
Effects of Clinical Pathways on Cesarean Sections in China: Length of Stay and Direct Hospitalization Cost Based on Meta-Analysis of Randomized Controlled Trials and Controlled Clinical Trials


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
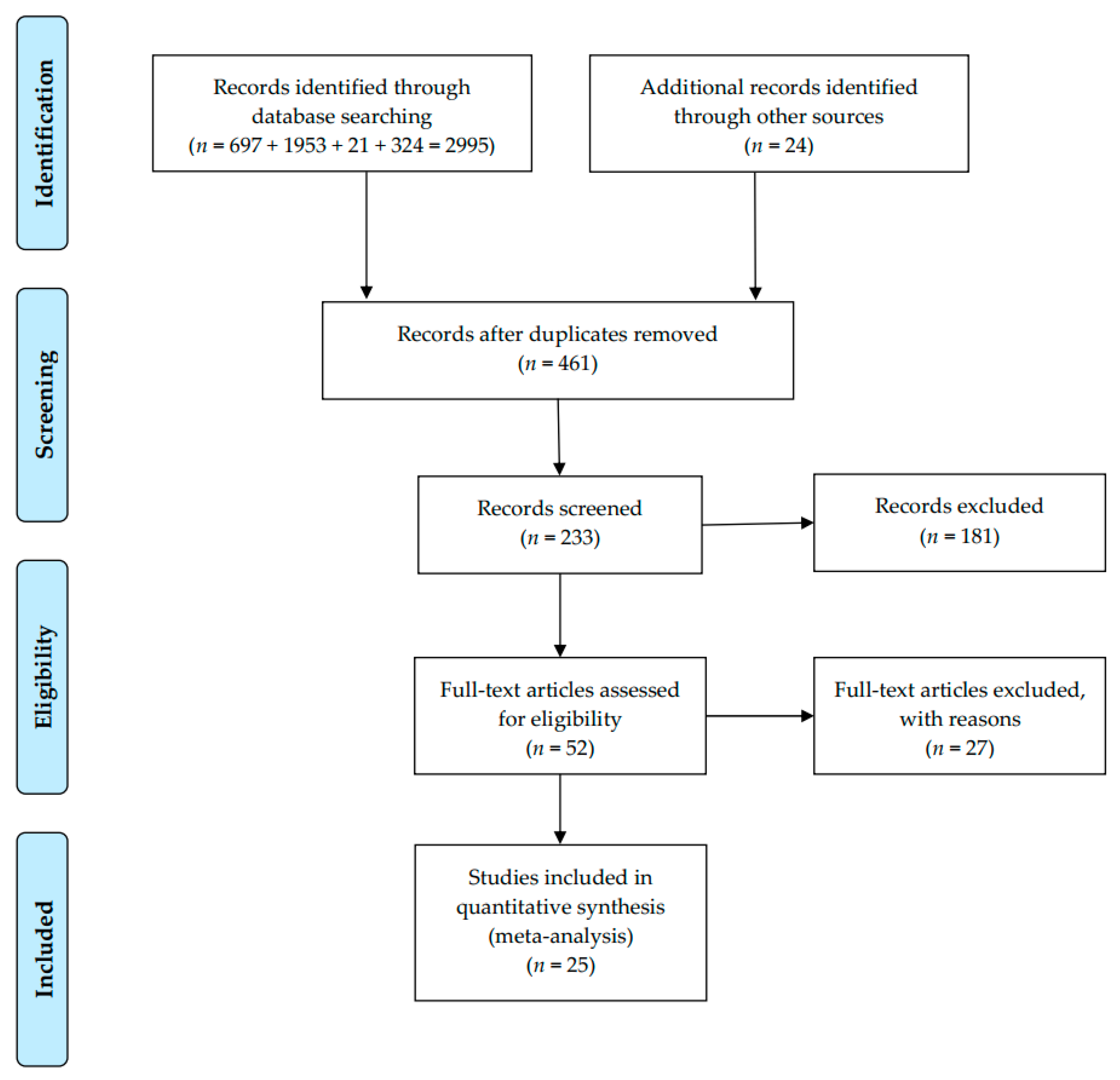
2.3. Search and Study Selection
2.4. Statistics Items and Data Collection Process
2.5. Risk of Bias Assessment
2.6. Summary Measures
2.7. Synthesis of Results and Data Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Risk of Bias within Studies (Quality Assessment)
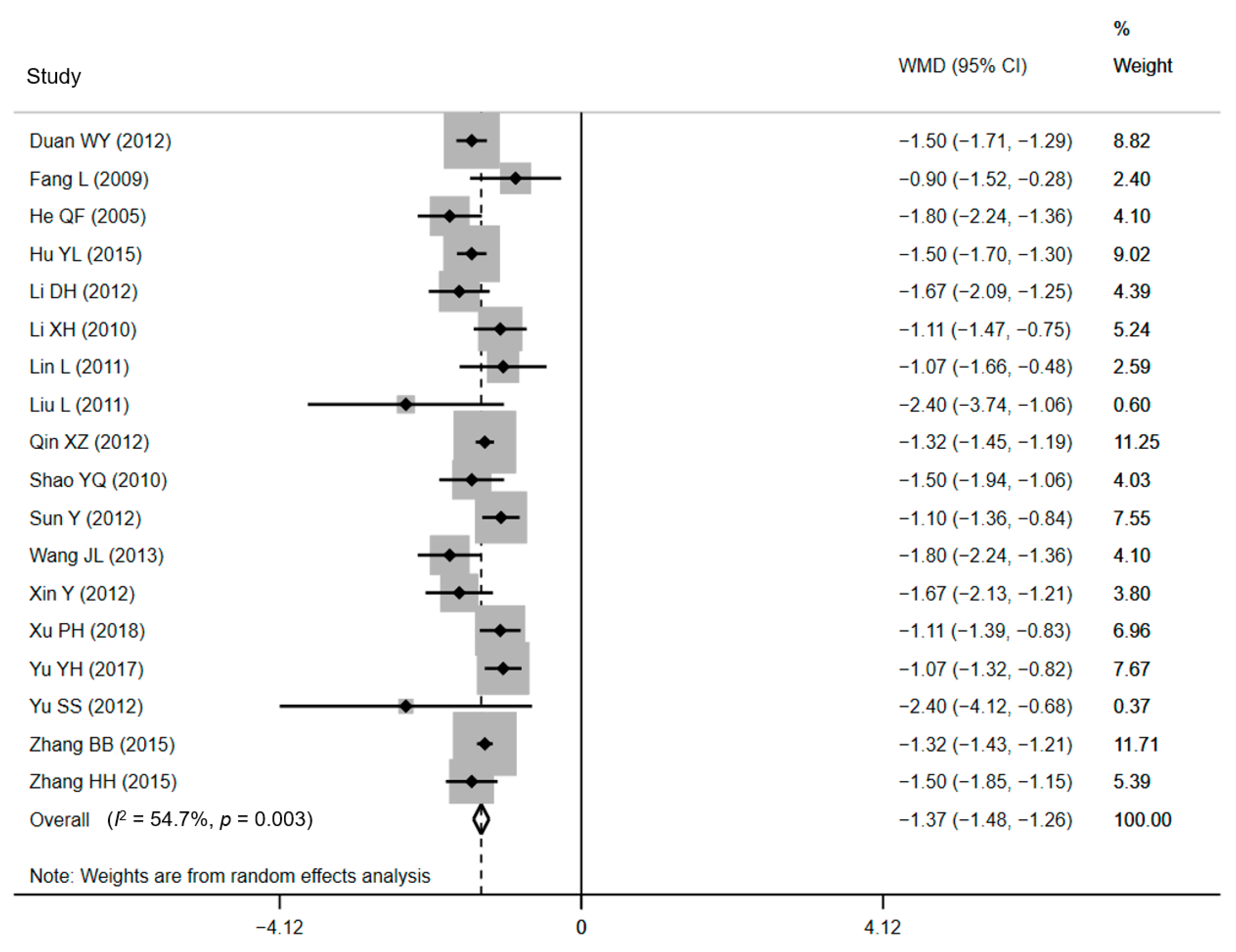
3.3. Effect of CPW: LOS
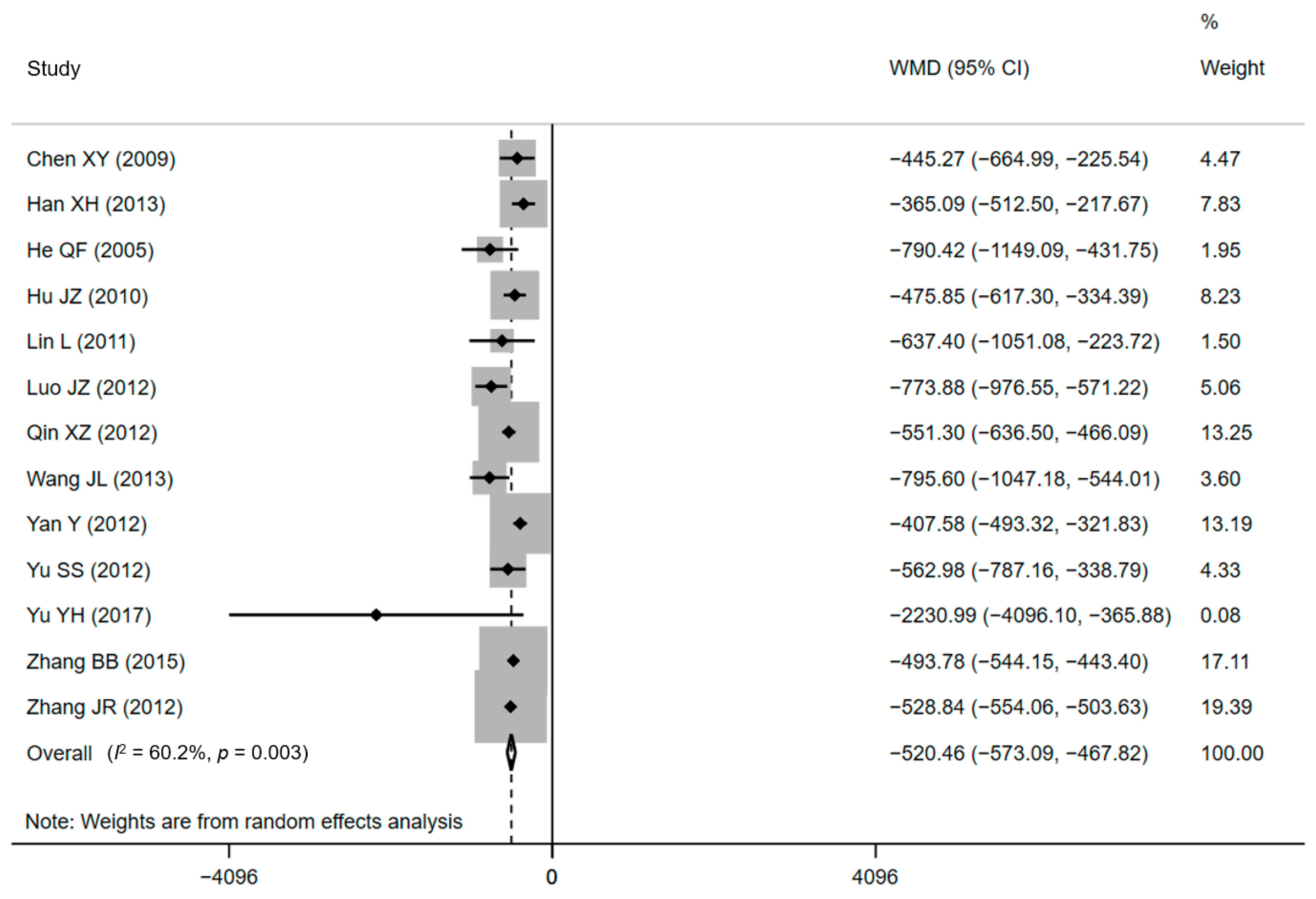
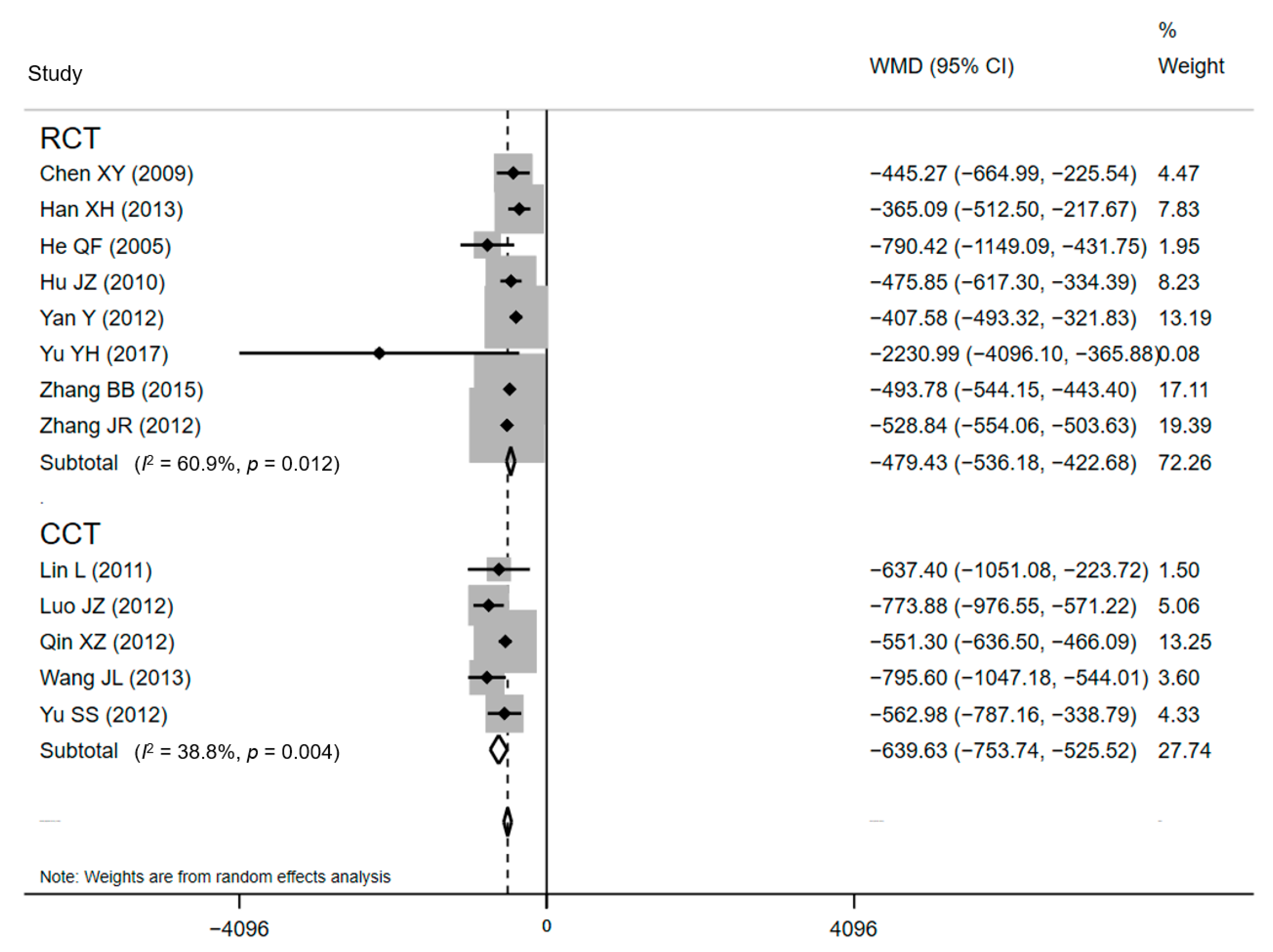
3.4. Effect of CPW: DHC
3.5. Sensitivity Analyses and Publication Bias
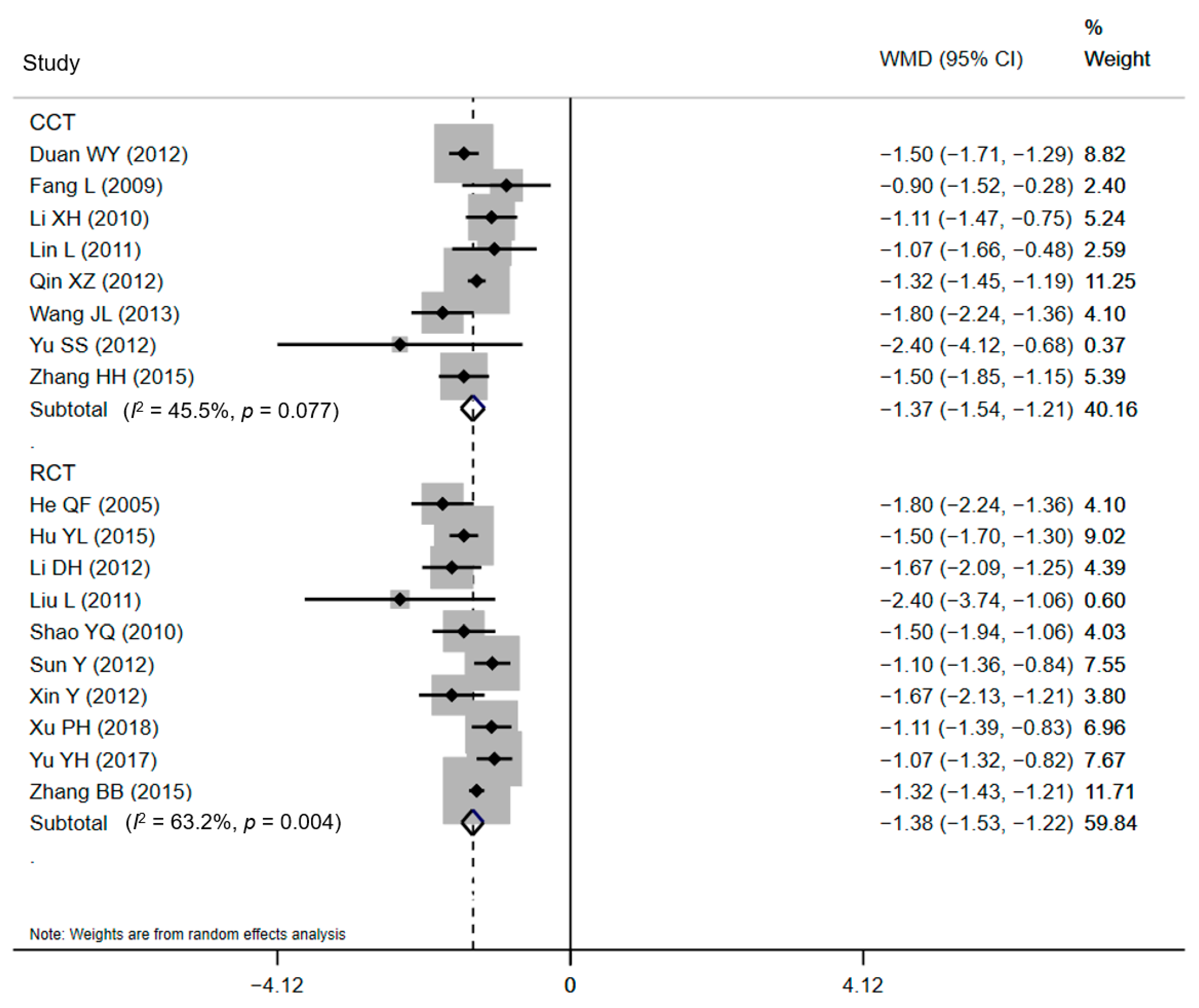
3.6. Meta-Regression and Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.; Barros, F.C.; Juan, L.; Moller, A.B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global epidemiology of use of and disparities in caesarean sections. Lancet 2018, 392, 1341–1348. [Google Scholar] [CrossRef]
- Wang, X.; Hellerstein, S.; Hou, L.; Zou, L.; Ruan, Y.; Zhang, W. Caesarean deliveries in China. BMC Pregnancy Childbirth 2017, 17, 54. [Google Scholar] [CrossRef]
- Gao, Y.; Tang, Y.; Tong, M.; Du, Y.; Chen, Q. Does attendance of a prenatal education course reduce rates of caesarean section on maternal request? A questionnaire study in a tertiary women hospital in Shanghai, China. BMJ Open 2019, 9, e029437. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Meikle, S.; Zheng, J.; Sun, W.; Li, Z. Cesarean delivery on maternal request in southeast China. Obstet. Gynecol. 2008, 111, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Xu, L.; Guo, Y.; Ronsmans, C. Factors influencing rising caesarean section rates in China between 1988 and 2008. Bull. World Health Organ. 2012, 90, 30–39. [Google Scholar] [CrossRef]
- Hong, X. Factors related to the high cesarean section rate and their effects on the “price transparency policy” in Beijing, China. Tohoku J. Exp. Med. 2007, 212, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Bogg, L.; Huang, K.; Long, Q.; Shen, Y.; Hemminki, E. Dramatic increase of Cesarean deliveries in the midst of health reforms in rural China. Soc. Sci. Med. 2010, 70, 1544–1549. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Zhang, Y.; Raven, J.; Wu, Z.; Bogg, L.; Tang, S.; Hemminki, E. Giving birth at a health-care facility in rural China: Is it affordable for the poor? Bull. World Health Organ. 2011, 89, 144–152. [Google Scholar] [CrossRef]
