A Network Analysis of Research Topics and Trends in End-of-Life Care and Nursing


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Research Procedure
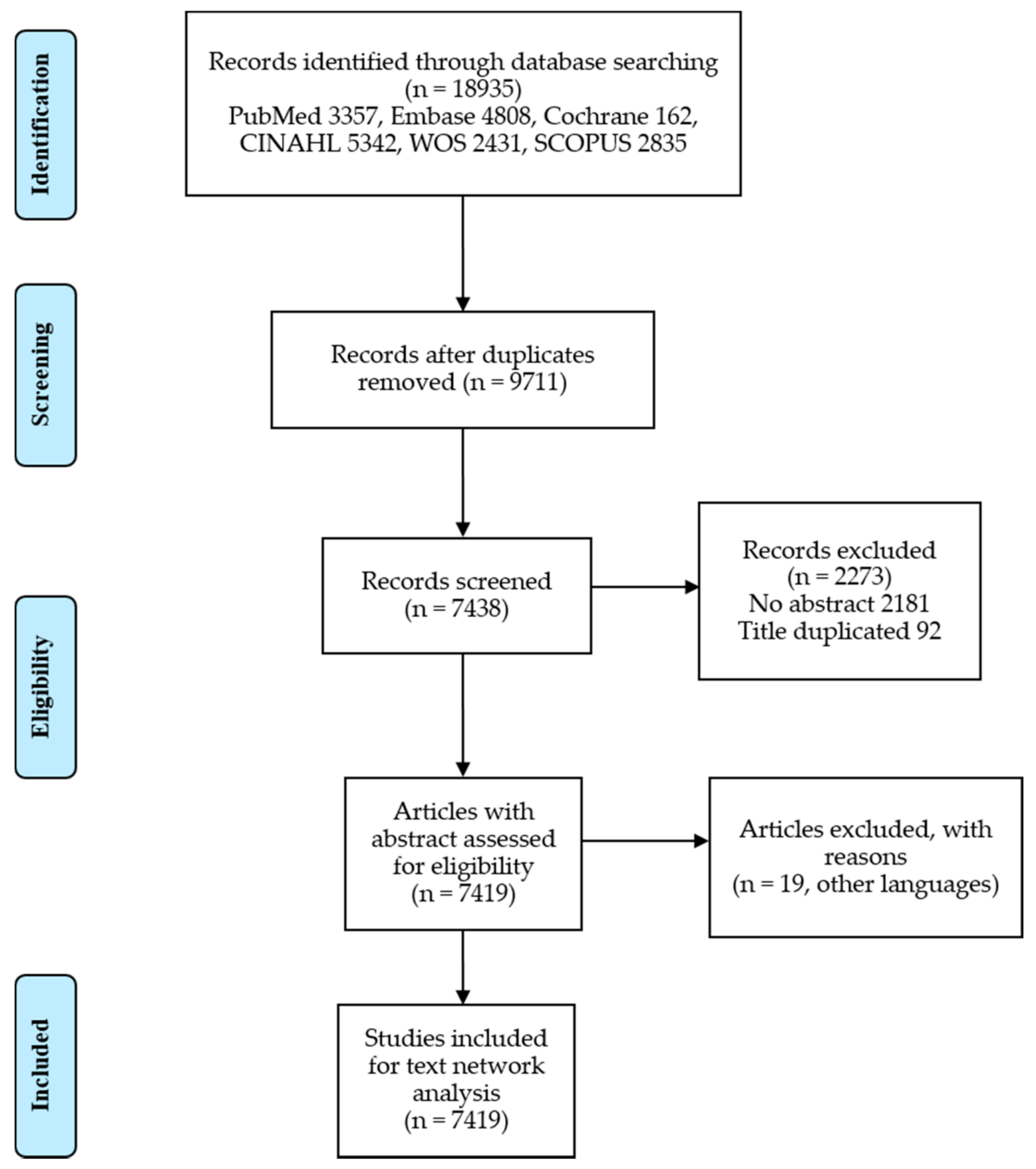
2.2. Process of Search and Selection
2.3. Keyword Extraction and Preprocessing of the Titles
2.4. Keyword Analysis
2.5. Topic Analysis
3. Results
3.1. Core Keywords that Emerged from the EOL Care Studies
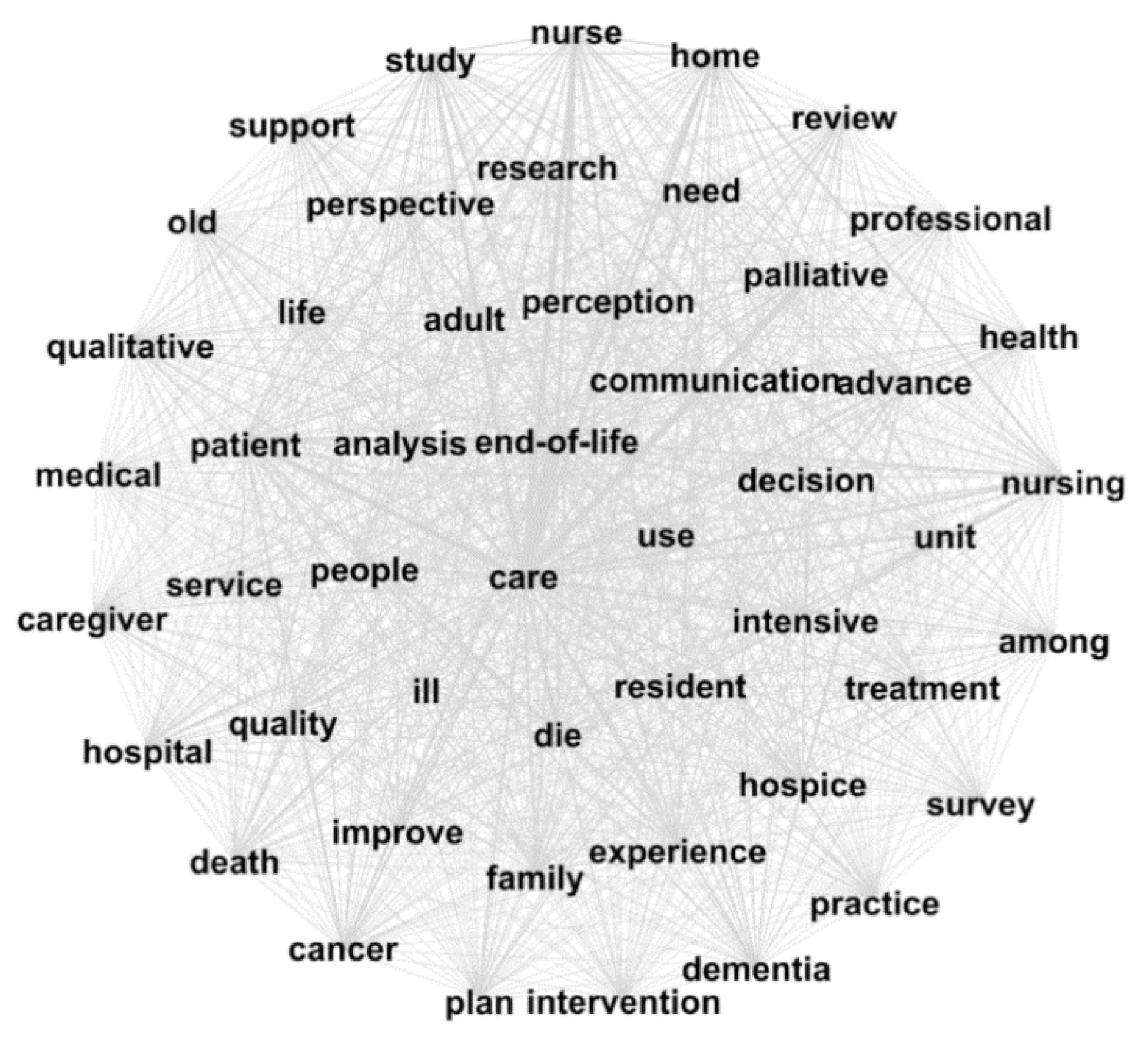
3.2. Semantic Network Analysis
3.3. Keywords by Five-Years Cycle
3.4. Frequency According to Contiguous Sequence Word Analysis of Research Titles
3.5. Topic Analysis of the Abstract
- Ethical problems of the decision to end the treatment: there are “decision,” “ethical,” “euthanasia,” “sedation,” and “withdrawal” in order of weight. Additionally, words such as “decision-making,” “suicide,” and “withhold” are topics related to patient self-determination, such as discontinuation of treatment. The subtopic of these words was interpreted as a study relating to ethical problems based on what the patient’s earlier statements, euthanasia, and suicide. There are still no clear answers to the problems associated with withdrawal or withholding life-sustaining treatment. Studies on ethical issues arising between the patient’s right to self-determination and the obligations of medical personnel are being conducted.
