Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Body Weight, BMI, and Obesity Measurements
2.3. Measurements of Cardiorespiratory Performance
2.4. Measurements of Muscle Performance
2.5. Statistical Analysis
3. Results from Gender within-Groups Analyses
3.1. Changes in the BMI-for-Age during the 4 Years
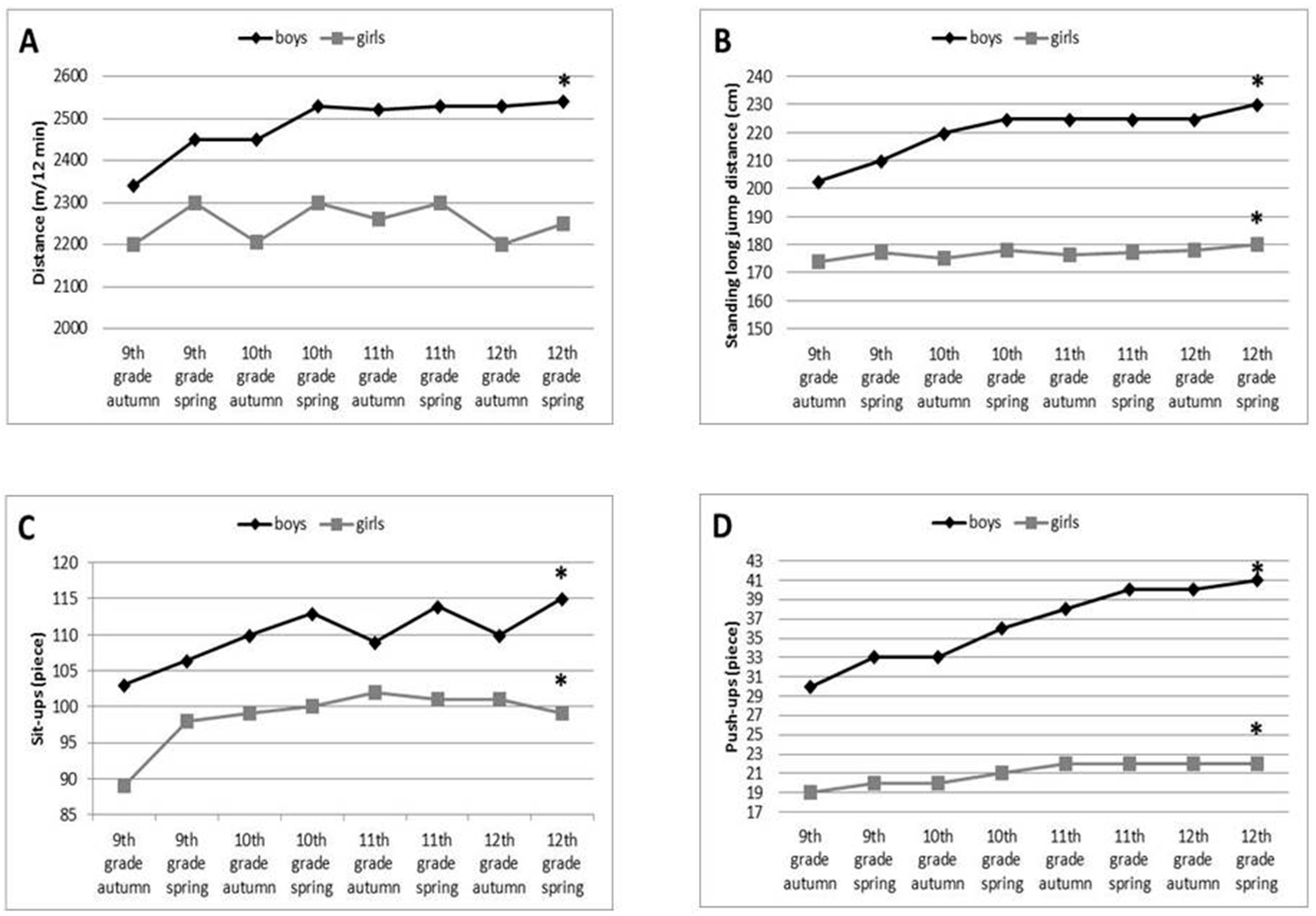
3.1.1. Cardiorespiratory Performance of Boys and Girls during the 4 Years
3.1.2. Muscle Performances of Boys and Girls during the Four Years
