
‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Settings
2.2. Participants of the Study
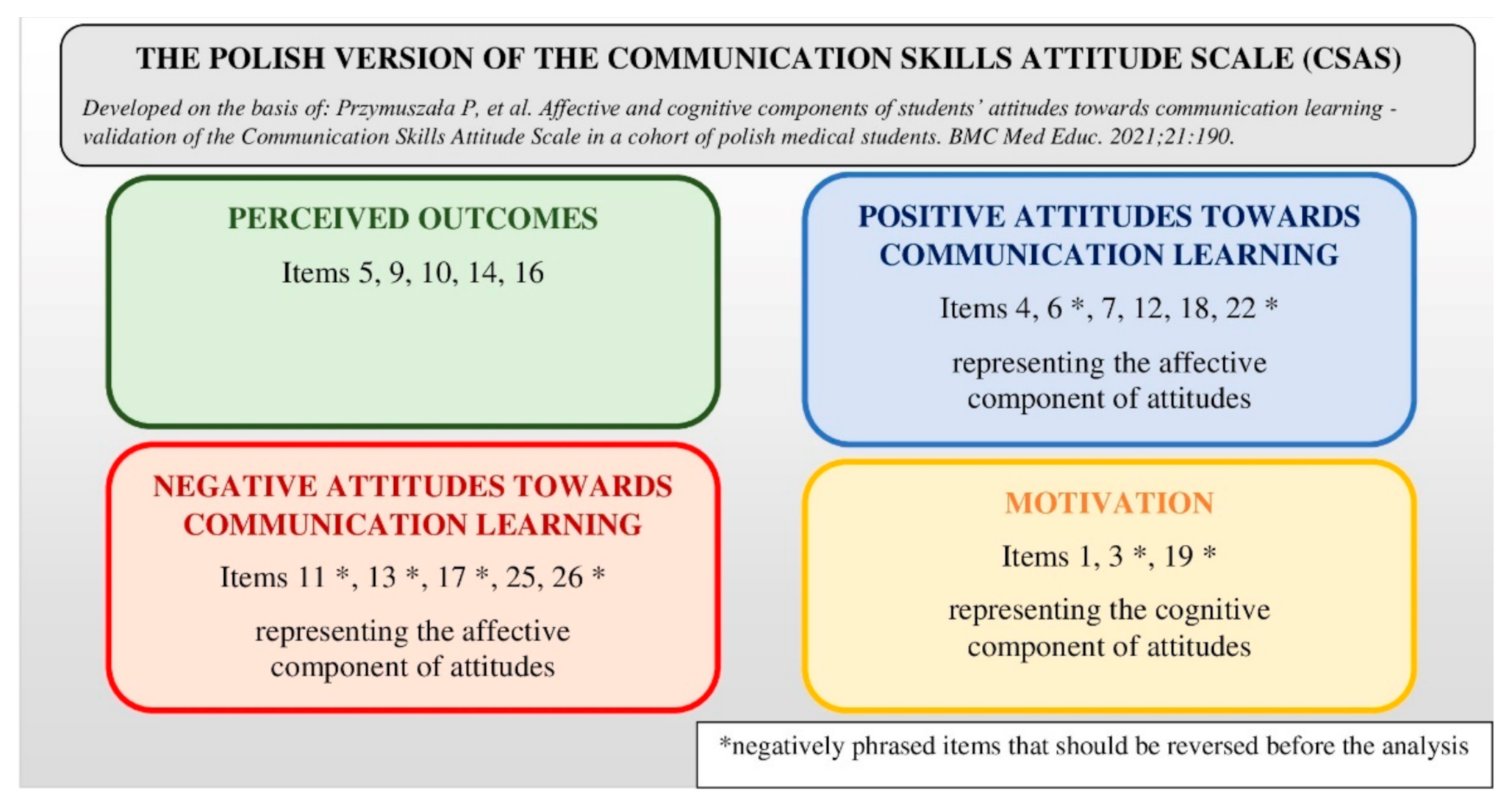
2.3. Research Tools
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Students’ Attitudes towards Communication Learning