- Symptom management to improve the quality of life: among the top weight words, the word “cancer” was differentiated from other groups. There were also “symptom,” “quality,” “pain,” and “life”. Based on this, these are focused on pain interventions to improve the quality of life of cancer patients. Pain management is one of the important factors in EOL care. Especially, pain management for cancer patients is an important influence on the patient’s quality of life.
- Development of EOL knowledge education programs: this subtopic group contains words for education such as “student,” “practice,” “program,” and “knowledge.” Additionally, not only “student” but also “nurse” and “staff” were included, so the subject of education was not limited. It was interpreted as a study developing and researching education programs pertaining to life-sustaining treatment and palliative care for nurses and nursing students. With an increase in the demand for EOL care, the need for education programs for medical personnel is increasing. Consequently, it was confirmed that program development studies were in progress.
- Advanced care planning for older adults: “advance,” “preference,” “plan,” and “decision” are terms related to “ACP (advanced care plan)” and “AD” (advance directives). In particular, the subjects were limited to the elderly through the words “dementia” and “old.” This refers to writing an advanced directive and advanced care planning upon discussion with a physician (or resident) to reflect adult patients’ preferences and wishes. There are ethical problems related to older and dementia patients. Currently, many studies are being conducted on the life-sustaining treatment of elderly patients. There have been studies to focus on advance planning of care treatment in case of chronic diseases such as dementia.
- Home-based hospice: this subtopic shows the phrases “home,” “people,” “death,” and “place,” which is the place that people prefer. It could also be deduced from the words “community,” “support” that there are studies of home-based hospice in the community. Home, hospital, and community need to provide a place for care. In addition to hospital-based hospice services, home-based hospice services are provided. Studies on how to provide such services were conducted.
- Communication experiences: it was found that “patient,” “nurse,” and “family,” which refer to the subjects, took the top place, and the words “experience,” “interview,” and “communication” describe the communication with the subjects. These include interview studies to survey EOL communication experiences in patients, caregivers, and healthcare providers. It is important to understand the patient’s preferences in EOL treatment. Accordingly, studies on communication experiences and methods were performed.
- Survey of patient symptoms: there are words for the subject such as “patient,” “family,” “caregiver.” Additionally, words “symptom,” “pain,” “quality,” “questionnaire,” “score,” “survey,” “measure,” and “scale” imply the meaning of examining the subject’s symptoms such as pain and quality. Methods of surveying pain and symptoms in EOL patients include scoring, scales, and questionnaires. It may appear to be the same as “2. Symptom management to improve the quality of life,” but the focus here was on the research methods and tools to be used to investigate the symptoms.
- Analysis of considering patients’ preferences: after the high weight word “hospice,” there are the words “home,” “hospital,” “facility,” “day,” “year,” and “receive”. This was interpreted as representing studies in which patients conducted surveys on preferred (“likely”) places and schedules related to hospice or palliative care and confirmed CI (confidence interval). There are studies in which physicians provided EOL care after receiving information about the desired place (home, hospital, or institution) and date (day and year) of care from the patient. Studies have been conducted on whether checking and applying the patient’s preferences yields better results.
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Nursing and Health Policy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Health Service UK. What End of Life Care Involves. Available online: https://www.nhs.uk/conditions/end-of-life-care/what-it-involves-and-when-it-starts/ (accessed on 30 October 2020).
