
Home Environment and Early Development of Rural Children: Evidence from Guizhou Province in China



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Child Development
2.3.2. Home Environment
2.3.3. Analytical Plan
3. Results
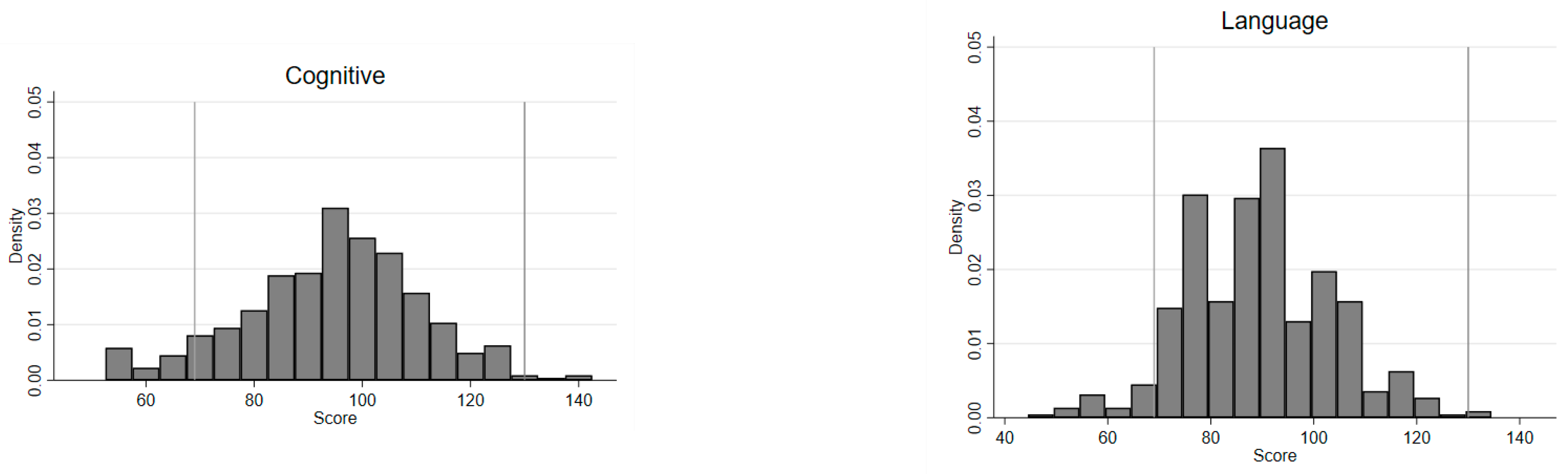
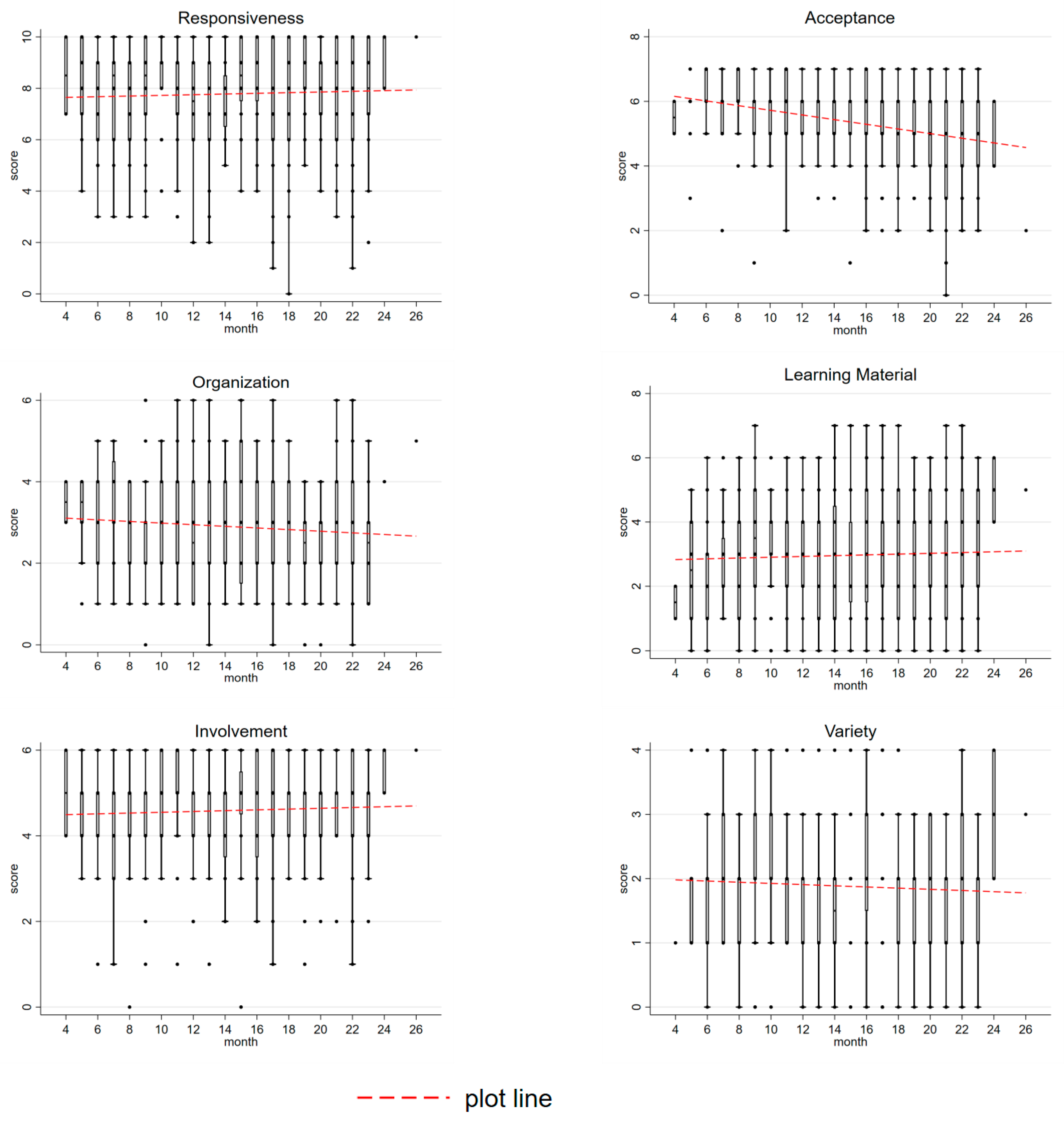
3.1. Descriptive Statistics
3.2. Regression Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | NICHD | This Study | |
|---|---|---|---|
| Responsiveness | 1. Caregiver spontaneously vocalizes to child at least twice | 97.9 | 77.0 |
| 2. Caregiver responds verbally to child’s vocalizations or verbalizations | 89.2 | 68.0 | |
| 3. Caregiver tells child name of object or person during visit | 80.2 | 49.6 | |
| 4. Caregiver’s speech is distinct, clear, and audible | 97.2 | 82.2 | |
| 5. Caregiver initiates verbal interchanges with visitor | 95.4 | 79.5 | |
| 6. Caregiver converses freely and easily | 98.5 | 88.5 | |
| 7. Caregiver permits child to engage in messy play | 83.2 | - | |
| 8. Caregiver spontaneously praises child at least twice | 64.7 | 60.1 | |
| 9. Caregiver’s voice conveys positive feelings toward child | 95.3 | 92.3 | |
| 10. Caregiver caresses or kisses child at least once | 80.7 | 93.9 | |
| 11. Caregiver responds positively to praise of child offered by visitor | 94.8 | 87.4 | |
| Average | 88.8 | 77.9 | |
| Acceptance | 12. Caregiver does not shout at child | 93.0 | 89.4 |
| 13. Caregiver does not express overt annoyance with or hostility to child | 90.7 | 98.0 | |
| 14. Caregiver neither slaps or spanks child during visit | 97.4 | 93.7 | |
| 15. No more than one instance of physical punishment during past week | 81.4 | 68.0 | |
| 16. Caregiver does not scold or criticize child during visit | 87.4 | 86.9 | |
| 17. Caregiver does not interfere with or restrict child three times during visit | 55.9 | 62.4 | |
| 18. At least 10 books are present and visible | 53.9 | 40.8 | |
| Average | 80.0 | 77.0 | |
| Organization | 19. Caregiver is one of no more than three regular substitutes used for child | 93.0 | 67.3 |
