
Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Sociodemographic Measures
2.2.2. Mental Well-Being Symptoms
2.2.3. Mental Illness Symptoms
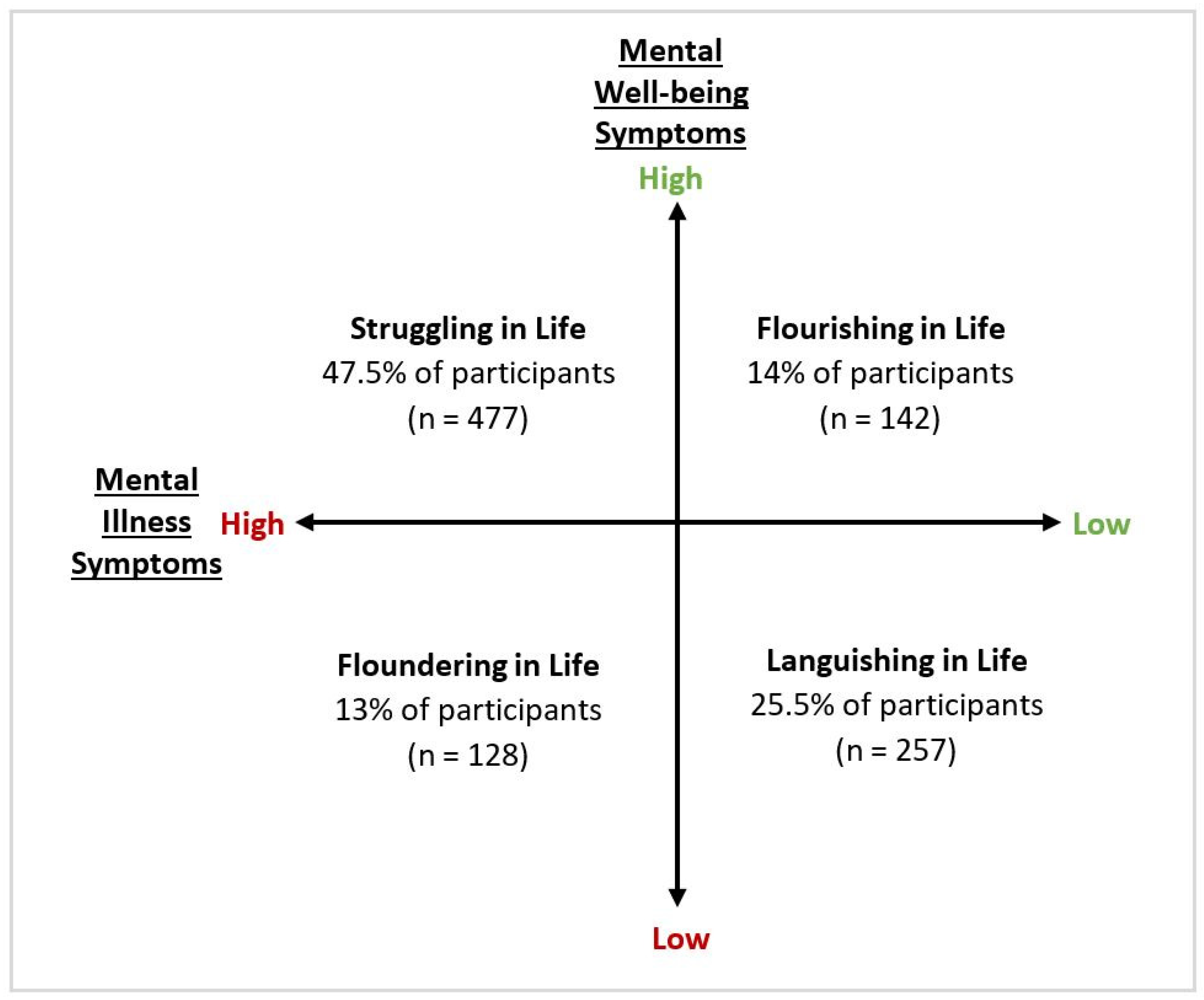
2.2.4. Complete Mental Health States
2.2.5. Employment and Financial Variables
2.2.6. Screen Time Variables
2.2.7. Nature Variables
2.2.8. Other Psychological Constructs
2.3. Procedure
2.4. Context