- Goode, D.; Black, P.; Lynch, J. Person-centred end-of-life curriculum design in adult pre-registration undergraduate nurse education: A three-year longitudinal evaluation study. Nurse Educ. Today 2019, 82, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Lunney, J.R.; Lynn, J.; Foley, D.J.; Lipson, S.; Guralnik, J.M. Patterns of Functional Decline at the End of Life. JAMA 2003, 289, 2387–2392. [Google Scholar] [CrossRef] [PubMed]
- Thorn, H.; Uhrenfeldt, L. Experiences of non-specialist nurses caring for patients and their significant others undergoing transitions during palliative end-of-life cancer care. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 1711–1746. [Google Scholar] [CrossRef] [PubMed]
- Nasu, K.; Konno, R.; Fukahori, H. End-of-life nursing care practice in long-term care settings for older adults: A qualitative systematic review. Int. J. Nurs. Pract. 2020, 26, e12771. [Google Scholar] [CrossRef] [PubMed]
- Stanyon, M.R.; Goldberg, S.E.; Astle, A.; Griffiths, A.; Gordon, A.L. The competencies of Registered Nurses working in care homes: A modified Delphi study. Age Ageing 2017, 46, 582–588. [Google Scholar] [CrossRef][Green Version]
- Dillworth, J.; Dickson, V.V.; Mueller, A.; Shuluk, J.; Yoon, H.W.; Capezuti, E. Nurses’ perspectives: Hospitalized older patients and end-of-life decision-making. Nurs. Crit. Care 2016, 21, e1–e11. [Google Scholar] [CrossRef]
- Zaman, S.; Inbadas, H.; Whitelaw, A.; Clark, D. Common or multiple futures for end of life care around the world? Ideas from the ‘waiting room of history’. Soc. Sci. Med. 2017, 172, 72–79. [Google Scholar] [CrossRef]
- Ji, Y.A.; Nam, S.; Kim, H.-G.; Lee, J.I.; Lee, S. Research topics and trends in medical education by social network analysis. BMC Med Educ. 2018, 18, 222. [Google Scholar] [CrossRef]
- Kwon, S.Y.; Bae, K.R. A Study on the Knowledge Structure of Cancer Survivors based on Social Network Analysis. J. Korean Acad. Nurs. 2016, 46, 50–58. [Google Scholar] [CrossRef]
- Min, H.S.; Kim, C.-Y. Exploratory Study of Publicness in Healthcare Sector through Text Network Analysis. Heal. Policy Manag. 2016, 26, 51–62. [Google Scholar] [CrossRef]
- Parnell, J.M.; Robinson, J.C. Social network analysis: Presenting an underused method for nursing research. J. Adv. Nurs. 2018, 74, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, R.; Wilson, A.; Reblin, M.; Clayton, M.F.; Ellington, L. Using Social Network Analysis to Investigate Positive EOL Communication. J. Pain Symptom Manag. 2018, 56, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S. Network Analysis Methods; Nonhyeong: Seoul, Korea, 2013; pp. 207–268. [Google Scholar]
- Blei, D.M. Probabilistic topic models. Commun. ACM 2012, 55, 77–84. [Google Scholar] [CrossRef]
- Kang, J.; Kim, S.; Roh, S. A Topic Modeling Analysis for Online News Article Comments on Nurses’ Workplace Bullying. J. Korean Acad. Nurs. 2019, 49, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Baek, Y. Text-Mining Using R.; Hanulmplus: Paju, Korea, 2017; pp. 13–235. [Google Scholar]
- Ryan, S.; Wong, J.; Chow, R.; Zimmermann, C. Evolving Definitions of Palliative Care: Upstream Migration or Confusion? Curr. Treat. Options Oncol. 2020, 21, 20. [Google Scholar] [CrossRef] [PubMed]
- Batstone, E.; Bailey, C.; Hallett, N. Spiritual care provision to end-of-life patients: A systematic literature review. J. Clin. Nurs. 2020, 29, 3609–3624. [Google Scholar] [CrossRef]
