
Online Videos as a Source of Physiotherapy Exercise Tutorials for Patients with Lumbar Disc Herniation—A Quality Assessment

 , , ,
, , , 
Abstract
1. Introduction
2. Material and Methods
Statistical Analysis
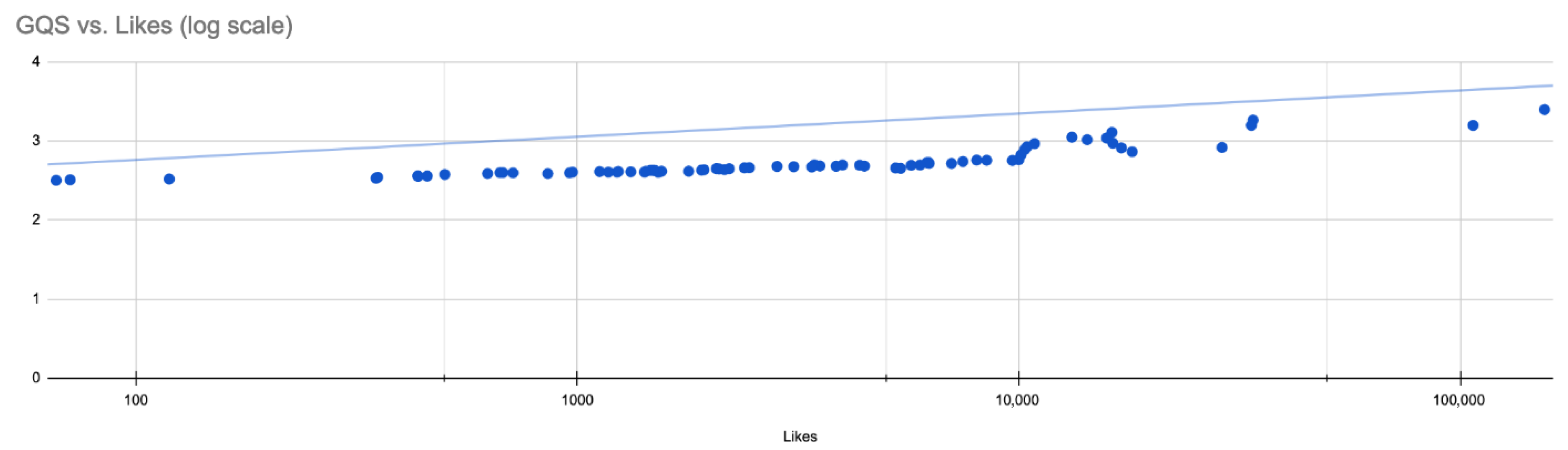
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GQS Rating. | Fleiss’ Kappa | p-Value | LB 95%CI | UB 95%CI |
|---|---|---|---|---|
| overall | 0.066 | 0.002 | 0.025 | 0.107 |
| 1 | 0.063 | 0.084 | −0.008 | 0.135 |
| 2 | 0.051 | 0.159 | −0.02 | 0.123 |
| 3 | 0.107 | 0.003 | 0.035 | 0.179 |
| 4 | 0.028 | 0.449 | −0.044 | 0.099 |
| 5 | 0.042 | 0.249 | −0.03 | 0.114 |
References
- Dieleman, J.L.; Baral, R.; Birger, M.; Bui, A.L.; Bulchis, A.; Chapin, A.; Hamavid, H.; Horst, C.; Johnson, E.K.; Joseph, J.; et al. US Spending on Personal Health Care and Public Health, 1996–2013. JAMA 2016, 316, 2627. [Google Scholar] [CrossRef]
- Geurts, J.W.; Willems, P.C.; Kallewaard, J.-W.; van Kleef, M.; Dirksen, C. The Impact of Chronic Discogenic Low Back Pain: Costs and Patients’ Burden. Pain Res. Manag. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Soin, A.; Benyamin, R.M.; Singh, V.; Falco, F.J.; Calodney, A.K.; Grami, V.; Hirsch, J.A. An Update of the Systematic Appraisal of the Accuracy and Utility of Discography in Chronic Spinal Pain. Pain Physician 2018, 21, 91–110. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Staats, P.S.; Nampiaparampil, D.E.; Hirsch, J.A. What Is the Role of Epidural Injections in the Treatment of Lumbar Discogenic Pain: A Systematic Review of Comparative Analysis with Fusion. Korean J. Pain 2015, 28, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Pampati, V.; Benyamin, R.M.; Boswell, M.V. Analysis of Efficacy Differences between Caudal and Lumbar Interlaminar Epidural Injections in Chronic Lumbar Axial Discogenic Pain: Local Anesthetic Alone vs. Local Combined with Steroids. Int. J. Med. Sci. 2015, 12, 214–222. [Google Scholar] [CrossRef]
- Martin, B.I.; Turner, J.A.; Mirza, S.K.; Lee, M.J.; Comstock, B.A.; Deyo, R.A. Trends in Health Care Expenditures, Utilization, and Health Status Among US Adults With Spine Problems, 1997–2006. Spine 2009, 34, 2077–2084. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.L. The State of US Health, 1990–2010: Burden of Diseases, Injuries, and Risk Factors. JAMA 2013, 310, 591. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Manchikanti, L.; Kaye, A.D.; Abd-Elsayed, A. Treatment of Discogenic Low Back Pain: Current Treatment Strategies and Future Options—A Literature Review. Curr. Pain Headache Rep. 2019, 23, 86. [Google Scholar] [CrossRef] [PubMed]
