico, G.; Ieni, A.; Caltabiano, R.; Zeppa, P.; Tuccari, G. Aquaporin-1 expression in fluoro-edenite-induced mesothelioma effusions: An approach by cell-block procedure. Cytopathology. 2018, 29, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Angelico, G.; Caltabiano, R.; Loreto, C.; Ieni, A.; Tuccari, G.; Ledda, C.; Rapisarda, V. Immunohistochemical Expression of Aquaporin-1 in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Report. Int. J. Mol. Sci. 2018, 19, 685. [Google Scholar] [CrossRef] [PubMed]
- Kędzierska, H.; Piekiełko-Witkowska, A. Splicing factors of SR and hnRNP families as regulators of apoptosis in cancer. Cancer Lett. 2017, 396, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Anczuków, O.; Akerman, M.; Cléry, A.; Wu, J.; Shen, C.; Shirole, N.H.; Raimer, A.; Sun, S.; Jensen, M.A.; Hua, Y.; et al. SRSF1-Regulated Alternative Splicing in Breast Cancer. Mol. Cell 2015, 60, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Wang, R.; Li, X.; Yu, L.; Hua, D.; Sun, C.; Shi, C.; Luo, W.; Rao, C.; Jiang, Z.; et al. Splicing factor SRSF1 promotes gliomagenesis via oncogenic splice-switching of MYO1B. J. Clin. Investig. 2019, 129, 676–693. [Google Scholar] [CrossRef] [PubMed]
- Sheng, J.; Zhao, Q.; Zhao, J.; Zhang, W.; Sun, Y.; Qin, P.; Lv, Y.; Bai, L.; Yang, Q.; Chen, L.; et al. SRSF1 modulates PTPMT1 alternative splicing to regulate lung cancer cell radioresistance. EBioMedicine 2018, 38, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Malakar, P.; Shilo, A.; Mogilevsky, A.; Stein, I.; Pikarsky, E.; Nevo, Y.; Benyamini, H.; Elgavish, S.; Zong, X.; Prasanth, K.V.; et al. Long Noncoding RNA MALAT1 Promotes Hepatocellular Carcinoma Development by SRSF1 Upregulation and mTOR Activation. Cancer Res. 2017, 77, 1155–1167. [Google Scholar] [CrossRef]
- Li, H.; Guo, S.; Zhang, M.; Li, L.; Wang, F.; Song, B. Long non-coding RNA AGAP2-AS1 accelerates cell proliferation, migration, invasion and the EMT process in colorectal cancer via regulating the miR-4,668-3p/SRSF1 axis. J. Gene Med. 2020, 22, e3250. [Google Scholar] [CrossRef] [PubMed]
- Cammarata, F.P.; Forte, G.I.; Broggi, G.; Bravatà, V.; Minafra, L.; Pisciotta, P.; Calvaruso, M.; Tringali, R.; Tomasello, B.; Torrisi, F.; et al. Molecular Investigation on a Triple Negative Breast Cancer Xenograft Model Exposed to Proton Beams. Int. J. Mol. Sci. 2020, 21, 6337. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Filetti, V.; Ieni, A.; Rapisarda, V.; Ledda, C.; Vitale, E.; Varricchio, S.; Russo, D.; Lombardo, C.; Tuccari, G.; et al. MacroH2A1 Immunoexpression in Breast Cancer. Front. Oncol. 2020, 10, 1519. [Google Scholar] [CrossRef]
- Loreto, C.; La Rocca, G.; Anzalone, R.; Caltabiano, R.; Vespasiani, G.; Castorina, S.; Ralph, D.J.; Cellek, S.; Musumeci, G.; Giunta, S.; et al. The role of intrinsic pathway in apoptosis activation and progression in Peyronie’s disease. BioMed Res. Int. 2014, 2014, 616149. [Google Scholar] [CrossRef]
- Broggi, G.; Ieni, A.; Russo, D.; Varricchio, S.; Puzzo, L.; Russo, A.; Reibaldi, M.; Longo, A.; Tuccari, G.; Staibano, S.; et al. The Macro-Autophagy-Related Protein Beclin-1 Immunohistochemical Expression Correlates with Tumor Cell Type and Clinical Behavior of Uveal Melanoma. Front. Oncol. 2020, 10, 589849. [Google Scholar] [CrossRef]
- Barbagallo, D.; Caponnetto, A.; Brex, D.; Mirabella, F.; Barbagallo, C.; Lauretta, G.; Morrone, A.; Certo, F.; Broggi, G.; Caltabiano, R.; et al. CircSMARCA5 Regulates VEGFA mRNA Splicing and Angiogenesis in Glioblastoma Multiforme Through the Binding of SRSF1. Cancers 2019, 11, 194. [Google Scholar] [CrossRef]