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Main Analysis
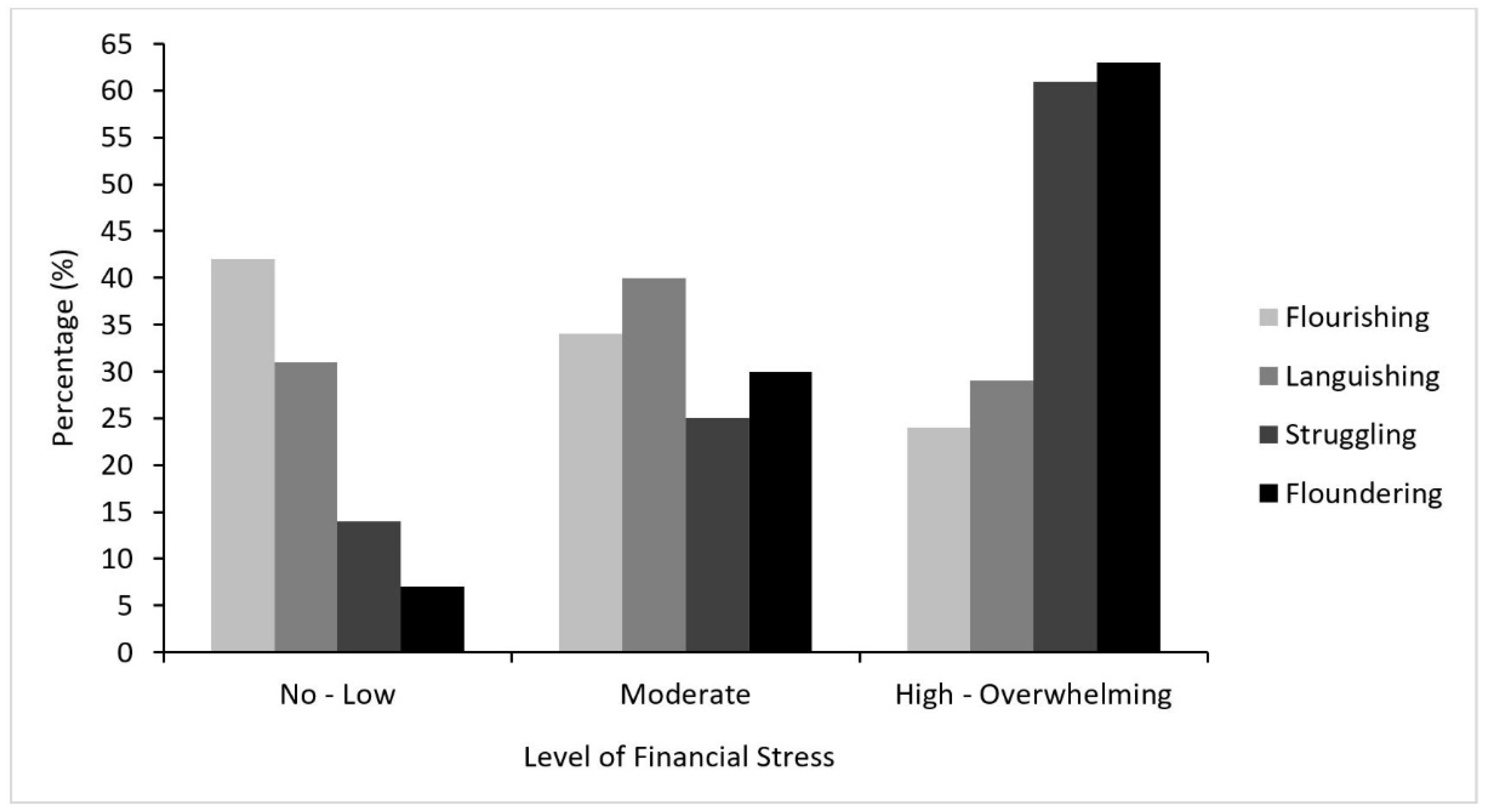
3.2.1. The Role of Living Arrangement, Employment Precarity and Financial Stress
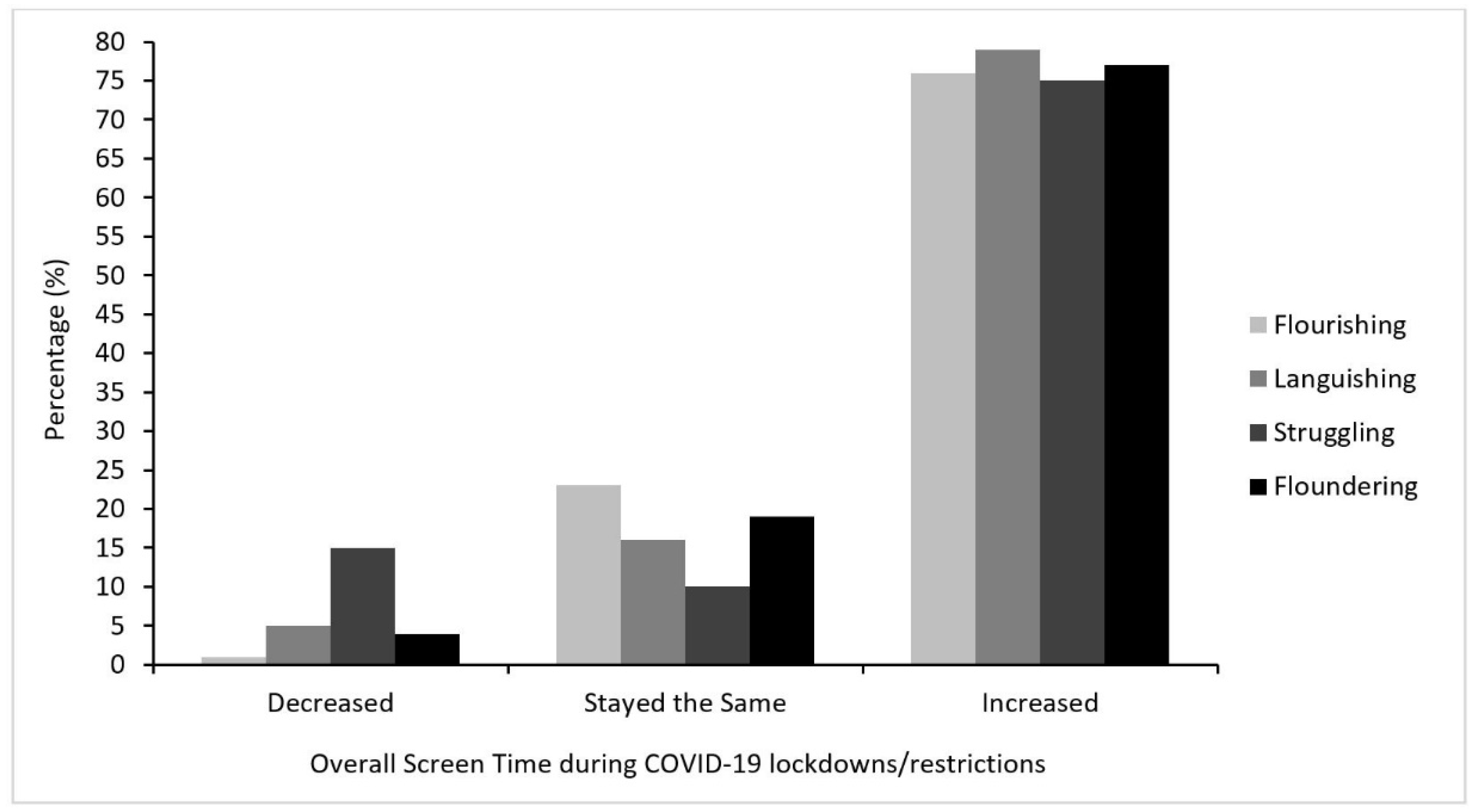
3.2.2. The Role of Screen Time
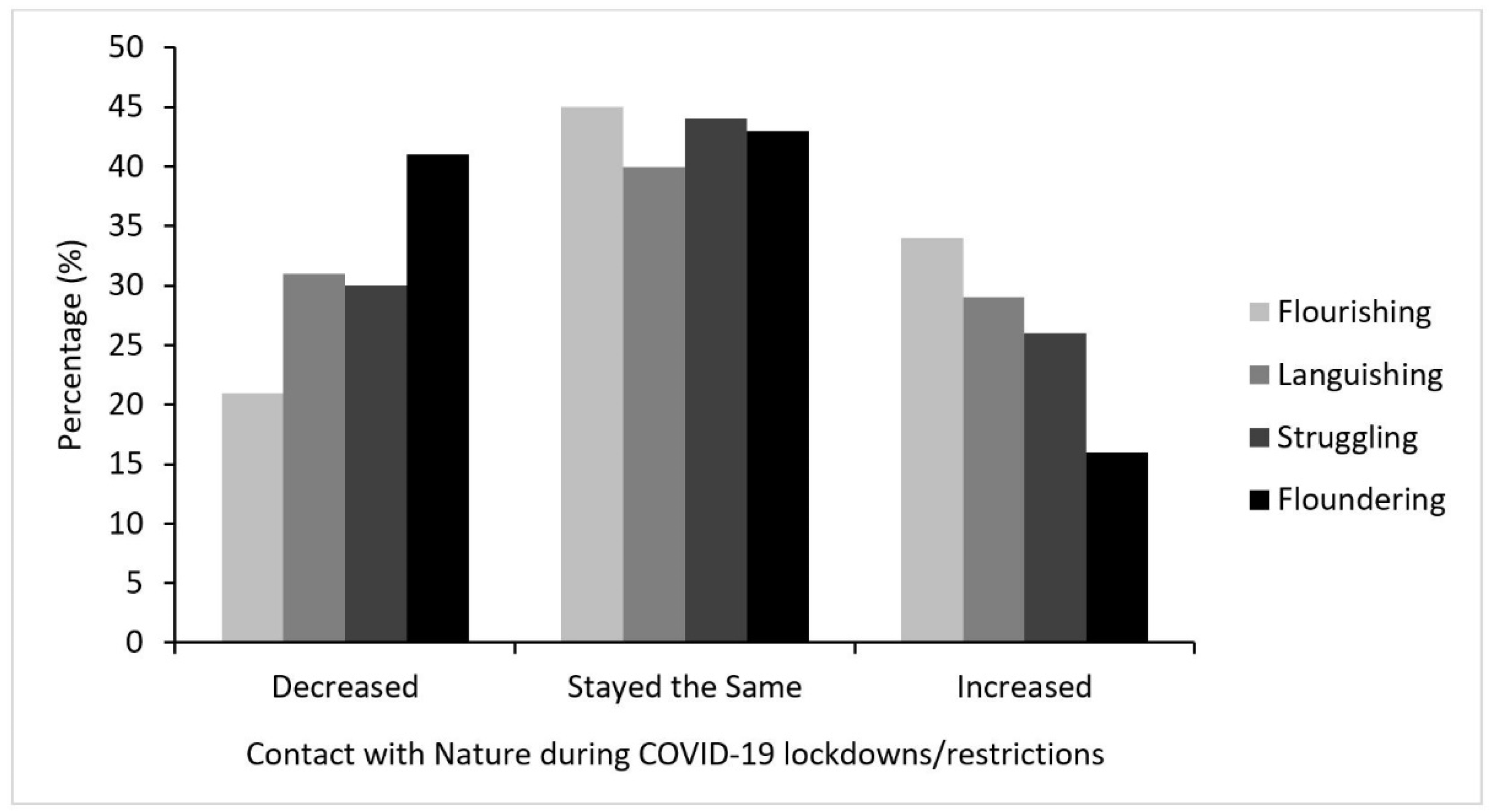
3.2.3. The Role of Nature
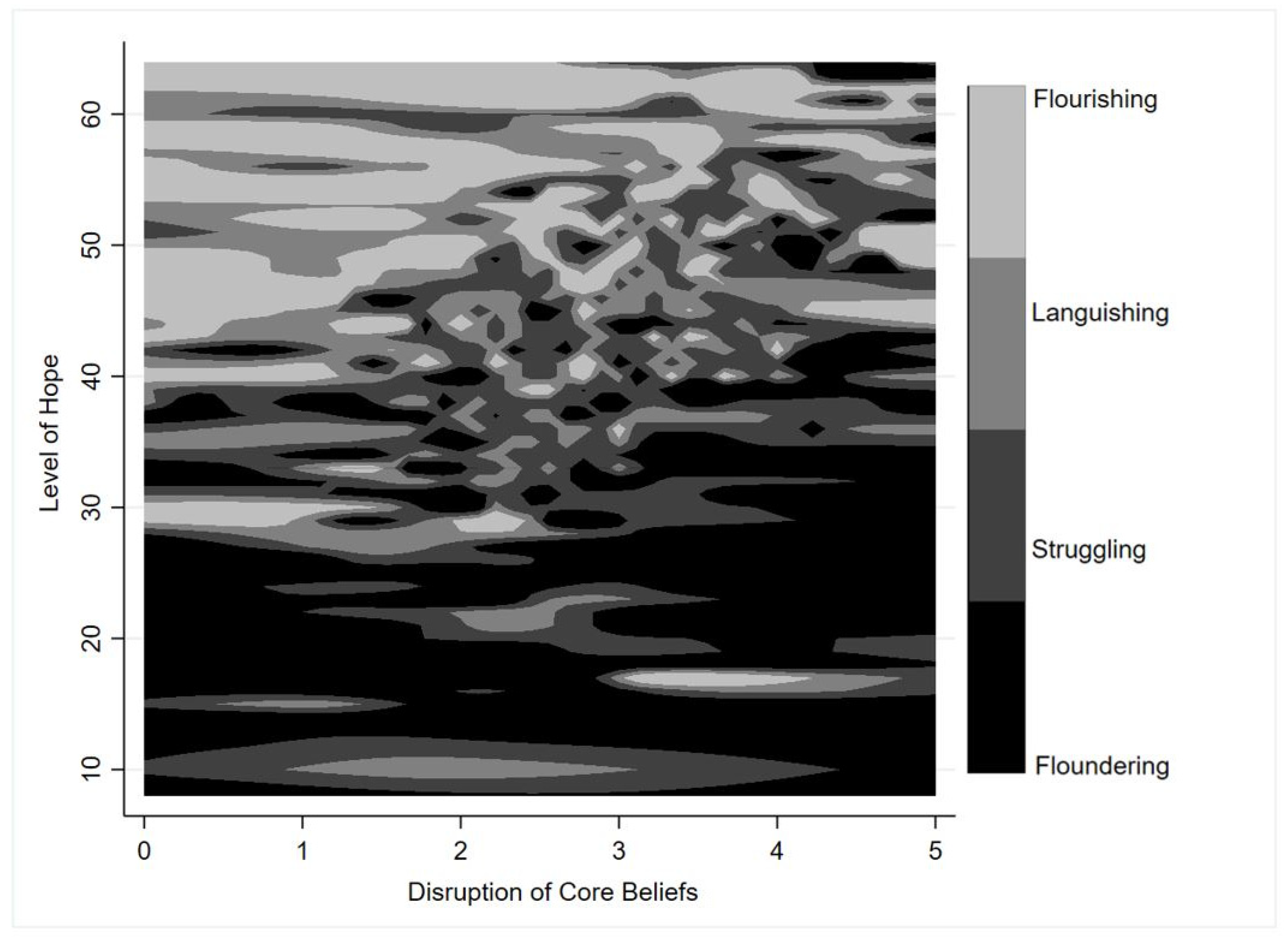
3.2.4. The Role of Other Psychological Constructs
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Government. COVID-19: A Chronology of State and Territory Government Announcements (Up Until 30 June 2020). Available online: https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/rp2021/Chronologies/COVID-19StateTerritoryGovernmentAnnouncements (accessed on 11 March 2021).
