
Comprehensive Geriatric Assessment and Clinical Outcomes in the Older People at the Emergency Department

 , , and
, , and
Abstract
1. Introduction
2. Methods
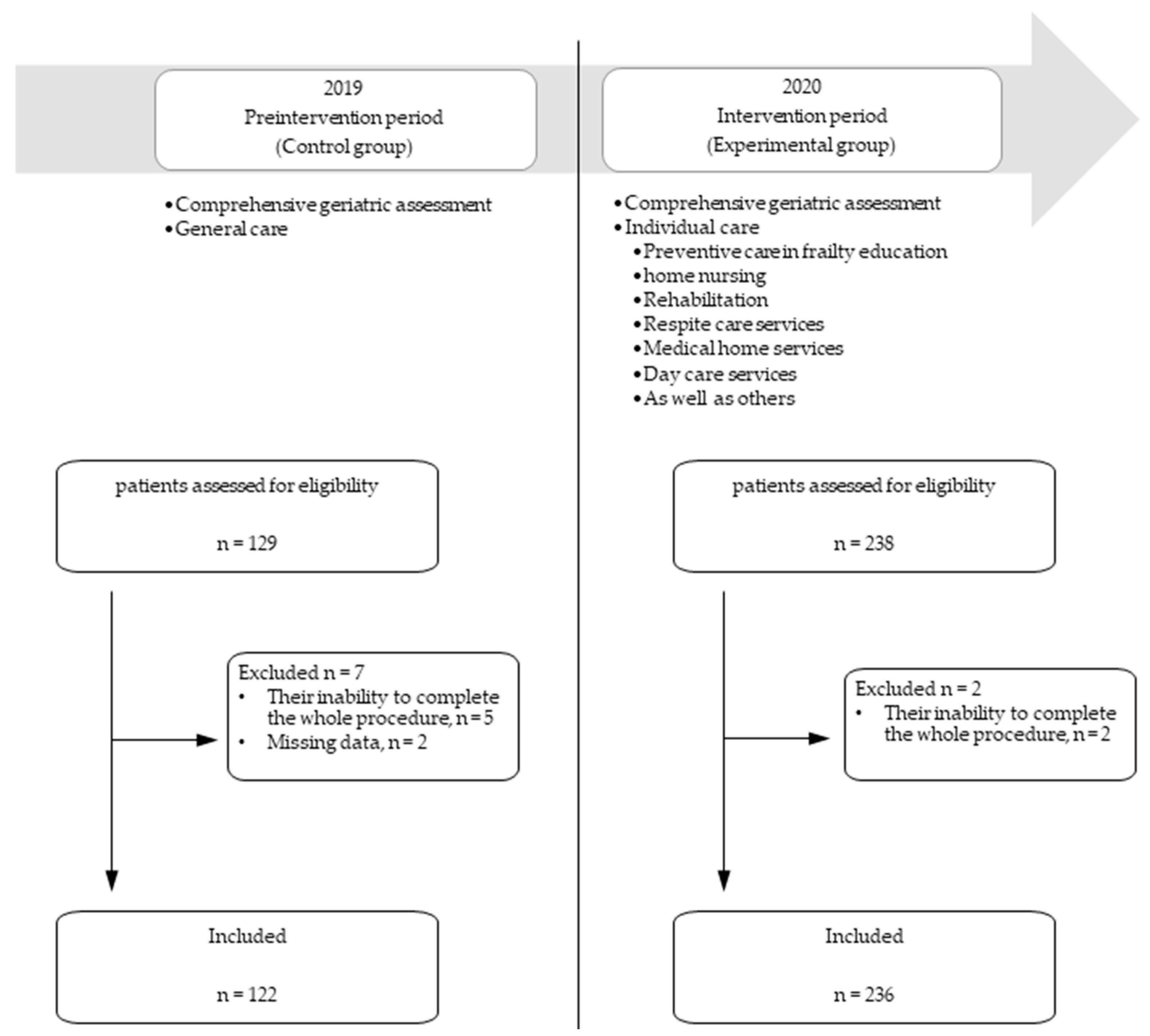
2.1. Study Design
2.2. Participants
2.3. Preintervention Period
2.4. Intervention Period
2.5. Outcome
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Huang, H.-H.; Chang, J.C.-Y.; Tseng, C.-C.; Yang, Y.-J.; Fan, J.-S.; Chen, Y.-C.; Peng, L.-N.; Yen, D.H.-T. Comprehensive geriatric assessment in the emergency department for the prediction of readmission among older patients: A 3-month follow-up study. Arch. Gerontol. Geriatr. 2021, 92, 104255. [Google Scholar] [CrossRef]
- Yim, V.W.T.; Graham, C.A.; Rainer, T.H. A comparison of emergency department utilization by elderly and younger adult patients presenting to three hospitals in Hong Kong. Int. J. Emerg. Med. 2009, 2, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Gerson, L.W.; Shvarch, L. Emergency medical service utilization by the elderly. Ann. Emerg. Med. 1982, 11, 610–612. [Google Scholar] [CrossRef]
- Sanders, A.B.; Morley, J.E. The older person and the emergency department. J. Am. Geriatr. Soc. 1993, 41, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Aminzadeh, F.; Dalziel, W.B. Older adults in the emergency department: A systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann. Emerg. Med. 2002, 39, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Downing, A.; Wilson, R. Older people’s use of Accident and Emergency services. Age Ageing 2005, 34, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Samaras, N.; Chevalley, T.; Samaras, D.; Gold, G. Older patients in the emergency department: A review. Ann. Emerg. Med. 2010, 56, 261–269. [Google Scholar] [CrossRef]
- Lowthian, J.A.; McGinnes, R.A.; Brand, C.A.; Barker, A.L.; Cameron, P.A. Discharging older patients from the emergency department effectively: A systematic review and meta-analysis. Age Ageing 2015, 44, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.C.; McKay, M.P.; Shaffer, A. Increasing rates of emergency department visits for elderly patients in the United States, 1993 to 2003. Ann. Emerg. Med. 2008, 51, 769–774. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Costello, M.; Small, C.; Spooner, L.; Flannery, A.; O’Reilly, L.; Heffernan, L.; Mannion, E.; Maughan, A.; Joyce, A.; et al. Comparison of Frailty Screening Instruments in the Emergency Department. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef]