3.2. Results from between-Weight-Groups Analyses
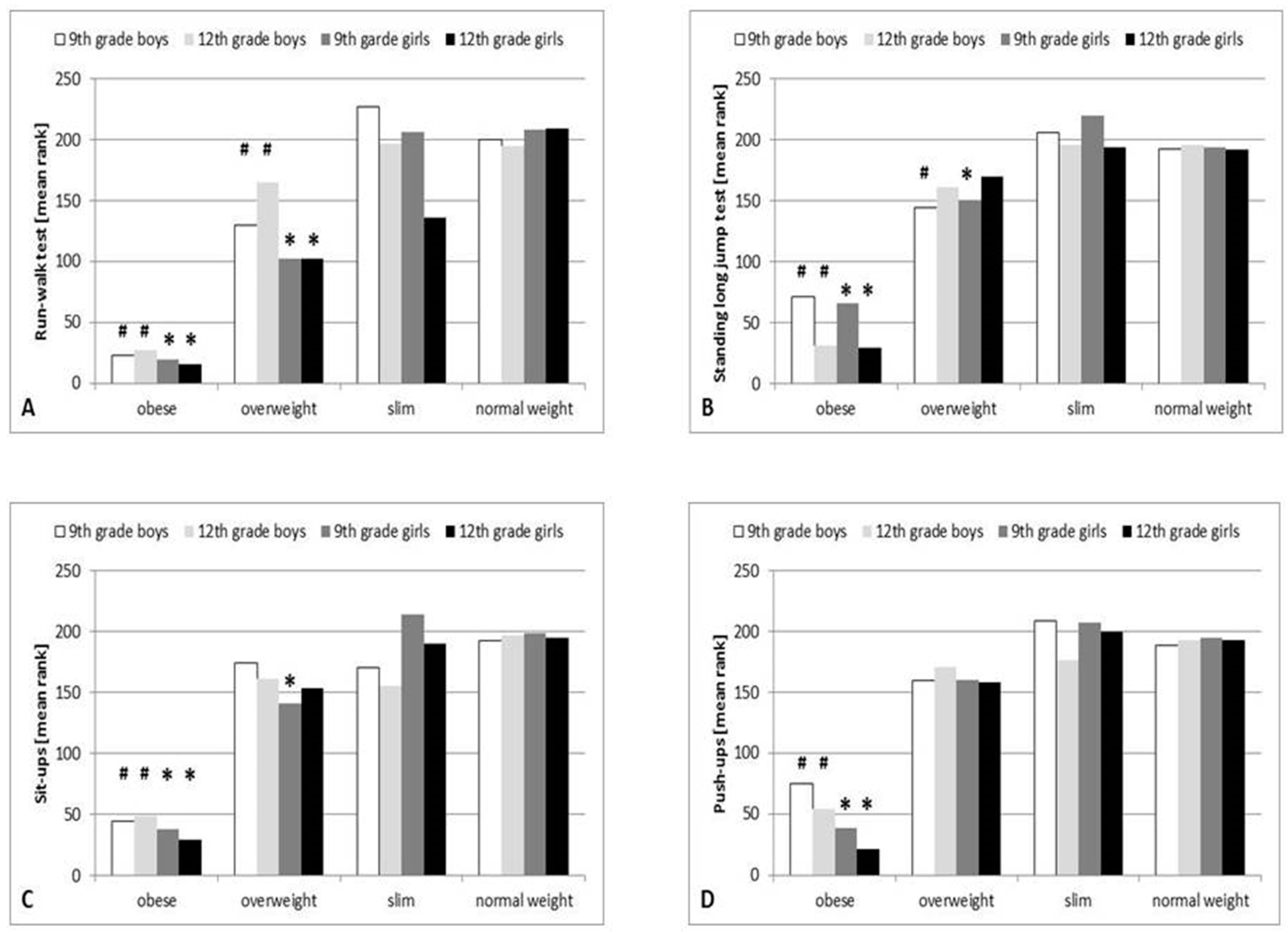
3.2.1. Association between Obesity and Overweight and Lower Limb Performance
3.2.2. Association between Obesity and Overweight and Hip Flexor and Abdominal Muscle Performance
3.2.3. Association between Obesity and Overweight and Shoulder and Arm Muscle Performance
3.3. Regression Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; NCHS Data Brief: Hyattsville, MD, USA, 2017; pp. 1–8.