- Tan, E.J.; Meyer, D.; Neill, E.; Phillipou, A.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Considerations for assessing the impact of the COVID-19 pandemic on mental health in Australia. Aust. N. Z. J. Psychiatry 2020, 54, 1067–1071. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef]
- Campion, J.; Javed, A.; Sartorius, N.; Marmot, M. Addressing the public mental health challenge of COVID-19. Lancet Psychiatry 2020, 7, 657–659. [Google Scholar] [CrossRef]
- Choi, K.R.; Heilemann, M.V.; Fauer, A.; Mead, M. A Second Pandemic: Mental Health Spillover From the Novel Coronavirus (COVID-19). J. Am. Psychiatr. Nurses Assoc. 2020, 26, 340–343. [Google Scholar] [CrossRef]
- Shakespeare-Finch, J.; Bowen-Salter, H.; Cashin, M.; Badawi, A.; Wells, R.; Rosenbaum, S.; Steel, Z. COVID-19: An Australian Perspective. J. Loss Trauma 2020, 25, 662–672. [Google Scholar] [CrossRef]
- Lifeline Australia. Lifeline Media Releases. Available online: https://www.lifeline.org.au/resources/news-and-media-releases/media-releases/ (accessed on 2 April 2021).
- AIHW. Mental Health Impact of COVID-19; AIHW: Canberra, Australia, 2020.
- Lenz, B. The Transition From Adolescence to Young Adulthood: A Theoretical Perspective. J. Sch. Nurs. 2001, 17, 300–306. [Google Scholar] [CrossRef]
- Scales, P.C.; Benson, P.L.; Oesterle, S.; Hill, K.G.; Hawkins, J.D.; Pashak, T.J. The dimensions of successful young adult development: A conceptual and measurement framework. Appl. Dev. Sci. 2016, 20, 150–174. [Google Scholar] [CrossRef]
- Vancea, M.; Utzet, M. How unemployment and precarious employment affect the health of young people: A scoping study on social determinants. Scand. J. Public Health 2016, 45, 73–84. [Google Scholar] [CrossRef]
- Chesters, J.; Cuervo, H. Adjusting to new employment landscapes: Consequences of precarious employment for young Australians. Econ. Labour Relat. Rev. 2019, 30, 222–240. [Google Scholar] [CrossRef]
- Canivet, C.; Bodin, T.; Emmelin, M.; Toivanen, S.; Moghaddassi, M.; Östergren, P.-O. Precarious employment is a risk factor for poor mental health in young individuals in Sweden: A cohort study with multiple follow-ups. BMC Public Health 2016, 16, 687. [Google Scholar] [CrossRef]
- Fisher, J.R.; Tran, T.D.; Hammarberg, K.; Sastry, J.; Nguyen, H.; Rowe, H.; Popplestone, S.; Stocker, R.; Stubber, C.; Kirkman, M. Mental health of people in Australia in the first month of COVID-19 restrictions: A national survey. Med. J. Aust. 2020, 213, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Bleidorn, W.; Schwaba, T. Prsonality development in emerging adulthood. In Personality Development Across the Lifespan; Specht, J., Ed.; Academic Press Elsevier: Cambridge, MA, USA, 2017. [Google Scholar]
- Fingerman, K.L. Millennials and Their Parents: Implications of the New Young Adulthood for Midlife Adults. Innov. Aging 2017, 1. [Google Scholar] [CrossRef] [PubMed]
- Browning, M.; Larson, L.; Sharaievska, I.; Rigolon, A.; McAnirlin, O.; Mullenbach, L.; Cloutier, S.; Vu, T.; Thomsen, J.; Reigner, N.; et al. Psychological impacts from COVID-19 among university students: Risk factors across seven states in the United States. PLoS ONE 2021. [Google Scholar] [CrossRef] [PubMed]
- Eden, A.L.; Johnson, B.K.; Reinecke, L.; Grady, S.M. Media for Coping During COVID-19 Social Distancing: Stress, Anxiety, and Psychological Well-Being. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Lisitsa, E.; Benjamin, K.S.; Chun, S.K.; Skalisky, J.; Hammond, L.E.; Mezulis, A.H. Loneliness among young adults during covid-19 pandemic: The mediational roles of social media use and social support seeking. J. Soc. Clin. Psychol. 2020, 39, 708–726. [Google Scholar] [CrossRef]
- Hubbard, G.; den Daas, C.; Dixon, D.; Johnston, M.; Murchie, P.; Thompson, C.W. Is rurality, area deprivation, access to outside space and green space associated with mental health during the Covid-19 pandemic? A cross sectional study from the Covid-19 Health and Adherence Research in Scotland (CHARIS) project. Int. J. Environ. Res. Public Health 2021, 18, 3869. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Green, J.; Quintana, A.; Gitomer, A.; Chwe, H.; Simonson, M.; Lazer, D.; Baum, M.A.; Lin, J.; Ognyanova, K.; et al. The COVID States Project #23: Depression among young adults. Oxf. Prepr. 2021. [Google Scholar] [CrossRef]
- Dawel, A.; Shou, Y.; Smithson, M.; Cherbuin, N.; Banfield, M.; Calear, A.L.; Farrer, L.M.; Gray, D.; Gulliver, A.; Housen, T.; et al. The Effect of COVID-19 on Mental Health and Wellbeing in a Representative Sample of Australian Adults. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Newby, J.M.; O’Moore, K.; Tang, S.; Christensen, H.; Faasse, K. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS ONE 2020, 15, e0236562. [Google Scholar] [CrossRef]
- Rossell, S.L.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Meyer, D. An overview of current mental health in the general population of Australia during the COVID-19 pandemic: Results from the COLLATE project. Psychiatry Res. 2021, 296, 113660. [Google Scholar] [CrossRef]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the “ECLB-COVID19” multi countries survey. medRxiv 2020. [Google Scholar] [CrossRef]
- Garfin, D.R. Technology as a coping tool during the coronavirus disease 2019 (COVID-19) pandemic: Implications and recommendations. Stress Health 2020, 36, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Stainback, K.; Hearne, B.N.; Trieu, M.M. COVID-19 and the 24/7 News Cycle: Does COVID-19 News Exposure Affect Mental Health? Socius 2020, 6. [Google Scholar] [CrossRef]
- Bendau, A.; Petzold, M.B.; Pyrkosch, L.; Mascarell Maricic, L.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A.; Plag, J. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2020. [Google Scholar] [CrossRef]
- Pahayahay, A.; Khalili-Mahani, N. What Media Helps, What Media Hurts: A Mixed Methods Survey Study of Coping with COVID-19 Using the Media Repertoire Framework and the Appraisal Theory of Stress. J. Med. Internet Res. 2020, 22, e20186. [Google Scholar] [CrossRef] [PubMed]