- Abu-Ghori, I.K.; Bodrick, M.M.; Hussain, R.; Rassool, G.H. Nurses’ involvement in end-of-life care of patients after a do not resuscitate decision on general medical units in Saudi Arabia. Intensiv. Crit. Care Nurs. 2016, 33, 21–29. [Google Scholar] [CrossRef]
- Shelkowitz, E.; Vessella, S.L.; O’Reilly, P.; Tucker, R.; Lechner, B.E. Counseling for personal care options at neonatal end of life: A quantitative and qualitative parent survey. BMC Palliat. Care 2015, 14, 1–11. [Google Scholar] [CrossRef]
- Hui, D.; Nooruddin, Z.I.; Didwaniya, N.; Dev, R.; De La Cruz, M.; Kim, S.H.; Kwon, J.H.; Hutchins, R.; Liem, C.; Bruera, E. Concepts and Definitions for “Actively Dying,” “End of Life,” “Terminally Ill,” “Terminal Care,” and “Transition of Care”: A Systematic Review. J. Pain Symptom Manag. 2014, 47, 77–89. [Google Scholar] [CrossRef]
- Sabatino, C.P. Death in the legislature: Inventing legal tools for autonomy. N. Y. Univ. Rev. Law Soc. Chang. 1991, 19, 309–339. [Google Scholar]
- Choi, E.K.; Hong, J.; Kim, M.S.; Keam, B.; Kim, M.; Heo, D.S.; Park, H.Y. The decision-making process regarding life-sustaining treatment in four countries: Taiwan, Japan, the US, and the UK. Korean J. Med. Eth. 2017, 20, 131–151. [Google Scholar]
- Scherer, Y.K.; Jezewski, M.A.; Graves, B.; Wu, Y.-W.B.; Bu, X. Advance directives and end-of-life decision making: Survey of critical care nurses’ knowledge, attitude, and experience. Crit. Care Nurse 2006, 26, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Efstathiou, N.; Clifford, C. The critical care nurse’s role in End-of-Life care: Issues and challenges. Nurs. Crit. Care 2011, 16, 116–123. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Palliative Care. Available online: https://www.who.int/news-room/fact-sheets/detail/palliative-care (accessed on 30 October 2020).
- National Hospice and Palliative Care Organization. Standards of Practice for Pediatric Hospice and Palliative Care Programs; National Hospice and Palliative Care: Alexandria, VA, USA, 2007; pp. 1–47. [Google Scholar]
- Kim, C.H.; Kim, M.S.; Shin, H.Y.; Song, I.G.; Moon, Y.J. How to Implement Quality Pediatric Palliative Care Services in South Korea: Lessons from Other Countries. Korean J. Hosp. Palliat. Care 2019, 22, 105–116. [Google Scholar] [CrossRef]
- Santos, P.R.; Júnior, J.R.F.G.C.; Filho, J.N.G.D.S.; Ferreira, T.P.; Oliveira, S.D.S. Religious coping methods predict depression and quality of life among end-stage renal disease patients undergoing hemodialysis: A cross-sectional study. BMC Nephrol. 2017, 18, 1–8. [Google Scholar] [CrossRef]
- Wilson, C.S.; Forchheimer, M.; Heinemann, A.W.; Warren, A.M.; McCullumsmith, C. Assessment of the relationship of spiritual well-being to depression and quality of life for persons with spinal cord injury. Disabil. Rehabil. 2016, 39, 491–496. [Google Scholar] [CrossRef]
- Chaar, E.A.; Hallit, S.; Hajj, A.; Aaraj, R.; Kattan, J.; Jabbour, H.; Khabbaz, L.R. Evaluating the impact of spirituality on the quality of life, anxiety, and depression among patients with cancer: An observational transversal study. Support. Care Cancer 2018, 26, 2581–2590. [Google Scholar] [CrossRef]
- Hirsch, H.L.; Donovan, R.E. The right to die: Medico-legal implications of in re Quinlan. Rutgers Law Rev. 1976, 30, 267–303. [Google Scholar]
- Zelaya, A. Cruzan v. Director, Missouri Department of Health. J. Contemp. Legal Issues 2004, 14, 313–321. [Google Scholar]
