
The Lived Experiences of Stigmatization in the Process of HIV Status Disclosure among People Living with HIV in Taiwan

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Setting
2.3. Data Analysis
2.4. Methodological Rigor
2.5. Ethical Considerations
3. Results
3.1. Characteristics of Participants
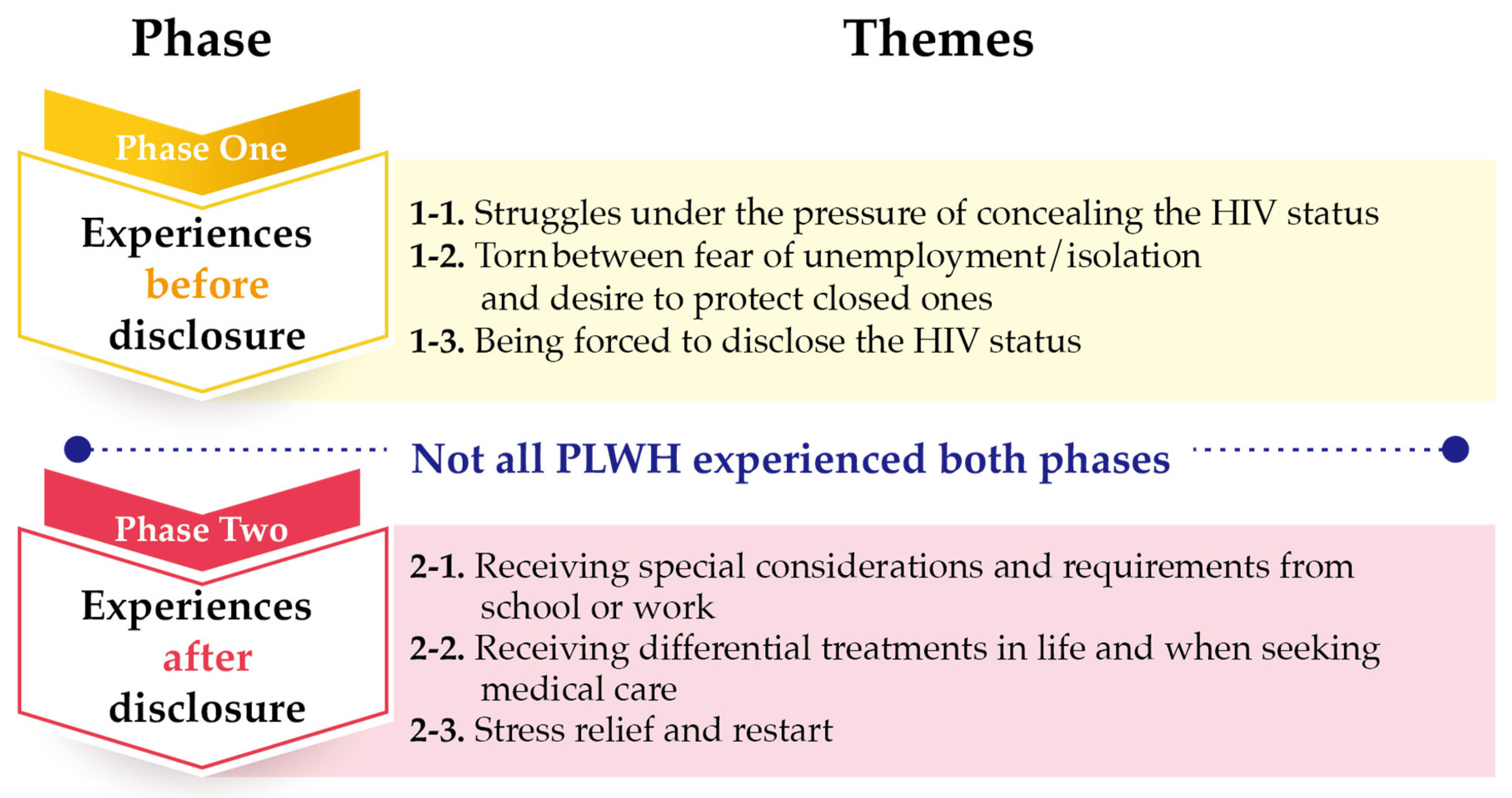
3.2. Themes
3.2.1. Experiences before Disclosure
Struggles under the Pressure of Concealing the HIV Status
“I do not take the antiretroviral medication in front of my colleagues. If I need to take my medication, I would pretend to drink water. So, my colleagues would not see it. Or, I would take my medication at a place where my colleagues would not see, like the lunch room. Sometimes, my colleagues would ask me “do you have cold?”. I would tell them “yes” or I was just taking B complex. I have been hiding it. I do not voluntarily tell them my disease”.(participant #3, 27 years old)
“Initially,only my older sister knew about my diagnosis. However, I sensed that this has created stress on her. I am the only son and, therefore, bear the responsibility to have children to carry the family name. However, I am a gay person with HIV infection. My parents would be unable to accept it if they found out about my diagnosis. I come from a traditional family. My parents have great expectations for me. So, after my older sister became aware of my illness, I asked her not to tell anyone. But, I could tell that this secret has created a lot of stress on her. I have been thinking if I should go ahead and tell my parents”.(participant #6, 25 years old)
Torn between Fear of Unemployment/Isolation and Desire to Protect Closed Ones
“My sister and I watched a TV show a few years ago. When she knew about the actor’s HIV-positive status, she had a strong reaction. She said who dared to bury their corpses! This incident reminded me that my sister cannot accept HIV-positive people. This is why I would never talk about my diagnosis”.(participant #10, 31 years old)
“I choose to tell my partner because I like him a lot. I think it is necessary to tell him about my health. Just like protecting my family, I want to protect him too. I have already been infected with HIV. I do not want to harm others. Because I like him, I am obligated to tell him and protect him. So, I choose to tell him”.(participant #5, 35 years old)
Being Forced to Disclose the HIV Status
“One of the antiretroviral medications needs refrigeration. One time my dad and stepmom saw it because I did not hide the medication well. They questioned me about the medication. Because they both knew about my sexual orientation, they directly associated “a gay taking medications” with “HIV”.(participant #14, 33 years old)
“The day I broke up with my ex-boyfriend, I quarreled with him. As a result, he was shouting outside our rental house. So the neighbors knew that I am an HIV- positive person. He also went to my workplace and told my colleagues that I am HIV positive. I was very embarrassed. Later, some of his friends and others asked me if I was infected with HIV”.(participant #6, 25 years old)
3.2.2. Experiences after Disclosure
Receiving Special Considerations and Requirements from School or Work
“At first, my school cared a lot about my health. Then, they became more concerned about whether I would choose to quit school. I was told that they would notify my parents if I did not cooperate. I was asked to wash dishes and clothes separately from others. I was not allowed to swim. To me, quitting school created an excruciating scar that I could never forget. It was like someone cut my face with a knife”.(participant #19, 26 years old)