- Wiederhold, B.K. Using social media to our advantage: Alleviating anxiety during a pandemic. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 197–198. [Google Scholar] [CrossRef]
- Lopez, B.; Kennedy, C.; McPhearson, T. Parks are Critical Urban Infrastructure: Perception and Use of Urban Green Spaces in NYC During COVID-19. Preprints 2020. [Google Scholar] [CrossRef]
- Day, B.H. The Value of Greenspace Under Pandemic Lockdown. Environ. Resour. Econ. 2020, 76, 1161–1185. [Google Scholar] [CrossRef]
- Mell, I.; Whitten, M. Access to Nature in a Post Covid-19 World: Opportunities for Green Infrastructure Financing, Distribution and Equitability in Urban Planning. Int. J. Environ. Res. Public Health 2021, 18, 1527. [Google Scholar] [CrossRef]
- Lu, Y.; Zhao, J.; Wu, X.; Lo, S.M. Escaping to nature during a pandemic: A natural experiment in Asian cities during the COVID-19 pandemic with big social media data. Sci. Total Environ. 2021, 777, 146092. [Google Scholar] [CrossRef]
- Corley, J.; Okely, J.; Taylor, A.; Page, D.; Welstead, M.; Skarabela, B.; Redmond, P.; Cox, S.; Russ, T. Home garden use during COVID-19. J. Environ. Psychol. 2021, 73, 101545. [Google Scholar] [CrossRef]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Lercher, P.; Browning, M.H.E.M.; Stoyanov, D.; Petrova, N.; Novakov, S.; Dimitrova, D.D. Does greenery experienced indoors and outdoors provide an escape and support mental health during the COVID-19 quarantine? Environ. Res. 2020, 2020, 110420. [Google Scholar] [CrossRef]
- Robinson, J.M.; Brindley, P.; Cameron, R.; MacCarthy, D.; Jorgensen, A. Nature’s Role in Supporting Health during the COVID-19 Pandemic: A Geospatial and Socioecological Study. Int. J. Environ. Res. Public Health 2021, 18, 2227. [Google Scholar] [CrossRef] [PubMed]
- Soga, M.; Evans, M.J.; Tsuchiya, K.; Fukano, Y. A room with a green view: The importance of nearby nature for mental health during the COVID-19 pandemic. Ecol. Appl. 2021, 31, e2248. [Google Scholar] [CrossRef] [PubMed]
- Burnett, H.; Olsen, J.R.; Nicholls, N.; Mitchell, R. Change in time spent visiting and experiences of green space following restrictions on movement during the COVID-19 pandemic: A nationally representative cross-sectional study of UK adults. BMJ Open 2021, 11, e044067. [Google Scholar] [CrossRef]
- Richardson, M.; Hamlin, I. Noticing nature, nature connectedness and time in nature: Associations with Human and Nature’s Wellbeing during the Corona Pandemic. J. Public Ment. Health 2021. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Smith, L.J.; Richardson, A.L.; D’Souza, J.M.; Long, L.J. Examining the longitudinal effects and potential mechanisms of hope on COVID-19 stress, anxiety, and well-being. Cogn. Behav. Ther. 2021, 1–12. [Google Scholar] [CrossRef]
- Milman, E.; Lee, S.A.; Neimeyer, R.A.; Mathis, A.A.; Jobe, M.C. Modeling pandemic depression and anxiety: The mediational role of core beliefs and meaning making. J. Affect. Disord. Rep. 2020, 2, 100023. [Google Scholar] [CrossRef]
- Iasiello, M.; van Agteren, J.; Muir Cochrane, E. Mental Health and/or Mental Illness: A Scoping Review of the Evidence and Implications of the Dual-Continua Model of Mental Health. Evid. Base Aust. N. Z. Sch. Gov. 2020, 1, 45. [Google Scholar] [CrossRef]
- Keyes, C.L. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.; Dhingra, S.; Simoes, E. Change in Level of Positive Mental Health as a Predictor of Future Risk of Mental Illness. Am. J. Public Health 2010, 100, 2366–2371. [Google Scholar] [CrossRef]
- Venning, A.; Wilson, A.; Kettler, L.; Eliott, J. Mental Health among Youth in South Australia: A Survey of Flourishing, Languishing, Struggling, and Floundering. Aust. Psychol. 2013, 48, 299–310. [Google Scholar] [CrossRef]
- Teng, E.; Venning, A.; Winefield, H.; Crabb, S. Half Full or Half Empty: The Measurement of Mental Health and Mental Illness in Emerging Australian Adults. Soc. Inq. Well-Being 2015, 1, 1–12. [Google Scholar] [CrossRef][Green Version]
- Keyes, C.L. Mental health in adolescence: Is America’s youth flourishing? Am. J. Orthopsychiatry 2006, 76, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Knoesen, R.; Naudé, L. Experiences of flourishing and languishing during the first year at university. J. Ment. Health 2018, 27, 269–278. [Google Scholar] [CrossRef]
- Antaramian, S.P. A Dual-Factor Model of Mental Health: Understanding Student Engagement and School Performance Using a Person-Centered Approach; University of South Carolina: Columbia, SC, USA, 2010. [Google Scholar]
- Antaramian, S.P.; Huebner, E.S.; Hills, K.J.; Valois, R.F. A dual-factor model of mental health: Toward a more comprehensive understanding of youth functioning. Am. J. Orthopsychiatry 2010, 80, 462. [Google Scholar] [CrossRef]
- Eklund, K.; Dowdy, E.; Jones, C.; Furlong, M. Applicability of the dual-factor model of mental health for college students. J. Coll. Stud. Psychother. 2010, 25, 79–92. [Google Scholar] [CrossRef]
- Hallion, M.; Taylor, A.; Roberts, R. Complete mental health in adult siblings of those with a chronic illness or disability. Disabil. Rehabil. 2018, 40, 296–301. [Google Scholar] [CrossRef]
- Kim, S.E. Complete mental health and suicide resilience among University Students in South Korea. Int. Inf. Inst. Inf. 2017, 20, 5959–5966. [Google Scholar]
- Macaskill, A.; Denovan, A. Assessing psychological health: The contribution of psychological strengths. Br. J. Guid. Couns. 2014, 42, 320–337. [Google Scholar] [CrossRef]
- Renshaw, T.L.; Cohen, A.S. Life satisfaction as a distinguishing indicator of college student functioning: Further validation of the two-continua model of mental health. Soc. Indic. Res. 2014, 117, 319–334. [Google Scholar] [CrossRef]
- Vela, J.C.; Lu, M.-T.P.; Lenz, A.S.; Savage, M.C.; Guardiola, R. Positive psychology and Mexican American college students’ subjective well-being and depression. Hisp. J. Behav. Sci. 2016, 38, 324–340. [Google Scholar] [CrossRef]
- (ABS) ABoS. Socio-Economic Indexes for Areas; ABS: Canberra, Australia, 2018.