| 20. Child is taken on an outing at least once a week | 57.7 | 53.4 | |
| 21. Child gets out of house at least four times a week | 84.8 | 56.8 | |
| 22. Caregiver has an emergency medical and/or accident plan | 69.6 | - | |
| 23. Child has a special place for toys and treasures | 81.7 | 39.9 | |
| 24. Child’s play environment is safe | 41.0 | 71.5 | |
| Average | 71.3 | 57.8 | |
| Learning Materials | 25. Muscle activity toys or equipment | 87.8 | 39.4 |
| 26. Push or pull toy | 80.1 | 34.2 | |
| 27. Stroller or walker, kiddie car, scooter, or tricycle | 87.4 | 74.8 | |
| 28. Caregiver provides toys for child to play with during the visit | 97.7 | 37.8 | |
| 29. Cuddly toy or role-playing toys | 96.9 | 44.4 | |
| 30. Learning facilitators—mobile, table and chair, high chair, playpen | 75.8 | - | |
| 31. Simple eye–hand coordination toys | 93.3 | 48.4 | |
| 32. Complex eye–hand coordination toys | 62.9 | 16.9 | |
| 33. Toys for literature and music | 71.7 | - | |
| Average | 83.7 | 42.3 | |
| Involvement | 34. Caregiver keeps child in visual range, looks at often | 81.4 | 91.2 |
| 35. Caregiver talks to child while doing household work | 60.3 | 89.2 | |
| 36. Caregiver consciously encourages developmental advance | 81.2 | 89.9 | |
| 37. Caregiver invests maturing toys with value via personal attention | 65.2 | 79.1 | |
| 38. Caregiver structures child’s play periods | 68.6 | 81.8 | |
| 39. Caregiver provides toys that challenge child to develop new skills | 65.2 | 28.2 | |
| Average | 70.3 | 76.6 | |
| Variety | 40. Caregiver reads stories to child at least three times weekly | 74.5 | 16.2 |
| 41. Child eats at least one meal with caregiver and/or other children | 93.0 | 77.7 | |
| 42. Caregiver and child visit or receive from neighbors or friends about once a month | 75.5 | 77.0 | |
| 43. Child has three or more books of his/her own | 84.5 | 17.3 | |
| Average | 81.9 | 47.1 |
References
- WHO. Early Child Development. Available online: https://www.who.int/topics/early-child-development/en/ (accessed on 22 February 2021).