- Perry, J.E.; Churchill, L.R.; Kirshner, H.S. The Terri Schiavo Case: Legal, Ethical, and Medical Perspectives. Ann. Intern. Med. 2005, 143, 744–748. [Google Scholar] [CrossRef]
- Kim, M. The Problems and the Improvement Plan of the Hospice/Palliative Care and Dying Patient’s Decisions on Life-Sustaining Treatment Act. Korean J. Hosp. Palliat. Care 2018, 21, 1–8. [Google Scholar] [CrossRef]
- Zadeh, R.S.; Eshelman, P.; Setla, J.; Kennedy, L.; Hon, E.; Basara, A. Environmental Design for End-of-Life Care: An Integrative Review on Improving the Quality of Life and Managing Symptoms for Patients in Institutional Settings. J. Pain Symptom Manag. 2018, 55, 1018–1034. [Google Scholar] [CrossRef] [PubMed]
- Fleming, D.A.; Sheppard, V.B.; Mangan, P.A.; Taylor, K.L.; Tallarico, M.; Adams, I.; Ingham, J. Caregiving at the End of Life: Perceptions of Health Care Quality and Quality of Life Among Patients and Caregivers. J. Pain Symptom Manag. 2006, 31, 407–420. [Google Scholar] [CrossRef] [PubMed]
- Balboni, T.A.; Vanderwerker, L.C.; Block, S.D.; Paulk, M.E.; Lathan, C.S.; Peteet, J.R.; Prigerson, H.G. Religiousness and Spiritual Support Among Advanced Cancer Patients and Associations With End-of-Life Treatment Preferences and Quality of Life. J. Clin. Oncol. 2007, 25, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Connolly, M.; Perryman, J.; McKenna, Y.; Orford, J.; Thomson, L.; Shuttleworth, J.; Cocksedge, S. SAGE & THYME™: A model for training health and social care professionals in patient-focussed support. Patient Educ. Couns. 2010, 79, 87–93. [Google Scholar] [CrossRef]
- Greene, M.G.; Adelman, R.D. Physician–older patient communication about cancer. Patient Educ. Couns. 2003, 50, 55–60. [Google Scholar] [CrossRef]
- Barclay, J.S.; Blackhall, L.J.; Tulsky, J.A. Communication Strategies and Cultural Issues in the Delivery of Bad News. J. Palliat. Med. 2007, 10, 958–977. [Google Scholar] [CrossRef]
- Park, E.-J.; Kim, Y.; Park, C.S. A Comparison of Hospice Care Research Topics between Korea and Other Countries Using Text Network Analysis. J. Korean Acad. Nurs. 2017, 47, 600. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Source | Query | Result | |
|---|---|---|---|
| PubMed | #1 | “End-of-life care” [All Fields] AND (“nursing” [Subheading] OR “nursing” [All Fields] OR “nursing” [MeSH Terms]) | 3357 |
| Embase | #1 | end-of-life care’ AND (‘nursing’/de OR ‘nursing’ OR ‘nursing service’ OR ‘nursing service, hospital’ OR ‘nursing services’ OR ‘nursing support’ OR ‘nursing, private duty’ OR ‘nursing, supervisory’ OR ‘office nursing’ OR ‘private duty nursing’) | 4808 |
| Cochrane | #1 | End-of-life care | 553 |
| #2 | MeSH descriptor: [Nursing] explode all trees | 3192 | |
| #3 | nursing | 31,911 | |
| #4 | #2 OR #3 | 32,125 | |
| #5 | #1 AND #4 | 162 | |
| CINAHL (CINAHLHeadings) | #1 | “End-of-life care” | 16,884 |
| #2 | nursing | 657,389 | |
| #3 | #1 AND #2 | 5342 | |
| Web of Science | #1 | “End-of-life care” AND nursing | 2431 |
| Scopus | #1 | “End-of-life care” AND nursing | 2835 |
| Rank | Keyword | F | Keyword | Degree Centrality | Keyword | Betweenness Centrality |
|---|---|---|---|---|---|---|
| 1 | care | 5655 | care | 0.6991 | care | 0.2583 |
| 2 | end-of-life | 2973 | end-of-life | 0.5304 | end-of-life | 0.1253 |
| 3 | patient | 1503 | patient | 0.3948 | patient | 0.0620 |
| 4 | palliative | 1380 | palliative | 0.3647 | palliative | 0.0450 |
| 5 | nurse | 1329 | nurse | 0.3391 | nurse | 0.0404 |
| 6 | home | 990 | study | 0.3072 | study | 0.0319 |