“I took Efavirenz and had severe rashes. My boss found out about it. He became concerned about it and asked me to see a doctor. My rashes were rather severe at the time. Because my work was about organic food, we had heightened sensitivity about medicine and diseases. So, my boss kept on questioning about my rashes. He even requested information about my doctor’s visit and medications so that he might get a second opinion. He believed that he had the right to know because he simply wanted to help a colleague and he was my boss. In the end, he even threatened to fire me if I did to provide the requested information. This had jeopardized my right”.(participant #14, 33 years old)
Receiving Differential Treatments in Life and When Seeking Medical Care
“As far as the tableware, my dad bought bowls, chopsticks, spoons, and other silverware for my personal use. So, I told my mom I will not eat at home. I thought … why would you exclude me! I wanted to say how could it become like this. I realized, then, I was different from others”.(participant #7, 27 years old)
“I was isolated from the beginning. My parents thought HIV was transmitted through droplets. So, my dad separated my toothbrush and toothpaste from other family member’s personal care items. The washbasin went from one to two. Originally, we only had one washbasin in the bathroom. My dad added another one. I thought he has gone overboard. Our bathroom was rather small. Why complicate things! At that moment, I began to feel sad about the situation”.(participant #7, 27 years old)
“After my boyfriend knew about my HIV infection, he chose to be silent and disappeared for a while. He appeared one day and wanted to break up with me. I held him and asked him not to leave me. He said, don’t force him. He could not do it. My ex-boyfriend and I are still deeply in love with each other. But our relationship could not continue because of my HIV infection”.(participant #13, 30 years old)
“When I took my lab results to my primary care physician, I could tell that he knew about my HIV infection. He was taken back by my HIV status. I was afraid already. But it was hurtful having to face my physician’s reaction”.(participant #15, 42 years old)
“When the healthcare providers knew that they might have an HIV-positive patient, they became concerned about the possibility of being infected with HIV. They were not sure if they should be wearing full personal protective equipment. When I heard about their reactions, I did not want to share my HIV status with them or my social work friends”.(participant #16, 26 years old)
Stress Relief and Restart
“I think (after I told others about my HIV status) my emotional stress had decreased. If you did not say anything about it, you would not have the freedom to do things. But, after you told others, they would pay attention to my illness and I would also take measures to prevent the spreading of the illness. You would feel less stressed”.(participant #5, 35 years old)
“Watching TV, listening to music, avoid talking about it, and then exercising. I think time helped getting rid of these unpleasant feelings. It might be hidden somewhere in my heart. I try not to think about it”.(participant #10, 31 years old)