- Zhang, L.; Yi, H.; Luo, R.; Liu, C.; Rozelle, S. The human capital roots of the middle income trap: The case of China. Agric. Econ. 2013, 44, 151–162. [Google Scholar] [CrossRef]
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef]
- Wang, L.; Liang, W.; Zhang, S.; Jonsson, L.; Li, M.; Yu, C.; Sun, Y.; Ma, Q.; Bai, Y.; Abbey, C.; et al. Are infant/toddler developmental delays a problem across rural China? J. Comp. Econ. 2019, 47, 458–469. [Google Scholar] [CrossRef]
- Duncan, G.J.; Magnuson, K.; Votruba-Drzal, E. Boosting Family Income to Promote Child Development. Future Child. 2014, 24, 99–120. [Google Scholar] [CrossRef]
- Lugo-Gil, J.; Tamis-Lemonda, C.S. Family Resources and Parenting Quality: Links to Childrens Cognitive Development across the First 3 Years. Child Dev. 2008, 79, 1065–1085. [Google Scholar] [CrossRef]
- Anderson, J.W.; Johnstone, B.M.; Remley, D.T. Breast-feeding and cognitive development: A meta-analysis. Am. J. Clin. Nutr. 1999, 70, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.C.; Adair, L.S. Breast-feeding influences cognitive development in Filipino children. J. Nutr. 2005, 135, 2589–2595. [Google Scholar] [CrossRef]
- Fergusson, D.; Beautrais, A.; Silva, P. Breast-feeding and cognitive development in the first seven years of life. Soc. Sci. Med. 1982, 16, 1705–1708. [Google Scholar] [CrossRef]
- Martorell, R. The nature of child malnutrition and its long-term implications. Food Nutr. Bull. 1999, 20, 288–292. [Google Scholar] [CrossRef]
- Oddy, W.H.; Kendall, G.E.; Blair, E.; De Klerk, N.H.; Stanley, F.J.; Landau, L.I.; Silburn, S.; Zubrick, S. Breast feeding and cognitive development in childhood: A prospective birth cohort study. Paediatr. Perinat. Epidemiol. 2003, 17, 81–90. [Google Scholar] [CrossRef]
- UNICEF. Home Environment. Available online: https://data.unicef.org/topic/early-childhood-development/home-environment/ (accessed on 22 February 2021).