- Du Plooy, D.R.; Lyons, A.; Kashima, E.S. Predictors of Flourishing and Psychological Distress Among Migrants to Australia: A Dual Continuum Approach. J. Happiness Stud. 2019, 20, 561–578. [Google Scholar] [CrossRef]
- Keyes, C.L.; Wissing, M.; Potgieter, J.P.; Temane, M.; Kruger, A.; van Rooy, S. Evaluation of the mental health continuum-short form (MHC-SF) in setswana-speaking South Africans. Clin. Psychol. Psychother 2008, 15, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357. [Google Scholar] [CrossRef]
- Prawitz, A.; Garman, E.; Benoit, S.; Barbara, O.N.; Kim, J.; Drentea, P. InCharge Financial Distress/Financial Well-Being Scale: Development, Administration, and Score Interpretation. Financ. Couns. Plan. 2006, 17. [Google Scholar] [CrossRef]
- Oswald, T.K.; Rumbold, A.R.; Kedzior, S.G.E.; Moore, V.M. Psychological impacts of “screen time” and “green time” for children and adolescents: A systematic scoping review. PLoS ONE 2020, 15, e0237725. [Google Scholar] [CrossRef]
- Annerstedt van den Bosch, M.; Mudu, P.; Uscila, V.; Barrdahl, M.; Kulinkina, A.; Staatsen, B.; Swart, W.; Kruize, H.; Zurlyte, I.; Egorov, A.I. Development of an urban green space indicator and the public health rationale. Scand. J. Public Health 2016, 44, 159–167. [Google Scholar] [CrossRef]
- Snyder, C.; Harris, C.; Anderson, J.; Holleran, S.; Irving, L.; Sigmon, S. Adult Hope Scale (AHS). J. Personal. Soc. Psychol. 2007, 60, 570–585. [Google Scholar] [CrossRef]
- Cann, A.; Calhoun, L.; Tedeschi, R.; Kilmer, R.; Gil-Rivas, V.; Vishnevsky, T.; Danhauer, S. The Core Beliefs Inventory: A brief measure of disruption in the assumptive world. Anxiety Stress Coping 2009, 23, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Matilla-Santander, N.; Ahonen, E.; Albin, M.; Baron, S.; Bolíbar, M.; Bosmans, K.; Burström, B.; Cuervo, I.; Davis, L.; Gunn, V.; et al. COVID-19 and Precarious Employment: Consequences of the Evolving Crisis. Int. J. Health Serv. 2021. [Google Scholar] [CrossRef]
- Geary, R.S.; Wheeler, B.; Lovell, R.; Jepson, R.; Hunter, R.; Rodgers, S. A call to action: Improving urban green spaces to reduce health inequalities exacerbated by COVID-19. Prev. Med. 2021, 145, 106425. [Google Scholar] [CrossRef] [PubMed]
- Lades, L.K.; Laffan, K.; Daly, M.; Delaney, L. Daily emotional well-being during the COVID-19 pandemic. Br. J. Health Psychol. 2020, 25, 902–911. [Google Scholar] [CrossRef]
- Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H.; Nowell, M. Urban nature in a time of crisis: Recreational use of green space increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [Google Scholar] [CrossRef]
- Grima, N.; Corcoran, W.; Hill-James, C.; Langton, B.; Sommer, H.; Fisher, B. The importance of urban natural areas and urban ecosystem services during the COVID-19 pandemic. PLoS ONE 2020, 15, e0243344. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Mavoa, S.; Badland, H.M.; Giles-Corti, B. Do low-income neighbourhoods have the least green space? A cross-sectional study of Australia’s most populous cities. BMC Public Health 2014, 14, 292. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Lopez, S.J. The Oxford Handbook of Hope; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Braun-Lewensohn, O.; Abu-Kaf, S.; Kalagy, T. Hope and Resilience During a Pandemic Among Three Cultural Groups in Israel: The Second Wave of Covid-19. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Leontopoulou, S. Hope Interventions for the Promotion of Well-Being Throughout the Life Cycle. In Oxford Research Encyclopedia of Education; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Campbell, R.M.; Venn, T.J.; Anderson, N.M. Cost and performance tradeoffs between mail and internet survey modes in a nonmarket valuation study. J. Environ. Manag. 2018, 210, 316–327. [Google Scholar] [CrossRef]
- Pierce, M.; McManus, S.; Jessop, C.; John, A.; Hotopf, M.; Ford, T.; Hatch, S.; Wessely, S.; Abel, K.M. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry 2020, 7, 567–568. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 May 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mental Health State | K-10 a | MHC-SF b |
|---|---|---|
| Flourishing (Complete Mental Health) | Likely to be well (<20) or mild (20–24) psychological distress | Feels 1 of the 3 emotional well-being symptoms “every day” or “almost every day” and feels 6 of the 11 social/psychological symptoms “every day” or “almost every day” |
| Languishing (Incomplete Mental Health) | Likely to be well (<20) or mild (20–24) psychological distress | Not compatible with Flourishing |
| Struggling (Incomplete Mental Illness) | Moderate (25–29) or severe (30+) psychological distress | Not compatible with Floundering |
| Floundering (Complete Mental Illness) | Moderate (25–29) or severe (30+) psychological distress | Feels 1 of the 3 emotional well-being symptoms “never” or “once or twice” and feels 6 of the 11 social/psychological well-being symptoms “never” or “once or twice” |
| Study Variable | Total n (%) | Flourishing n (%) | Languishing n (%) | Struggling n (%) | Floundering n (%) | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | 0.69 | |||||
