
Characterizing Breakthrough Cancer Pain Using Ecological Momentary Assessment with a Smartphone App: Feasibility and Clinical Findings

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Procedures and Sample
2.2. Measures
2.2.1. Daily Assessment with the App
- -
- Treatment adherence: Daily treatment intake was measured with a single item, “Have you taken the pain medication prescribed by your doctor today?”. Response options are: (a) “Yes, I have taken it”, (b) “No, but I will take it”, and (c) “I have not taken it and I will not take it today”.
- -
- Pain severity: This item assesses the current level of pain (“Please indicate your current level of pain”). Responses range from 0 = “No pain” at all to 10 = “Extreme pain”.
- -
- Fatigue: This item evaluates fatigue intensity (“Please indicate your current level of fatigue”). Responses range from 0 = “No fatigue at all” to 10 = “Extreme fatigue”.
- -
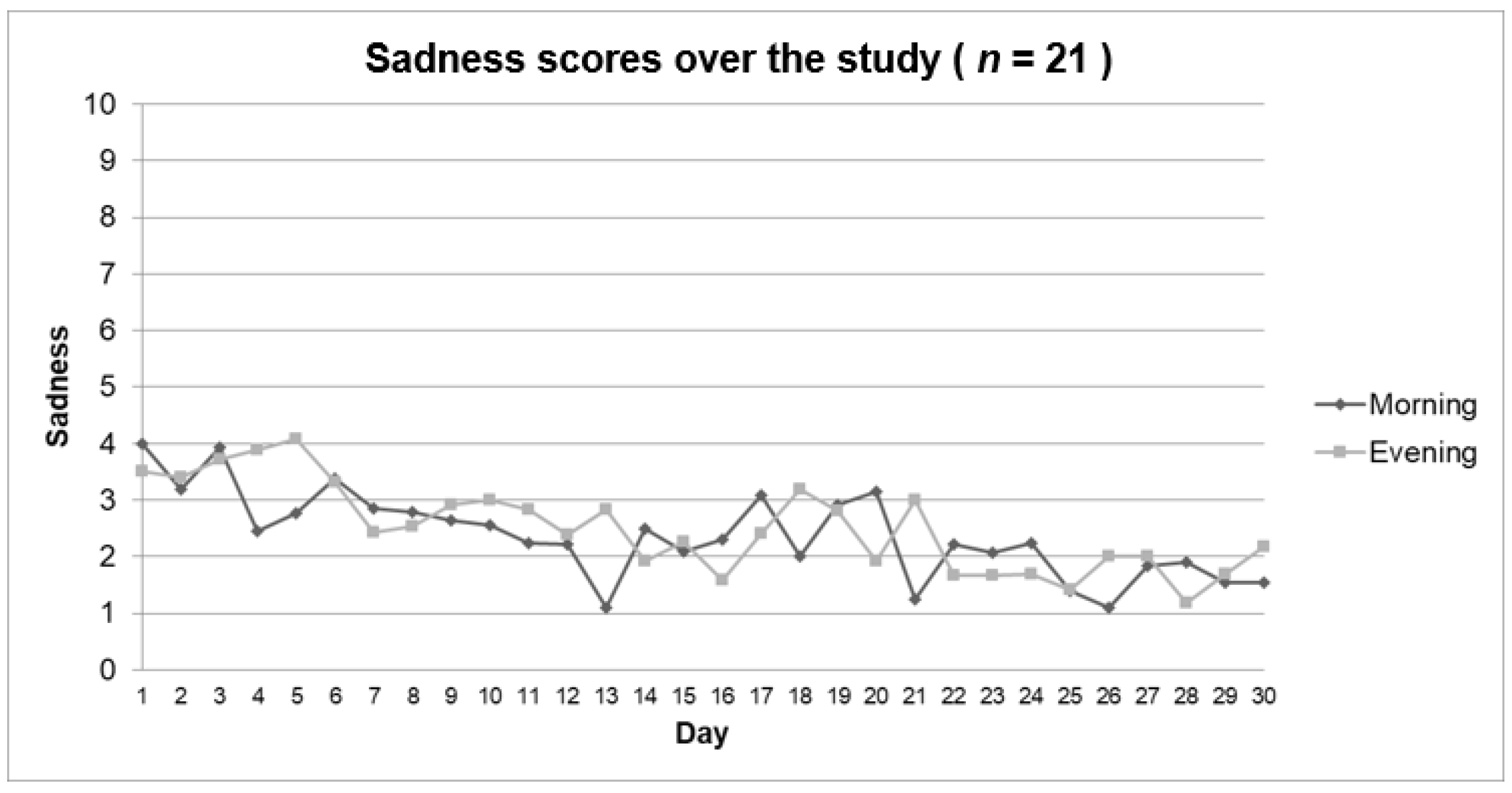
- Mood: Three items were employed to assess the intensity of happiness (“Please indicate your current level of happiness”), sadness (“Please indicate your current level of sadness”), and anxiety (“Please indicate your current level of anxiety”). The three items use a similar response scale ranging from 0 = “No happiness/sadness/anxiety” at all to 10 = “Extreme happiness/sadness/anxiety”.