- Cai, W.W.; Marks, J.S.; Chen, C.H.; Zhuang, Y.X.; Morris, L.; Harris, J.R. Increased cesarean section rates and emerging patterns of health insurance in Shanghai, China. Am. J. Public Health 1998, 88, 777–780. [Google Scholar] [CrossRef]
- Brunenberg, D.E.; van Steyn, M.J.; Sluimer, J.C.; Bekebrede, L.L.; Bulstra, S.K.; Joore, M.A. Joint recovery programme versus usual care: An economic evaluation of a clinical pathway for joint replacement surgery. Med. Care 2005, 43, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, A.; Vanhaecht, K.; Van Herck, P.; Sermeus, W.; Faggiano, F.; Marchisio, S.; Panella, M. Effects of clinical pathways in the joint replacement: A meta-analysis. BMC Med. 2009, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Aspland, E.; Gartner, D.; Harper, P. Clinical pathway modelling: A literature review. Health Syst. 2019, 10, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Padman, R. Data-driven clinical and cost pathways for chronic care delivery. Am. J. Manag. Care 2016, 22, 816–820. [Google Scholar]
- Kim, S.; Losina, E.; Solomon, D.H.; Wright, J.; Katz, J.N. Effectiveness of clinical pathways for total knee and total hip arthroplasty: Literature review. J. Arthroplast. 2003, 18, 69–74. [Google Scholar] [CrossRef]
- Panella, M.; Marchisio, S.; Di Stanislao, F. Reducing clinical variations with clinical pathways: Do pathways work? Int. J. Qual. Health Care 2003, 15, 509–521. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Sermeus, W.; Tuerlinckx, G.; Witters, I.; Vandenneucker, H.; Bellemans, J. Development of a clinical pathway for total knee arthroplasty and the effect on length of stay and in-hospital functional outcome. Acta Orthop. Belg. 2005, 71, 439–444. [Google Scholar] [PubMed]
- Vanhaecht, K.; Bellemans, J.; De Witte, K.; Diya, L.; Lesaffre, E.; Sermeus, W. Does the organization of care processes affect outcomes in patients undergoing total joint replacement? J. Eval. Clin. Pract. 2010, 16, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Campbell, H.; Hotchkiss, R.; Bradshaw, N.; Porteous, M. Integrated care pathways. BMJ 1998, 316, 133–137. [Google Scholar] [CrossRef]