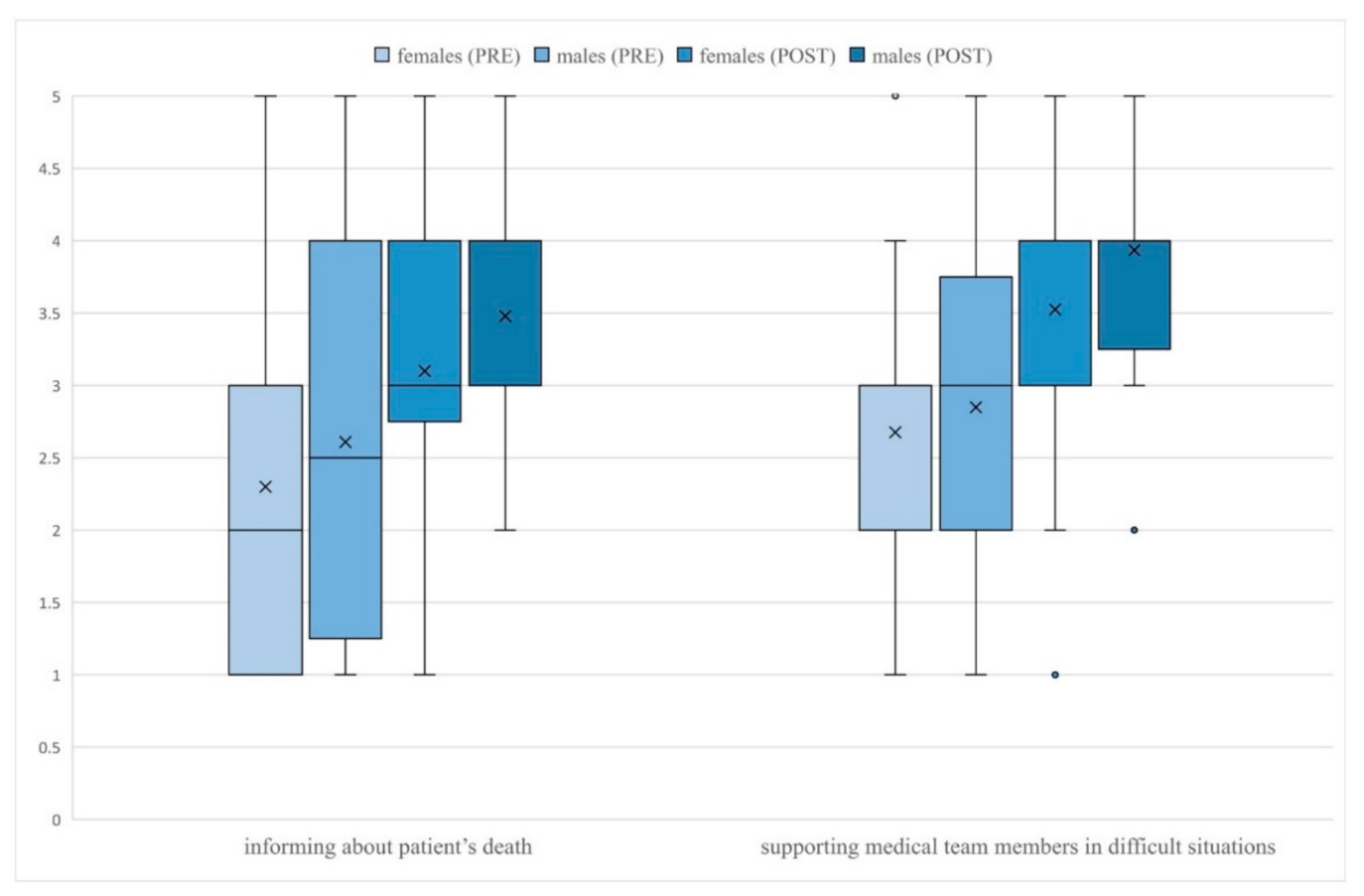
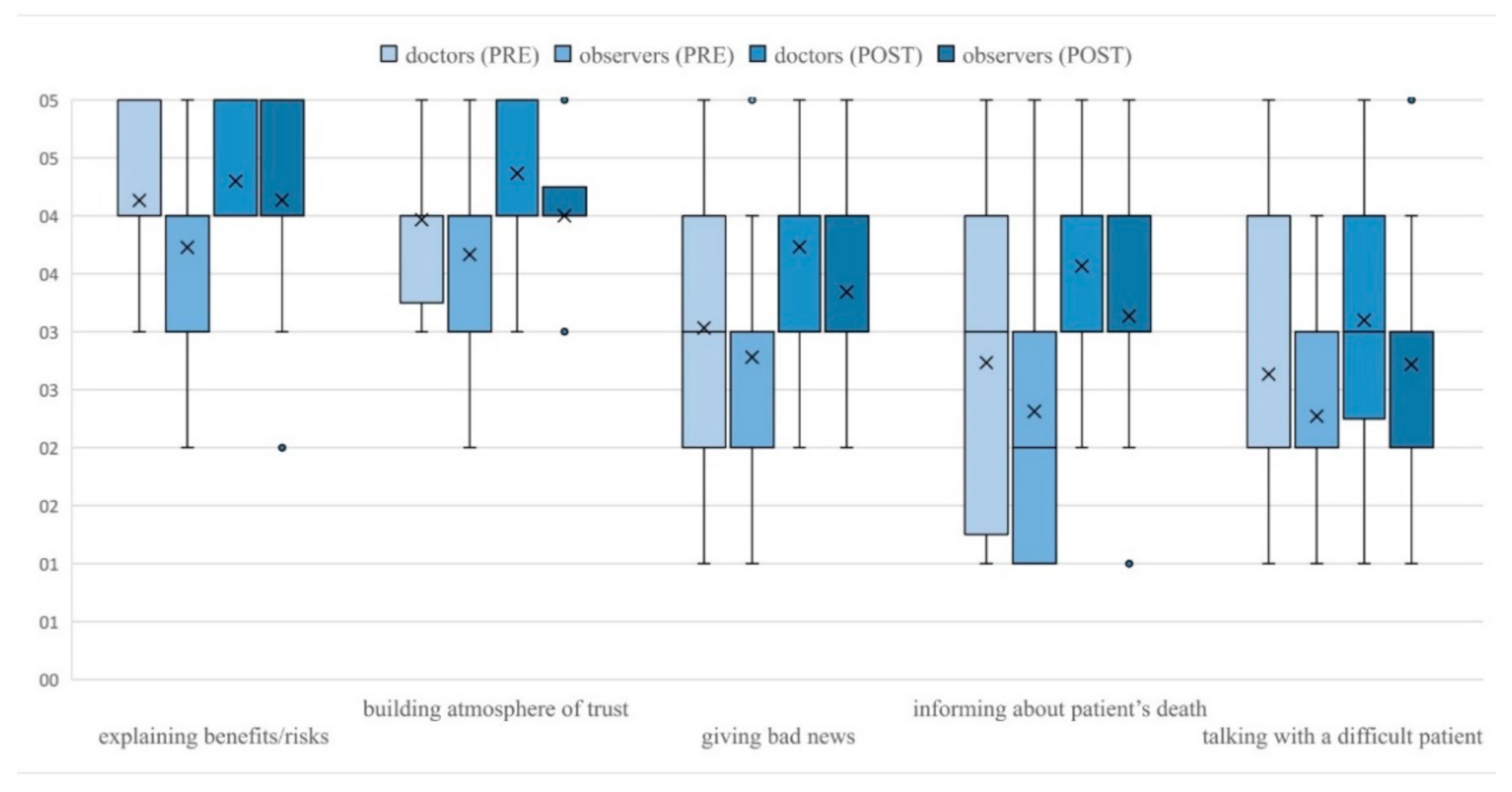
3.2. Students’ Self-Efficacy of Their Communication Skills before and after the Course
3.3. Students’ Opinions about the Course
“They allow us to face situations we didn’t have the opportunity to experience during classes in a hospital.”
“The possibility to test ourselves in safe conditions with difficult situations we may encounter in the future. Also, our reactions to them and the emotions they trigger.”