- Ellis, G.; Marshall, T.; Ritchie, C. Comprehensive geriatric assessment in the emergency department. Clin. Interv. Aging 2014, 9, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians; American Geriatrics Society; Emergency Nurses Association; Society for Academic Emergency Medicine; Geriatric Emergency Department Guidelines Task Force. Geriatric emergency department guidelines. Ann. Emerg. Med. 2014, 63, e7–e25. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.M.; Freiermuth, C.E.; Shepherd-Banigan, M.; Ragsdale, L.; Eucker, S.A.; Goldstein, K.; Hastings, S.N.; Rodriguez, R.L.; Fulton, J.; Ramos, K.; et al. Emergency Department Interventions for Older Adults: A Systematic Review. J. Am. Geriatr. Soc. 2019, 67, 1516–1525. [Google Scholar] [CrossRef]
- Jay, S.; Whittaker, P.; Mcintosh, J.; Hadden, N. Can consultant geriatrician led comprehensive geriatric assessment in the emergency department reduce hospital admission rates? A systematic review. Age Ageing 2017, 46, 366–372. [Google Scholar] [CrossRef]
- Chen, T.-B.; Yiao, S.-Y.; Sun, Y.; Lee, H.-J.; Yang, S.-C.; Chiu, M.-J.; Chen, T.-F.; Lin, K.-N.; Tang, L.-Y.; Lin, C.-C.; et al. Comorbidity and dementia: A nationwide survey in Taiwan. PLoS ONE 2017, 12, e0175475. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Rankin, A.; Cadogan, C.A.; Patterson, S.M.; Kerse, N.; Cardwell, C.R.; Bradley, M.C.; Ryan, C.; Hughes, C. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 2018, 9, CD008165. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–53. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-F.; Huang, Y.-H.; Ju, L.-Y.; Weng, S.-C.; Lee, Y.-S.; Chou, Y.-Y.; Lin, C.-S.; Lin, S.-Y. Health-Related Quality of Life Measured by EQ-5D in Relation to Hospital Stay and Readmission in Elderly Patients Hospitalized for Acute Illness. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D.E.; Palmer, R.M.; Kresevic, D.M.; Fortinsky, R.H.; Kowal, J.; Chren, M.-M.; Landefeld, C.S. Acute care for elders units produced shorter hospital stays at lower cost while maintaining patients’ functional status. Health Aff. (Millwood) 2012, 31, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017, 9, CD006211. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Stuck, A.E.; Siu, A.L.; Wieland, D. Impacts of geriatric evaluation and management programs on defined outcomes: Overview of the evidence. J. Am. Geriatr. Soc. 1991, 39, 8S–16S. [Google Scholar] [CrossRef]
- Fry, M.; Fitzpatrick, L.; Considine, J.; Shaban, R.Z.; Curtis, K. Emergency department utilisation among older people with acute and/or chronic conditions: A multi-centre retrospective study. Int. Emerg. Nurs. 2018, 37, 39–43. [Google Scholar] [CrossRef]
- Gorichky, R.R. ED Care Coordination: An Effective Approach for At-Risk, Frail Older Adults. J. Emerg. Nurs. 2015, 41, 438–440. [Google Scholar] [CrossRef]
- Blomaard, L.C.; de Groot, B.; Lucke, J.A.; de Gelder, J.; Booijen, A.M.; Gussekloo, J.; Mooijaart, S.P. Implementation of the acutely presenting older patient (APOP) screening program in routine emergency department care: A before-after study. Z. Gerontol. Geriatr. 2021, 54, 113–121. [Google Scholar] [CrossRef]