- -
- Perceived utility of pain treatment: This item evaluates the perceived pain relief after the baseline pain medication intake (“Please indicate to what extent the baseline medication relieved your pain today”). Responses range from 0% = “No relief at all” to 100% = “Complete relief”.
- -
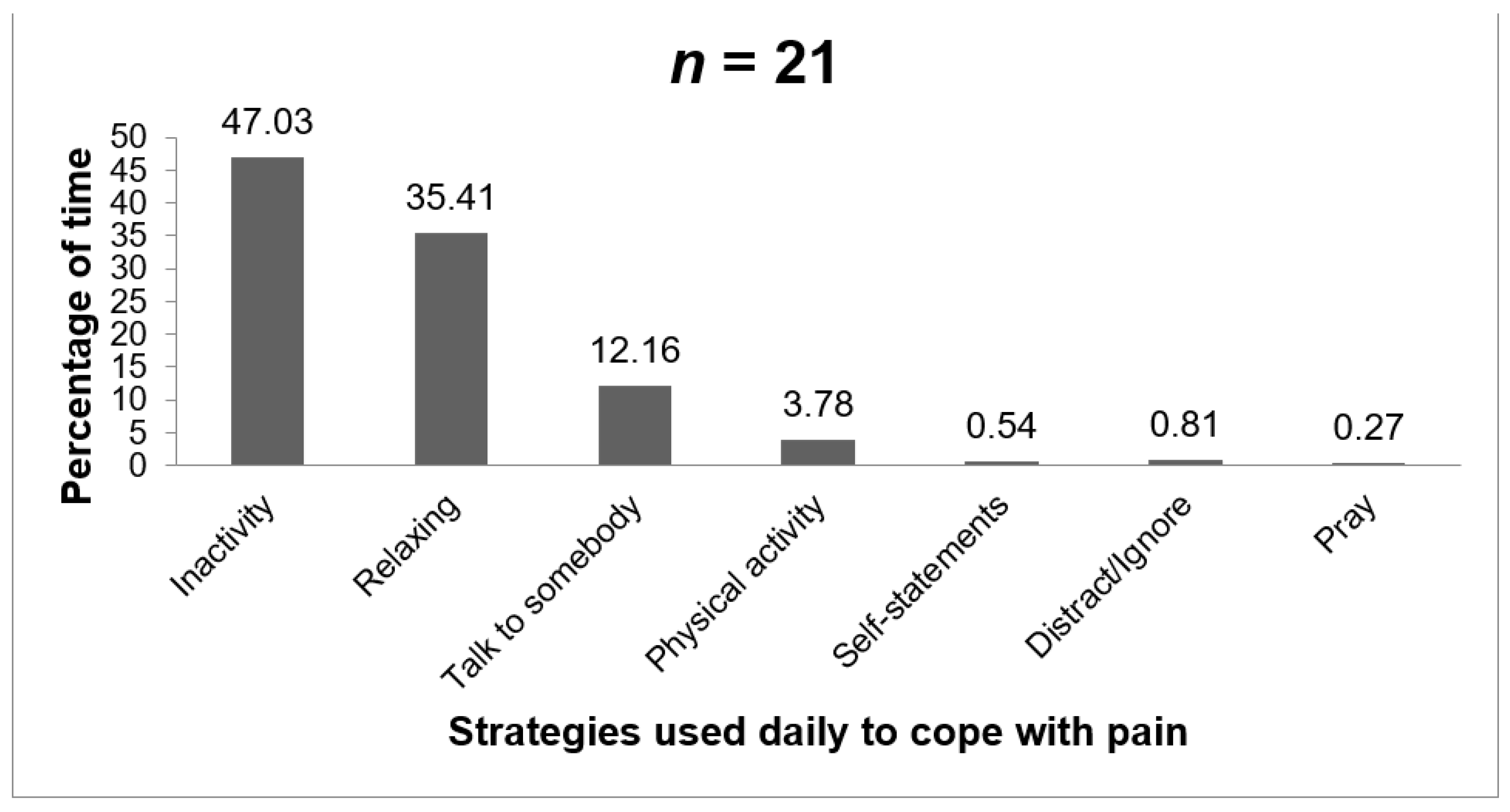
- Coping strategies: we explored the coping strategies implemented by patients on a given day (“Select the coping strategies that you have used today to cope with pain. You can choose more than one option”). The following list of coping strategies was presented to the patients: inactivity, relaxing, talking to somebody, physical activity, coping self-statements, distracting/ignoring the pain, or praying. This list was created after reviewing the most frequent coping strategies employed in pain research and was validated to be used with the app in a previous investigation [45].