- Rotter, T.; Kugler, J.; Koch, R.; Gothe, H.; Twork, S.; van Oostrum, J.M.; Steyerberg, E.W. A systematic review and meta-analysis of the effects of clinical pathways on length of stay, hospital costs and patient outcomes. BMC Health Serv. Res. 2008, 8, 265. [Google Scholar] [CrossRef]
- Song, X.P.; Tian, J.H.; Cui, Q.; Zhang, T.T.; Yang, K.H.; Ding, G.W. Could clinical pathways improve the quality of care in patients with gastrointestinal cancer? A meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 8361–8366. [Google Scholar] [CrossRef]
- El Baz, N.; Middel, B.; van Dijk, J.P.; Oosterhof, A.; Boonstra, P.W.; Reijneveld, S.A. Are the outcomes of clinical pathways evidence-based? A critical appraisal of clinical pathway evaluation research. J. Eval. Clin. Pract. 2007, 13, 920–929. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Jefferson, T.O. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ 1996, 313, 275–283. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Mulrow, O.A. Cochrane Collaboration Handbook; John Wiley & Sons, Ltd.: Chichester, UK, 2011. [Google Scholar]
- Paz-Bailey, G.; Noble, M.; Salo, K.; Tregear, S.J. Prevalence of HIV among U.S. female sex workers: Systematic review and meta-analysis. AIDS Behav. 2016, 20, 2318–2331. [Google Scholar] [CrossRef] [PubMed]
- Melsen, W.G.; Bootsma, M.C.; Rovers, M.M.; Bonten, M.J. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration, 2011. Available online: www.handbook.cochrane.org (accessed on 20 March 2021).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Kiran, A.; Crespillo, A.P.; Rahimi, K. Graphics and statistics for cardiology: Data visualisation for meta-analysis. Heart 2017, 103, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Normand, S.L. Meta-analysis: Formulating, evaluating, combining, and reporting. Stat. Med. 1999, 18, 321–359. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Palmer, T.M.; Peters, J.L.; Sutton, A.J.; Moreno, S.G. Contour-enhanced funnel plots for meta-analysis. Stata J. 2008, 8, 242–254. [Google Scholar] [CrossRef]
- Chen, X.Y.; Da, S.C.; Zhang, S.Q.; Wang, Q.Y.; Zhao, M. The effect evaluation of clinical pathway in planned cesarean section. Mod. Med. Health 2009, 25, 2298–2300. (In Chinese) [Google Scholar]
- Duan, W.Y. Application of clinical pathway in planned cesarean section. Chin. Community Dr. Med. Ed. 2012, 14, 151–152. (In Chinese) [Google Scholar]
