Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment of the Selected Studies
2.4. Population, Intervention, Comparison, and Outcome Data Extraction
2.5. Outcome Measures and Statistical Analysis
3. Results
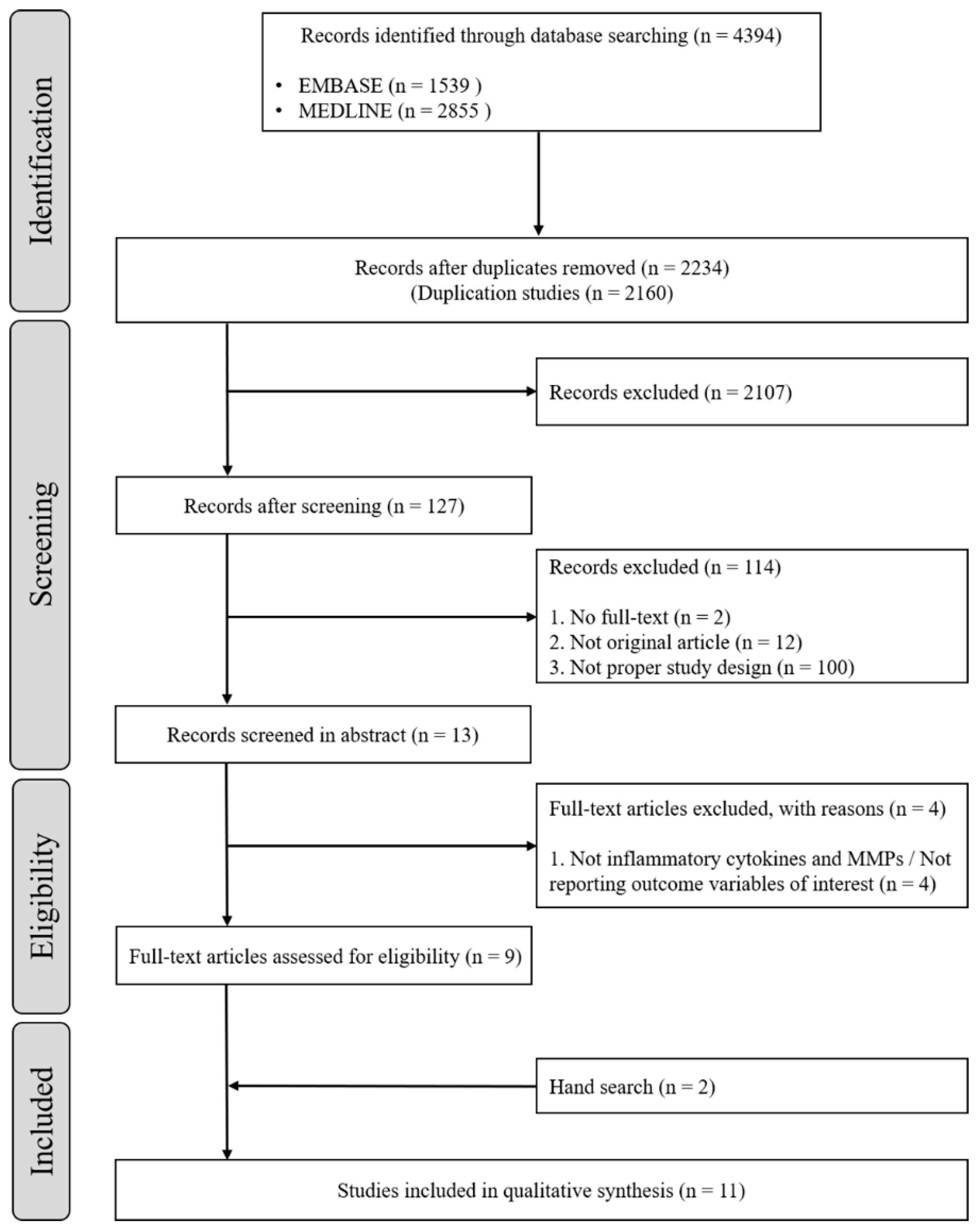
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Excluded Studies
3.4. Main Findings
3.5. Quality Assessment
3.6. Data Synthesis and Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Wei, L.; Borgnakke, W.S.; Thornton-Evans, G.; Zhang, X.; Lu, H.; McGuire, L.C.; Genco, R.J. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontology 2000, 72, 76–95. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html (accessed on 10 November 2020).