2.2.2. On-Demand Assessment of Breakthrough Pain with the App
2.2.3. App Usability and Satisfaction (Evaluated by Phone or by Paper-and-Pencil)
2.2.4. Clinical Alarms
- Baseline pain > 5 for two consecutive days;
- Vomiting/nausea for two consecutive days;
- More than four episodes of breakthrough pain in 1 day;
- Breakthrough pain lasts for over 90 min.
2.3. Data Protection Policies in the App
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Cancer Pain Status and Treatment at Study Onset
3.3. Evolution of Patient Status during the Study as Reported Daily in the App
3.4. Breakthrough Pain Episodes and Characteristics
3.5. Perceived Utility of the Baseline Medication for Pain during the Study
3.6. Use of Daily Strategies to Cope with the Pain
3.7. Alarms
3.8. Feasibility
3.9. App Usability and Satisfaction (Patients and Medical Staff)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

Appendix C

References
- Løhre, E.T.; Thronæs, M.; Klepstad, P. Breakthrough cancer pain in 2020. Curr. Opin. Support. Palliat. Care 2020, 14, 94–99. [Google Scholar] [CrossRef]
- Davies, A.N.; Dickman, A.; Reid, C.; Stevens, A.M.; Zeppetella, G. The management of cancer-related breakthrough pain: Recommendations of a task group of the Science Committee of the Association for Palliative Medicine of Great Britain and Ireland. Eur. J. Pain 2009, 13, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Boceta, J.; Samper, D.; de la Torre, A.; Sánchez-de la Rosa, R.; González, G. Usability, Acceptability, and Usefulness of an mHealth App for Diagnosing and Monitoring Patients With Breakthrough Cancer Pain. JMIR Cancer 2019, 5, e10187. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Portenoy, R.K. Breakthrough cancer pain: Twenty-five years of study. Pain 2016, 157, 2657–2663. [Google Scholar] [CrossRef] [PubMed]
- Ripamonti, C.I.; Bandieri, E.; Roila, F. Management of cancer pain: ESMO clinical practice guidelines. Ann. Oncol. 2011, 22, vi69–vi77. [Google Scholar] [CrossRef]
- Deandrea, S.; Corli, O.; Consonni, D.; Villani, W.; Greco, M.T.; Apolone, G. Prevalence of breakthrough cancer pain: A systematic review and a pooled analysis of published literature. J. Pain Symptom Manag. 2014, 47, 57–76. [Google Scholar] [CrossRef]
- Calvo Verges, N.; de Castro Carpeño, J.; Gálvez Ruiz, R.; Gómez Sancho, M.; Ferri, C.; Olay Gayoso, L.; Villegas Estévez, F. DIO 360° Abordaje Integral del Paciente con Dolor Irruptivo Oncológico; LUZÁN 5, S.L: Madrid, Spain, 2015. [Google Scholar]
- Mercadante, S.; Marchetti, P.; Cuomo, A.; Caraceni, A.; Mediati, R.D.; Vellucci, R.; Mammucari, M.; Natoli, S.; Lazzari, M.; Dauri, M.; et al. Factors influencing the clinical presentation of breakthrough pain in cancer patients. Cancers 2018, 10, 175. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, V.T.; Oset, M.M.; Masferrer, J.P.; Pardo, E.H.; Sorolla, E.J.; Largo, S.C.; Tormo, V.; Marcos, M.; Pardo, J.; Aymar, N.; et al. Prevalence and characterization of breakthrough pain in cancer patients with proctalgia treated with 3D pelvic radiotherapy. Clin. Transl. Oncol. 2019, 21, 1707–1711. [Google Scholar] [CrossRef] [PubMed]
- Fortner, B.V.; Okon, T.A.; Portenoy, R.K. A survey of pain-related hospitalizations, emergency department visits, and physician office visits reported by cancer patients with and without history of breakthrough pain. J. Pain 2002, 3, 38–44. [Google Scholar] [CrossRef]
- Portenoy, R.K.; Payne, D.; Jacobsen, P. Breakthrough pain: Characteristics and impact in patients with cancer pain. Pain 1999, 81, 129–134. [Google Scholar] [CrossRef]
- Canal-Sotelo, J.; Trujillano-Cabello, J.; Larkin, P.; Arraràs-Torrelles, N.; González-Rubió, R.; Rocaspana-Garcia, M.; Barallat-Gimeno, E. Prevalence and characteristics of breakthrough cancer pain in an outpatient clinic in a Catalan teaching hospital: Incorporation of the Edmonton Classification System for Cancer pain into the diagnostic algorithm. BMC Palliat. Care 2018, 17, 81. [Google Scholar] [CrossRef]