- Thackeray, A.; Fritz, J.M.; Lurie, J.D.; Zhao, W.; Weinstein, J.N. Nonsurgical Treatment Choices by Individuals with Lumbar Intervertebral Disc Herniation in the United States: Associations with Long-Term Outcomes. Am. J. Phys. Med. Rehabil. 2017, 96, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.M.; Andrade, N.S.; Neuman, B.J. Lumbar Disc Herniation. Curr. Rev. Musculoskelet. Med. 2017, 10, 507–516. [Google Scholar] [CrossRef]
- Martin, B.I.; Deyo, R.A.; Mirza, S.K.; Turner, J.A.; Comstock, B.A.; Hollingworth, W.; Sullivan, S.D. Expenditures and Health Status among Adults with Back and Neck Problems. JAMA 2008, 299, 656–664. [Google Scholar] [CrossRef]
- Andersson, G.B. Epidemiological Features of Chronic Low-Back Pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Al Qaraghli, M.I.; De Jesus, O. Lumbar Disc Herniation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Koes, B.W.; van Tulder, M.W.; Peul, W.C. Diagnosis and Treatment of Sciatica. BMJ 2007, 334, 1313–1317. [Google Scholar] [CrossRef] [PubMed]
- Gugliotta, M.; da Costa, B.R.; Dabis, E.; Theiler, R.; Jüni, P.; Reichenbach, S.; Landolt, H.; Hasler, P. Surgical versus Conservative Treatment for Lumbar Disc Herniation: A Prospective Cohort Study. BMJ Open 2016, 6, e012938. [Google Scholar] [CrossRef] [PubMed]
- Atlas, S.J.; Keller, R.B.; Wu, Y.A.; Deyo, R.A.; Singer, D.E. Long-Term Outcomes of Surgical and Nonsurgical Management of Sciatica Secondary to a Lumbar Disc Herniation: 10 Year Results from the Maine Lumbar Spine Study. Spine 2005, 30, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Skinner, J.S.; Hanscom, B.; Tosteson, A.N.A.; Herkowitz, H.; Fischgrund, J.; Cammisa, F.P.; Albert, T.; et al. Surgical vs Nonoperative Treatment for Lumbar Disk Herniation: The Spine Patient Outcomes Research Trial (SPORT) Observational Cohort. JAMA 2006, 296, 2451–2459. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.L.; Deyo, R.A.; Atlas, S.J.; Singer, D.E.; Chapin, A.; Keller, R.B. Assessing Health-Related Quality of Life in Patients with Sciatica. Spine 1995, 20, 1899–1908. [Google Scholar] [CrossRef]
- Atlas, S.J.; Deyo, R.A.; Keller, R.B.; Chapin, A.M.; Patrick, D.L.; Long, J.M.; Singer, D.E. The Maine Lumbar Spine Study, Part II. 1-Year Outcomes of Surgical and Nonsurgical Management of Sciatica. Spine 1996, 21, 1777–1786. [Google Scholar] [CrossRef]