- Salminen, A.; Elisa Kopra, K.A.; Hyvärinen, K.; Paju, S.; Mäntylä, P.; Buhlin, K.; Nieminen, M.S.; Sinisalo, J.; Pussinen, P.J. Quantitative PCR analysis of salivary pathogen burden in periodontitis. Front. Cell. Infect. Microbiol. 2015, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Jokstad, A. The 2018 AAP/EFP classification of periodontal diseases, a focus on “risks” as a faux ami and language gone on holiday. Clin. Exp. Dent. Res. 2019, 5, 449. [Google Scholar] [CrossRef]
- Fortunato, L.; Bennardo, F.; Buffone, C.; Giudice, A. Is the application of platelet concentrates effective in the prevention and treatment of medication-related osteonecrosis of the jaw? A systematic review. J. Cranio-Maxillofacial Sur. 2020, 48, 268–285. [Google Scholar] [CrossRef]
- Giannobile, W.V.; McDevitt, J.T.; Niedbala, R.S.; Malamud, D. Translational and clinical applications of salivary diagnostics. Adv. Dent. Res. 2011, 23, 375–380. [Google Scholar] [CrossRef]
- Zhang, L.; Henson, B.S.; Camargo, P.M.; Wong, D.T. The clinical value of salivary biomarkers for periodontal disease. Periodontology 2000, 51, 25–37. [Google Scholar] [CrossRef]
- Kaufman, E.; Lamster, I.B. Analysis of saliva for periodontal diagnosis. J. Clin. Periodontol. 2000, 27, 453–465. [Google Scholar] [CrossRef]
- Isaza-Guzmán, D.M.; Cardona-Vélez, N.; Gaviria-Correa, D.E.; Martínez-Pabón, M.C.; Castaño-Granada, M.C.; Tobón-Arroyave, S.I. Association study between salivary levels of interferon (IFN)-gamma, interleukin (IL)-17, IL-21, and IL-22 with chronic periodontitis. Arch. Oral Biol. 2015, 60, 91–99. [Google Scholar] [CrossRef]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef]
- Da Costa, T.A.; Silva, M.J.B.; Alves, P.M.; Chica, J.E.L.; Barcelos, E.Z.; Giani, M.A.A.; Garlet, G.P.; da Silva, J.S.; Rodrigues Júnior, V.; Rodrigues, D.B.R.; et al. Inflammation biomarkers of advanced disease in nongingival tissues of chronic periodontitis patients. Mediators Inflamm. 2015, 2015, 983782. [Google Scholar] [CrossRef] [PubMed]
- Izadi Borujeni, S.; Mayer, M.; Eickholz, P. Activated matrix metalloproteinase-8 in saliva as diagnostic test for periodontal disease? A case–control study. Med. Microbiol. Immunol. 2015, 204, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Hernández-Ríos, P.A.; Gamonal, J.A.; Tervahartiala, T.; Brignardello-Petersen, R.; Mantyla, P.; Sorsa, T.; Hernández, M. Matrix metalloproteinases and myeloperoxidase in gingival crevicular fluid provide site-specific diagnostic value for chronic periodontitis. J. Clin. Periodontol. 2014, 41, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Sorsa, T.; Kallio, M.A.; Tervahartiala, T.; Emingil, G.; Han, B.; Mäntylä, P. The utility of gingival crevicular fluid matrix metalloproteinase-8 response patterns in prediction of site-level clinical treatment outcome. J. Periodontol. 2015, 86, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; De Sousa, T.S.; Taba, M.; Teofilo, J.M.; Jacob-Ferreira, A.L.B.; Tanus-Santos, J.E.; Novaes, A.B.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Mäntylä, P.; Tervahartiala, T.; Pussinen, P.J.; Gamonal, J.; Hernandez, M. MMP activation in diagnostics of periodontitis and systemic inflammation. J. Clin. Periodontol. 2011, 38, 817–819. [Google Scholar] [CrossRef]
- Booth, V.; Young, S.; Cruchley, A.; Taichman, N.S.; Paleolog, E. Vascular endothelial growth factor in human periodontal disease. J. Periodontal Res. 1998, 33, 491–499. [Google Scholar] [CrossRef]