- Irwin, L.G.; Siddiqi, A.; HErtzman, C. Early Child Development: A Powerful Equalizer; Human Early Learning Partnership: Vancouver, BC, Canada, 2007. [Google Scholar]
- Francesconi, M.; Heckman, J.J. Symposium on Child Development and Parental Investment: Introduction. Econ. J. 2016, 126, F1–F27. [Google Scholar] [CrossRef]
- Heckman, J.J. Skill formation and the economics of investing in disadvantaged children. Science 2006, 312, 1900–1902. [Google Scholar] [CrossRef] [PubMed]
- Heckman, J.J. The economics of inequality: The value of early childhood education. Am. Educ. 2011, 35, 31. [Google Scholar]
- Heckman, J.; Pinto, R.; Savelyev, P. Understanding the mechanisms through which an influential early childhood program boosted adult outcomes. Am. Econ. Rev. 2013, 103, 2052–2086. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.S.; Knight, J. Influence of the Home Environment on the Development of Obesity in Children. Pediatrics 1999, 103, e85. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.H.; Caldwell, B.M.; Rock, S.L.; Ramey, C.T.; Barnard, K.E.; Gray, C.; Hammond, M.A.; Mitchell, S.; Gottfried, A.W.; Siegel, L. Home environment and cognitive development in the first 3 years of life: A collaborative study involving six sites and three ethnic groups in North America. Dev. Psychol. 1989, 25, 217–235. [Google Scholar] [CrossRef]
- Payne, A.C.; Whitehurst, G.J.; Angell, A.L. The role of home literacy environment in the development of language ability in preschool children from low-income families. Early Child. Res. Q. 1994, 9, 427–440. [Google Scholar] [CrossRef]
- Grantham-Mcgregor, S.; Yin, B.C.; Cueto, S.; Glewwe, P.P.; Strupp, B. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Gustafson, S.L.; Rhodes, R.E. Parental correlates of physical activity in children and early adolescents. Sports Med. 2006, 36, 79–97. [Google Scholar] [CrossRef]
- Pugliese, J.; Tinsley, B. Parental socialization of child and adolescent physical activity: A meta-analysis. J. Fam. Psychol. 2007, 21, 331. [Google Scholar] [CrossRef]
- Engle, P.L.; Black, M.M.; Behrman, J.R.; De Mello, M.C.; Gertler, P.J.; Kapiriri, L.; Martorell, R.; Young, M.E.; Group, I.C.D.S. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 369, 229–242. [Google Scholar] [CrossRef]
- Gottfried, A.W.; Schlackman, J.; Gottfried, A.E.; Boutin-Martinez, A.S. Parental Provision of Early Literacy Environment as Related to Reading and Educational Outcomes Across the Academic Lifespan. Parenting 2015, 15, 24–38. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Tamis-LeMonda, C.S. Maternal responsiveness and cognitive development in children. New Dir. Child Dev. 1989, 1989, 49–61. [Google Scholar] [CrossRef] [PubMed]
- McLoyd, V.C. Socioeconomic disadvantage and child development. Am. Psychol. 1998, 53, 185. [Google Scholar] [CrossRef]
- Lu, H.J.; Chang, L. Parenting and Socialization of Only Children in Urban China: An Example of Authoritative Parenting. J. Genet. Psychol. 2013, 174, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Li, H. ‘Tiger mom, panda dad’: A study of contemporary Chinese parenting profiles. Early Child Dev. Care 2019, 189, 284–300. [Google Scholar] [CrossRef]
- Chang, L.; Chen, B.-B.; Ji, L.Q. Attributions and Attitudes of Mothers and Fathers in China. Parenting 2011, 11, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Farver, J.A.; Zhang, Z.; Zeng, Q.; Yu, L.; Cai, B. Mainland Chinese parenting styles and parent-child interaction. Int. J. Behav. Dev. 2005, 29, 524–531. [Google Scholar] [CrossRef]
- Liu, S.; Liu, Y.; Wang, S.; Liu, H. The Impact of Parental Educational Mode on the Problem Behavior of Migrant Children. J. Xian Jiaotong Univ. 2015, 35, 87–93. [Google Scholar] [CrossRef]
- Nyland, B.; Nyland, C.; Maharaj, E.A. Early childhood education and care in urban China: The importance of parental choice. Early Child Dev. Care 2009, 179, 517–528. [Google Scholar] [CrossRef]