- Gordon, E.H.; Peel, N.M.; Samanta, M.; Theou, O.; Howlett, S.E.; Hubbard, R.E. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 2017, 89, 30–40. [Google Scholar] [CrossRef]
- Gordon, E.H.; Hubbard, R.E. Differences in frailty in older men and women. Med. J. Aust. 2020, 212, 183–188. [Google Scholar] [CrossRef]
- Parker, S.G.; McCue, P.; Phelps, K.; McCleod, A.; Arora, S.; Nockels, K.; Kennedy, S.; Roberts, H.; Conroy, S. What is Comprehensive Geriatric Assessment (CGA)? An umbrella review. Age Ageing 2018, 47, 149–155. [Google Scholar] [CrossRef]
- Theou, O.; Campbell, S.; Malone, M.L.; Rockwood, K. Older Adults in the Emergency Department with Frailty. Clin. Geriatr. Med. 2018, 34, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.T.; Dent, E.; Alkhouri, H.; Kellett, J.; Williamson, M.; Asha, S.; Holdgate, A.; Mackenzie, J.; Winoto, L.; Fajardo-Pulido, D.; et al. Which frailty scale for patients admitted via Emergency Department? A cohort study. Arch. Gerontol. Geriatr. 2019, 80, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Stiffler, K.A.; Finley, A.; Midha, S.; Wilber, S.T. Frailty assessment in the emergency department. J. Emerg. Med. 2013, 45, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Joosten, E.; Demuynck, M.; Detroyer, E.; Milisen, K. Prevalence of frailty and its ability to predict in hospital delirium, falls, and 6-month mortality in hospitalized older patients. BMC Geriatr. 2014, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Pulok, M.H.; Theou, O.; van der Valk, A.M.; Rockwood, K. The role of illness acuity on the association between frailty and mortality in emergency department patients referred to internal medicine. Age Ageing 2020, 49, 1071–1079. [Google Scholar] [CrossRef]
- Michalski-Monnerat, C.; Carron, P.-N.; Nguyen, S.; Büla, C.; Mabire, C. Assessing Older Patients’ Vulnerability in the Emergency Department: A Study of InterRAI ED Screener Accuracy. J. Am. Geriatr. Soc. 2020, 68, 2914–2920. [Google Scholar] [CrossRef]
- Conroy, S.P.; Stevens, T.; Parker, S.G.; Gladman, J.R.F. A systematic review of comprehensive geriatric assessment to improve outcomes for frail older people being rapidly discharged from acute hospital: ‘interface geriatrics’. Age Ageing 2011, 40, 436–443. [Google Scholar] [CrossRef]
- van der Kluit, M.J.; Dijkstra, G.J.; de Rooij, S.E. The decision-making process for unplanned admission to hospital unveiled in hospitalised older adults: A qualitative study. BMC Geriatr. 2018, 18, 318. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.N.; Jones, C.M.C.; Richardson, T.M.; Conwell, Y.; Katz, P.; Schneider, S.M. Prevalence of depression and cognitive impairment in older adult emergency medical services patients. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 2011, 15, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Fogg, C.; Meredith, P.; Culliford, D.; Bridges, J.; Spice, C.; Griffiths, P. Cognitive impairment is independently associated with mortality, extended hospital stays and early readmission of older people with emergency hospital admissions: A retrospective cohort study. Int. J. Nurs. Stud. 2019, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Laurence, B.; Mncube-Barnes, F.M.; Laurence, S.S.; Woods, D.; Eiland, D. Depression and the Likelihood of Hospital Admission from the Emergency Department among Older Patients with HIV. J. Health Care Poor Underserved 2019, 30, 131–142. [Google Scholar] [CrossRef]
- Mackin, R.S.; Areán, P.A. Incidence and documentation of cognitive impairment among older adults with severe mental illness in a community mental health setting. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2009, 17, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Ligthart-Melis, G.C.; Wijers, S.L.J.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. High Prevalence of Physical Frailty Among Community-Dwelling Malnourished Older Adults-A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.P.; McDonald, C.K.; Palmer, M.A.; Sinnott, M. Malnutrition associated with increased risk of frail mechanical falls among older people presenting to an emergency department. Emerg. Med. Australas. 2009, 21, 386–394. [Google Scholar] [CrossRef]
- Oliveira, M.R.M.; Fogaça, K.C.P.; Leandro-Merhi, V.A. Nutritional status and functional capacity of hospitalized elderly. Nutr. J. 2009, 8, 54. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 358) | Preintervention (n = 122) | Intervention (n = 236) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Demographic characteristics | |||||||
| Age (years) | 82 | (79–87) | 82 | (79–89) | 82 | (78–86) | 0.083 |
| Gender | 0.001 | ||||||
| Female | 204 | (57.0%) | 85 | (69.7%) | 119 | (50.4%) | |
| Male | 154 | (43.0%) | 37 | (30.3%) | 117 | (49.6%) | |
| BMI (kg/m2) | 24.1 | (21.4–26.6) | 24.20 | (21.8–27.3) | 23.91 | (21.3–26.2) | 0.284 |
| Educational level | 0.222 | ||||||
| Illiterate | 79 | (22.1%) | 20 | (16.4%) | 59 | (25.0%) | |
| Literate | 22 | (6.2%) | 8 | (6.6%) | 14 | (5.9%) | |
| Primary school | 146 | (40.8%) | 58 | (47.5%) | 88 | (37.3%) | |
| Junior high school | 31 | (8.7%) | 11 | (9.0%) | 20 | (8.5%) | |
| Senior high school | 42 | (11.7%) | 16 | (13.1%) | 26 | (11.0%) | |
| University | 38 | (10.6%) | 9 | (7.4%) | 29 | (12.3%) | |
| Geriatric assessment characteristics | |||||||
| Falls in the last month | 58 | (16.4%) | 24 | (20.5%) | 34 | (14.4%) | 0.192 |
| Falls in the last year | 111 | (31.4%) | 38 | (32.5%) | 73 | (30.9%) | 0.863 |
| Decision-making person—oneself a | 166 | (46.4%) | 60 | (49.2%) | 106 | (44.9%) | 0.512 |
| Caregiver—oneself b | 150 | (41.9%) | 48 | (39.3%) | 102 | (43.2%) | 0.554 |
| Charlson comorbidity index | 2 | (1–4) | 2 | (1–3) | 2 | (1–4) | 0.021 |