| M = 21.23 (SD 1.93) | M = 21.37 (SD 1.90) | M = 21.37 (SD 1.87) | M = 21.14 (SD 1.20) | M = 21.09 (SD 1.92) | ||
| Gender | 0.19 | |||||
| Male | 450 (45%) | 61 (43%) | 226 (47%) | 115 (45%) | 48 (38%) | |
| Female | 548 (55%) | 81 (57%) | 246 (52%) | 141 (55%) | 80 (62%) | |
| Gender Diverse/Non-Binary * | 6 (<1%) | 0 (0%) | 5 (1%) | 1 (<1%) | 0 (0%) | |
| Birthplace | 0.36 | |||||
| In Australia | 801 (80%) | 113 (80%) | 391 (77%) | 197 (82%) | 100 (78%) | |
| Outside Australia | 203 (20%) | 29 (20%) | 86 (23%) | 60 (18%) | 28 (22%) | |
| State/Territory of Residence | 0.98 | |||||
| Australian Capital Territory | 15 (1%) | 2 (1%) | 7 (1%) | 4 (2%) | 2 (2%) | |
| New South Wales | 330 (33%) | 47 (33%) | 161 (34%) | 87 (34%) | 35 (27%) | |
| Queensland | 160 (16%) | 22 (15%) | 70 (15%) | 43 (17%) | 25 (20%) | |
| South Australia | 79 (8%) | 9 (6%) | 40 (8%) | 19 (7%) | 11 (9%) | |
| Tasmania | 39 (4%) | 9 (6%) | 16 (3%) | 9 (3%) | 5 (4%) | |
| Victoria | 274 (27%) | 35 (25%) | 133 (28%) | 68 (26%) | 38 (30%) | |
| Western Australia | 107 (11%) | 18 (13%) | 50 (10%) | 27 (11%) | 12 (9%) | |
| Area-Level Socioeconomic Status Quintile | 0.57 | |||||
| 1 (most disadvantaged) | 191 (19%) | 24 (17%) | 101 (21%) | 39 (15%) | 27 (21%) | |
| 2 | 149 (15%) | 19 (13%) | 71 (15%) | 39 (15%) | 20 (16%) | |
| 3 | 205 (20%) | 32 (23%) | 97 (20%) | 50 (19%) | 26 (20%) | |
| 4 | 224 (22%) | 31 (22%) | 93 (20%) | 68 (26%) | 32 (25%) | |
| 5 (most advantaged) | 235 (23%) | 36 (25%) | 115 (24%) | 61 (24%) | 23 (18%) | |
| Studying in 2020 | 0.04 | |||||
| Not studying | 343 (34%) | 54 (38%) | 92 (36%) | 153 (32%) | 44 (35%) | |
| Year 11 or 12 (high school) | 71 (7%) | 7 (5%) | 14 (5%) | 44 (7%) | 6 (5%) | |
| VET or PD | 208 (21%) | 27 (19%) | 38 (15%) | 110 (21%) | 33 (26%) | |
| University | 381 (38%) | 54 (38%) | 112 (44%) | 170 (38%) | 45 (35%) | |
| Type of Residential Dwelling | 0.47 | |||||
| Apartment/Unit (Multi-Storey Group) | 135 (13%) | 15 (11%) | 37 (14%) | 73 (15%) | 19 (15%) | |
| Unit (Single-Storey Group) | 144 (14%) | 16 (11%) | 37 (14%) | 72 (15%) | 10 (8%) | |
| Town house | 88 (9%) | 12 (9%) | 20 (8%) | 44 (9%) | 12 (10%) | |
| House | 634 (63%) | 98 (69%) | 163 (63%) | 287 (60%) | 86 (68%) | |
| Months in COVID-19 lockdowns | 0.34 | |||||
| M = 3.57 (SD 2.74) | M = 3.73 (SD 2.80) | M = 3.68 (SD 2.69) | M = 3.29 (SD 2.63) | M = 4.20 (SD 3.04) |
| Variables | Languishing vs. Flourishing | Struggling vs. Flourishing | Floundering vs. Flourishing |
|---|---|---|---|
| Living arrangement | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) |
| Alone | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Couple | 0.58 (0.20–1.70) | 0.51 (0.19–1.35) | 0.67 (0.20–2.19) |
| Parent(s) and/or sibling(s) | 0.55 (0.22–1.37) | 0.31 (0.13–0.71) | 0.43 (0.16–1.19) |
| Dependent child(ren) (with or without partner) | 0.39 (0.11–1.30) | 0.31 (0.11–0.92) | 0.36 (0.09–1.47) |
| Housemate(s)/Friend(s) | 0.85 (0.30–2.46) | 0.42 (0.16–1.11) | 0.66 (0.20–2.14) |
| Other mix | 0.85 (0.29–2.52) | 0.51 (0.19–1.38) | 0.66 (0.20–2.23) |
| Employment precarity | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) |
| Permanent | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Fixed-Term | 3.32 (1.27–8.71) | 3.52 (1.42–8.68) | 2.92 (0.88–9.67) |
| Regular Casual Hours | 1.40 (0.77–2.53) | 1.50 (0.88–2.53) | 1.65 (0.77–3.55) |
| Irregular Casual Hours | 1.39 (0.62–3.12) | 1.39 (0.68–2.86) | 4.02 (1.67–9.67) |
| JobKeeper (COVID-19 welfare support) | 2.84 (0.74–10.88) | 4.27 (1.25–14.60) | 7.89 (1.97–31.51) |
| Not Employed | 1.99 (1.17–3.38) | 1.17 (0.71–1.93) | 3.22 (1.67–6.23) |
| Working from home was stressful | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) |
| Disagree | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Neutral | 1.07 (0.38–3.00) | 1.31 (0.50–3.41) | 2.67 (0.51–14.00) |
| Agree | 1.07 (0.44–2.56) | 2.98 (1.35–6.56) | 4.58 (1.10–19.06) |
| Change in work hours during COVID-19 | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) |
| Stayed the same | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Decreased | 0.96 (0.57–1.61) | 2.61 (1.62–4.20) | 3.21 (1.61–6.41) |
| Increased | 0.96 (0.45–2.06) | 3.01 (1.54–5.88) | 3.47 (1.39–8.64) |
| Change in income during COVID-19 | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) |
| Stayed the same | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Decreased | 1.28 (0.74–2.21) | 2.53 (1.54–4.15) | 2.54 (1.32–4.89) |
| Increased | 1.19 (0.63–2.26) | 2.11 (1.19–3.75) | 1.09 (0.47–2.57) |
| Financial Stress | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) |
| No-to-Low | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Moderate | 1.63 (1.01–2.64) | 2.10 (1.29–3.40) | 5.33 (2.35–12.10) |
| High-to-Overwhelming | 1.66 (0.98–2.82) | 7.27 (4.42–11.97) | 15.28 (6.81–34.30) |
| Variables | Languishing vs. Flourishing | Struggling vs. Flourishing | Floundering vs. Flourishing | |||
|---|---|---|---|---|---|---|
| Change in screen time | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) | |||