- Galateau-Salle, F.; Churg, A.; Roggli, V.; Travis, W.D. World Health Organization CoMMittee for Tumors of the Pleura. The 2015 World Health Organization Classification of Tumors of the Pleura: Advances since the 2004 Classification. J. Thorac. Oncol. 2016, 11, 142–154. [Google Scholar] [CrossRef]
- Barbagallo, D.; Caponnetto, A.; Cirnigliaro, M.; Brex, D.; Barbagallo, C.; D’Angeli, F.; Morrone, A.; Caltabiano, R.; Barbagallo, G.M.; Ragusa, M.; et al. CircSMARCA5 Inhibits Migration of Glioblastoma Multiforme Cells by Regulating a Molecular Axis Involving Splicing Factors SRSF1/SRSF3/PTB. Int. J. Mol. Sci. 2018, 19, 480. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, D.; Caponnetto, A.; Barbagallo, C.; Battaglia, R.; Mirabella, F.; Brex, D.; Stella, M.; Broggi, G.; Altieri, R.; Certo, F.; et al. The GAUGAA Motif Is Responsible for the Binding between circSMARCA5 and SRSF1 and Related Downstream Effects on Glioblastoma Multiforme Cell Migration and Angiogenic Potential. Int. J. Mol. Sci. 2021, 22, 1678. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Salvatorelli, L.; Barbagallo, D.; Certo, F.; Altieri, R.; Tirrò, E.; Massimino, M.; Vigneri, P.; Guadagno, E.; Maugeri, G.; et al. Diagnostic Utility of the Immunohistochemical Expression of Serine and Arginine Rich Splicing Factor 1 (SRSF1) in the Differential Diagnosis of Adult Gliomas. Cancers 2021, 13, 2086. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age (Years) | Gender | Pathological Subtype | Survival Time (Months) | SRSF1 IS | SRSF1 ES | SRSF1 IRS | MVD (n/mm2) |
|---|---|---|---|---|---|---|---|---|
| 1 | 69 | M | Epithelioid | 1.5 | 3 | 3 | 9 | 132/mm2 |
| 2 | 50 | M | Biphasic (20% Epithelioid, 80% Sarcomatoid) | 16 | 3 | 4 | 12 | 103/mm2 |
| 3 | 69 | F | Sarcomatoid | 5 | 2 | 4 | 8 | 147/mm2 |
| 4 | 74 | F | Epithelioid | 13 | 2 | 2 | 4 | 84/mm2 |
| 5 | 85 | M | Epithelioid | 23 | 2 | 4 | 8 | 79/mm2 |
| 6 | 93 | F | Biphasic (40% Epithelioid, 60% Sarcomatoid) | 7.5 | 3 | 3 | 9 | 139/mm2 |
| 7 | 58 | F | Epithelioid | 18 | 2 | 3 | 6 | 88/mm2 |
| 8 | 55 | M | Epithelioid | 37 | 3 | 2 | 6 | 64/mm2 |
| 9 | 75 | M | Biphasic (40% Epithelioid, 60% Sarcomatoid) | 60 | 2 | 3 | 6 | 28/mm2 |
| 10 | 56 | M | Epithelioid | 12 | 2 | 4 | 8 | 94/mm2 |
| MVD | High SRSF1 | Low SRSF1 |
|---|---|---|
| High | 5 | 0 |
| Low | 1 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broggi, G.; Angelico, G.; Filetti, V.; Ledda, C.; Lombardo, C.; Vitale, E.; Rapisarda, V.; Loreto, C.; Caltabiano, R. Immunohistochemical Expression of Serine and Arginine-Rich Splicing Factor 1 (SRSF1) in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 6249. https://doi.org/10.3390/ijerph18126249
Broggi G, Angelico G, Filetti V, Ledda C, Lombardo C, Vitale E, Rapisarda V, Loreto C, Caltabiano R. Immunohistochemical Expression of Serine and Arginine-Rich Splicing Factor 1 (SRSF1) in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6249. https://doi.org/10.3390/ijerph18126249
Chicago/Turabian StyleBroggi, Giuseppe, Giuseppe Angelico, Veronica Filetti, Caterina Ledda, Claudia Lombardo, Ermanno Vitale, Venerando Rapisarda, Carla Loreto, and Rosario Caltabiano. 2021. "Immunohistochemical Expression of Serine and Arginine-Rich Splicing Factor 1 (SRSF1) in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Study" International Journal of Environmental Research and Public Health 18, no. 12: 6249. https://doi.org/10.3390/ijerph18126249
APA StyleBroggi, G., Angelico, G., Filetti, V., Ledda, C., Lombardo, C., Vitale, E., Rapisarda, V., Loreto, C., & Caltabiano, R. (2021). Immunohistochemical Expression of Serine and Arginine-Rich Splicing Factor 1 (SRSF1) in Fluoro-Edenite-Induced Malignant Mesothelioma: A Preliminary Study. International Journal of Environmental Research and Public Health, 18(12), 6249. https://doi.org/10.3390/ijerph18126249