“The possibility to discuss the scenes afterward, having a sort of catharsis from emotions occurring during the scenes.”
“Too little time for every student to participate in their own case.”
“The awareness that this is a simulation makes them a little unreal.”
“During the course nothing, there should be more of them.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, R.; Dunn, S.; Byrnes, K.; Morris, R.; Heinrich, P.; Shaw, J. Doctors’ Stress Responses and Poor Communication Performance in Simulated Bad-News Consultations. Acad. Med. 2009, 84, 1595–1602. [Google Scholar] [CrossRef]
- Helft, P.R.; Petronio, S. Communication Pitfalls with Cancer Patients: “Hit-and-Run” Deliveries of Bad News. J. Am. Coll. Surg. 2007, 205, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Pascucci, R.C.; Weinstock, P.H.; O’Connor, B.E.; Fancy, K.M.; Meyer, E.C. Integrating Actors Into a Simulation Program. Simul. Healthc. J. Soc. Simul. Healthc. 2014, 9, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.K.; Pascucci, R.; Fancy, K.; Coleman, K.; Zurakowski, D.; Meyer, E.C. The educational value of improvisational actors to teach communication and relational skills: Perspectives of interprofessional learners, faculty, and actors. Patient Educ. Couns. 2014, 96, 381–388. [Google Scholar] [CrossRef]
- Quail, M.; Brundage, S.B.; Spitalnick, J.; Allen, P.J.; Beilby, A.J. Student self-reported communication skills, knowledge and confidence across standardised patient, virtual and traditional clinical learning environments. BMC Med. Educ. 2016, 16, 5775. [Google Scholar] [CrossRef] [PubMed]
- Beigzadeh, A.; Bahmanbijari, B.; Sharifpoor, E.; Rahimi, M. Standardized patients versus simulated patients in medical education: Are they the same or different. J. Emerg. Pract. Trauma 2015, 2, 25–28. [Google Scholar] [CrossRef]
- Cerbin Koczorowska, M.; Przymuszała, P.; Waszyk Nowaczyk, M.; Plewka, B.; Marciniak, R. The Need for Simulated Patient Method Implementation in Pharmaceutical Education in Poland. Indian J. Pharm. Educ. Res. 2020, 54, 875–880. [Google Scholar] [CrossRef]
- Chen, Y.C.; Kiersma, M.E.; Abdelmageed, A. Evaluation of student perceptions of standardized patient simulation on patient counseling confidence during introductory pharmacy practice experiences. Curr. Pharm. Teach. Learn. 2015, 7, 811–818. [Google Scholar] [CrossRef]
- Smithson, J.; Bellingan, M.; Glass, B.; Mills, J. Standardized patients in pharmacy education: An integrative literature review. Curr. Pharm. Teach. Learn. 2015, 7, 851–863. [Google Scholar] [CrossRef]
- Schlegel, C.; Woermann, U.; Rethans, J.J.; Van Der Vleuten, C. Validity evidence and reliability of a simulated patient feedback instrument. BMC Med. Educ. 2012, 12, 6. [Google Scholar] [CrossRef]
- Cleland, J.A.; Abe, K.; Rethans, J.J. The use of simulated patients in medical education: AMEE Guide No 42 1. Med. Teach. 2009, 31, 477–486. [Google Scholar] [CrossRef]
- Ludwig, A.B.; Raff, A.C.; Lin, J.; Schoenbaum, E. Group observed structured encounter (GOSCE) for third-year medical students improves self-assessment of clinical communication. Med. Teach. 2017, 39, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Konopasek, L.; Kelly, K.V.; Bylund, C.L.; Wenderoth, S.; Storey-Johnson, C. The Group Objective Structured Clinical Experience: Building communication skills in the clinical reasoning context. Patient Educ. Couns. 2014, 96, 79–85. [Google Scholar] [CrossRef]
