
Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Hearing Screening
2.3. Otoscopy and PTA
2.4. Questionnaire
2.5. Statistics
3. Results
3.1. Hearing Screening, Otoscopy and PTA
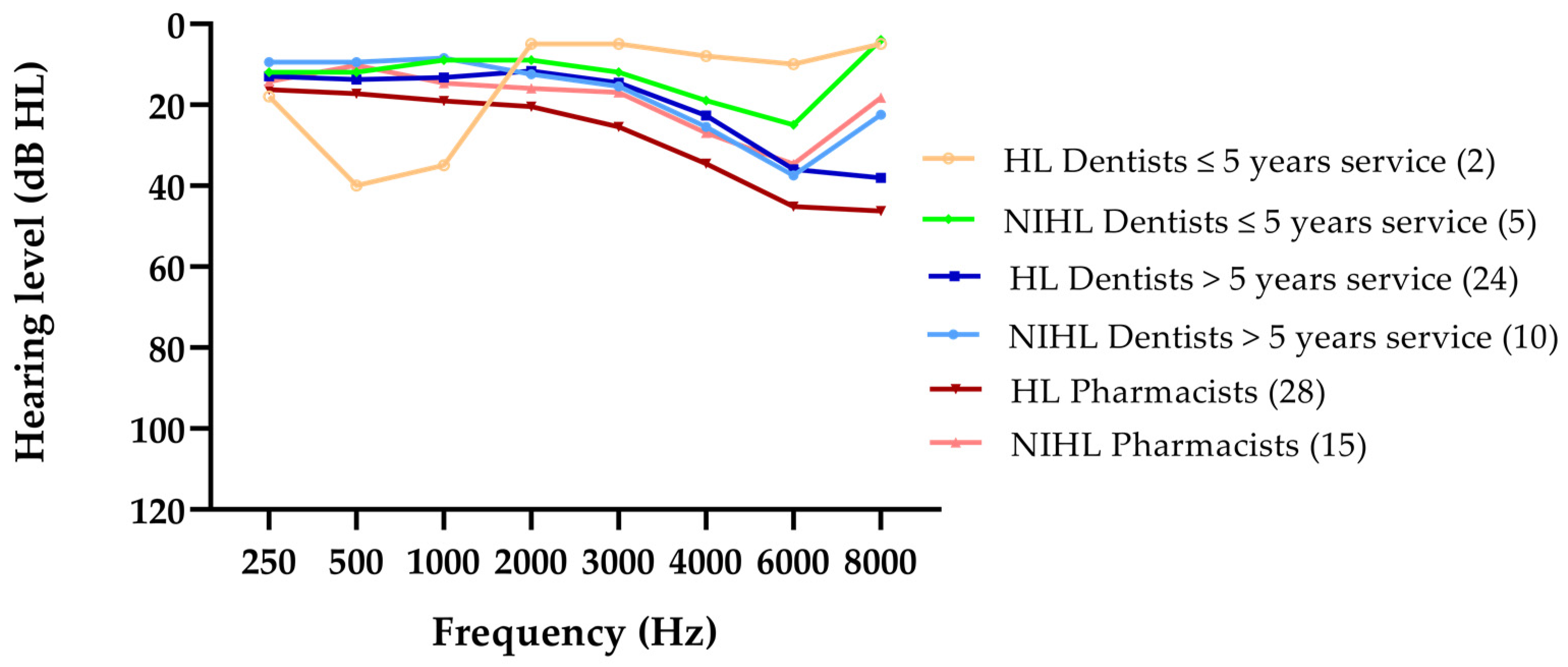
3.2. Pattern of HL
3.3. NIHL Due to Dentistry or Not?
3.4. Survey
3.4.1. General Information
3.4.2. Exposure to Noise
3.4.3. Annoyance
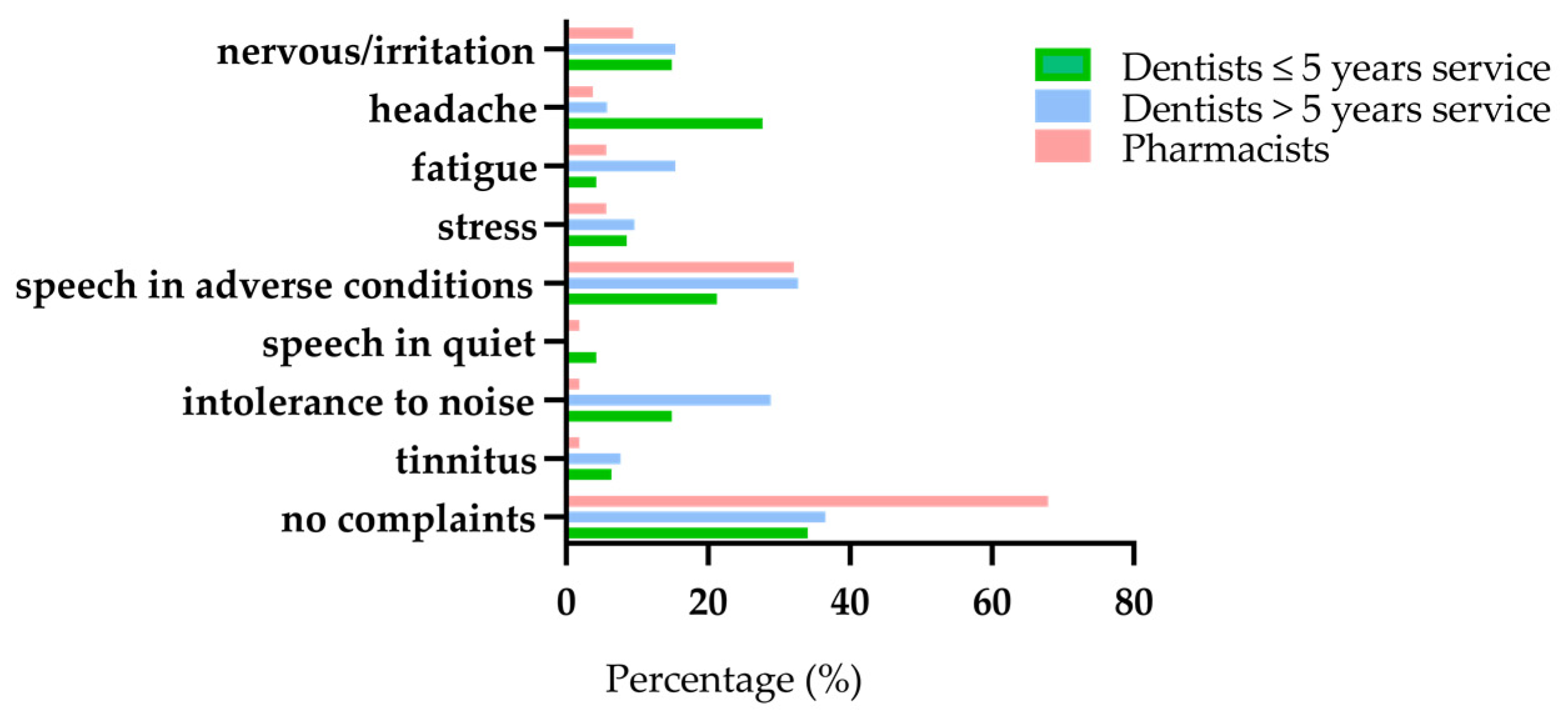
3.4.4. Complaints
3.4.5. Knowledge on HL and Hearing Protection
4. Discussions
4.1. Hearing Loss
4.2. Annoyance
4.3. Exposure and Equipment
4.4. Hearing Care
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dube, K.J.; Ingale, L.T.; Ingale, S.T. Hearing impairment among workers exposed to excessive levels of noise in ginning industries. Noise Health 2011, 13, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Engdahl, B.; Tambs, K. Occupation and the risk of hearing impairment--results from the Nord-Trøndelag study on hearing loss. Scand. J. Work. Environ. Health 2009, 36, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurti, S. Sensorineural Hearing Loss Associated with Occupational Noise Exposure: Effects of Age-Corrections. Int. J. Environ. Res. Public Health 2009, 6, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, K.F.; Dos Santos, R.B.; Klien, C.A., Jr. Assessment of noise intensity in a dental teaching clinic. BDJ Open 2017, 3, 17010. [Google Scholar] [CrossRef] [PubMed]
- Hopp, E.S. Acoustic Trauma in High-Speed Dental Drills. Laryngoscope 1962, 72, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, H.C. Decibel ratings of dental office sounds. J. Prosthet. Dent. 1981, 45, 175–178. [Google Scholar] [CrossRef]
- Mueller, H.J.; Sabri, Z.I.; Suchak, A.J.; McGill, S.; Stanford, J.W. Noise level evaluation of dental handpieces. J. Oral Rehabilitation 1986, 13, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.O.; Ali, W.J. Noise Levels, Noise Annoyance and Hearing-Related Problems in a Dental College. Arch. Environ. Occup. Health 2016, 72, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Bali, N.; Acharya, S.; Anup, N. An assessment of the effect of sound produced in a dental clinic on the hearing of dentists. Oral Health Prev Dent. 2007, 5, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Barek, S.; Adam, O.; Motsch, J.F. Large band spectral analysis and harmful risks of dental turbines. Clin. Oral Investig. 1999, 3, 49–54. [Google Scholar] [CrossRef]