- Fang, L.; Mao, J.E.; Wang, N.; Xue, T.H.; Tang, J.Q.; Chen, H.Q. Clinical pathway of cesarean delivery. J. Nurs. 2009, 24, 19–20. (In Chinese) [Google Scholar]
- Han, X.H.; Zhang, Q.Q.; Luo, W.Y. Application and effect analysis of clinical pathway in planned cesarean section. Land Reclam. Med. 2013, 35, 195–197. (In Chinese) [Google Scholar]
- He, Q.F.; Zhu, L.L. Application of clinical pathway in selective cesarean section. Chin. J. Mod. Clin. Med. 2005, 3, 16. (In Chinese) [Google Scholar]
- Hu, Y.L. Application of planned cesarean section clinical pathway in primary hospital. Mod. Hosp. 2015, 15, 110. (In Chinese) [Google Scholar]
- Hu, J.Z.; Zhou, X.M.; Fang, M.Z. The application of clinical pathway in the management of single disease of cesarean section. Chin. Prim. Med. 2010, 17, 2293–2294. (In Chinese) [Google Scholar]
- Li, D.H. Evaluation of the effect of clinical pathway application in planned cesarean section. Mod. Distance Educ. Tradit. Chin. Med. China 2012, 10, 134. (In Chinese) [Google Scholar]
- Li, X.H.; Peng, Q.Y. The effect of clinical pathway in cesarean section. Mod. Drug Appl. China 2010, 4, 85. (In Chinese) [Google Scholar]
- Lin, L. Application of clinical pathway in planned cesarean section. Health Qual. Manag. China 2011, 18, 8–10. (In Chinese) [Google Scholar]
- Liu, L.; Tan, Y.; Lai, C.S.; Luo, Q.L.; Yang, D.M. Evaluation of clinical pathway in planned cesarean section. Chin. Community Dr. Med. Ed. 2011, 13, 150. (In Chinese) [Google Scholar]
- Luo, J.Z.; Zou, X.G.; Wang, X.S. Analysis of the cost of hospitalization in the implementation of the clinical pathway of lower uterine cesarean section. Chin. Community Dr. Med. Ed. 2012, 14, 142–143. (In Chinese) [Google Scholar]
- Qin, X.Z. The application of clinical pathway in the management of single disease of cesarean section. Massage Rehabil. Med. 2012, 3, 33. (In Chinese) [Google Scholar]
- Shao, Y.Q.; Wang, M.Y.; Nie, T.Y. Application of clinical pathway in selective cesarean section. Qilu J. Nurs. 2010, 16, 70–71. (In Chinese) [Google Scholar]
- Sun, Y.; Wu, Q.; Ren, N.Z. Retrospective analysis of clinical pathway application of planned cesarean section. Mod. Hosp. Manag. 2012, 10, 56–58. (In Chinese) [Google Scholar]
- Wang, J.L.; Ge, X.H.; Gan, N. Analysis of the effect of the clinical pathway of planned cesarean section. China Health Ind. 2013, 10, 26–27. (In Chinese) [Google Scholar]