| Polypharmacy | 231 | (64.5%) | 78 | (63.9%) | 153 | (64.8%) | 0.959 |
| Mini-mental state examination | 22 | (18–26) | 21 | (16–25) | 23 | (19–27) | 0.014 |
| Barthel index before emergency department c | 90 | (68.8–100) | 90 | (55–100) | 90 | (70–100) | 0.536 |
| Lawton scale d | 5 | (2–7) | 5 | (2–7) | 5 | (2–7) | 0.393 |
| Mini Nutritional Assessment Short-Form | 11 | (9–12) | 9 | (7–11) | 11 | (9–13) | <0.001 |
| Frailty components | 3 | (3–4) | 3 | (3–4) | 3 | (2.3–4) | 0.075 |
| Exhaustion e | 159 | (44.4%) | 63 | (51.6%) | 96 | (40.7%) | 0.048 |
| Weight loss f | 48 | (13.4%) | 26 | (21.3%) | 22 | (9.3%) | 0.002 |
| Hand grip strength g | 291 | (81.3%) | 104 | (85.3%) | 187 | (79.2%) | 0.167 |
| Walking speed h | 309 | (86.3%) | 96 | (78.7%) | 213 | (90.3%) | 0.003 |
| Low energy expenditure i | 303 | (84.6%) | 107 | (87.7%) | 196 | (83.1%) | 0.247 |
| EQ-5D utility index j | 0.5 | (0.2–0.7) | 0.5 | (0.2–0.7) | 0.5 | (0.3–0.7) | 0.460 |
| EQ- visual analogue scale | 60 | (45–70) | 50 | (30–60) | 60 | (50–78.8) | <0.001 |
| Robust (n = 7) | Pre-Frail (n = 77) | Frail (n = 274) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Demographic characteristics | |||||||
| Age (years) | 77 | (77–83) | 80 | (78–84.5) | 83 | (79–88) | 0.001 |
| Gender | 0.148 | ||||||
| Female | 6 | (85.7%) | 48 | (62.3%) | 150 | (54.7%) | |
| Male | 1 | (14.3%) | 29 | (37.7%) | 124 | (45.3%) | |
| BMI (kg/m2) | 24.9 | (23.8–27.7) | 24.3 | (22.0–27.2) | 24.0 | (21.3–26.4) | 0.503 |
| Educational level | 0.003 | ||||||
| Illiterate | 0 | (0%) | 9 | (11.7%) | 70 | (25.6%) | |
| Literate | 0 | (0%) | 0 | (0%) | 22 | (8.0%) | |
| Primary school | 4 | (57.1%) | 35 | (45.5%) | 107 | (39.1%) | |
| Junior high school | 0 | (0%) | 12 | (15.6%) | 19 | (6.9%) | |
| Senior high school | 1 | (14.3%) | 8 | (10.4%) | 33 | (12.0%) | |
| University | 2 | (28.6%) | 13 | (16.9%) | 23 | (8.4%) | |
| Geriatric assessment characteristics | |||||||
| Falls in the last month | 1 | (14.3%) | 3 | (4.0%) | 54 | (20.0%) | 0.004 |
| Falls in the last year | 2 | (28.6%) | 9 | (11.8%) | 100 | (37.0%) | <0.001 |
| Decision-making person—oneself | 7 | (100%) | 49 | (63.6%) | 110 | (40.2%) | <0.001 |
| Caregiver—oneself | 5 | (71.4%) | 54 | (70.1%) | 91 | (33.2%) | <0.001 |
| Charlson comorbidity index | 0 | (0–2) | 2 | (1–3) | 2 | (1–4) | <0.001 |
| Polypharmacy | 2 | (28.6%) | 37 | (48.1%) | 192 | (70.1%) | <0.001 |
| Mini-mental state examination | 27.5 | (24.8–28.5) | 26 | (23–27) | 21 | (16–25) | <0.001 |
| Barthel index before emergency department | 100 | (100–100) | 100 | (95–100) | 80 | (53.8–95) | <0.001 |
| Lawton scale | 7 | (6–8) | 7 | (6–8) | 4 | (1–6) | <0.001 |
| Mini Nutritional Assessment Short-Form | 12 | (11–13) | 12 | (11–13.5) | 10 | (8–12) | <0.001 |
| EQ-5D utility index | 0.8 | (0.6–0.8) | 0.7 | (0.7–0.8) | 0.4 | (0.1–0.7) | <0.001 |