“I was not confident. However, I have been working hard to identify an aspect to restore my confidence, such as work. I wanted to do a good job with work and live a good life so that my friends and families would not worry about me. That would be my source of confidence and happiness”.(participant #10, 31 years old)
4. Discussion
4.1. Phase One: Experiences before Disclosure
4.2. Phase Two: Experiences after Disclosure
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. UNAIDS Data 2019. 2019. Available online: https://www.unaids.org/en/resources/documents/2019/2019-UNAIDS-data (accessed on 27 April 2021).
- Taiwan Centers for Disease Control. 2020-03 HIV/AIDS Statistical Report. 2020. Available online: http://at.cdc.tw/LS6K48 (accessed on 27 April 2021).
- Group, I.S.S.; Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fatkenheuer, G.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. Prescription for The Use of Anti-Human Immunodeficiency Virus Drugs. 2021. Available online: https://www.cdc.gov.tw/File/Get/Vpyi67BvwJ8wHGxvUtFFWA (accessed on 27 April 2021).
- Turan, B.; Hatcher, A.M.; Weiser, S.D.; Johnson, M.O.; Rice, W.S.; Turan, J.M. Framing mechanisms linking HIV-related stigma, adherence to treatment, and health outcomes. AJPH 2017, 107, 863–869. [Google Scholar] [CrossRef]
- Guy, A.A.; Niel, K.; Franco Duran, R.E. Disclosure and Stigma of a Positive HIV-Serostatus: A Two-Step Cluster Analysis of the HIV Disclosure Scale. AIDS Behav. 2018, 22, 1606–1613. [Google Scholar] [CrossRef]
- Ko, N.Y.; Lee, H.; Hsu, S.; Wang, W.; Huang, M.; Ko, W.-C. Differences in HIV disclosure by modes of transmission in Taiwanese families. AIDS Care 2007, 19, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Tsai, M.-C. Effects of family context on adolescents’ psychological problems: Moderated by pubertal timing, and mediated by self-esteem and interpersonal relationships. Appl. Res. Qual. Life 2016, 11, 907–923. [Google Scholar] [CrossRef]
- Tsai, M.-C.; Strong, C.; Lin, C.-Y. Effects of pubertal timing on deviant behaviors in Taiwan: A longitudinal analysis of 7th-to 12th-grade adolescents. J. Adolesc. 2015, 42, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Fang, X. Rights and Goods: On Same-sex Marriage. Int. J. Chin. Comp. Philos. Med. 2018, 16, 14. [Google Scholar]
- Tang, S. Same-sex Marriage and Confucian Ethics: A Response to Professor Fang Xudong. Int. J. Chin. Comp. Philos. Med. 2018, 16, 119–123. [Google Scholar]
- Chuang, P.; Liu, C.-T. AIDS Storm: The Stigma of HIV/AIDS Means to the Client and the Public. Nurs. Res. 1997, 5, 52–64. [Google Scholar] [CrossRef]
- Chen, C.H.; Wang, Y.T.; Shu, B.C. Self-Awareness of Disease Stigma: Reflections of Healthcare Professionals. J. Nurs. 2017, 64, 12–18. [Google Scholar] [CrossRef]
- Lin, C.-Y. An Exploratory Study of Barriers to Medical Treatment and Employment and Coping Strategies among HIV-Positive Gay Men; National Taiwan Normal University: Taipei, Taiwan, 2011. [Google Scholar]
- Smit, P.J.; Brady, M.; Carter, M.; Fernandes, R.; Lamore, L.; Meulbroek, M.; Ohayon, M.; Platteau, T.; Rehberg, P.; Rockstroh, J.; et al. HIV-related stigma within communities of gay men: A literature review. AIDS Care 2012, 24, 405–412. [Google Scholar] [CrossRef]
- Chaudoir, S.R.; Fisher, J.D. The disclosure processes model: Understanding disclosure decision making and postdisclosure outcomes among people living with a concealable stigmatized identity. Psychol. Bull. 2010, 136, 236–256. [Google Scholar] [CrossRef] [PubMed]