- Sulaiman, N.D.; Shorbagi, S.I.; Abdalla, N.Y.; Daghistani, M.T.; Mahmoud, I.E.; Al-Moslih, A.M. Group OSCE (GOSCE) as a formative clinical assessment tool for pre-clerkship medical students at the University of Sharjah. J. Taibah Univ. Med. Sci. 2018, 13, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, C.; Roschlaub, S.; Harendza, S.; Keim, R.; Scherer, M. Medical students’ communication skills in clinical education: Results from a cohort study. Patient Educ. Couns. 2017, 100, 1874–1881. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Vergare, M.J.; Maxwell, K.; Brainard, G.; Herrine, S.K.; Isenberg, G.A.; Veloski, J.; Gonnella, J.S. The Devil is in the Third Year: A Longitudinal Study of Erosion of Empathy in Medical School. Acad. Med. 2009, 84, 1182–1191. [Google Scholar] [CrossRef]
- Neumann, M.; Edelhäuser, F.; Tauschel, D.; Fischer, M.R.; Wirtz, M.; Woopen, C.; Haramati, A.; Scheffer, C. Empathy Decline and Its Reasons: A Systematic Review of Studies With Medical Students and Residents. Acad. Med. 2011, 86, 996–1009. [Google Scholar] [CrossRef]
- Cleland, J.; Foster, K.; Moffat, M. Undergraduate students’ attitudes to communication skills learning differ depending on year of study and gender. Med. Teach. 2005, 27, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.; Sheard, C. The relationship between medical students’ attitudes towards communication skills learning and their demographic and education-related characteristics. Med. Educ. 2002, 36, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Witt, M.M.; Jankowska, K.A. Breaking bad news in genetic counseling—problems and communication tools. J. Appl. Genet. 2018, 59, 449–452. [Google Scholar] [CrossRef]
- Pendleton, D.; Schofield, T.; Tate, P. The Consultation: An Approach to Learning and Teaching; Oxford University Press: Oxford, UK, 1984. [Google Scholar]
- Przymuszała, P.; Cerbin-Koczorowska, M.; Marciniak-Stępak, P.; Zielińska-Tomczak, Ł.; Piszczek, M.; Jasiński, J.; Marciniak, R. Affective and cognitive components of students’ attitudes towards communication learning—validation of the Communication Skills Attitude Scale in a cohort of polish medical students. BMC Med. Educ. 2021, 21, 190. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.; Sheard, C.; Davies, S. The development of a scale to measure medical students’ attitudes towards communication skills learning: The Communication Skills Attitude Scale (CSAS). Med. Educ. 2002, 36, 141–147. [Google Scholar] [CrossRef]
- British Educational Research Association (BERA). Ethical Guidelines for Educational Research, 4th ed.; BERA: London, UK, 2018. [Google Scholar]
- Wright, K.B.; Bylund, C.; Ware, J.; Parker, P.; Query, J.L.; Baile, W. Medical Student Attitudes Toward Communication Skills Training and Knowledge of Appropriate Provider-Patient Communication: A Comparison of First-Year and Fourth-Year Medical Students. Med. Educ. Online 2006, 11, 4594. [Google Scholar] [CrossRef]