- Rudrakshi, C.; Srinivas, N.; Mehta, D.S. A comparative evaluation of hepatocyte growth factor levels in gingival crevicular fluid and saliva and its correlation with clinical parameters in patients with and without chronic periodontitis: A clinico-biochemical study. J. Indian Soc. Periodontol. 2011, 15, 147–151. [Google Scholar] [CrossRef]
- Sánchez, G.A.; Miozza, V.A.; Delgado, A.; Busch, L. Salivary IL-1β and PGE2 as biomarkers of periodontal status, before and after periodontal treatment. J. Clin. Periodontol. 2013, 40, 1112–1117. [Google Scholar] [CrossRef]
- Yang, X.; Chen, L.; Yaping, P. The influences of periodontal status and periodontal pathogen quantity on salivary 8-hydroxydeoxyguanosine and interleukin-17 levels. J. Periodontol. 2016, 87, 591–600. [Google Scholar] [CrossRef]
- Sexton, W.M.; Lin, Y.; Kryscio, R.J.; Dawson, D.R., 3rd; Ebersole, J.L.; Miller, C.S. Salivary biomarkers of periodontal disease in response to treatment. J. Clin. Periodontol. 2011, 38, 434–441. [Google Scholar] [CrossRef]
- Öngöz Dede, F.; Balli, U.; Bozkurt Doğan, Ş.; Güven, B. Interleukin-32 levels in gingival crevicular fluid and saliva of patients with chronic periodontitis after periodontal treatment. J. Periodontal Res. 2017, 52, 397–407. [Google Scholar] [CrossRef]
- Kaushik, R.; Yeltiwar, R.K.; Pushpanshu, K. Salivary interleukin-1β levels in patients with chronic periodontitis before and after periodontal phase I therapy and healthy controls: A case-control study. J. Periodontol. 2011, 82, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Prakasam, S.; Srinivasan, M. Evaluation of salivary biomarker profiles following non-surgical management of chronic periodontitis. Oral Dis. 2014, 20, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Rangbulla, V.; Nirola, A.; Gupta, M.; Batra, P.; Gupta, M. Salivary IgA, Interleukin-1β and MMP-8 as Salivary Biomarkers in Chronic Periodontitis Patients. Chin. J. Dent. Res. 2017, 20, 43–51. [Google Scholar] [CrossRef]
- Shyu, K.G.; Choy, C.S.; Wang, D.C.L.; Huang, W.C.; Chen, S.Y.; Chen, C.H.; Lin, C.T.; Chang, C.C.; Huang, Y.K. Change of scaling-induced proinflammatory cytokine on the clinical efficacy of periodontitis treatment. Sci. World J. 2015, 2015, 289647. [Google Scholar] [CrossRef] [PubMed]
- Kinney, J.S.; Morelli, T.; Braun, T.; Ramseier, C.A.; Herr, A.E.; Sugai, J.V.; Shelburne, C.E.; Rayburn, L.A.; Singh, A.K.; Giannobile, W.V. Saliva/pathogen biomarker signatures and periodontal disease progression. J. Dent. Res. 2011, 90, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Meschiari, C.A.; Marcaccini, A.M.; Santos Moura, B.C.; Zuardi, L.R.; Tanus-Santos, J.E.; Gerlach, R.F. Salivary MMPs, TIMPs, and MPO levels in periodontal disease patients and controls. Clin. Chim. Acta 2013, 421, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; Manzano-Moreno, F.J.; Ruiz, C.; Illescas-Montes, R. Molecular Sciences Salivary Biomarkers and Their Application in the Diagnosis and Monitoring of the Most Common Oral Pathologies. Int. J. Mol. Sci. 2020, 21, 51–73. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Reeves, B.C.; Deeks, J.J.; Higgins, J.P.; Shea, B.; Tugwell, P.; Wells, G.A. Including non-randomized studies on intervention effects. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 595–620. [Google Scholar]