- Serovich, J.M. A test of two HIV disclosure theories. AIDS Educ. Prev. 2001, 13, 355–364. [Google Scholar] [CrossRef]
- Wang, W.-P. The Impact of Family Relationships on HIV Infection Disclosure and Coping Behaviors. Master Thesis, National Taiwan University, Taipei, Taiwan, 2012. [Google Scholar]
- Tsai, M.-C.L.; Liang, P.; Jiun, W.S.; Chu, F.M. Stress, Needs, and Quality of Life of People Living with Human Immunodeficiency Virus/AIDS in North East China. Hu Li Za Zhi 2017, 64, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Qiao, S.; Li, X.; Zhou, Y.; Shen, Z.; Tang, Z. AIDS impact special issue 2015: Interpersonal factors associated with HIV partner disclosure among HIV-infected people in China. AIDS Care 2016, 28 (Suppl. 1), 37–43. [Google Scholar] [CrossRef]
- UNAIDS. The People Living with HIV Stigma Index in Taiwan. 2018. Available online: https://www.stigmaindex.org/country-report/taiwan/ (accessed on 27 April 2021).
- Chen, S.-J.; Lew-Ting, C.-Y.; Tsai, Y.-F.; Hsiung, P.-C. The Intimate Relationship of Gay Men with HIV/AIDS-Focus on the Emotional Aspect. J. Ment. Health 2004, 17, 97–126. [Google Scholar] [CrossRef]
- Hutson, S.P.; Darlington, C.K.; Hall, J.M.; Heidel, R.E.; Gaskins, S. Stigma and Spiritual Well-being among People Living with HIV/AIDS in Southern Appalachia. Issues Ment. Health Nurs. 2018, 39, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.H.; Kleinman, A. ‘Face’and the embodiment of stigma in China: The cases of schizophrenia and AIDS. Soc. Sci. Med. 2008, 67, 398–408. [Google Scholar] [CrossRef]
- Braje, S.E.; Hall, G.C.N. Coping as a Mediator Between Losing Face and Depressive and Social Anxiety Symptoms Among Asian Americans. J. Cross Cult. Psychol. 2016, 47, 1114–1129. [Google Scholar] [CrossRef]
- Yang, L.H.; Kleinman, A.; Link, B.G.; Phelan, J.C.; Lee, S.; Good, B. Culture and stigma: Adding moral experience to stigma theory. Soc. Sci. Med. 2007, 64, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Florom-Smith, A.L.; de Santis, J.P. Exploring the concept of HIV-related stigma. Nurs. Forum 2012, 47, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Lowther, K.; Selman, L.; Harding, R.; Higginson, I.J. Experience of persistent psychological symptoms and perceived stigma among people with HIV on antiretrovir.al therapy (ART): A systematic review. Int. J. Nurs. Stud. 2014, 51, 1171–1189. [Google Scholar] [CrossRef]
- Mekuria, L.A.; Sprangers, M.A.; Prins, J.M.; Yalew, A.W.; Nieuwkerk, P.T. Health-related quality of life of HIV-infected adults receiving combination antiretroviral therapy in Addis Ababa. AIDS Care 2015, 27, 934–945. [Google Scholar] [CrossRef] [PubMed]
- Steward, W.T.; Chandy, S.; Singh, G.; Panicker, S.T.; Osmand, T.A.; Heylen, E.; Ekstrand, M.L. Depression is not an inevitable outcome of disclosure avoidance: HIV stigma and mental health in a cohort of HIV-infected individuals from Southern India. Psychol. Health Med. 2011, 16, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.Z.; Kahn, D.L.; Steeves, R.H. Hermeneutic Phenomenological Research: A Practical Guide for Nurse Researchers; Sage Publications: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Lee, K.; Steven, K. Why use qualitative research methods to understand the meaning of clients’ experiences in healthcare research? Int. J. Public Health Clin. Sci. 2015, 2, 1–6. [Google Scholar]
- Waltz, C.F.; Strickland, O.L.; Lenz, E.R. Measurement in Nursing and Health Research; Springer Publishing Company: New York, NY, USA, 2010. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Beverly Hills: Los Angeles, CA, USA, 1985. [Google Scholar]