- Yue, A.; Shi, Y.; Luo, R.; Chen, J.; Rozelle, S. China’s Invisible Crisis: Cognitive Delays among Rural Toddlers and the Absence of Modern Parenting. China J. 2017, 78, 50–80. [Google Scholar] [CrossRef]
- Luo, R.; Jia, F.; Yue, A.; Zhang, L.; Lyu, Q.; Shi, Y.; Yang, M.; Medina, A.; Kotb, S.; Rozelle, S. Passive parenting and its association with early child development. Early Child Dev. Care 2019, 189, 1709–1723. [Google Scholar] [CrossRef]
- Wang, B.; Luo, X.; Yue, A.; Tang, L.; Shi, Y. Family Environment In Rural China And The Link With Early Childhood Development. Early Child Dev. Care 2020, 1–14. [Google Scholar] [CrossRef]
- Albers, C.A.; Grieve, A.J. Test review: Bayley, N. Bayley scales of infant and toddler development–third edition. San Antonio, TX: Harcourt assessment. J. Psychoeduc. Assess. 2007, 25, 180–190. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development: Bayley-III; The Psychological Corporation: San Antonio, TX, USA, 2006. [Google Scholar]
- Bos, A.F. Bayley-II or Bayley-III: What do the scores tell us? Dev. Med. Child Neurol. 2013, 55, 978–979. [Google Scholar] [CrossRef]
- Attanasio, O.; Cattan, S.; Fitzsimons, E.; Meghir, C.; Rubio-Codina, M. Estimating the Production Function for Human Capital: Results from a Randomized Control Trial in Colombia. Am. Econ. Rev. 2020, 110, 48–85. [Google Scholar] [CrossRef]
- Sylvia, S.; Warrinnier, N.; Luo, R.; Yue, A.; Attanasio, O.; Medina, A.; Rozelle, S. From Quantity to Quality: Delivering a Home-based Parenting Intervention through China’s Family Planning Cadres. Econ. J. 2018, 131, 1365–1400. [Google Scholar] [CrossRef]
- Bradley, R.H.; Caldwell, B.M.; Corwyn, R.F. The Child Care HOME Inventories: Assessing the quality of family child care homes. Early Child. Res. Q. 2003, 18, 294–309. [Google Scholar] [CrossRef]
- Bradley, R.H.; Corwyn, R.F. Caring for children around the world: A view from HOME. Int. J. Behav. Dev. 2005, 29, 468–478. [Google Scholar] [CrossRef]
- Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Taylor & Francis Group: Mahwah, UK, 2002. [Google Scholar]
- Hoff, E. The Specificity of Environmental Influence: Socioeconomic Status Affects Early Vocabulary Development Via Maternal Speech. Child Dev. 2003, 74, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-M.; Mahoney, G. The Effects of Mother’s Style of Interaction on Children’s Engagement:Implications for Using Responsive Interventions with Parents. Top. Early Child. Spec. Educ. 2004, 24, 31–38. [Google Scholar] [CrossRef]
- Petrocelli, J.V. Hierarchical Multiple Regression in Counseling Research: Common Problems and Possible Remedies. Meas. Eval. Couns. Dev. 2003, 36, 9–22. [Google Scholar] [CrossRef]
- Schady, N. Parents’ Education, Mothers’ Vocabulary, and Cognitive Development in Early Childhood: Longitudinal Evidence From Ecuador. Am. J. Public Health 2011, 101, 2299–2307. [Google Scholar] [CrossRef]
- Russell, A.; Aloa, V.; Feder, T.; Glover, A.; Miller, H.; Palmer, G. Sex-Based Differences in Parenting Styles in a Sample with Preschool Children. Aust. J. Psychol. 1998, 50, 89–99. [Google Scholar] [CrossRef]
- Brody, G.H. Siblings’ Direct and Indirect Contributions to Child Development. Curr. Dir. Psychol. Sci. 2004, 13, 124–126. [Google Scholar] [CrossRef]
- Statistics Bureau of Guizhou Province. Guizhou 1% Population Sample Survey 2015; China Statistical Press: Guizhou, China, 2017. [Google Scholar]
- Eshel, N.; Daelmans, B.; De Mello, M.; Martines, J. Responsive parenting: Interventions and outcomes. Bull. World Health Organ. 2006, 84, 991–998. [Google Scholar] [PubMed]
- Bradley, R.H. Constructing and Adapting Causal and Formative Measures of Family Settings: The HOME Inventory as Illustration. J. Fam. Theory Rev. 2015, 7, 381–414. [Google Scholar] [CrossRef] [PubMed]