- Yoshie, H.; Tai, H.; Kobayashi, T.; Oda-Gou, E.; Nomura, Y.; Numabe, Y.; Ito, K.; Kurihara, H.; Kamoi, K. Salivary enzyme levels after scaling and interleukin-1 genotypes in Japanese patients with chronic periodontitis. J. Periodontol. 2007, 78, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Todorovic, T.; Dozic, I.; Barrero, M.V.; Ljuskovic, B.; Pejovic, J.; Marjanovic, M.; Knezevic, M. Salivary enzymes and periodontal disease. Medicina Oral Patología Oral y Cirugía Bucal. Ed. Inglesa 2006, 11, 4. [Google Scholar]
- Ersin Kalkan, R.; Öngöz Dede, F.; Gökmenoğlu, C.; Kara, C. Salivary fetuin-A, S100A12, and high-sensitivity C-reactive protein levels in periodontal diseases. Oral Dis. 2018, 24, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Kurgan, Ş.; Önder, C.; Altıngöz, S.M.; Bağış, N.; Uyanık, M.; Serdar, M.A.; Kantarcı, A. High sensitivity detection of salivary 8-hydroxy deoxyguanosine levels in patients with chronic periodontitis. J. Periodontal Res. 2015, 50, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Haigh, B.J.; Stewart, K.W.; Whelan, J.R.; Barnett, M.P.; Smolenski, G.A.; Wheeler, T.T. Alterations in the salivary proteome associated with periodontitis. J. Clin. Periodontol. 2010, 37, 241–247. [Google Scholar] [CrossRef]
- Ramseier, C.A.; Kinney, J.S.; Herr, A.E.; Braun, T.; Sugai, J.V.; Shelburne, C.A.; Rayburn, L.A.; Tran, H.M.; Singh, A.K.; Giannobile, W. V Identification of pathogen and host-response markers correlated with periodontal disease. J. Periodontol. 2009, 80, 436–446. [Google Scholar] [CrossRef]
- Polimeni, G.; Xiropaidis, A.V.; Wikesjo, U.M.E. Biology and principles of periodontal wound healing/regeneration. Periodontology 2000 2006, 41, 30–47. [Google Scholar] [CrossRef]
- Arias-Bujanda, N.; Regueira-Iglesias, A.; Balsa-Castro, C.; Nibali, L.; Donos, N.; Tomás, I. Accuracy of single molecular biomarkers in saliva for the diagnosis of periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 2–18. [Google Scholar] [CrossRef]
- Miller, C.S.; King, C.P.J.; Langub, M.C.; Kryscio, R.J.; Thomas, M. V Salivary biomarkers of existing periodontal disease: A cross-sectional study. J. Am. Dent. Assoc. 2006, 137, 322–329. [Google Scholar] [CrossRef]
- Fine, D.H.; Markowitz, K.; Furgang, D.; Fairlie, K.; Ferrandiz, J.; Nasri, C.; McKiernan, M.; Donnelly, R.; Gunsolley, J. Macrophage inflammatory protein-1α: A salivary biomarker of bone loss in a longitudinal cohort study of children at risk for aggressive periodontal disease? J. Periodontol. 2009, 80, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Cochran, D.D.T.G.D. The Contribution of Interleukin-1 and Tumor Necrosis Factor to Periodontal Tissue Destruction; Wiley: Hoboken, NJ, USA, 2003; Volume 74, pp. 391–401. [Google Scholar]
- Franco, C.; Patricia, H.-R.; Timo, S.; Claudia, B.; Marcela, H. Matrix metalloproteinases as regulators of periodontal inflammation. Int. J. Mol. Sci. 2017, 18, 240. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, X.; Yan, H.; Huang, L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e9642. [Google Scholar] [CrossRef] [PubMed]
- Michalowicz, B.S.; Novak, M.J.; Hodges, J.S.; DiAngelis, A.; Buchanan, W.; Papapanou, P.N.; Mitchell, D.A.; Ferguson, J.E.; Lupo, V.; Bofill, J.; et al. Serum inflammatory mediators in pregnancy: Changes after periodontal treatment and association with pregnancy outcomes. J. Periodontol. 2009, 80, 1731–1741. [Google Scholar] [CrossRef]