- Rees, C.E.; Sheard, C.E.; McPherson, A.C. A qualitative study to explore undergraduate medical students’ attitudes towards communication skills learning. Med. Teach. 2002, 24, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Bylund, C.L.; Eddington, J.; Gueguen, J.A.; Kissane, D.W. Discussing prognosis in an oncology setting: Initial evaluation of a communication skills training module. Psychooncology 2010, 19, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.; Park, K.H.; Park, S.Y. Verbal communication of students with high patient–physician interaction scores in a clinical performance examination assessed by standardized patients. Korean J. Med. Educ. 2017, 29, 241–251. [Google Scholar] [CrossRef]
- Liew, S.-C.; Dutta, S.; Sidhu, J.K.; De-Alwis, R.; Chen, N.; Sow, C.-F.; Barua, A. Assessors for communication skills: SPs or healthcare professionals? Med. Teach. 2014, 36, 626–631. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subscale of the Polish Version of CSAS 1 | n | Mean (SD) | p-Value 2 | ||
|---|---|---|---|---|---|
| PRE | POST | ||||
| Perceived outcomes | Total | 126 | 4.06 (0.66) | 4.28 (0.73) | <0.001 |
| Females | 80 | 4.14 (0.63) | 4.32 (0.63) | <0.001 | |
| Males | 46 | 3.93 (0.71) | 4.23 (0.89) | 0.002 | |
| Doctors | 30 | 4.13 (0.72) | 4.42 (0.61) | 0.004 | |
| Observers | 96 | 4.04 (0.65) | 4.24 (0.76) | <0.001 | |
| Positive Attitudes Towards Communication Learning | Total | 126 | 3.40 (0.63) | 3.60 (0.65) | <0.001 |
| Females | 80 | 3.39 (0.63) | 3.55 (0.62) | 0.004 | |
| Males | 46 | 3.41 (0.63) | 3.68 (0.70) | <0.001 | |
| Doctors | 30 | 3.56 (0.61) | 3.78 (0.58) | 0.004 | |
| Observers | 96 | 3.35 (0.63) | 3.54 (0.66) | <0.001 | |
| Negative Attitudes Towards Communication Learning | Total | 126 | 3.93 (0.50) | 4.14 (0.54) | <0.001 |
| Females | 80 | 3.94 (0.49) | 4.14 (0.57) | <0.001 | |
| Males | 46 | 3.90 (0.52) | 4.14 (0.50) | <0.001 | |
| Doctors | 30 | 3.89 (0.54) | 4.07 (0.55) | 0.019 | |
| Observers | 96 | 3.94 (0.49) | 4.16 (0.54) | <0.001 | |
| Motivation | Total | 126 | 3.49 (0.81) | 3.38 (0.88) | 0.104 |
| Females | 80 | 3.57 (0.75) | 3.40 (0.80) | 0.023 | |
| Males | 46 | 3.36 (0.89) | 3.34 (1.02) | 0.967 | |
| Doctors | 30 | 3.58 (0.84) | 3.30 (0.84) | 0.088 | |
| Observers | 96 | 3.47 (0.80) | 3.40 (0.90) | 0.309 | |
| Students’ Self-Efficacy Ratings before and after the Course (1 = Very Poor; 5 = Very Good) | n | Mean (SD) | M | Q1 | Q3 | p-Value 1 | |
|---|---|---|---|---|---|---|---|
| verbal communication | PRE | 126 | 3.75 (0.78) | 4 | 3 | 4 | 0.014 |
| POST | 126 | 3.92 (0.67) | 4 | 4 | 4 | ||
| non-verbal communication | PRE | 126 | 3.51 (0.86) | 4 | 3 | 4 | <0.001 |
| POST | 126 | 3.75 (0.76) | 4 | 3 | 4 | ||
| talking with an adult patient | PRE | 126 | 3.95 (0.65) | 4 | 4 | 4 | 0.066 |
| POST | 125 | 4.05 (0.62) | 4 | 4 | 4 | ||
| using language understandable to patients | PRE | 125 | 3.83 (0.91) | 4 | 3 | 4 | 0.076 |
| POST | 126 | 3.98 (0.77) | 4 | 3 | 5 | ||
| identifying patient’s needs, expectations | PRE | 126 | 3.52 (0.81) | 4 | 3 | 4 | <0.001 |
| POST | 126 | 3.80 (0.76) | 4 | 3 | 4 | ||
| meeting patient’s needs, expectations | PRE | 126 | 3.65 (0.74) | 4 | 3 | 4 | 0.017 |
| POST | 126 | 3.83 (0.76) | 4 | 3 | 4 | ||
| identifying the patient’s emotions | PRE | 126 | 4.00 (0.84) | 4 | 4 | 5 | 0.043 |
| POST | 126 | 4.16 (0.71) | 4 | 4 | 5 | ||
| adequately reacting to patient’s emotions | PRE | 126 | 3.36 (0.92) | 3 | 3 | 4 | 0.005 |
| POST | 124 | 3.63 (0.80) | 4 | 3 | 4 | ||
| adjusting the conversation to patient’s capabilities and emotional state | PRE | 125 | 3.51 (0.95) | 3 | 3 | 4 | <0.001 |