- Wong, J.J.; Côté, P.; Sutton, D.A.; Randhawa, K.; Yu, H.; Varatharajan, S.; Goldgrub, R.; Nordin, M.; Gross, D.P.; Shearer, H.M.; et al. Clinical Practice Guidelines for the Noninvasive Management of Low Back Pain: A Systematic Review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain 2017, 21, 201–216. [Google Scholar] [CrossRef] [PubMed]
- Falvey, J.R.; Krafft, C.; Kornetti, D. The Essential Role of Home- and Community-Based Physical Therapists During the COVID-19 Pandemic. Phys. Ther. 2020, 100, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Minghelli, B.; Soares, A.; Guerreiro, A.; Ribeiro, A.; Cabrita, C.; Vitoria, C.; Nunes, C.; Martins, C.; Gomes, D.; Goulart, F.; et al. Physiotherapy Services in the Face of a Pandemic. Rev. Assoc. Med. Bras. 2020, 66, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Gitkind, A.I.; Levin, S.; Dohle, C.; Herbold, J.; Thomas, M.; Oh-Park, M.; Bartels, M.N. Redefining Pathways into Acute Rehabilitation during the COVID-19 Crisis. Pm R 2020, 12, 837–841. [Google Scholar] [CrossRef] [PubMed]
- Prvu Bettger, J.; Resnik, L.J. Telerehabilitation in the Age of COVID-19: An Opportunity for Learning Health System Research. Phys. Ther. 2020, 100, 1913–1916. [Google Scholar] [CrossRef] [PubMed]
- Springer, B.; Bechler, U.; Koller, U.; Windhager, R.; Waldstein, W. Online Videos Provide Poor Information Quality, Reliability, and Accuracy Regarding Rehabilitation and Return to Sport After Anterior Cruciate Ligament Reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 3037–3047. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.A.; Griffith, R.A.; Ng, J.J.; Reinert, S.E.; Friedmann, P.D.; Moulton, A.W. Patients’ Use of the Internet for Medical Information. J. Gen. Intern. Med. 2002, 17, 180–185. [Google Scholar] [CrossRef]
- Fox, S.; Rainie, L. E-Patients and the Online Health Care Revolution. Physician Exec. 2002, 28, 14–17. [Google Scholar]
- Starman, J.S.; Gettys, F.K.; Capo, J.A.; Fleischli, J.E.; Norton, H.J.; Karunakar, M.A. Quality and Content of Internet-Based Information for Ten Common Orthopaedic Sports Medicine Diagnoses. JBJS 2010, 92, 1612–1618. [Google Scholar] [CrossRef]
- MacLeod, M.G.; Hoppe, D.J.; Simunovic, N.; Bhandari, M.; Philippon, M.J.; Ayeni, O.R. YouTube As an Information Source for Femoroacetabular Impingement: A Systematic Review of Video Content. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 136–142. [Google Scholar] [CrossRef]
- Pew Research Centre. Social Media Usage: 2005–2015. Available online: https://www.pewresearch.org/internet/2015/10/08/social-networking-usage-2005-2015/ (accessed on 10 January 2021).