- Behle, J.H.; Sedaghatfar, M.H.; Demmer, R.T.; Wolf, D.L.; Celenti, R.; Kebschull, M.; Belusko, P.B.; Herrera-Abreu, M.; Lalla, E.; Papapanou, P.N. Heterogeneity of systemic inflammatory responses to periodontal therapy. J. Clin. Periodontol. 2009, 36, 287–294. [Google Scholar] [CrossRef]
- De Lima, C.L.; Acevedo, A.C.; Grisi, D.C.; Taba, M.; Guerra, E.; De Luca Canto, G. Host-derived salivary biomarkers in diagnosing periodontal disease: Systematic review and meta-analysis. J. Clin. Periodontol. 2016, 43, 492–502. [Google Scholar] [CrossRef]
- Zwahlen, R.; Walz, A.; Rot, A. In vitro and in vivo activity and pathophysiology of human interleukin-8 and related peptides. Academic Press. Int. Rev. Exp. Pathol. 1993, 34, 27–42. [Google Scholar]
- Cheng, W.C.; Hughes, F.J.; Taams, L.S. The presence, function and regulation of IL-17 and Th17 cells in periodontitis. J. Clin. Periodontol. 2014, 41, 541–549. [Google Scholar] [CrossRef]
- Frodge, B.D.; Ebersole, J.L.; Kryscio, R.J.; Thomas, M.V.; Miller, C.S. Bone remodeling biomarkers of periodontal disease in saliva. J. Periodontol. 2008, 79, 1913–1919. [Google Scholar] [CrossRef]
- Goutoudi, P.; Diza, E.; Arvanitidou, M. Effect of periodontal therapy on crevicular fluid interleukin-1β and interleukin-10 levels in chronic periodontitis. J. Dent. 2004, 32, 511–520. [Google Scholar] [CrossRef]
- Moon, Y.M.; Yoon, B.Y.; Her, Y.M.; Oh, H.J.; Lee, J.S.; Kim, K.W.; Lee, S.J.; Woo, Y.J.; Park, K.S.; Park, S.H.; et al. IL-32 and IL-17 interact and have the potential to aggravate osteoclastogenesis in rheumatoid arthritis. Arthritis Res. Ther. 2012, 14, R246. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.S.; Foley, J.D.; Bailey, A.L.; Campell, C.L.; Humphries, R.L.; Christodoulides, N.; Redding, S.W. Current developments in salivary diagnostics. Biomark. Med. 2010, 4, 171–189. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Participant Characteristics | |
|---|---|---|
| Patient Group | Control Group | |
| Yoshie et al. (2007) [34] |
| N/A |
| Sexton et al. (2011) [22] |
| |
| <Criteria for periodontal disease> | ||
| ||
| Kinney et al. (2011) [28] |
| |
| <Criteria for periodontitis> | <Criteria for periodontal health and gingivitis> | |
|
| |
| Kaushik et al. (2011) [24] |
| |
| <Criteria for periodontitis> | <Criteria for periodontal health> | |
|
| |
| Sánchez et al. (2013) [20] |
| |
| <Criteria for periodontitis> | <Criteria for periodontal health> | |
|
| |
| Meschiari et al. (2013) [29] |
| |
| <Criteria for periodontal disease> | <Criteria for periodontal health> | |
|
| |
| Prakasam et al. (2014) [25] |
| |
| <Criteria for chronic periodontitis> | <Criteria for periodontal health>. | |
|
| |
| Shyu et al. (2015) [27] |
| N/A |
| <Criteria for chronic periodontitis> | ||
| ||
| Yang et al. (2016) [21] |
| |
| <Criteria for chronic periodontitis> | <Criteria for periodontal health> | |
|
| |
| Öngöz et al. (2017) [23] |
| |
| <Criteria for chronic periodontitis> | <Criteria for periodontal health> | |
|
| |
| Rangbulla et al. (2017) [26] | <periodontitis criteria> | <Criteria for periodontal health> |
|
| |
| Author (year) | Patient Group | Control Group | Sample Collection | Inflammatory Cytokines | Main Findings | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years; Mean ± SD) | N (Male/Female) | Treatment | Period (Saliva Sampling after Treatment) | Age (years; Mean ± SD) | N (Male/Female) | Treatment | Period (Saliva Sampling after Treatment) | ||||