- Mercadante, S. Breakthrough pain in cancer patients: Prevalence, mechanisms and treatment options. Curr. Opin. Anaesthesiol. 2015, 28, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Buchanan, A.; Zeppetella, G.; Porta-Sales, J.; Likar, R.; Weismayr, W.; Slama, O.; Korhonen, T.; Filbet, M.; Poulain, P.; et al. Breakthrough cancer pain: An observational study of 1000 european oncology patients. J. Pain Symptom Manag. 2013, 46, 619–628. [Google Scholar] [CrossRef]
- Davies, A.N.; Elsner, F.; Filbet, M.J.; Porta-Sales, J.; Ripamonti, C.; Santini, D.; Webber, K. Breakthrough cancer pain (BTcP) management: A review of international and national guidelines. BMJ Support. Palliat. Care 2018, 8, 241–249. [Google Scholar] [CrossRef]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef] [PubMed]
- García-Palacios, A.; Herrero, R.; Belmonte, M.A.; Castilla, D.; Guixeres, J.; Molinari, G.; Banos, R.M.; Baños, R.M.; Botella, C.; Garcia-Palacios, A.; et al. Ecological momentary assessment for chronic pain in fibromyalgia using a smartphone: A randomized crossover study. Eur. J. Pain 2014, 18, 862–872. [Google Scholar] [CrossRef]
- Davis, M.P. Fentanyl for breakthrough pain: A systematic review. Expert Rev. Neurother. 2011, 11, 1197–1216. [Google Scholar] [CrossRef] [PubMed]
- Kratz, A.L.; Murphy, S.L.; Braley, T.J. Ecological Momentary Assessment of Pain, Fatigue, Depressive, and Cognitive Symptoms Reveals Significant Daily Variability in Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2017, 98, 2142–2150. [Google Scholar] [CrossRef]
- Zeppetella, G. An assessment of the safety, efficacy, and acceptability of intranasal fentanyl citrate in the management of cancer-related breakthrough pain: A pilot study. J. Pain Symptom Manag. 2000, 20, 253–258. [Google Scholar] [CrossRef]
- Beute, F.; de Kort, Y.; Ijsselsteijn, W. Restoration in its natural context: How ecological momentary assessment can advance restoration research. Int. J. Environ. Res. Public Health 2016, 13, 420. [Google Scholar] [CrossRef]
- Lang-Rollin, I.; Berberich, G. Psycho-oncology. Dialogues Clin. Neurosci. 2018, 20, 13–21. [Google Scholar] [CrossRef]
- Bower, J.E.; Bak, K.; Berger, A.; Breitbart, W.; Escalante, C.P.; Ganz, P.A.; Schnipper, H.H.; Lacchetti, C.; Ligibel, J.A.; Lyman, G.H.; et al. Screening, assessment, and management of fatigue in adult survivors of cancer: An American Society of Clinical Oncology clinical practice guideline adaptation. J. Clin. Oncol. 2014, 32, 1840–1850. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Guglielmo, M.; Horneber, M.; Roila, F.; Weis, J.; Jordan, K.; Ripamonti, C.I. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef]
- Andersen, B.L.; DeRubeis, R.J.; Berman, B.S.; Gruman, J.; Champion, V.L.; Massie, M.J.; Holland, J.C.; Partridge, A.H.; Bak, K.; Somerfield, M.R.; et al. Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: An American Society of Clinical Oncology guideline adaptation. J. Clin. Oncol. 2014, 32, 1605–1619. [Google Scholar] [CrossRef]
- Álvarez-Salvago, F.; Galiano-Castillo, N.; Arroyo-Morales, M.; Cruz-Fernández, M.; Lozano-Lozano, M.; Cantarero-Villanueva, I. Health status among long-term breast cancer survivors suffering from higher levels of fatigue: A cross-sectional study. Support. Care Cancer 2018, 26, 3649–3658. [Google Scholar] [CrossRef]
- Gonzalez-Guerrero, J.F.; Alcorta-Garza, A.G.; Alcorta-Nuñez, F.; Melgoza-Alcorta, E.M.; Gonzalez-Rodriguez, M.; Gonzalez-Alcorta, C.B.; Alcorta-Garza, A. Association of the quality of psychosocial support and quality of life in patients with chronic oncological pain. J. Clin. Oncol. 2019, 37, e23113. [Google Scholar] [CrossRef]
- Moloney, N.A.; Pocovi, N.C.; Dylke, E.S.; Graham, P.L.; De Groef, A. Psychological Factors Are Associated with Pain at All Time Frames After Breast Cancer Surgery: A Systematic Review with Meta-Analyses. Pain Med. 2021, 22, 915–947. [Google Scholar] [CrossRef] [PubMed]