| POST | 126 | 3.93 (0.76) | 4 | 3 | 4 | ||
| verifying whether the patient understood provided information | PRE | 126 | 3.60 (0.87) | 4 | 3 | 4 | <0.001 |
| POST | 126 | 4.15 (0.74) | 4 | 4 | 5 | ||
| showing patient respect and empathy | PRE | 126 | 4.29 (0.76) | 4 | 4 | 5 | 0.002 |
| POST | 126 | 4.48 (0.56) | 5 | 4 | 5 | ||
| obtaining informed consent from patients | PRE | 126 | 4.02 (0.75) | 4 | 4 | 4 | 0.005 |
| POST | 126 | 4.24 (0.66) | 4 | 4 | 5 | ||
| explaining benefits and risks of a given procedure | PRE | 126 | 3.83 (0.75) | 4 | 3 | 4 | <0.001 |
| POST | 126 | 4.17 (0.69) | 4 | 4 | 5 | ||
| building the atmosphere of trust | PRE | 126 | 3.74 (0.77) | 4 | 3 | 4 | <0.001 |
| POST | 126 | 4.09 (0.73) | 4 | 4 | 5 | ||
| giving bad news to patients or their family | PRE | 126 | 2.84 (1.06) | 3 | 2 | 4 | <0.001 |
| POST | 126 | 3.44 (0.85) | 4 | 3 | 4 | ||
| informing the family about the patient’s death | PRE | 126 | 2.41 (1.15) | 2 | 1 | 3 | <0.001 |
| POST | 126 | 3.24 (0.87) | 3 | 3 | 4 | ||
| talking with a difficult, demanding patient | PRE | 126 | 2.36 (1.02) | 2 | 2 | 3 | <0.001 |
| POST | 126 | 2.81 (0.90) | 3 | 2 | 3 | ||
| supporting members of the medical team in difficult situations | PRE | 126 | 2.74 (1.02) | 3 | 2 | 3 | <0.001 |
| POST | 126 | 3.67 (0.88) | 4 | 3 | 4 | ||
| Rated Aspect of the Course (1 = Very Poor; 5 = Very Good) | n | Mean (SD) | M | Q1 | Q3 | Good or Very Good |
|---|---|---|---|---|---|---|
| General impression from the course | 126 | 4.53 (0.69) | 5 | 4 | 5 | 92.86% |
| Usefulness in communication skills learning | 126 | 4.56 (0.72) | 5 | 4 | 5 | 92.06% |
| Atmosphere during the course | 126 | 4.78 (0.52) | 5 | 5 | 5 | 98.41% |
| Teachers conducting the course | 126 | 4.83 (0.39) | 5 | 5 | 5 | 99.21% |
| The way SPs portrayed their roles | 126 | 4.69 (0.58) | 5 | 4 | 5 | 96.83% |
| Layout and equipment of the consultation room | 126 | 4.71 (0.56) | 5 | 5 | 5 | 94.44% |
| Scenarios used during the course | 126 | 4.62 (0.62) | 5 | 4 | 5 | 92.86% |
| Observing other students | 126 | 4.22 (1.10) | 5 | 4 | 5 | 77.78% |
| Feedback received from teachers | 126 | 4.78 (0.49) | 5 | 5 | 5 | 96.83% |
| Feedback received from SPs | 126 | 4.52 (0.70) | 5 | 4 | 5 | 91.27% |
| Feedback received from other students | 126 | 4.41 (0.81) | 5 | 4 | 5 | 88.89% |
| Own engagement during the course | 126 | 4.29 (0.76) | 4 | 4 | 5 | 87.30% |
| Engagement of other students during the course | 126 | 4.25 (0.69) | 4 | 4 | 5 | 88.89% |
| Statement Describing the Course (1 = Definitely Disagree; 5 = Definitely Agree) | n | Mean (SD) | M | Q1 | Q3 | Agree or Definitely Agree |
|---|---|---|---|---|---|---|
| Classes with simulated patients are a good idea and should be organized more often. | 126 | 4.53 (0.81) | 5 | 4 | 5 | 89.68% |
| My communication skills improved after the course with simulated patients. | 126 | 4.25 (0.83) | 4 | 4 | 5 | 84.13% |
| The knowledge and skills from the course will be useful in my future professional carrier. | 125 | 4.52 (0.74) | 5 | 4 | 5 | 91.20% |
| After the course, it will be easier for me to talk with real patients. | 126 | 4.37 (0.81) | 5 | 4 | 5 | 86.51% |
| After the course, I have more appreciation for the significance of communication skills in the physician’s profession. | 126 | 4.32 (0.93) | 5 | 4 | 5 | 80.95% |