- Wang, Y. To observe the clinical application effect of clinical pathway in caesarean section. Chin. Med. Innovat. 2013, 10, 129–130. (In Chinese) [Google Scholar]
- Xin, Y.; Fu, Q. Application of clinical pathway in the standardized diagnosis and treatment of planned cesarean section. Chin. Clin. Res. 2012, 25, 414–415. (In Chinese) [Google Scholar]
- Xu, P.H.; Zou, W.J.; Wang, G.P.; Guo, S. Cost and effect analysis of clinical pathway management in planned cesarean section. J. Qiqihar Med. Coll. 2018, 39, 1663–1664. (In Chinese) [Google Scholar]
- Yan, Y. Clinical effect of clinical pathway management in planned cesarean section. Int. Med. Health Guide 2012, 18, 566–568. (In Chinese) [Google Scholar]
- Yu, Y.H. Clinical analysis of 60 cases of the cesarean section of the cicatricial uterus. Matern. Child Health 2017, 28, 436. (In Chinese) [Google Scholar]
- Yu, S.S.; Wu, X.H.; Chen, Q.; Quan, Y.P. Application of clinical pathway in planned cesarean section. J. Nanjing Med. Univ. Soc. Sci. 2012, 12, 474–476. (In Chinese) [Google Scholar]
- Zhang, B.B.; Wang, L.Y.; Wang, C.; Qu, Z.D.; Wang, Y. Application of clinical pathway management in cesarean section. Res. Women Health Home Abroad 2015, 2, 99. (In Chinese) [Google Scholar]
- Zhang, H.H.; Li, J.; Gao, X.F. The effect of selective cesarean section in primary hospital. Shanxi Med. J. 2015, 44, 800–802. (In Chinese) [Google Scholar]
- Zhang, J.R.; Feng, J.L.; Li, W.X. Application of planned cesarean section clinical pathway in primary hospital. Hebei Med. 2012, 34, 2715–2716. (In Chinese) [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar]
- Liang, J.; Mu, Y.; Li, X.; Tang, W.; Wang, Y.; Liu, Z.; Huang, X.; Scherpbier, R.W.; Guo, S.; Li, M.; et al. Relaxation of the one child policy and trends in caesarean section rates and birth outcomes in China between 2012 and 2016: Observational study of nearly seven million health facility births. BMJ 2018, 360, k817. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.X.; Zhao, Y.Y.; Wang, Y.Q. Analysis of the characteristics of pregnancy and delivery before and after implementation of the two-child policy. Chin. Med. J. 2018, 131, 37–42. [Google Scholar] [CrossRef]
- Hellerstein, S.; Feldman, S.; Duan, T. Survey of obstetric care and cesarean delivery rates in Shanghai, China. Birth 2016, 43, 193–199. [Google Scholar] [CrossRef] [PubMed]