- Colombo, D.; Fernández-Álvarez, J.; Suso-Ribera, C.; Cipresso, P.; Valev, H.; Leufkens, T.; Sas, C.; Garcia-Palacios, A.; Riva, G.; Botella, C. The need for change: Understanding emotion regulation antecedents and consequences using ecological momentary assessment. Emotion 2020, 20, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of digital technologies in health care during the COVID-19 pandemic: Systematic review of early scientific literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, T.R.; Shiffman, S. Ecological Momentary Assessment. In The Wiley-Blackwell Handbook of Addiction Psychopharmacology; Wiley-Blackwell: Hoboken, NJ, USA, 2013; pp. 541–565. ISBN 9781119978268. [Google Scholar]
- Smyth, J.M. Ecological Momentary Assessment Research in Behavioral medicine. J. Happiness Stud. 2003, 4, 35–52. [Google Scholar] [CrossRef]
- Armstrong, K.A.; Semple, J.L.; Coyte, P.C. Replacing ambulatory surgical follow-up visits with mobile app home monitoring: Modeling cost-effective scenarios. J. Med. Internet Res. 2014, 16, e213. [Google Scholar] [CrossRef] [PubMed]
- Kaasa, S.; Loge, J.H.; Aapro, M.; Albreht, T.; Anderson, R.; Bruera, E.; Brunelli, C.; Caraceni, A.; Cervantes, A.; Currow, D.C.; et al. Integration of oncology and palliative care: A Lancet Oncology Commission. Lancet Oncol. 2018, 19, e588–e653. [Google Scholar] [CrossRef]
- Denis, F.; Basch, E.; Septans, A.-L.; Bennouna, J.; Urban, T.; Dueck, A.C.; Letellier, C. Two-Year Survival Comparing Web-Based Symptom Monitoring vs Routine Surveillance Following Treatment for Lung Cancer. JAMA 2019, 321, 306. [Google Scholar] [CrossRef]
- May, M.; Junghaenel, D.U.; Ono, M.; Stone, A.A.; Schneider, S. Ecological Momentary Assessment Methodology in Chronic Pain Research: A Systematic Review. J. Pain 2018, 19, 699–716. [Google Scholar] [CrossRef]
- Eurostat Individuals Using the Internet for Seeking Health-Related Information. Available online: https://ec.europa.eu/eurostat/databrowser/view/tin00101/default/table?lang=en (accessed on 17 December 2019).
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Mesas, Á.; Server, A.; Medel, J.; García-Palacios, A. Telemonitoring in chronic pain management using smartphone apps: A randomized controlled trial comparing usual assessment against app-based monitoring with and without clinical alarms. Int. J. Environ. Res. Public Health 2020, 17, 6568. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, K.A.; Coyte, P.C.; Bhatia, R.S.; Semple, J.L. The Effect of Mobile App Home Monitoring on Number of In-Person Visits Following Ambulatory Surgery: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2015, 4, e65. [Google Scholar] [CrossRef]
- Balestrieri, M.; Isola, M.; Bonn, R.; Tam, T.; Vio, A.; Linden, M.; Maso, E. Validation of the Italian version of Mini-ICF-APP, a short instrument for rating activity and participation restrictions in psychiatric disorders. Epidemiol. Psychiatr. Sci. 2013, 22, 81–91. [Google Scholar] [CrossRef]
- Spook, J.E.; Paulussen, T.; Kok, G.; Van Empelen, P. Monitoring dietary intake and physical activity electronically: Feasibility, usability, and ecological validity of a mobile-based ecological momentary assessment tool. J. Med. Internet Res. 2013, 15, e214. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Weng, L.; Chen, Z.; Cai, H.; Lin, X.; Hu, Z.; Li, N.; Lin, B.; Zheng, B.; Zhuang, Q.; et al. Development and testing of a mobile app for pain management among cancer patients discharged from hospital treatment: Randomized controlled trial. JMIR mHealth uHealth 2019, 7, e12542. [Google Scholar] [CrossRef]
- Salazar, A.; de Sola, H.; Failde, I.; Moral-Munoz, J.A. Measuring the quality of mobile apps for the management of pain: Systematic search and evaluation using the mobile app rating scale. JMIR mHealth uHealth 2018, 6, e10718. [Google Scholar] [CrossRef]