| EQ- visual analogue scale | 80 | (65–89.5) | 60 | (50–70) | 60 | (30–70) | 0.009 |
| Simple Model | Multiple Model (n = 318) | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | p Value | OR | (95%CI) | p Value | |||
| Demographic characteristics | ||||||||
| Age (years) | 1.04 | (0.99–1.08) | 0.100 | |||||
| Gender | ||||||||
| Female | ref. | ref. | ||||||
| Male | 0.58 | (0.37–0.92) | 0.019 | 0.80 | (0.46–1.40) | 0.433 | ||
| BMI (kg/m2) | 0.99 | (0.95–1.04) | 0.805 | |||||
| Educational level | ||||||||
| Illiterate | ref. | ref. | ||||||
| Literate | 1.27 | (0.43–3.73) | 0.662 | 1.01 | (0.28–3.61) | 0.992 | ||
| Primary school | 1.87 | (1.00–3.50) | 0.049 | 1.44 | (0.63–3.28) | 0.390 | ||
| Junior high school | 2.45 | (1.01–5.94) | 0.048 | 1.89 | (0.64–5.59) | 0.248 | ||
| Senior high school | 1.69 | (0.74–3.88) | 0.213 | 1.11 | (0.39–3.18) | 0.840 | ||
| University | 1.98 | (0.85–4.59) | 0.113 | 2.46 | (0.90–6.71) | 0.079 | ||
| Geriatric assessment characteristics | ||||||||
| Falls in the last month | 0.95 | (0.52–1.74) | 0.862 | |||||
| Falls in the last year | 0.76 | (0.46–1.24) | 0.266 | |||||
| Decision-making person—oneself | 0.69 | (0.44–1.08) | 0.102 | |||||
| Caregiver—oneself | 0.81 | (0.52–1.27) | 0.359 | |||||
| Charlson comorbidity index | 0.95 | (0.84–1.08) | 0.448 | |||||
| Polypharmacy | 0.83 | (0.52–1.30) | 0.411 | |||||
| Mini-mental state examination | 0.99 | (0.95–1.03) | 0.646 | |||||
| Barthel index before emergency department | 0.99 | (0.99–1.00) | 0.193 | |||||
| Lawton scale | 0.96 | (0.88–1.04) | 0.278 | |||||
| Mini Nutritional Assessment Short-Form | 0.86 | (0.79–0.94) | 0.001 | 1.03 | (0.91–1.18) | 0.604 | ||
| Frailty | 1.20 | (0.97–1.50) | 0.100 | |||||
| EQ-5D utility index | 0.72 | (0.39–1.32) | 0.287 | |||||
| EQ- visual analogue scale | 1.00 | (0.98–1.01) | 0.460 | |||||
| Caring program | ||||||||
| Preintervention | ref. | ref. | ||||||
| Intervention | 0.29 | (0.18–0.47) | <0.001 | 0.33 | (0.18–0.58) | <0.001 | ||
| Simple Model | Multiple Model | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | p Value | OR | (95%CI) | p Value | |||
| Demographic characteristics | ||||||||
| Age (years) | 0.99 | (0.95–1.04) | 0.786 | |||||
| Gender | ||||||||
| Female | ref. | |||||||
| Male | 0.84 | (0.53–1.32) | 0.443 | |||||
| BMI (kg/m2) | 1.00 | (0.95–1.05) | 0.881 | |||||
| Educational level | ||||||||
| Illiterate | ref. | |||||||
| Literate | 1.39 | (0.51–3.76) | 0.515 | |||||
| Primary school | 0.98 | (0.54–1.80) | 0.956 | |||||
| Junior high school | 1.54 | (0.64–3.67) | 0.333 | |||||
| Senior high school | 1.22 | (0.54–2.72) | 0.632 | |||||
| University | 0.99 | (0.42–2.33) | 0.985 | |||||
| Geriatric assessment characteristics | ||||||||
| Falls in the last month | 0.91 | (0.49–1.70) | 0.777 | |||||
| Falls in the last year | 1.33 | (0.82–2.15) | 0.242 | |||||