- He, X.Y.; Bundorf, M.K.; Gu, J.J.; Zhou, P.; Xue, D. Compliance with clinical pathways for inpatient care in Chinese public hospitals. BMC Health Serv. Res. 2015, 15, 459. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Bundorf, K.; Bai, F.; Tang, H.; Xue, D. Relationship between physician financial incentives and clinical pathway compliance: A cross-sectional study of 18 public hospitals in China. BMJ Open 2019, 9, e027540. [Google Scholar] [CrossRef] [PubMed]
- McLeod, R.S.; Aarts, M.A.; Chung, F.; Eskicioglu, C.; Forbes, S.S.; Conn, L.G.; McCluskey, S.; McKenzie, M.; Morningstar, B.; Nadler, A.; et al. Development of an enhanced recovery after surgery guideline and implementation strategy based on the knowledge-to-action cycle. Ann. Surg. 2015, 262, 1016–1025. [Google Scholar] [CrossRef]
- Medves, J.; Godfrey, C.; Turner, C.; Paterson, M.; Harrison, M.; MacKenzie, L.; Durando, P. Systematic review of practice guideline dissemination and implementation strategies for healthcare teams and team-based practice. Int. J. Evid. Based Healthc. 2010, 8, 79–89. [Google Scholar]
- Adedeji, A.R.; Tumbo, J.; Govender, I. Adherence of doctors to a clinical guideline for hypertension in Bojanala district, North-West Province, South Africa. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 776. [Google Scholar] [CrossRef][Green Version]
- Rotter, T.; Kinsman, L.; James, E.; Machotta, A.; Willis, J.; Snow, P.; Kugler, J. The effects of clinical pathways on professional practice, patient outcomes, length of stay, and hospital costs: Cochrane systematic review and meta-analysis. Eval. Health Prof. 2012, 35, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Marrie, T.J.; Lau, C.Y.; Wheeler, S.L.; Wong, C.J.; Vandervoort, M.K.; Feagan, B.G. A controlled trial of a critical pathway for the treatment of community-acquired pneumonia. CAPITAL Study Investigators. Community-Acquired Pneumonia Intervention Trial Assessing Levofloxacin. JAMA 2000, 283, 749–755. [Google Scholar] [CrossRef]
- Usui, K.; Kage, H.; Soda, M.; Noda, H.; Ishihara, T. Electronic clinical pathway for community acquired pneumonia (e-CP CAP). Nihon Kokyuki Gakkai Zasshi 2004, 42, 620–624. [Google Scholar]
- Yong-Mei, B.; De-Min, H.; Dong-Bo, W.; Qi-Zhi, M.; Yue-Da, P. Meta-analysis of the effect of the clinical pathway applied to patients with endoscopic sinus surgery in China. J. Otorhinolaryngol. Relat. Spec. 2019, 81, 159–170. [Google Scholar] [CrossRef]