- Zhao, P.; Yoo, I.; Lancey, R.; Varghese, E. Mobile applications for pain management: An app analysis for clinical usage. BMC Med. Inform. Decis. Mak. 2019, 19, 106. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Ribera-Canudas, M.V.; Botella, C.; García-Palacios, A. Validity, Reliability, Feasibility, and Usefulness of Pain Monitor, a Multidimensional Smartphone App for Daily Monitoring of Adults with Heterogeneous Chronic Pain. Clin. J. Pain 2018, 34, 900–908. [Google Scholar] [CrossRef]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A “quick and dirty” usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, A.B., McClelland, I.L., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Zeppetella, G.; Davies, A.; Eijgelshoven, I.; Jansen, J.P. A Network Meta-Analysis of the Efficacy of Opioid Analgesics for the Management of Breakthrough Cancer Pain Episodes. J. Pain Symptom Manag. 2014, 47, 772–785.e5. [Google Scholar] [CrossRef]
- Mercadante, S.; Caraceni, A.; Masedu, F.; Scipioni, T.; Aielli, F. Breakthrough Cancer Pain in Patients Receiving Low Doses of Opioids for Background Pain. Oncologist 2020, 25, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Gatti, A.; Mediati, R.D.; Reale, C.; Cuomo, A.; Vellucci, R.; Russo, G.; Costantini, A.; Canneti, A.; Luzi, M.; Mammucari, M.; et al. Breakthrough pain in patients referred to pain clinics: The Italian pain network retrospective study. Adv. Ther. 2012, 29, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Richarz, U. End-of-Dose Pain in Chronic Pain: Does it Vary with the Use of Different Long-Acting Opioids? Pain Pract. 2014, 14, 757–769. [Google Scholar] [CrossRef]
- Timmerman, J.G.; Dekker-van Weering, M.G.H.; Tönis, T.M.; Hermens, H.J.; Vollenbroek-Hutten, M.M.R. Relationship between patterns of daily physical activity and fatigue in cancer survivors. Eur. J. Oncol. Nurs. 2015, 19, 162–168. [Google Scholar] [CrossRef]
- Zheng, J.; Chernack, B. Cancer-Related Fatigue in Breast and Gynecologic Cancers. In Breast Cancer and Gynecologic Cancer Rehabilitation; Elsevier: Amsterdam, The Netherlands, 2021; pp. 39–50. [Google Scholar]
- Chien, T.W.; Lai, C.Y.; Huang, S.S.; Tsai, L.Y.; Tsai, M.C.; Tsay, S.L. Cancer pain and lower functional status predict poor trajectories of symptom and fatigue distress in patients with lung cancer. Eur. J. Cancer Care 2021, 30, e13403. [Google Scholar] [CrossRef] [PubMed]
- Theobald, D.E. Cancer pain, fatigue, distress, and insomnia in cancer patients. Clin. Cornerstone 2004, 6, S15–S21. [Google Scholar] [CrossRef]
- Christe, G.; Pizzolato, V.; Meyer, M.; Nzamba, J.; Pichonnaz, C. Unhelpful beliefs and attitudes about low back pain in the general population: A cross-sectional survey. Musculoskelet. Sci. Pract. 2021, 52, 102342. [Google Scholar] [CrossRef] [PubMed]
- Esteve, R.; Ramírez-Maestre, C.; López-Martínez, A. Adjustment to Chronic Pain: The Role of Pain Acceptance, Coping Strategies, and Pain-Related Cognitions Rosa. Ann. Behav. Med. 2007, 33, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Ramond, A.; Bouton, C.; Richard, I.; Roquelaure, Y.; Baufreton, C.; Legrand, E.; Huez, J.F. Psychosocial risk factors for chronic low back pain in primary care—A systematic review. Fam. Pract. 2011, 28, 12–21. [Google Scholar] [CrossRef]
- Tan, G.; Teo, I.; Anderson, K.O.; Jensen, M.P. Adaptive versus maladaptive coping and beliefs and their relation to chronic pain adjustment. Clin. J. Pain 2011, 27, 769–774. [Google Scholar] [CrossRef]
- Vowles, K.E.; McCracken, L.M.; Sowden, G.; Ashworth, J. Psychological Flexibility in Coping with Chronic Pain. Clin. J. Pain 2014, 30, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Suso-Ribera, C.; Camacho-Guerrero, L.; McCracken, L.M.; Maydeu-Olivares, A.; Gallardo-Pujol, D. Social problem solving in chronic pain: An integrative model of coping predicts mental health in chronic pain patients. J. Health Psychol. 2016, 21, 1015–1025. [Google Scholar] [CrossRef]
- Sheppes, G.; Scheibe, S.; Suri, G.; Gross, J.J. Emotion-Regulation Choice. Psychol. Sci. 2011, 22, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Suso-Ribera, C.; Mesas, A.; Medel, J.; Server, A.; Marquez, E.; Castilla, D.; Zaragoza, I.; Garcia-Palacios, A. Improving pain treatment with a smartphone app: Study protocol for a randomized controlled trial. Trials 2018, 19, 145. [Google Scholar] [CrossRef]
- Statcounter Global Stats Mobile Operating System Market Share Spain. Available online: https://gs.statcounter.com/os-market-share/mobile/spain (accessed on 3 May 2021).