| Yoshie et al. (2007) [34] | CP: 55.1 ± 2.0 | 49 (24/25) | SRP | At baseline and 4 weeks | N/A | N/A | N/A | N/A | SWS | IL-1 | IL-1A allele 2 non-carriers displayed a significant decrease in salivary AST and ALT levels; the carriers did not show any changes in the salivary levels of the enzymes after scaling. |
| Sexton et al. (2011) [22] | CP: 40.3 ± 10.0 | 35 (26/9) | SRP and OHI | At 0, 16, and 28 weeks | CP: 47.3 ± 8.8 | 33 (21/12) | OHI | At week 0, 16 and 28 | UWS | IL-1β, IL-8, MMP-8, MIP-1α, and TNF-α | Baseline TNF-α levels changed significantly at both follow-up visits (16 and 28 weeks), regardless of the treatment group. IL-1β and MMP-8 levels decreased significantly from baseline (p < 0.04) in the SRP group only. MMP-8 and MIP-1α levels were significantly reduced in comparison with those in the non-responders to treatment (p = 0.01, 0.05 respectively). In receiver-operating characteristic analyses, MMP-8 produced the highest area under the curve (≥0.7; p = 0.01). |
| Kinney et al. (2011) [28] | Mild CP: 54; Moderate to severe CP: 50 | Mild: 24 (11/13); Modertate to Severe: 20 (7/13) | SRP and OHI | Bi-monthly over a 12-month period | Periodontally-healthy: 46 Gingivitis: 46 | Periodontally-healthy: 15(9/6) Gingivitis: 24(10/14) | Prophylaxis and OHI | Bi-monthly over a 12-month period | UWS | IL-1β, MMP-8, and MMP-9 | Moderate to severe periodontitis patients demonstrated reduction of MMP-8, MMP-9, and IL-1β at 12 months in comparison with baseline (p < 0.05). |
| Kaushik et al. (2011) [24] | Moderate-to-severe CP: 34.9 ± 6.4 | 28 (8/20) | SRP and OHI | Before and 1 month | Periodontally-healthy: 33.6 ± 4.1 | 24 (9/15) | No treatment | Before and 1 month | UWS | IL-1β | IL-1β levels in periodontitis patients reduced significantly post-treatment but were still significantly higher than the baseline values of controls. IL-1β showed a significant positive correlation with percentage probing depth, bleeding on probing, gingival index, and periodontal index. |
| Sánchez et al. (2013) [20] | Mild periodontitis: 38.3 Moderate periodontitis: 41.6 Severe periodontitis: 46.8 | Mild 18 (14/4) Moderate 21 (17/4) Severe 20 (14/6) | SRP and OHI | At 3 months | Periodontally-healthy: 34.3 | 15 (10/5) | OHI | At 3 months | UWS | IL-1β and PGE2 | IL-1β and PGE2 levels reduced significantly post-treatment. With a selected threshold of 212 pg/mL, salivary IL1-β predicted periodontitis with 78% sensitivity and 100% specificity. With a selected threshold of 121 pg/mL, salivary PGE2 predicted periodontitis with 78% sensitivity and 91% specificity. |
| Meschiari et al. (2013) [29] | None | 19 (none) | SRP | Before and after 3 months of treatment | Periodontally-healthy: none | 11 (none) | OHI and prophylaxis | Before and after 3 months of treatment | SWS | MMP-8 and TIMP-2 | MMP-8 and TIMP-2 baseline concentrations in the periodontal group were significantly higher than those in the controls, but their concentrations decreased after non-surgical therapy. |
| Prakasam et al. (2014) [25] | Moderate to severe CP: 40.80 ± 10.07 | 18 (9/9) | SRP | At 1 and 6 weeks | Periodontally-healthy: 28.00 ± 2.94 | 18 (10/8) | Prophylaxis | Approximately 1–2 weeks | UWS | IL-4, IL-6, IL-10, and IL-17 | IL-4 and IL-6 levels were significantly higher and IL-10 and IL-17 levels were significantly lower in chronic periodontitis patients in comparison with healthy controls. IL-4 levels were lower at 6 weeks post-SRP. IL-6 and -17 levels did not change post-SRP. IL-10 levels were significantly higher at 6 weeks post-SRP. |