- Nievar, M.A.; Moske, A.K.; Johnson, D.J.; Chen, Q. Parenting Practices in Preschool Leading to Later Cognitive Competence: A Family Stress Model. Early Educ. Dev. 2014, 25, 318–337. [Google Scholar] [CrossRef]
- Anders, Y.; Rossbach, H.-G.; Weinert, S.; Ebert, S.; Kuger, S.; Lehrl, S.; von Maurice, J. Home and preschool learning environments and their relations to the development of early numeracy skills. Early Child. Res. Q. 2012, 27, 231–244. [Google Scholar] [CrossRef]
- Dearing, E.; Casey, B.M.; Ganley, C.M.; Tillinger, M.; Laski, E.; Montecillo, C. Young girls’ arithmetic and spatial skills: The distal and proximal roles of family socioeconomics and home learning experiences. Early Child. Res. Q. 2012, 27, 458–470. [Google Scholar] [CrossRef]
- Bornstein, M.H. Cultural Approaches to Parenting. Parenting 2012, 12, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Richman, A.L.; Miller, P.M.; LeVine, R.A. Cultural and educational variations in maternal responsiveness. Dev. Psychol. 1992, 28, 614. [Google Scholar] [CrossRef]
- Chang, H.; Dong, X.-y.; MacPhail, F. Labor Migration and Time Use Patterns of the Left-behind Children and Elderly in Rural China. World Dev. 2011, 39, 2199–2210. [Google Scholar] [CrossRef]
- Chen, F.; Liu, G. The Health Implications of Grandparents Caring for Grandchildren in China. J. Gerontol. Ser. B 2011, 67B, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.; Zuo, D. Grandparents caring for grandchildren in rural China: Consequences for emotional and cognitive health in later life. Aging Ment Health 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]




| Variable | Unit | Mean | SD | SE (mean) | Min | Max | N |
|---|---|---|---|---|---|---|---|
| Age | months | 14.620 | 5.478 | 0.260 | 4 | 26 | 445 |
| Gender | 1 = male, 2 = female | 1.425 | 0.495 | 0.023 | 1 | 2 | 445 |
| Ethnic minority | 0 = no, 1 = yes | 0.225 | 0.418 | 0.020 | 0 | 1 | 445 |
| Low-income group | 0 = no, 1 = yes | 0.193 | 0.395 | 0.019 | 0 | 1 | 445 |
| Parent’s education | years | 7.787 | 3.373 | 0.160 | 0 | 19 | 445 |
| Siblings | number | 1.328 | 1.166 | 0.055 | 0 | 7 | 445 |
| Birthweight | grams | 3226.169 | 670.224 | 31.807 | 1500 | 6500 | 444 |
| Breastfeeding | 0 = no, 1 = yes | 0.791 | 0.407 | 0.019 | 0 | 1 | 444 |
| Nutrition supplements | 0 = no, 1 = yes | 0.440 | 0.497 | 0.024 | 0 | 1 | 445 |
| Parent smoking | 0 = no, 1 = yes | 0.607 | 0.489 | 0.023 | 0 | 1 | 445 |
| Score Type | Scale | Mean | SD | Min | Max |
|---|---|---|---|---|---|
| BSID-III composite scores | Cognitive | 94.45 | 16.32 | 55 | 140 |
| Language | 89.68 | 13.83 | 47 | 132 | |
| Motoric | 95.35 | 15.78 | 46 | 145 | |
| Social–emotional | 85.35 | 11.91 | 55 | 130 | |
| BSID-III raw scores | Cognitive | 43.56 | 11.17 | 7 | 71 |
| Receptive communication | 15.24 | 4.91 | 4 | 29 | |
| Expressive communication | 16.01 | 6.87 | 2 | 33 | |
| Fine motor | 30.49 | 6.48 | 8 | 45 | |
| Gross motor | 42.19 | 12.63 | 12 | 72 | |
| Social–emotional | 73.20 | 17.01 | 8 | 133 |
| Scale | Male | Female | t-Statistics | p-Value |
|---|---|---|---|---|
| Cognitive | 44.82 | 41.85 | −2.79 | 0.006 |
| Receptive communication | 15.45 | 14.96 | −1.04 | 0.298 |
| Expressive communication | 16.36 | 15.53 | −1.27 | 0.206 |
| Fine motor | 31.08 | 29.68 | −2.26 | 0.024 |
| Gross motor | 43.38 | 40.59 | −2.31 | 0.021 |
| Social–emotional | 74.32 | 71.68 | −1.62 | 0.105 |
| Sub-Score | Mean | SD | Min | Max |
|---|---|---|---|---|
| Responsiveness | 7.79 | 2.09 | 0 | 10 |
| Acceptance | 5.39 | 1.31 | 0 | 7 |
| Organization | 2.89 | 1.41 | 0 | 5 |
| Learning material | 2.96 | 1.88 | 0 | 7 |
| Involvement | 4.59 | 1.21 | 0 | 6 |
| Variety | 1.88 | 0.96 | 0 | 4 |
| Total score | 25.50 | 5.37 | 10 | 39 |
| Sub-Score | Gender | Ethnicity | ||||
|---|---|---|---|---|---|---|