| 7 | nursing | 914 | home | 0.2833 | nursing | 0.0308 |
| 8 | study | 907 | nursing | 0.2833 | die | 0.0308 |
| 9 | die | 775 | die | 0.2700 | death | 0.0258 |
| 10 | death | 664 | cancer | 0.2448 | home | 0.0246 |
| 11 | cancer | 645 | death | 0.2361 | cancer | 0.0170 |
| 12 | family | 619 | advance | 0.2079 | hospice | 0.0118 |
| 13 | advance | 579 | family | 0.2063 | family | 0.0112 |
| 14 | experience | 524 | experience | 0.1971 | experience | 0.0112 |
| 15 | dementia | 414 | use | 0.1867 | advance | 0.0107 |
| 16 | hospice | 396 | hospice | 0.1655 | use | 0.0097 |
| 17 | review | 393 | hospital | 0.1649 | hospital | 0.0076 |
| 18 | people | 388 | people | 0.1606 | qualitative | 0.0072 |
| 19 | use | 348 | life | 0.1568 | life | 0.0070 |
| 20 | hospital | 348 | among | 0.1548 | health | 0.0068 |
| 21 | intensive | 339 | review | 0.1541 | review | 0.0068 |
| 22 | quality | 335 | health | 0.1530 | practice | 0.0060 |
| 23 | unit | 334 | practice | 0.1521 | people | 0.0059 |
| 24 | practice | 322 | quality | 0.1515 | quality | 0.0053 |
| 25 | life | 287 | dementia | 0.1513 | dementia | 0.0052 |
| 26 | old | 282 | qualitative | 0.1437 | perspective | 0.0052 |
| 27 | health | 281 | unit | 0.1434 | among | 0.0050 |
| 28 | among | 280 | old | 0.1363 | support | 0.0047 |
| 29 | qualitative | 276 | survey | 0.1350 | old | 0.0043 |
| 30 | resident | 274 | intensive | 0.1346 | research | 0.0042 |
| Rank | Keywords (n = 2) | F | Keyword (n = 3) | F | |||
|---|---|---|---|---|---|---|---|
| 1 | end-of-life | care | 1829 | intensive | care | unit | 255 |
| 2 | palliative | care | 1071 | advance | care | plan | 197 |
| 3 | nursing | home | 390 | nursing | home | resident | 127 |
| 4 | intensive | care | 327 | palliative | end-of-life | care | 116 |
| 5 | care | unit | 293 | care | die | patient | 83 |
| 6 | advance | care | 234 | improve | end-of-life | care | 81 |
| 7 | care | plan | 227 | quality | end-of-life | care | 73 |
| 8 | cancer | patient | 214 | care | intensive | care | 61 |
| 9 | care | nurse | 194 | provide | end-of-life | care | 60 |
| 10 | care | die | 194 | care | nursing | home | 60 |
| 11 | qualitative | study | 176 | ill | cancer | patient | 59 |
| 12 | care | home | 171 | terminally | ill | cancer | 56 |
| 13 | terminally | ill | 167 | critical | care | nurse | 54 |
| 14 | home | resident | 160 | terminally | ill | patient | 52 |
| 15 | care | patient | 153 | end-of-life | care | intensive | 49 |
| 16 | die | patient | 149 | end-of-life | care | patient | 48 |
| 17 | critical | care | 141 | end-of-life | care | people | 47 |
| 18 | nurse | home | 140 | end-of-life | care | nursing | 42 |
| 19 | systematic | review | 137 | palliative | care | patient | 41 |
| 20 | palliative | end-of-life | 133 | long-term | care | facility | 40 |
| long-term | care | 133 | |||||
| Subtopic Groups | Keywords (Weight) |
|---|---|
| 1. Ethical problems of the decision to end the treatment | Decision (0.025), ethical (0.017), euthanasia (0.016), sedation (0.015), withdrawal (0.012), make (0.011), case (0.010), ethic (0.010), medical (0.009), practice (0.009), treatment (0.009), decision-making (0.008), suicide (0.007), process (0.007), request (0.007), patient (0.006), statement (0.006), physician (0.006), nurse (0.006), withhold (0.006) |