- Gurbuz, M.K.; Çatli, T.; Cingi, C.; Yaz, A.; Bal, C. Occupational Safety Threats Among Dental Personnel and Related Risk Factors. J. Craniofacial Surg. 2013, 24, e599–e602. [Google Scholar] [CrossRef]
- Fernandes, S.; Carvalho, A.P.; Gallas, M.; Vaz, P.; Matos, P.A. Noise levels in dental schools. Eur. J. Dent. Educ. 2006, 10, 32–37. [Google Scholar] [CrossRef]
- Theodoroff, S.M.; Folmer, R.L. Hearing loss associated with long-term exposure to high-speed dental handpieces. Gen. Dent. 2015, 63, 71–76. [Google Scholar]
- Willershausen, B.; Callaway, A.; Wolf, T.G.; Ehlers, V.; Scholz, L.; Wolf, D.; Letzel, S. Hearing assessment in dental practitioners and other academic professionals from an urban setting. Head Face Med. 2014, 10, 1. [Google Scholar] [CrossRef]
- Wilson, J.D.; Darby, M.L.; Tolle, S.L.; Sever, J.C., Jr. Effects of occupational ultrasonic noise exposure on hearing of dental hygienists: A pilot study. J. Dent. Hyg. JDH 2002, 76, 262–269. [Google Scholar]
- Burk, A.; Neitzel, R.L. An exploratory study of noise exposures in educational and private dental clinics. J. Occup. Environ. Hyg. 2016, 13, 741–749. [Google Scholar] [CrossRef][Green Version]
- Ramsey, R.; Greenough, J.; Breeze, J. Noise-induced hearing loss in the military dental setting: A UK legislative perspective. BMJ Mil. Health 2020, 166, e53–e56. [Google Scholar] [CrossRef]
- Choosong, T.; Kaimook, W.; Tantisarasart, R.; Sooksamear, P.; Chayaphum, S.; Kongkamol, C.; Srisintorn, W.; Phakthongsuk, P. Noise Exposure Assessment in a Dental School. Saf. Health Work. 2011, 2, 348–354. [Google Scholar] [CrossRef]
- Daud, M.K.; Noh, N.F.; Sidek, D.S.; Abd Rahman, N.; Abd Rani, N.A.; Zakaria, M.N. Screening of dental staff nurses for noise induced hearing loss. B ENT 2011, 7, 245–249. [Google Scholar]
- Dutta, A.; Mala, K.; Acharya, S.R. Sound levels in conservative dentistry and endodontics clinic. J. Conserv. Dent. 2013, 16, 121–125. [Google Scholar] [CrossRef]
- Jadid, K.; Klein, U.; Meinke, D. Assessment of noise exposures in a pediatric dentistry residency clinic. Pediatr. Dent. 2011, 33, 343–348. [Google Scholar] [PubMed]
- Myers, J.; John, A.B.; Kimball, S.; Fruits, T. Prevalence of Tinnitus and Noise-induced Hearing Loss in Dentists. Noise Health 2016, 18, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Al-Omoush, S.A.; Abdul-Baqi, K.J.; Zuriekat, M.; Alsoleihat, F.; Elmanaseer, W.R.; Jamani, K.D. Assessment of occupational noise-related hearing impairment among dental health personnel. J. Occup. Health 2020, 62, 12093. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.C.; De Melo, A.D.P.; Santos, C.C. A study of the high-frequency hearing thresholds of dentistry professionals. Int. Arch. Otorhinolaryngol. 2012, 16, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Messano, G.A.; Petti, S. General dental practitioners and hearing impairment. J. Dent. 2012, 40, 821–828. [Google Scholar] [CrossRef]
- Forman-Franco, B.; Abramson, A.L.; Stein, T. High-speed drill noise and hearing: Audiometric survey of 70 dentists. J. Am. Dent. Assoc. 1978, 97, 479–482. [Google Scholar] [CrossRef]
- Gonçalves, C.G.D.O.; Santos, L.; Lobato, D.; Ribas, A.; Lacerda, A.B.M.; Marques, J. Characterization of Hearing Thresholds from 500 to 16,000 Hz in Dentists: A Comparative Study. Int. Arch. Otorhinolaryngol. 2014, 19, 156–160. [Google Scholar] [CrossRef][Green Version]
- Rahko, A.A.; Karma, P.H.; Rahko, K.T.; Kataja, M.J. High-frequency hearing of dental personnel. Community Dent. Oral Epidemiol. 1988, 16, 268–270. [Google Scholar] [CrossRef]
- Al-Rawi, N.H.; Al Nuaimi, A.S.; Sadiqi, A.; Azaiah, E.; Ezzeddine, D.; Ghunaim, Q.; Abbas, Z. Occupational noise-induced hearing loss among dental professionals. Quintessence Int. 2019, 50, 245–250. [Google Scholar] [CrossRef]
- Ma, K.W.; Wong, H.M.; Mak, C.M. Dental Environmental Noise Evaluation and Health Risk Model Construction to Dental Professionals. Int. J. Environ. Res. Public Health 2017, 14, 1084. [Google Scholar] [CrossRef]
- Khaimook, W.; Suksamae, P.; Choosong, T.; Chayarpham, S.; Tantisarasart, R. The Prevalence of Noise-Induced Occupational Hearing Loss in Dentistry Personnel. Work. Health Saf. 2014, 62, 357–360. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 7029: Acoustics—Statistical Distribution of Hearing Thresholds as a Function of Age, 2nd ed.; International Organization for Standardization: Geneva, Switzerland, 2000. [Google Scholar]
- Golmohammadi, R.; Darvishi, E. The Combined Effects of Occupational Exposure to Noise and Other Risk Factors—A Systematic Review. Noise Health 2019, 21, 125–141. [Google Scholar] [CrossRef]
- Franssen, E.A.M.; Wiechen, C.M.A.G.V.; Nagelkerke, N.J.D.; Lebret, E. Aircraft noise around a large international airport and its impact on general health and medication use. Occup. Environ. Med. 2004, 61, 405–413. [Google Scholar] [CrossRef]