| Stayed the same | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Decreased | 4.53 (0.95–21.72) | 23.85 (5.44–104.41) | 3.27 (0.58–18.37) | |||
| Increased | 1.42 (0.83–2.37) | 2.20 (1.32–3.65) | 1.18 (0.65–2.17) | |||
| Experience variables | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) | |||
| Screen time helped connect with family and friends | ||||||
| Neutral | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Disagree | 0.56 (0.18–1.76) | 0.55 (0.19–1.56) | 0.72 (0.22–2.34) | |||
| Agree | 0.55 (0.22–1.36) | 0.19 (0.08–0.43) | 0.24 (0.09–0.62) | |||
| Found myself disengaging from technology communications | ||||||
| Neutral | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Disagree | 1.12 (0.66–1.91) | 0.74 (0.44–1.25) | 0.43 (0.20–0.90) | |||
| Agree | 1.15 (0.67–1.99) | 1.76 (1.07–2.89) | 1.92 (1.05–3.51) | |||
| Screen time was fatiguing | ||||||
| Neutral | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Disagree | 0.50 (0.26–0.97) | 0.47 (0.25–0.89) | 0.51 (0.22–1.16) | |||
| Agree | 1.11 (0.63–1.96) | 1.67 (0.97–2.88) | 1.29 (0.66–2.51) | |||
| Technology helped me cope | ||||||
| Neutral | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Disagree | 1.24 (0.57–2.72) | 1.44 (0.67–3.09) | 2.56 (1.06–6.14) | |||
| Agree | 0.65 (0.39–1.07) | 1.08 (0.67–1.76) | 0.96 (0.52–1.76) | |||
| Needed to restrict exposure to news | ||||||
| Neutral | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |||
| Disagree | 0.96 (0.52–1.76) | 0.69 (0.38–1.24) | 0.60 (0.28–1.27) | |||
| Agree | 1.05 (0.61–1.84) | 1.08 (0.64–1.82) | 0.78 (0.41–1.48) | |||
| Variables | Languishing vs. Flourishing | Struggling vs. Flourishing | Floundering vs. Flourishing |
|---|---|---|---|
| Access to residential outdoor space | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) |
| Yes | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| No | 0.98 (0.24–4.05) | 3.22 (0.95–10.86) | 5.02 (1.35–18.63) |
| Perceived neighbourhood naturalness | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) |
| Highly built | 1.95 (0.61–6.25) | 2.00 (0.65–6.12) | 4.05 (1.24–13.27) |
| Moderately built | 1.34 (0.71–2.54) | 1.11 (0.60–2.06) | 1.31 (0.62–2.74) |
| Even mix of built and natural | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Moderately green/natural | 1.21 (0.74–1.97) | 1.67 (1.07–2.65) | 1.12 (0.63–2.01) |
| Highly green/natural | 0.35 (0.14–0.85) | 1.56 (0.82–2.98) | 0.25 (0.07–0.91) |
| Greenspace and/or bluespace within walking distance | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) |
| Yes | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| No | 1.77 (1.02–3.06) | 1.62 (0.97–2.73) | 1.47 (0.78–2.77) |
| Variables | Languishing vs. Flourishing | Struggling vs. Flourishing | Floundering vs. Flourishing | ||
|---|---|---|---|---|---|
| Change in contact with nature during COVID-19 | RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) | ||
| Stayed the same | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | ||
| Decreased | 1.66 (0.97–2.83) | 1.46 (0.89–2.39) | 1.98 (1.09–3.58) | ||
| Increased | 0.96 (0.59–1.57) | 0.79 (0.51–1.24) | 0.49 (0.26–0.95) | ||
| Experience variables | RRRb (95% CI) | RRRb (95% CI) | RRRb (95% CI) | ||
| Spending time in nature felt like “getting away” | |||||
| Disagree | 3.22 (1.18–8.76) | 4.35 (1.67–11.33) | 5.92 (2.06–17.03) | ||
| Neutral | 1.70 (0.95–3.05) | 1.51 (0.87–2.63) | 1.88 (0.95–3.70) | ||
| Agree | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | ||
| Spending time in nature felt uncomfortable | |||||
| Disagree | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | ||
| Neutral | 1.39 (0.74–2.59) | 2.61 (1.46–4.69) | 2.10 (1.03–4.25) | ||
| Agree | 1.35 (0.69–2.63) | 5.51 (3.05–9.94) | 2.32 (1.10–4.89) |
| Variables | Languishing vs. Flourishing | Struggling vs. Flourishing | Floundering vs. Flourishing |
|---|---|---|---|
| RRRa (95% CI) | RRRa (95% CI) | RRRa (95% CI) | |
| Increasing Levels of Hope | 0.90 (0.87–0.92) | 0.85 (0.83–0.88) | 0.76 (0.73–0.79) |
| Increasing Disruption of Core Beliefs | 1.06 (0.85–1.32) | 1.97 (1.56–2.48) | 2.83 (2.04–3.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oswald, T.K.; Rumbold, A.R.; Kedzior, S.G.E.; Kohler, M.; Moore, V.M. Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature. Int. J. Environ. Res. Public Health 2021, 18, 5630. https://doi.org/10.3390/ijerph18115630
Oswald TK, Rumbold AR, Kedzior SGE, Kohler M, Moore VM. Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature. International Journal of Environmental Research and Public Health. 2021; 18(11):5630. https://doi.org/10.3390/ijerph18115630
Chicago/Turabian StyleOswald, Tassia K., Alice R. Rumbold, Sophie G. E. Kedzior, Mark Kohler, and Vivienne M. Moore. 2021. "Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature" International Journal of Environmental Research and Public Health 18, no. 11: 5630. https://doi.org/10.3390/ijerph18115630
APA StyleOswald, T. K., Rumbold, A. R., Kedzior, S. G. E., Kohler, M., & Moore, V. M. (2021). Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature. International Journal of Environmental Research and Public Health, 18(11), 5630. https://doi.org/10.3390/ijerph18115630