| Decision-making person—oneself | 0.58 | (0.37–0.93) | 0.022 | 0.64 | (0.33–1.25) | 0.190 | ||
| Caregiver—oneself | 0.57 | (0.36–0.92) | 0.020 | 0.93 | (0.48–1.79) | 0.831 | ||
| Charlson comorbidity index | 1.06 | (0.94–1.20) | 0.346 | |||||
| Polypharmacy | 1.19 | (0.74–1.92) | 0.470 | |||||
| Mini-mental state examination | 0.95 | (0.91–0.99) | 0.007 | 0.97 | (0.92–1.01) | 0.137 | ||
| Barthel index before emergency department | 0.99 | (0.99–1.00) | 0.215 | |||||
| Lawton scale | 0.97 | (0.89–1.05) | 0.473 | |||||
| Mini Nutritional Assessment Short-Form | 0.92 | (0.84–1.00) | 0.063 | |||||
| Frailty | 1.19 | (0.95–1.49) | 0.126 | |||||
| EQ-5D utility index | 0.80 | (0.43–1.49) | 0.483 | |||||
| EQ- visual analogue scale | 1.00 | (0.99–1.01) | 0.707 | |||||
| Caring program | ||||||||
| Preintervention | ref. | |||||||
| Intervention | 0.73 | (0.46–1.16) | 0.183 | |||||
| Simple Model | Multiple Model | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | p Value | OR | (95%CI) | p Value | |||
| Demographic characteristics | ||||||||
| Age (years) | 0.97 | (0.92–1.02) | 0.230 | |||||
| Gender | ||||||||
| Female | ref. | |||||||
| Male | 0.79 | (0.46–1.33) | 0.368 | |||||
| BMI (kg/m2) | 0.99 | (0.94–1.05) | 0.846 | |||||
| Educational level | ||||||||
| Illiterate | ref. | |||||||
| Literate | 1.25 | (0.40–3.94) | 0.697 | |||||
| Primary school | 1.25 | (0.63–2.47) | 0.528 | |||||
| Junior high school | 1.02 | (0.36–2.94) | 0.965 | |||||
| Senior high school | 0.71 | (0.25–1.99) | 0.517 | |||||
| University | 1.14 | (0.44–2.98) | 0.792 | |||||
| Geriatric assessment characteristics | ||||||||
| Falls in the last month | 0.58 | (0.26–1.28) | 0.176 | |||||
| Falls in the last year | 0.87 | (0.50–1.54) | 0.641 | |||||
| Decision-making person—oneself | 0.46 | (0.26–0.79) | 0.005 | 0.63 | (0.34–1.17) | 0.143 | ||
| Caregiver—oneself | 0.77 | (0.46–1.31) | 0.341 | |||||
| Charlson comorbidity index | 1.17 | (1.02–1.35) | 0.025 | 1.12 | (0.96–1.30) | 0.138 | ||
| Polypharmacy | 1.25 | (0.72–2.16) | 0.428 | |||||
| Mini-mental state examination | 0.93 | (0.89–0.98) | 0.00 * | 0.96 | (0.91–1.01) | 0.114 | ||
| Barthel index before emergency department | 1.00 | (0.99–1.01) | 0.463 | |||||
| Lawton scale | 0.97 | (0.89–1.07) | 0.569 | |||||
| Mini Nutritional Assessment Short-Form | 0.94 | (0.85–1.04) | 0.253 | |||||
| Frailty | 1.33 | (1.02–1.74) | 0.037 | 1.13 | (0.81–1.57) | 0.463 | ||
| EQ-5D utility index | 0.89 | (0.44–1.80) | 0.736 | |||||
| EQ- visual analogue scale | 1.00 | (0.98–1.01) | 0.788 | |||||
| Caring program | ||||||||
| Preintervention | ref. | |||||||
| Intervention | 0.79 | (0.46–1.35) | 0.388 | |||||
| Simple Model | Multiple Model | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | p Value | OR | (95%CI) | p Value | |||
| Demographic characteristics | ||||||||
| Age (years) | 0.99 | (0.91–1.08) | 0.883 | |||||
| Gender | ||||||||