- Cheng, C.; Ho, R.T.H.; Guo, Y.; Zhu, M.; Yang, W.; Li, Y.; Liu, Z.; Zhuo, S.; Liang, Q.; Chen, Z.; et al. Development and Feasibility of a Mobile Health–Supported Comprehensive Intervention Model (CIMmH) for Improving the Quality of Life of Patients With Esophageal Cancer After Esophagectomy: Prospective, Single-Arm, Nonrandomized Pilot Study. J. Med. Internet Res. 2020, 22, e18946. [Google Scholar] [CrossRef]
- Crafoord, M.-T.; Fjell, M.; Sundberg, K.; Nilsson, M.; Langius-Eklöf, A. Engagement in an Interactive App for Symptom Self-Management during Treatment in Patients With Breast or Prostate Cancer: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e17058. [Google Scholar] [CrossRef] [PubMed]
- Moradian, S.; Krzyzanowska, M.K.; Maguire, R.; Morita, P.P.; Kukreti, V.; Avery, J.; Liu, G.; Cafazzo, J.; Howell, D. Usability Evaluation of a Mobile Phone–Based System for Remote Monitoring and Management of Chemotherapy-Related Side Effects in Cancer Patients: Mixed-Methods Study. JMIR Cancer 2018, 4, e10932. [Google Scholar] [CrossRef]
- Zapata, B.C.; Fernández-Alemán, J.L.; Idri, A.; Toval, A. Empirical Studies on Usability of mHealth Apps: A Systematic Literature Review. J. Med. Syst. 2015, 39, 1. [Google Scholar] [CrossRef] [PubMed]
- Kongshaug, N.; Skolbekken, J.-A.; Faxvaag, A.; Hofsli, E. Cancer Patients’ Perceived Value of a Smartphone App to Enhance the Safety of Home-Based Chemotherapy: Feasibility Study. JMIR Form. Res. 2021, 5, e20636. [Google Scholar] [CrossRef] [PubMed]
- Low, C.A.; Danko, M.; Durica, K.C.; Kunta, A.R.; Mulukutla, R.; Ren, Y.; Bartlett, D.L.; Bovbjerg, D.H.; Dey, A.K.; Jakicic, J.M. A Real-Time Mobile Intervention to Reduce Sedentary Behavior Before and After Cancer Surgery: Usability and Feasibility Study. JMIR Perioper. Med. 2020, 3, e17292. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Morning | Evening | Comparison and Effect Size | |||||
|---|---|---|---|---|---|---|---|
| Variables | Mean (SD) | Median | Mean (SD) | Median | t | p | d |
| Pain severity | 2.88 (2.08) | 2.83 | 3.52 (2.29) | 3.55 | 0.88 | 0.383 | 0.27 |
| Fatigue | 3.13 (2.37) | 3.03 | 3.75 (2.36) | 3.83 | 0.95 | 0.350 | 0.29 |
| Happiness | 3.83 (2.33) | 4.10 | 3.58 (2.38) | 3.88 | 0.34 | 0.733 | 0.11 |
| Sadness | 2.38 (2.55) | 1.62 | 2.51 (2.55) | 1.97 | 0.17 | 0.870 | 0.05 |
| Anxiety | 1.67 (2.14) | 0.73 | 1.65 (2.01) | 0.92 | 0.03 | 0.975 | 0.01 |
| Patient ID | BTcP Episodes | Onset Time | Pain at Onset | Time of Loop 1 | Pain at Loop 1 | Time of Loop 2 | Pain at Loop 2 | Time of Loop 3 | Pain at Loop 3 | Duration of Episode |
|---|---|---|---|---|---|---|---|---|---|---|
| Onco0022 | 4 | 21:32 | 7 | 22:05 | 4 | <30′ | ||||
| 09:27 | 7 | 10:01 | 4 | <30′ | ||||||
| 21:41 | 7 | 22:13 | 3 | <30′ | ||||||
| 08:32 | 7 | 09:04 | 6 | 09:44 | 4 | 30–60′ | ||||
| Onco0026 | 1 | 20:12 | 6 | 20:45 | 3 | <30′ | ||||
| Onco0028 | 1 | 22:56 | 7 | 23:31 | 2 | <30′ | ||||
| Onco0030 | 1 | 20:00 | 7 | 20:34 | 3 | <30′ | ||||
| Onco0034 | 6 | 12:54 | 8 | 13:37 | 6 | 14:08:47 | 2 | 30–60′ | ||
| 14:25 | 6 | 14:59 | 3 | <30′ | ||||||
| 14:19 | 6 | 15:01 | 6 | 15:32:49 | 5 | 16:04:13 | 3 | 60–90′ | ||
| 13:13 | 7 | 13:49 | 3 | <30′ | ||||||
| 13:57 | 7 | 14:39 | 3 | <30′ | ||||||
| 12:56 | 8 | 13:29 | 3 | <30′ | ||||||
| Onco0062 | 3 | 01:53 | 8 | 2:26 | 9 | 2:58 | 3 | 30–60′ | ||
| 10:39 | 8 | 11:11 | 3 | <30′ | ||||||
| 10:26 | 7 | 11:09 | 8 | 11:40 | 3 | 30–60′ | ||||
| Onco0068 | 1 | 19:04 | 6 | 19:36 | 3 | <30′ | ||||
| Onco0076 | 1 | 23:57 | 6 | 00:29 | 4 | <30′ | ||||
| Onco0087 | 1 | 14:35 | 7 | 15:10 | 2 | <30′ |
| Patient ID | Alarm | Medical Response to the Alarm |
|---|---|---|
| Onco0022 | Baseline pain > 5 during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0022 | Baseline pain > 5 during 2 consecutive days | Telephone contact to arrange an appointment |
| Onco0022 | Baseline pain > 5 during 2 consecutive days | Telephone contact to arrange an appointment |
| Onco0022 | Baseline pain > 5 during 2 consecutive days | Telephone contact to arrange an appointment |