| Simulated patients were well-prepared and credible while playing their roles. | 126 | 4.63 (0.57) | 5 | 4 | 5 | 95.24% |
| The course with simulated patients constituted an interesting experience for me. | 126 | 4.52 (0.73) | 5 | 4 | 5 | 92.86% |
| Scenarios involved situations that can happen to me in my future work. | 126 | 4.63 (0.60) | 5 | 4 | 5 | 97.62% |
| Thanks to observing other students, I can better see my earlier mistakes. | 126 | 4.12 (0.92) | 4 | 4 | 5 | 78.57% |
| I think that I gained a lot as a result of participating in the course. | 124 | 4.42 (0.73) | 5 | 4 | 5 | 88.71% |
| I would willingly participate in a similar course in the future. | 126 | 4.44 (0.94) | 5 | 4 | 5 | 86.51% |
| Statement Describing the Course (1 = Definitely Disagree; 5 = Definitely Agree) | n | Mean (SD) | M | Q1 | Q3 | Agree or Definitely Agree |
|---|---|---|---|---|---|---|
| During the course, I had the impression that I was talking with real patients. | 30 | 4.30 (0.78) | 4.5 | 4 | 5 | 80.00% |
| Scenarios realized during the course were too easy and did not constitute any challenge for me. | 30 | 1.90 (0.75) | 2 | 1 | 2 | 3.33% |
| Talking with the simulated patient, I was feeling like a real doctor. | 30 | 4.03 (0.80) | 4 | 4 | 5 | 76.67% |
| During the course, I felt the motivation to do the best I can to help the patient. | 30 | 4.63 (0.55) | 5 | 4 | 5 | 96.67% |
| The possibility to observe other students constituted an additional occasion to learn. | 30 | 4.40 (0.84) | 5 | 4 | 5 | 90.00% |
| The presence of other students as observers was not a problem for me. | 30 | 3.93 (1.12) | 4 | 3.25 | 5 | 73.33% |
| The presence of other students was troublesome and distracting. | 30 | 2.23 (1.17) | 2 | 1 | 3 | 23.33% |
| The feedback from simulated patients and other students made me realize things I did not notice before. | 30 | 4.20 (0.87) | 4 | 4 | 5 | 76.67% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Przymuszała, P.; Marciniak-Stępak, P.; Cerbin-Koczorowska, M.; Borowczyk, M.; Cieślak, K.; Szlanga, L.; Zielińska-Tomczak, Ł.; Marciniak, R. ‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students. Int. J. Environ. Res. Public Health 2021, 18, 5772. https://doi.org/10.3390/ijerph18115772
Przymuszała P, Marciniak-Stępak P, Cerbin-Koczorowska M, Borowczyk M, Cieślak K, Szlanga L, Zielińska-Tomczak Ł, Marciniak R. ‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students. International Journal of Environmental Research and Public Health. 2021; 18(11):5772. https://doi.org/10.3390/ijerph18115772
Chicago/Turabian StylePrzymuszała, Piotr, Patrycja Marciniak-Stępak, Magdalena Cerbin-Koczorowska, Martyna Borowczyk, Katarzyna Cieślak, Lidia Szlanga, Łucja Zielińska-Tomczak, and Ryszard Marciniak. 2021. "‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students" International Journal of Environmental Research and Public Health 18, no. 11: 5772. https://doi.org/10.3390/ijerph18115772
APA StylePrzymuszała, P., Marciniak-Stępak, P., Cerbin-Koczorowska, M., Borowczyk, M., Cieślak, K., Szlanga, L., Zielińska-Tomczak, Ł., & Marciniak, R. (2021). ‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students. International Journal of Environmental Research and Public Health, 18(11), 5772. https://doi.org/10.3390/ijerph18115772