- Stutterheim, S.E.; Brands, R.; Baas, I.; Lechner, L.; Kok, G.; Bos, A.E. HIV status disclosure in the workplace: Positive and stigmatizing experiences of health care workers living with HIV. J. Assoc. Nurses AIDS Care 2017, 28, 923–937. [Google Scholar] [CrossRef] [PubMed]
- Zang, C.; He, X.; Liu, H. Selective disclosure of HIV status in egocentric support networks of people living with HIV/AIDS. AIDS Behav. 2015, 19, 72–80. [Google Scholar] [CrossRef][Green Version]
- Ting, C.Y.; Li, F.Y.; Fang, C.T. Evolving HIV-related clinical experiences, knowledge, and attitudes of physicians: A comparison of 1994 and 2012 survey. Taiwan J. Public Health 2013, 32, 435–448. [Google Scholar] [CrossRef]
- Henry, E.; Bernier, A.; Lazar, F.; Matamba, G.; Loukid, M.; Bonifaz, C.; Diop, S.; Otis, J.; Préau, M. “Was it a mistake to tell others that you are infected with HIV?”: Factors associated with regret following HIV disclosure among people living with HIV in five countries (Mali, Morocco, Democratic Republic of the Congo, Ecuador and Romania). Results from a community-based research. AIDS Behav. 2015, 19, 311–321. [Google Scholar] [CrossRef]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N. Engl. J. Med. 2016, 375, 830–839. [Google Scholar] [CrossRef]
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; van Lunzen, J.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy. JAMA 2016, 316, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Obermeyer, C.M.; Baijal, P.; Pegurri, E. Facilitating HIV disclosure across diverse settings: A review. Am. J. Public Health 2011, 101, 1011–1023. [Google Scholar] [CrossRef] [PubMed]
- Fekete, E.M.; Williams, S.L.; Skinta, M.D.; Bogusch, L.M. Gender differences in disclosure concerns and HIV-related quality of life. AIDS Care 2016, 28, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Lourdes Association. 2017 Survey Report on the Living Conditions of HIV-Infected People in Taiwan. 2017. Available online: https://www.cdc.gov.tw/Category/Page/rCV9N1rGUz9wNr8lggsh2Q (accessed on 27 April 2021).


{kind=link}
|
|
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.-H.; Huang, C.-Y.; Ko, N.-Y.; Tung, H.-H.; Huang, H.-M.; Cheng, S.-F. The Lived Experiences of Stigmatization in the Process of HIV Status Disclosure among People Living with HIV in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 5089. https://doi.org/10.3390/ijerph18105089
Yu C-H, Huang C-Y, Ko N-Y, Tung H-H, Huang H-M, Cheng S-F. The Lived Experiences of Stigmatization in the Process of HIV Status Disclosure among People Living with HIV in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(10):5089. https://doi.org/10.3390/ijerph18105089
Chicago/Turabian StyleYu, Chia-Hui, Chu-Yu Huang, Nai-Ying Ko, Heng-Hsin Tung, Hui-Man Huang, and Su-Fen Cheng. 2021. "The Lived Experiences of Stigmatization in the Process of HIV Status Disclosure among People Living with HIV in Taiwan" International Journal of Environmental Research and Public Health 18, no. 10: 5089. https://doi.org/10.3390/ijerph18105089
APA StyleYu, C.-H., Huang, C.-Y., Ko, N.-Y., Tung, H.-H., Huang, H.-M., & Cheng, S.-F. (2021). The Lived Experiences of Stigmatization in the Process of HIV Status Disclosure among People Living with HIV in Taiwan. International Journal of Environmental Research and Public Health, 18(10), 5089. https://doi.org/10.3390/ijerph18105089