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T. Long-term effects of adolescent obesity: Time to act. Nat. Rev. Endocrinol. 2018, 14, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Twig, G.; Tirosh, A.; Leiba, A.; Levine, H.; Shor, D.B.-A.; Derazne, E.; Haklai, Z.; Goldberger, N.; Kasher-Meron, M.; Yifrach, D.; et al. BMI at age 17 years and diabetes mortality in midlife: A nationwide cohort of 2.3. million adolescents. Diabetes Care 2016, 39, 1996–2003. [Google Scholar] [CrossRef]
- Andersen, L.B.; Harro, M.; Sardinha, L.B.; Froberg, K.; Ekelund, U.; Brage, S.; Anderssen, S.A. Physical activity and clustered cardiovascular risk in children: A cross-sectional study (The European Youth Heart Study). Lancet 2006, 368, 299–304. [Google Scholar] [CrossRef]
- Grøntved, A.; Ried-Larsen, M.; Møller, N.C.; Kristensen, P.L.; Froberg, K.; Brage, S.; Andersen, L.B. Muscle strength in youth and cardiovascular risk in young adulthood (the European Youth Heart Study). Br. J. Sports Med. 2015, 49, 90–94. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Qi, X.; Locke, J.; Rehman, S. Childhood and Adolescent Obesity in the United States: A Public Health Concern. Glob. Pediatr. Health 2019, 6, 2333794X19891305. [Google Scholar] [CrossRef]
- Lee, E.Y.; Yoon, K.H. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. (Lond.) 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Twig, G.; Yaniv, G.; Levine, H.; Leiba, A.; Goldberger, N.; Derazne, E.; Shor, D.B.-A.; Tzur, D.; Afek, A.; Shamiss, A.; et al. Body-Mass Index in 2.3 Million Adolescents and Cardiovascular Death in Adulthood. N. Engl. J. Med. 2016, 374, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008; U.S. Department of Health and Human Services: Washington, DC, USA, 2008.
- Cao, M.; Quan, M.; Zhuang, J. Effect of High-Intensity Interval Training versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Children and Adolescents: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1533. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Léger, L.A.; Olds, T.S.; Cazorla, G. Secular trends in the performance of children and adolescents (1980–2000): An analysis of 55 studies of the 20m shuttle run test in 11 countries. Sports Med. 2003, 33, 285–300. [Google Scholar] [CrossRef]
- Brage, S.; Wedderkopp, N.; Ekelund, U.; Franks, P.W.; Wareham, N.J.; Andersen, L.B.; Froberg, K. Features of the metabolic syndrome are associated with objectively measured physical activity and fitness in children: The European Youth Heart Study (EYHS). Diabetes Care 2004, 27, 2141–2148. [Google Scholar] [CrossRef]
- Fryar, C.D.; Carroll, M.D.; Ogden, C.L. Prevalence of Obesity among Children and Adolescents: United States, Trends 1963–1965 through 2009–2010; National Center for Health Statistics: Hyattsville, MD, USA, 2012.
- Livingstone, B. Epidemiology of childhood obesity in Europe. Eur. J. Pediatr. 2000, 159 (Suppl. 1), S14–S34. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Rizzo, N.S.; Hurtig-Wennlöf, A.; Ortega, F.B.; Wärnberg, J.; Sjöström, M. Relations of total physical activity and intensity to fitness and fatness in children: The European Youth Heart Study. Am. J. Clin. Nutr. 2006, 84, 299–303. [Google Scholar] [CrossRef]
- Thomas, N.E.; Baker, J.S.; Davies, B. Established and recently identified coronary heart disease risk factors in young people: The influence of physical activity and physical fitness. Sports Med. 2003, 33, 633–650. [Google Scholar] [CrossRef]
- Platat, C.; Wagner, A.; Klumpp, T.; Schweitzer, B.; Simon, C. Relationship of physical activity with metabolic syndrome features and low-grade inflammation in adolescents. Diabetologia 2006, 49, 2078–2085. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Ortega, F.B.; Castillo, R.; Martín-Matillas, M.; Kwak, L.; Vicente-Rodríguez, G.; Noriega, J.; Tercedor, P.; Sjöström, M.; Moreno, L.A.; et al. Physical activity, fitness, weight status, and cognitive performance in adolescents. J. Pediatr. 2010, 157, 917–922. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond.) 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Artero, E.G.; Ruiz, J.R.; Ortega, F.B.; España-Romero, V.; Vicente-Rodríguez, G.; Molnar, D.; Gottrand, F.; González-Gross, M.; Breidenassel, C.; Moreno, L.A.; et al. Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: The HELENA study. Pediatr. Diabetes 2011, 12, 704–712. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefts in Children and Adolescents? A Systematic Review and Meta Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Gutiérrez, A.; Moreno, L.A.; Tresaco, B.; Martínez, J.A.; González-Lamuño, D.; Wärnberg, J.; Castillo, M.; the AVENA Study Group. Is physical fitness a good predictor of cardiovascular disease risk factors in normal-weight and overweight or obese adolescents? The AVENA Study. Int. J. Obes. Relat. Metab. Disord. 2004, 28, S120. [Google Scholar]