| Male | Female | p-Value | Han | Non-Han | p-Value | |
| Responsiveness | 7.74 | 7.85 | 0.57 | 7.89 | 7.55 | 0.12 |
| Acceptance | 5.38 | 5.40 | 0.89 | 5.29 | 5.62 | 0.01 |
| Organization | 2.83 | 2.98 | 0.26 | 2.89 | 2.89 | 0.99 |
| Learning material | 3.12 | 2.74 | 0.03 | 2.97 | 2.94 | 0.89 |
| Involvement | 4.56 | 4.63 | 0.58 | 4.63 | 4.52 | 0.39 |
| Variety | 1.89 | 1.88 | 0.93 | 1.88 | 1.88 | 1.00 |
| Dependent Variables | Cognitive | Language | Motor | Social–Emotional | |||
|---|---|---|---|---|---|---|---|
| Explanatory Variables | Receptive Communication | Expressive Communication | Fine Motor | Gross Motor | |||
| Step 0: Village-Level Fixed Effects | |||||||
| Step 1: Socioeconomic Variables | |||||||
| Low-income | −2.627 *** | −0.962 ** | −0.824 | −0.725 | −1.279 * | −0.174 | |
| (0.787) | (0.364) | (0.527) | (0.461) | (0.649) | (1.721) | ||
| Ethnic minority | −0.313 | 0.357 | 0.894* | −0.511 | −0.360 | 0.603 | |
| (0.892) | (0.441) | (0.521) | (0.427) | (0.741) | (1.373) | ||
| Parent’s education | 0.301 * | 0.120 *** | 0.142 ** | 0.105 | 0.230 ** | 0.298 | |
| (0.153) | (0.062) | (0.070) | (0.075) | (0.098) | (0.230) | ||
| Age | 1.671 *** | 0.702 *** | 1.050 *** | 1.001 *** | 2.111 *** | 2.414 *** | |
| (0.052) | (0.034) | (0.048) | (0.033) | (0.054) | (0.092) | ||
| Male | 1.079 | −0.251 | −0.263 | 0.262 | 0.500 | −0.234 | |
| (0.732) | (0.317) | (0.415) | (0.383) | (0.602) | (1.198) | ||
| Siblings | −0.630 ** | −0.190 | −0.557 *** | 0.078 | −0.263 | −0.582 | |
| (0.262) | (0.151) | (0.158) | (0.167) | (0.249) | (0.591) | ||
| Constant | 15.370 *** | 4.970 | 0.835 | 15.200 | 10.577 | 39.387 | |
| (1.822) | (0.826) | (0.861) | (15.200) | (1.364) | (2.724) | ||
| R2 | 0.685 | 0.595 | 0.696 | 0.731 | 0.835 | 0.596 | |
| ΔR2 | 0.648 | 0.571 | 0.655 | 0.678 | 0.790 | 0.563 | |
| Step 2: Nutrition and health variables | |||||||
| Nutrition supplements | 0.439 | 0.309 | 0.336 | 0.041 | 0.864 * | 1.172 | |
| 0.598 | (0.289) | (0.346) | (0.383) | (0.497) | (1.053) | ||
| Birthweight | 2.963 * | 0.971 | 1.294 | 1.996 * | 0.009 | 4.641 | |
| 1.473 | (0.613) | (1.054) | (0.654) | (1.166) | (2.799) | ||
| Breastfeeding | 0.597 | 0.651 | 0.273 | 0.663 | 1.126 * | 0.429 | |
| 0.788 | (0.408) | (0.388) | (0.498) | (0.620) | (1.411) | ||
| Smoke | −0.685 | −0.586* | −0.437 | −0.606 * | −0.343 | −1.183 | |
| 0.674 | (0.323) | (0.422) | (0.359) | (0.496) | (1.008) | ||
| Constant | −7.893 | −2.849 | −9.429 | −0.744 | 9.807 | 2.617 | |
| 11.741 | (4.966) | (8.479) | (5.412) | (9.588) | (2.617) | ||
| R2 | 0.703 | 0.610 | 0.706 | 0.739 | 0.838 | 0.605 | |
| ΔR2 | 0.018 | 0.015 | 0.010 | 0.008 | 0.002 | 0.010 | |
| Step 3: Home environment | |||||||
| HOME | 0.060 | 0.102 *** | 0.172 *** | 0.050 | 0.113 ** | 0.227 *** | |
| (0.058) | (0.034) | (0.038) | (0.039) | (0.043) | (0.079) | ||
| R2 | 0.703 | 0.620 | 0.720 | 0.741 | 0.839 | 0.609 | |
| ΔR2 | 0.001 | 0.010 | 0.014 | 0.001 | 0.002 | 0.004 | |
| Constant | −5.207 | −2.704 | −9.186 | −0.674 | 9.962 | 2.937 | |
| 12.037 | 4.953 | 8.315 | 5.369 | 9.396 | 22.275 | ||
| F-test | 170.52 | 70.29 | 83.78 | 186.27 | 171.56 | 102.55 | |
| Number of observations | 444 | 444 | 444 | 444 | 443 | 444 | |
| Dependent Variables | Cognitive | Receptive Communication | Expressive Communication | Fine Motor | Gross Motor | Social–Emotional | |
|---|---|---|---|---|---|---|---|
| Explanatory Variables | |||||||
| Step 0: Village-level fixed effects | |||||||
| Step 1: Socioeconomic variables | |||||||
| Low-income | −2.627 *** | −0.962 ** | −0.824 | −0.725 | −1.279 * | −0.174 | |
| (0.787) | (0.364) | (0.527) | (0.461) | (0.649) | (1.721) | ||
| Ethnic minority | −0.313 | 0.357 | 0.894 * | −0.511 | −0.360 | 0.603 | |
| (0.892) | (0.441) | (0.521) | (0.427) | (0.741) | (1.373) | ||
| Parent’s education | 0.301 * | 0.120 *** | 0.142 ** | 0.105 | 0.230** | 0.298 | |