| Female | ref. | |||||||
| Male | 1.09 | (0.44–2.70) | 0.854 | |||||
| BMI (kg/m2) | 1.00 | (0.91–1.10) | 0.979 | |||||
| Educational level | ||||||||
| Illiterate | ref. | |||||||
| Literate | 0.00 | (0.00– | 0.998 | |||||
| Primary school | 0.68 | (0.24–1.89) | 0.455 | |||||
| Junior high school | 0.71 | (0.14–3.62) | 0.680 | |||||
| Senior high school | 0.25 | (0.03–2.11) | 0.203 | |||||
| University | 0.28 | (0.03–2.35) | 0.239 | |||||
| Geriatric assessment characteristics | ||||||||
| Falls in the last month | 1.76 | (0.61–5.05) | 0.293 | |||||
| Falls in the last year | 1.19 | (0.46–3.06) | 0.725 | |||||
| Decision-making person—oneself | 0.27 | (0.09–0.83) | 0.022 | 0.28 | (0.07–1.12) | 0.072 | ||
| Caregiver—oneself | 0.58 | (0.22–1.54) | 0.272 | |||||
| Charlson comorbidity index | 1.10 | (0.87–1.40) | 0.413 | |||||
| Polypharmacy | 1.69 | (0.60–4.78) | 0.319 | |||||
| Mini-mental state examination | 0.93 | (0.86–1.00) | 0.065 | |||||
| Barthel index before emergency department | 0.99 | (0.98–1.01) | 0.205 | |||||
| Lawton scale | 0.93 | (0.79–1.09) | 0.355 | |||||
| Mini Nutritional Assessment Short-Form | 0.79 | (0.67–0.93) | 0.005 | 0.96 | (0.71–1.30) | 0.781 | ||
| Frailty | 2.09 | (1.21–3.60) | 0.008 | 2.48 | (1.07–5.74) | 0.033 | ||
| EQ-5D utility index | 0.54 | (0.16–1.86) | 0.329 | |||||
| EQ- visual analogue scale | 0.97 | (0.95–0.99) | 0.007 | 0.99 | (0.96–1.01) | 0.260 | ||
| Caring program | ||||||||
| Preintervention | ref. | ref. | ||||||
| Intervention | 0.26 | (0.10–0.66) | 0.005 | 0.21 | (0.05–0.95) | 0.043 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-F.; Lin, P.-C.; Hu, S.-Y.; Tsan, Y.-T.; Liao, W.-K.; Lin, S.-Y.; Lin, T.-C. Comprehensive Geriatric Assessment and Clinical Outcomes in the Older People at the Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 6164. https://doi.org/10.3390/ijerph18116164
Lin C-F, Lin P-C, Hu S-Y, Tsan Y-T, Liao W-K, Lin S-Y, Lin T-C. Comprehensive Geriatric Assessment and Clinical Outcomes in the Older People at the Emergency Department. International Journal of Environmental Research and Public Health. 2021; 18(11):6164. https://doi.org/10.3390/ijerph18116164
Chicago/Turabian StyleLin, Cheng-Fu, Po-Chen Lin, Sung-Yuan Hu, Yu-Tse Tsan, Wei-Kai Liao, Shih-Yi Lin, and Tzu-Chieh Lin. 2021. "Comprehensive Geriatric Assessment and Clinical Outcomes in the Older People at the Emergency Department" International Journal of Environmental Research and Public Health 18, no. 11: 6164. https://doi.org/10.3390/ijerph18116164
APA StyleLin, C.-F., Lin, P.-C., Hu, S.-Y., Tsan, Y.-T., Liao, W.-K., Lin, S.-Y., & Lin, T.-C. (2021). Comprehensive Geriatric Assessment and Clinical Outcomes in the Older People at the Emergency Department. International Journal of Environmental Research and Public Health, 18(11), 6164. https://doi.org/10.3390/ijerph18116164