- Koller, U.; Waldstein, W.; Schatz, K.-D.; Windhager, R. YouTube Provides Irrelevant Information for the Diagnosis and Treatment of Hip Arthritis. Int. Orthop. 2016, 40, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, B.F.; Nacitarhan, V.; Koca, T.T.; Berk, E. YouTube as a Source of Patient Information for Ankylosing Spondylitis Exercises. Clin. Rheumatol. 2019, 38, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Madathil, K.C.; Rivera-Rodriguez, A.J.; Greenstein, J.S.; Gramopadhye, A.K. Healthcare Information on YouTube: A Systematic Review. Health Inform. J. 2015, 21, 173–194. [Google Scholar] [CrossRef]
- Lewis, S.P.; Heath, N.L.; Sornberger, M.J.; Arbuthnott, A.E. Helpful or Harmful? An Examination of Viewers’ Responses to Nonsuicidal Self-Injury Videos on YouTube. J. Adolesc. Health 2012, 51, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; Amritphale, A.; Sawhney, A.; Dubey, D.; Srivastav, N. Analysis of YouTube as a Source of Information for West Nile Virus Infection. Clin. Med. Res. 2014, 12, 129–132. [Google Scholar] [CrossRef]
- Bernard, A.; Langille, M.; Hughes, S.; Rose, C.; Leddin, D.; Veldhuyzen van Zanten, S. A Systematic Review of Patient Inflammatory Bowel Disease Information Resources on the World Wide Web. Am. J. Gastroenterol. 2007, 102, 2070–2077. [Google Scholar] [CrossRef]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An Instrument for Judging the Quality of Written Consumer Health Information on Treatment Choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Staunton, P.F.; Baker, J.F.; Green, J.; Devitt, A. Online Curves: A Quality Analysis of Scoliosis Videos on YouTube. Spine 2015, 40, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.; Geurts, J.; Valderrabano, V.; Hügle, T. Educational Quality of YouTube Videos on Knee Arthrocentesis. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 2013, 19, 373–376. [Google Scholar] [CrossRef]
- Ovenden, C.D.; Brooks, F.M. Anterior Cervical Discectomy and Fusion YouTube Videos as a Source of Patient Education. Asian Spine J. 2018, 12, 987–991. [Google Scholar] [CrossRef]
- Haldeman, S.; Nordin, M.; Tavares, P.; Mullerpatan, R.; Kopansky-Giles, D.; Setlhare, V.; Chou, R.; Hurwitz, E.; Treanor, C.; Hartvigsen, J.; et al. Distance Management of Spinal Disorders during the COVID-19 Pandemic and beyond: Evidence-Based Patient and Clinician Guides from the Global Spine Care Initiative (Preprint); JMIR Public Health and Surveillance: Toronto, ON, Canada, 2020. [Google Scholar]




| Median | Upper Quartile | Lower Quartile | |
|---|---|---|---|
| Views | 375,039 | 726,654 | 133,117 |
| Likes | 2962 | 8347 | 1232 |
| Dislikes | 153 | 332 | 55.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heisinger, S.; Huber, D.; Matzner, M.P.; Hasenoehrl, T.; Palma, S.; Sternik, J.; Trost, C.; Treiber, M.; Crevenna, R.; Grohs, J.G. Online Videos as a Source of Physiotherapy Exercise Tutorials for Patients with Lumbar Disc Herniation—A Quality Assessment. Int. J. Environ. Res. Public Health 2021, 18, 5815. https://doi.org/10.3390/ijerph18115815
Heisinger S, Huber D, Matzner MP, Hasenoehrl T, Palma S, Sternik J, Trost C, Treiber M, Crevenna R, Grohs JG. Online Videos as a Source of Physiotherapy Exercise Tutorials for Patients with Lumbar Disc Herniation—A Quality Assessment. International Journal of Environmental Research and Public Health. 2021; 18(11):5815. https://doi.org/10.3390/ijerph18115815
Chicago/Turabian StyleHeisinger, Stephan, Dominikus Huber, Michael Paul Matzner, Timothy Hasenoehrl, Stefano Palma, Julia Sternik, Carmen Trost, Michael Treiber, Richard Crevenna, and Josef Georg Grohs. 2021. "Online Videos as a Source of Physiotherapy Exercise Tutorials for Patients with Lumbar Disc Herniation—A Quality Assessment" International Journal of Environmental Research and Public Health 18, no. 11: 5815. https://doi.org/10.3390/ijerph18115815
APA StyleHeisinger, S., Huber, D., Matzner, M. P., Hasenoehrl, T., Palma, S., Sternik, J., Trost, C., Treiber, M., Crevenna, R., & Grohs, J. G. (2021). Online Videos as a Source of Physiotherapy Exercise Tutorials for Patients with Lumbar Disc Herniation—A Quality Assessment. International Journal of Environmental Research and Public Health, 18(11), 5815. https://doi.org/10.3390/ijerph18115815