| (0.153) | (0.062) | (0.070) | (0.075) | (0.098) | (0.230) | ||
| Age | 1.671 *** | 0.702 *** | 1.050 *** | 1.001 *** | 2.111 *** | 2.414 *** | |
| (0.052) | (0.034) | (0.048) | (0.033) | (0.054) | (0.092) | ||
| Male | 1.079 | −0.251 | −0.263 | 0.262 | 0.500 | −0.234 | |
| (0.732) | (0.317) | (0.415) | (0.383) | (0.602) | (1.198) | ||
| Siblings | −0.630 ** | −0.190 | −0.557 *** | 0.078 | −0.263 | −0.582 | |
| (0.262) | (0.151) | (0.158) | (0.167) | (0.249) | (0.591) | ||
| Constant | 15.370 *** | 4.970 | 0.835 | 15.200 | 10.577 | 39.387 | |
| (1.822) | (0.826) | (0.861) | (15.200) | (1.364) | (2.724) | ||
| R2 | 0.685 | 0.595 | 0.696 | 0.731 | 0.835 | 0.596 | |
| ΔR2 | 0.648 | 0.571 | 0.655 | 0.678 | 0.790 | 0.563 | |
| Step 2: Nutrition and health variables | |||||||
| Nutrition supplements | 0.439 | 0.309 | 0.336 | 0.041 | 0.864 * | 1.172 | |
| 0.598 | (0.289) | (0.346) | (0.383) | (0.497) | (1.053) | ||
| Birthweight | 2.963 * | 0.971 | 1.294 | 1.996 * | 0.009 | 4.641 | |
| 1.473 | (0.613) | (1.054) | (0.654) | (1.166) | (2.799) | ||
| Breastfeeding | 0.597 | 0.651 | 0.273 | 0.663 | 1.126 * | 0.429 | |
| 0.788 | (0.408) | (0.388) | (0.498) | (0.620) | (1.411) | ||
| Smoke | −0.685 | −0.586 * | −0.437 | −0.606 * | −0.343 | −1.183 | |
| 0.674 | (0.323) | (0.422) | (0.359) | (0.496) | (1.008) | ||
| Constant | −7.893 | −2.849 | −9.429 | −0.744 | 9.807 | 2.617 | |
| 11.741 | (4.966) | (8.479) | (5.412) | (9.588) | (2.617) | ||
| R2 | 0.703 | 0.610 | 0.706 | 0.739 | 0.838 | 0.605 | |
| ΔR2 | 0.018 | 0.015 | 0.010 | 0.008 | 0.002 | 0.010 | |
| Step 3: Home environment | |||||||
| Responsiveness | −0.226 | 0.137 * | 0.242 *** | 0.032 | 0.073 | 0.301 | |
| (0.144) | (0.076) | (0.081) | (0.093) | (0.126) | (0.211) | ||
| Acceptance | 0.138 | −0.006 | −0.115 | 0.003 | −0.052 | 0.337 | |
| (0.246) | (0.109) | (0.194) | (0.109) | (0.176) | (0.452) | ||
| Organization | 0.128 | 0.224 | 0.279 * | 0.064 | 0.427 * | −0.058 | |
| (0.309) | (0.147) | (0.161) | (0.155) | (0.216) | (0.438) | ||
| Learning Material | 0.525 *** | 0.201 * | 0.259 ** | 0. 272 ** | 0.399 ** | 0.252 | |
| (0.190) | (0.118) | (0.123) | (0.107) | (0.189) | (0.321) | ||
| Involvement | −0.231 | −0.155 | −0.018 | −0.178 | −0.284 | 0.486 | |
| (0.218) | (0.148) | (0.218) | (0.175) | (0.253) | (0.518) | ||
| Variety | 0.019 | 0.063 | 0.129 | −0.052 | −0.241 | −0.052 | |
| (0.389) | (0.181) | (0.231) | (0.201) | (0.389) | (0.627) | ||
| Constant | −2.144 | −1.862 | −8.280 | 0.671 | 11.934 | 2.132 | |
| (12.676) | (4.957) | (8.538) | (5.529) | (9.419) | (22.901) | ||
| F-test | 223.325 | 73.204 | 100.777 | 188.628 | 209.902 | 144.680 | |
| Number of observations | 444 | 444 | 444 | 444 | 443 | 444 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuhn, L.; Liu, C.; Wang, T.; Luo, R. Home Environment and Early Development of Rural Children: Evidence from Guizhou Province in China. Int. J. Environ. Res. Public Health 2021, 18, 6121. https://doi.org/10.3390/ijerph18116121
Kuhn L, Liu C, Wang T, Luo R. Home Environment and Early Development of Rural Children: Evidence from Guizhou Province in China. International Journal of Environmental Research and Public Health. 2021; 18(11):6121. https://doi.org/10.3390/ijerph18116121
Chicago/Turabian StyleKuhn, Lena, Chengfang Liu, Tianyi Wang, and Renfu Luo. 2021. "Home Environment and Early Development of Rural Children: Evidence from Guizhou Province in China" International Journal of Environmental Research and Public Health 18, no. 11: 6121. https://doi.org/10.3390/ijerph18116121
APA StyleKuhn, L., Liu, C., Wang, T., & Luo, R. (2021). Home Environment and Early Development of Rural Children: Evidence from Guizhou Province in China. International Journal of Environmental Research and Public Health, 18(11), 6121. https://doi.org/10.3390/ijerph18116121