- Woo, S.; Suh, C.H.; Eastham, J.A.; Zelefsky, M.J.; Morris, M.J.; Abida, W.; Scher, H.I.; Sidlow, R.; Becker, A.S.; Wibmer, A.G.; et al. Comparison of magnetic resonance imaging-stratified clinical pathways and systematic transrectal ultrasound-guided biopsy pathway for the detection of clinically significant prostate cancer: A systematic review and meta-analysis of randomized controlled trials. Eur. Urol. Oncol. 2019, 2, 605–616. [Google Scholar] [PubMed]
- Neuman, M.D.; Archan, S.; Karlawish, J.H.; Schwartz, J.S.; Fleisher, L.A. The relationship between short-term mortality and quality of care for hip fracture: A meta-analysis of clinical pathways for hip fracture. J. Am. Geriatr. Soc. 2009, 57, 2046–2054. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.M.; McNutt, R. A new strategy to improve quality: Rewarding actions rather than measures. JAMA 2009, 301, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Author | Publication Year | Study Period | Province | Study Design | No. of Participants | Risk of Bias |
|---|---|---|---|---|---|---|---|
| 1 | Chen XY [34] | 2009 | 2008 | Sichuan | RCT | 248 | Low |
| 2 | Duan WY [35] | 2012 | 2011 | Henan | CCT | 320 | High |
| 3 | Fang L [36] | 2009 | 2007–2008 | Hubei | CCT | 120 | High |
| 4 | Han XH [37] | 2013 | 2012–2013 | Xinjiang | RCT | 755 | Low |
| 5 | He QF [38] | 2005 | 2004–2005 | Guangdong | RCT | 100 | Low |
| 6 | Hu YL [39] | 2015 | 2013–2014 | Guangdong | RCT | 280 | Low |
| 7 | Hu JZ [40] | 2010 | 2009 | Guangdong | RCT | 320 | Low |
| 8 | Li DH [41] | 2012 | 2010–2011 | Hunan | RCT | 164 | Low |
| 9 | Li XH [42] | 2010 | 2010 | Jiangxi | CCT | 300 | High |
| 10 | Lin L [43] | 2011 | 2010 | Anhui | CCT | 67 | High |
| 11 | Liu L [44] | 2011 | 2010–2011 | Guangxi | RCT | 133 | Low |
| 12 | Luo JZ [45] | 2012 | 2011–2012 | Xinjiang | CCT | 212 | High |
| 13 | Qin XZ [46] | 2012 | 2010–2011 | Guangxi | CCT | 560 | High |
| 14 | Shao YQ [47] | 2010 | 2009–2010 | Shandong | RCT | 280 | Low |
| 15 | Sun Y [48] | 2012 | 2010–2011 | Guangdong | RCT | 330 | Low |
| 16 | Wang JL [49] | 2013 | 2012–2013 | Anhui | CCT | 100 | High |
| 17 | Wang Y [50] | 2013 | 2012 | Liaoning | CCT | 108 | High |
| 18 | Xin Y [51] | 2012 | 2009–2011 | Liaoning | RCT | 205 | Low |