- Seidler, A.; Wagner, M.; Schubert, M.; Dröge, P.; Römer, K.; Pons-Kühnemann, J.; Swart, E.; Zeeb, H.; Hegewald, J. Aircraft, road and railway traffic noise as risk factors for heart failure and hypertensive heart disease—A case-control study based on secondary data. Int. J. Hyg. Environ. Health 2016, 219, 749–758. [Google Scholar] [CrossRef]
- Stansfeld, S.A.; Berglund, B.; Clark, C.; Lopez-Barrio, I.; Fischer, P.; Ohrström, E.; Haines, M.M.; Head, J.; Hygge, S.; van Kamp, I.; et al. Aircraft and road traffic noise and children’s cognition and health: A cross-national study. Lancet 2005, 365, 1942–1949. [Google Scholar] [CrossRef]
- Tzivian, L.; Winkler, A.; Dlugaj, M.; Schikowski, T.; Vossoughi, M.; Fuks, K.; Weinmayr, G.; Hoffmann, B. Effect of long-term outdoor air pollution and noise on cognitive and psychological functions in adults. Int. J. Hyg. Environ. Health 2015, 218, 1–11. [Google Scholar] [CrossRef]
- Yoshida, T.; Osada, Y.; Kawaguchi, T.; Hoshiyama, Y.; Yoshida, K.; Yamamoto, K. Effects of Road Traffic Noise on Inhabitants of Tokyo. J. Sound Vib. 1997, 205, 517–522. [Google Scholar] [CrossRef]
- Gijbels, F.; Jacobs, R.; Princen, K.; Nackaerts, O.; Debruyne, F. Potential occupational health problems for dentists in Flanders, Belgium. Clin. Oral Investig. 2006, 10, 8–16. [Google Scholar] [CrossRef]
- Chen, W.-L.; Chen, C.-J.; Yeh, C.-Y.; Lin, C.-T.; Cheng, H.-C.; Chen, R.-Y. Workplace Noise Exposure and Its Consequent Annoyance to Dentists. J. Exp. Clin. Med. 2013, 5, 177–180. [Google Scholar] [CrossRef]
- Van den Borre, E.V.; Denys, S.; van Wieringen, A.; Wouters, J. The digit triplet test: A scoping review. Int. J. Audiol. 2021, 1–18. [Google Scholar] [CrossRef]
- Jansen, S.; Luts, H.; Dejonckere, P.; van Wieringen, A.; Wouters, J. Efficient Hearing Screening in Noise-Exposed Listeners Using the Digit Triplet Test. Ear Hear. 2013, 34, 773–778. [Google Scholar] [CrossRef] [PubMed]
- IBM SPSS Statistics for Windows; Version 27; IBM Corp.: Armonk, NY, USA, 2020.
- Hickox, A.E.; Liberman, M.C. Is noise-induced cochlear neuropathy key to the generation of hyperacusis or tinnitus? J. Neurophysiol. 2014, 111, 552–564. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, S.G.; Liberman, M.C. Adding Insult to Injury: Cochlear Nerve Degeneration after “Temporary” Noise-Induced Hearing Loss. J. Neurosci. 2009, 29, 14077–14085. [Google Scholar] [CrossRef] [PubMed]
- Fabry, D.A. Hearing loss as occupational hazard. Northwest Dent. 1995, 74, 29–32. [Google Scholar]