| Shyu et al. (2015) [27] | CP Nonprogress (NP) treatment group: 61.5 Effective treatment (ET) group: 56.0 | NP group 12 (5/7) ET group 10 (4/6) | Scaling | Before and after scaling | N/A | N/A | N/A | N/A | UWS | IL-1α, 1β, 6, 8, TNF-α, and β | Baseline IL-1α and scaling-stimulated IL-1α showed a positive correlation (r = 0.66 and p < 0.01). Baseline IL-1β and scaling-stimulated IL-1β also showed a positive correlation (r = 0.44 and p = 0.04). Scaling-stimulated IL-6 was significantly correlated with baseline IL-1α, IL-1β, IL-6, and TNF-α. The differences in IL-1α, IL-6, and IL-8 were significantly higher in the ET group than in the NP group. |
| Yang et al. (2016) [21] | CP: 36.593 ± 11.502 | 45 (19/26) | SRP and OHI | At baseline and at 1 and 3 months | Periodontally-healthy: 35.827 ± 8.012 | 47 (19/28) | No treatment | N/A | UWS | IL-17 | IL-17 levels significantly reduced post-treatment in comparison with the baseline (before treatment) levels, especially at 3 months than at 1 month after treatment. |
| Öngöz et al. (2017) [23] | Mild to moderate CP: 39.44 ± 3.15 | 27 (14/13) | SRP | Before and at 4 weeks | Periodontally-healthy: 37.30 ± 3.80 | 27 (12/15) | No treatment | Before assessment | UWS | IL-10, IL-32, and TNF-α | TNF-a and IL-32 levels in the periodontitis group were significantly lower after treatment compared with the baseline levels, but IL-10 levels were significantly higher. |
| Rangbulla et al. (2017) [26] | Moderate to severe CP: none | 30 (none) | SRP and OHI | Before and 12 weeks | Periodontally-healthy: none | 20 (none) | SRP and OHI | Before and 12 weeks | UWS | IL-1β and MMP-8 | IL-1β and MMP-8 levels in periodontitis patients reduced significantly after oral prophylaxis, but were still significantly higher than the baseline values of controls. |
| Authors (Year) | Confounding Bias | Selection Bias | Classification Bias | Intervention Bias | Missing Data Bias | Measurement Bias | Reporting Bias | Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Yoshie et al. (2007) [34] | PN | N | N | N | N | N | N | Low |
| Sexton et al. (2011) [22] | N | N | N | PN | UN | N | N | Low |
| Kinney et al. (2011) [28] | N | N | N | PN | N | N | N | Low |
| Kaushik et al. (2011) [24] | N | N | N | PN | N | N | N | Low |
| Sánchez et al. (2013) [20] | UN | N | N | PY | UN | N | N | Moderate |
| Meschiari et al. (2013) [29] | UN | N | N | PN | PN | N | N | Moderate |
| Prakasam et al. (2014) [25] | PN | N | N | N | N | N | N | Low |
| Shyu et al. (2015) [27] | N | N | N | N | N | N | N | Low |
| Yang et al. (2016) [21] | N | N | N | N | N | N | PY | Low |
| Öngöz et al. (2017) [23] | N | N | N | PN | N | N | N | Low |
| Rangbulla et al. (2017) [26] | PN | N | N | N | UN | N | N | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-Y.; Kim, H.-N. Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 194. https://doi.org/10.3390/ijerph18010194
Kim J-Y, Kim H-N. Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(1):194. https://doi.org/10.3390/ijerph18010194
Chicago/Turabian StyleKim, Ji-Youn, and Han-Na Kim. 2021. "Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 1: 194. https://doi.org/10.3390/ijerph18010194
APA StyleKim, J.-Y., & Kim, H.-N. (2021). Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(1), 194. https://doi.org/10.3390/ijerph18010194