| 19 | Xu PH [52] | 2018 | 2016–2017 | Anhui | RCT | 320 | Low |
| 20 | Yan Y [53] | 2012 | 2011 | Hunan | RCT | 226 | Low |
| 21 | Yu YH [54] | 2017 | 2015–2017 | Jiangsu | RCT | 60 | Low |
| 22 | Yu SS [55] | 2012 | 2010 | Jiangsu | CCT | 626 | High |
| 23 | Zhang BB [56] | 2015 | 2013–2014 | Liaoning | RCT | 1000 | Low |
| 24 | Zhang HH [57] | 2015 | 2009–2012 | Shanxi | CCT | 567 | High |
| 25 | Zhang JR [58] | 2012 | 2011 | Hebei | RCT | 360 | Low |
| Subgroup | Number of Studies | WMD | 95% CI | p-Value | Tests for Heterogeneity | p-Value for Interaction | ||
|---|---|---|---|---|---|---|---|---|
| p-Value (Q Statistic) | I2 (%) | |||||||
| LOS | 0.94 | |||||||
| RCT | 10 | −1.38 | −1.53 | −1.22 | <0.001 | <0.001 | 63.2 | |
| CCT | 8 | −1.37 | −1.54 | −1.21 | 0.08 | <0.001 | 45.4 | |
| DHC | 0.30 | |||||||
| RCT | 8 | −479.43 | −536.18 | −422.69 | 0.01 | <0.001 | 60.9 | |
| CCT | 5 | −520.46 | −573.09 | −467.83 | 0.16 | <0.001 | 38.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, D.; Zhang, C.; Shi, H. Effects of Clinical Pathways on Cesarean Sections in China: Length of Stay and Direct Hospitalization Cost Based on Meta-Analysis of Randomized Controlled Trials and Controlled Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 5918. https://doi.org/10.3390/ijerph18115918
Lin D, Zhang C, Shi H. Effects of Clinical Pathways on Cesarean Sections in China: Length of Stay and Direct Hospitalization Cost Based on Meta-Analysis of Randomized Controlled Trials and Controlled Clinical Trials. International Journal of Environmental Research and Public Health. 2021; 18(11):5918. https://doi.org/10.3390/ijerph18115918
Chicago/Turabian StyleLin, Dan, Chunyang Zhang, and Huijing Shi. 2021. "Effects of Clinical Pathways on Cesarean Sections in China: Length of Stay and Direct Hospitalization Cost Based on Meta-Analysis of Randomized Controlled Trials and Controlled Clinical Trials" International Journal of Environmental Research and Public Health 18, no. 11: 5918. https://doi.org/10.3390/ijerph18115918
APA StyleLin, D., Zhang, C., & Shi, H. (2021). Effects of Clinical Pathways on Cesarean Sections in China: Length of Stay and Direct Hospitalization Cost Based on Meta-Analysis of Randomized Controlled Trials and Controlled Clinical Trials. International Journal of Environmental Research and Public Health, 18(11), 5918. https://doi.org/10.3390/ijerph18115918