| Onco0022 | Baseline pain > 5 during 2 consecutive days | Telephone contact to increase medication |
| Onco0028 | Baseline pain > 5 during 2 consecutive days Vomiting during 2 consecutive days Nausea during 2 consecutive days | Telephone contact to increase medication |
| Onco0030 | Baseline pain > 5 during 2 consecutive days | Hospitalization due to difficult pain control |
| Onco0034 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0034 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0034 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0034 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0061 | Sleepiness/sedation during 2 consecutive days | Telephone contact to increase medication |
| Onco0061 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0067 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0064 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0067 | Sleepiness/sedation during 2 consecutive days | Telephone contact to arrange an appointment |
| Onco0067 | Sleepiness/sedation during 2 consecutive days | Telephone contact to increase medication |
| Onco0064 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0064 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0072 | Sleepiness/sedation during 2 consecutive days | Unsuccessful attempts to contact the patient |
| Onco0072 | Sleepiness/sedation during 2 consecutive days | Unsuccessful attempts to contact the patient |
| Onco0072 | Sleepiness/sedation during 2 consecutive days | Unsuccessful attempts to contact the patient |
| Onco0072 | Sleepiness/sedation during 2 consecutive days | Unsuccessful attempts to contact the patient |
| Onco0072 | Sleepiness/sedation during 2 consecutive days | Telephone contact to provide medical advice |
| Onco0073 | Baseline pain > 5 during 2 consecutive days | Telephone contact to provide medical advice |
| Main Conclusions Derived from Our Study |
|---|
| Ecological momentary characterization of baseline and BTcP episodes reported similar results compared to previous similar studies (i.e., BTcP pain intensity and duration) |
| Health-related variables, such as fatigue, mood, and coping, should be assessed in oncological care |
| Clinical alarms in the app were useful to detect undesirable events in the real context in which they occur. They help the professionals to rapidly detect and react to such events if necessary |
| App-based EMA is considered to be feasible by patients and clinicians, which supports that it can potentially be implemented in public health settings |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villegas, F.; Martínez-Borba, V.; Suso-Ribera, C.; Castilla, D.; Zaragoza, I.; García-Palacios, A.; Ferrer, C. Characterizing Breakthrough Cancer Pain Using Ecological Momentary Assessment with a Smartphone App: Feasibility and Clinical Findings. Int. J. Environ. Res. Public Health 2021, 18, 5991. https://doi.org/10.3390/ijerph18115991
Villegas F, Martínez-Borba V, Suso-Ribera C, Castilla D, Zaragoza I, García-Palacios A, Ferrer C. Characterizing Breakthrough Cancer Pain Using Ecological Momentary Assessment with a Smartphone App: Feasibility and Clinical Findings. International Journal of Environmental Research and Public Health. 2021; 18(11):5991. https://doi.org/10.3390/ijerph18115991
Chicago/Turabian StyleVillegas, Francisco, Verónica Martínez-Borba, Carlos Suso-Ribera, Diana Castilla, Irene Zaragoza, Azucena García-Palacios, and Carlos Ferrer. 2021. "Characterizing Breakthrough Cancer Pain Using Ecological Momentary Assessment with a Smartphone App: Feasibility and Clinical Findings" International Journal of Environmental Research and Public Health 18, no. 11: 5991. https://doi.org/10.3390/ijerph18115991
APA StyleVillegas, F., Martínez-Borba, V., Suso-Ribera, C., Castilla, D., Zaragoza, I., García-Palacios, A., & Ferrer, C. (2021). Characterizing Breakthrough Cancer Pain Using Ecological Momentary Assessment with a Smartphone App: Feasibility and Clinical Findings. International Journal of Environmental Research and Public Health, 18(11), 5991. https://doi.org/10.3390/ijerph18115991