| 2. Symptom management to improve the quality of life | Patient (0.044), care (0.037), palliative (0.023), cancer (0.021), review (0.014), intervention (0.012), disease (0.011), symptom (0.010), quality (0.009), end-of-life (0.009), study (0.009), use (0.008), management (0.008), include (0.008), treatment (0.007), need (0.007), research (0.006), pain (0.006), life (0.006), identify (0.006) |
| 3. Development of EOL knowledge education programs | Care (0.060), palliative (0.021), end-of-life (0.021), nurse (0.021), nursing (0.015), education (0.013), student (0.010), practice (0.010), program (0.009), provide (0.009), knowledge (0.009), staff (0.007), improve (0.007), eol (0.007), use (0.007), need (0.006), research (0.006), include (0.006), educational (0.005), develop (0.005) |
| 4. Advanced care planning for older adults | Advance (0.036), dementia (0.031), preference (0.018), treatment (0.016), end-of-life (0.015), plan (0.015), patient (0.015), decision (0.015), ACP (0.014), directive (0.013), discussion (0.011), old (0.010), AD (0.008), make (0.007), wish (0.007), care (0.006), resident (0.006), physician (0.006), adult (0.006), people (0.006) |
| 5. Home-based hospice | Care (0.057), home (0.036), people (0.016), death (0.016), die (0.016), service (0.015), palliative (0.013), hospital (0.013), end-of-life (0.013), study (0.009), need (0.009), place (0.008), staff (0.008), health (0.008), resident (0.008), patient (0.008), community (0.007), support (0.007), nursing (0.007), carers (0.007) |
| 6. Communication experiences | Care (0.045), patient (0.024), nurse (0.024), family (0.020), end-of-life (0.017), die (0.010), experience (0.010), study (0.010), death (0.008), provide (0.008), use (0.007), need (0.007), professional (0.006), support (0.006), interview (0.006), member (0.005), practice (0.005), communication (0.005), health (0.005), research (0.005) |
| 7. Survey of patient symptoms | Patient (0.026), care (0.017), family (0.014), nurse (0.013), study (0.013), death (0.012), die (0.011), caregiver (0.011), symptom (0.010), pain (0.010), quality (0.010), use (0.009), result (0.008), questionnaire (0.008), cancer (0.008), score (0.008), survey (0.008), end-of-life (0.007), measure (0.007), scale (0.007) |
| 8. Analysis of considering patients’ preferences | Care (0.039), hospice (0.026), patient (0.025), home (0.018), resident (0.015), hospital (0.012), use (0.012), death (0.011), end-of-life (0.010), nursing (0.009), die (0.009), facility (0.008), day (0.008), year (0.007), study (0.007), CI (0.007), EOL (0.007), result (0.007), likely (0.006), receive (0.006) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Jang, S.G.; Lee, K.-S. A Network Analysis of Research Topics and Trends in End-of-Life Care and Nursing. Int. J. Environ. Res. Public Health 2021, 18, 313. https://doi.org/10.3390/ijerph18010313
Kim K, Jang SG, Lee K-S. A Network Analysis of Research Topics and Trends in End-of-Life Care and Nursing. International Journal of Environmental Research and Public Health. 2021; 18(1):313. https://doi.org/10.3390/ijerph18010313
Chicago/Turabian StyleKim, Kisook, Seung Gyeong Jang, and Ki-Seong Lee. 2021. "A Network Analysis of Research Topics and Trends in End-of-Life Care and Nursing" International Journal of Environmental Research and Public Health 18, no. 1: 313. https://doi.org/10.3390/ijerph18010313
APA StyleKim, K., Jang, S. G., & Lee, K.-S. (2021). A Network Analysis of Research Topics and Trends in End-of-Life Care and Nursing. International Journal of Environmental Research and Public Health, 18(1), 313. https://doi.org/10.3390/ijerph18010313