- Zubick, H.H.; Tolentino, A.T.; Boffa, J. Hearing loss and the high speed dental handpiece. Am. J. Public Health 1980, 70, 633–635. [Google Scholar] [CrossRef][Green Version]
- Taylor, W.; Pearson, J.; Mair, A. The Hearing Threshold Levels of Dental Practitioners Exposed to Air Turbine Drill Noise. Br. Dent. J. 1965, 118, 206–210. [Google Scholar]
- Wilson, C.; Vaidyanathan, T.; Cinotti, W.; Cohen, S.; Wang, S. Hearing-damage Risk and Communication Interference in Dental Practice. J. Dent. Res. 1990, 69, 489–493. [Google Scholar] [CrossRef]
- Shepherd, D.; Heinonen-Guzejev, M.; Hautus, M.J.; Heikkilä, K. Elucidating the relationship between noise sensitivity and personality. Noise Health 2015, 17, 165–171. [Google Scholar] [CrossRef]
- Zadeh, L.M.; Silbert, N.H.; Sternasty, K.; Swanepoel, D.W.; Hunter, L.L.; Moore, D.R. Extended high-frequency hearing enhances speech perception in noise. Proc. Natl. Acad. Sci. USA 2019, 116, 23753–23759. [Google Scholar] [CrossRef]
- Maccà, I.; Scapellato, M.L.; Carrieri, M.; Maso, S.; Trevisan, A.; Bartolucci, G.B. High-frequency hearing thresholds: Effects of age, occupational ultrasound and noise exposure. Int. Arch. Occup. Environ. Health 2014, 88, 197–211. [Google Scholar] [CrossRef]
- Dey, A.; Sommers, M.S. Age-related differences in inhibitory control predict audiovisual speech perception. Psychol. Aging 2015, 30, 634–646. [Google Scholar] [CrossRef]
- Roque, L.; Karawani, H.; Gordon-Salant, S.; Anderson, S. Effects of Age, Cognition, and Neural Encoding on the Perception of Temporal Speech Cues. Front. Neurosci. 2019, 13, 749. [Google Scholar] [CrossRef]
- Van Gerven, P.W.M.; Vos, H.; Van Boxtel, M.P.J.; Janssen, S.A.; Miedema, H.M.E. Annoyance from environmental noise across the lifespan. J. Acoust. Soc. Am. 2009, 126, 187–194. [Google Scholar] [CrossRef]
- Bahannan, S.; El-Hamid, A.A.; Bahnassy, A. Noise level of dental handpieces and laboratory engines. J. Prosthet. Dent. 1993, 70, 356–360. [Google Scholar] [CrossRef]
- Monagahn, D.M.; Wilson, N.H.F.; Darvell, B.W. The performance of air-turbine handpieces in general dental practice. Oper. Dent. 2005, 30, 16–25. [Google Scholar]
- Kadanakuppe, S.; Bhat, P.K.; Jyothi, C.; Ramegowda, C. Assessment of noise levels of the equipments used in the dental teaching institution, Bangalore. Indian J. Dent. Res. 2011, 22, 424–431. [Google Scholar] [CrossRef]
- Smits, C.; Kapteyn, T.S.; Houtgast, T. Development and validation of an automatic speech-in-noise screening test by telephone. Int. J. Audiol. 2004, 43, 15–28. [Google Scholar] [CrossRef]
- Denys, S.; Hofmann, M.; Luts, H.; Guérin, C.; Keymeulen, A.; Van Hoeck, K.; van Wieringen, A.; Hoppenbrouwers, K.; Wouters, J. School-Age Hearing Screening Based on Speech-in-Noise Perception Using the Digit Triplet Test. Ear Hear. 2018, 39, 1104–1115. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Hearing; Licence:CC BY-NC-SA 3.0IGO; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Goderie, T.; van Wier, M.F.; Stam, M.; Lissenberg-Witte, B.I.; Merkus, P.; Smits, C.; Kramer, S.E. Association between Speech Recognition in Noise and Risk Factors of Cardiovascular Disease. Audiol. Neurotol. 2021, 2, 1–10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subject Characteristics | Dentists >5 Years Service (Ears = 106) | Pharmacists (Ears = 106) | Dentists ≤5 Years Service (Ears = 94) |
|---|---|---|---|
| Mean age in years (SD) | 46.6 (10.5) | 46.3 (10.8) | 25.6 (3.1) |
| Range in years | 29–66 | 29–64 | 22–36 |
| Female (%)/male (%) | 27 (51%)/26 (49%) | 27 (51%)/26 (49%) | 28 (60%)/19 (40%) |
| Excl. due to hear. aid (ears) | 2 | 0 | 0 |
| DTT passed (ears) | 71 | 66 | 81 |
| DTT failed (ears) | 33 | 40 | 13 |
| No HL after PTA | 8 | 6 | 7 |
| Occupational NIHL? | 5 | 7 | 2 |
| NIHL due to other causes | 5 | 8 | 3 |
| HL other than NIHL | 24 | 28 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dierickx, M.; Verschraegen, S.; Wierinck, E.; Willems, G.; van Wieringen, A. Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists. Int. J. Environ. Res. Public Health 2021, 18, 5617. https://doi.org/10.3390/ijerph18115617
Dierickx M, Verschraegen S, Wierinck E, Willems G, van Wieringen A. Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists. International Journal of Environmental Research and Public Health. 2021; 18(11):5617. https://doi.org/10.3390/ijerph18115617
Chicago/Turabian StyleDierickx, Michael, Suzanne Verschraegen, Els Wierinck, Guy Willems, and Astrid van Wieringen. 2021. "Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists" International Journal of Environmental Research and Public Health 18, no. 11: 5617. https://doi.org/10.3390/ijerph18115617
APA StyleDierickx, M., Verschraegen, S., Wierinck, E., Willems, G., & van Wieringen, A. (2021). Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists. International Journal of Environmental Research and Public Health, 18(11), 5617. https://doi.org/10.3390/ijerph18115617