- Eisenmann, J.C.; Katzmarzyk, P.T.; Perusse, L.; Tremblay, A.; Després, J.P.; Bouchard, C. Aerobic fitness, body mass index, and CVD risk factors among adolescents: The Québec family study. Int. J. Obes. (Lond.) 2005, 29, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Dumith, S.C.; Ramires, V.V.; Souza, M.A.; Moraes, D.S.; Petry, F.G.; Oliveira, E.S.; Ramires, S.V.; Hallal, P.C. Overweight/obesity and physical fitness among children and adolescents. J. Phys. Act. Health 2010, 7, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Liu, A.; Li, Y.; Hu, X.; Du, L.; Ma, J.; Xu, G.; Li, Y.; Guo, H.; Ma, G. The association of weight status with physical fitness among Chinese children. Int. J. Pediatr. 2010, 2010, 515414. [Google Scholar] [CrossRef]
- Chwałczyńska, A.; Jędrzejewski, G.; Lewandowski, Z.; Jonak, W.; Sobiech, K.A. Physical Fitness of Secondary School Adolescents in Relation to the Body Weight and the Body Composition: Classification According to Bioelectrical Impedance Analysis. Part II. J. Sports Med. Phys. Fit. 2017, 57, 252–259. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Bocanegra-Parrilla, R.; Ornelas, M.; Viciana, J. Criterion-related validity of the distance- and time-based walk/run field tests for estimating cardiorespiratory fitness: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0151671. [Google Scholar] [CrossRef]
- Pérez-Bey, A.; Segura-Jiménez, V.; Fernández-Santos, J.D.R.; Esteban-Cornejo, I.; Gómez-Martínez, S.; Veiga, O.L.; Marcos, A.; Castro-Piñero, J. The role of adiposity in the association between muscular fitness and cardiovascular disease. J. Pediatr. 2018, 199, 178–185.e4. [Google Scholar] [CrossRef]
- Messiah, S.E.; D’Agostino, E.M.; Patel, H.H.; Hansen, E.; Mathew, M.S.; Arheart, K.L. Sex differences in fitness outcomes among minority youth after participation in a park-based after-school program. Ann. Epidemiol. 2018, 28, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 2018, 52, 1445–14563. [Google Scholar] [CrossRef] [PubMed]
- Tanskey, L.A.; Goldberg, J.P.; Chui, K.; Must, A.; Wright, C.M.; Sacheck, J.M. A qualitative exploration of potential determinants of accelerated summer weight gain among school-age children: Perspectives from parents. BMC Pediatr. 2019, 19, 438. [Google Scholar] [CrossRef] [PubMed]
- Fogelholm, M.; Stigman, S.; Huisman, T.; Metsämuuronen, J. Physical fitness in adolescents with normal weight and overweight. Scand. J. Med. Sci. Sports 2008, 18, 162–170. [Google Scholar] [CrossRef]
- Liao, Y.; Chang, S.H.; Miyashita, M.; Stensel, D.; Chen, J.F.; Wen, L.T.; Nakamura, Y. Associations between health-related physical fitness and obesity in Taiwanese youth. J. Sports Sci. 2013, 31, 1797–1804. [Google Scholar] [CrossRef]
- Castro-Piñero, J.; González-Montesinos, J.L.; Mora, J.; Keating, X.D.; Girela-Rejón, M.J.; Sjöström, M.; Ruiz, J.R. Percentile values for muscular strength field tests in children aged 6 to 17 years: Influence of weight status. J. Strength. Cond. Res. 2009, 23, 2295–2310. [Google Scholar] [CrossRef]
- Eisenmann, J.C.; Wickel, E.E.; Welk, G.J.; Blair, S.N. Relationship between adolescent fitness and fatness and cardiovascular disease risk factors in adulthood: The Aerobics Center Longitudinal Study (ACLS). Am. Heart J. 2005, 149, 46–53. [Google Scholar] [CrossRef]
- Laitinen, T.T.; Pahkala, K.; Magnussen, C.G.; Viikari, J.S.; Oikonen, M.; Taittonen, L.; Mikkilä, V.; Jokinen, E.; Hutri-Kähönen, N.; Laitinen, T.; et al. Ideal cardiovascular health in childhood and cardiometabolic outcomes in adulthood: The Cardiovascular Risk in Young Finns Study. Circulation 2012, 125, 1971–1978. [Google Scholar] [CrossRef]
- Kumar, B.; Robinson, R.; Till, S. Physical activity and health in adolescence. Clin. Med. (Lond.) 2015, 15, 267–272. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GIRLS | ||||||
| Performance Type | 9th Grade | 12th Grade | ||||
| Obese | Overweight | Normal | Obese | Overweight | Normal | |
| run-walk | 19.61 | 102.06 | 207.97 | 15.21 | 102.37 | 208.8 |
| lower limb | 65.77 | 150.18 | 193.78 | 28.66 | 169.88 | 191.42 |
| hip flexor and abdominal muscle | 37.45 | 140.99 | 198.26 | 29.21 | 153.57 | 194.29 |
| shoulder and arm muscle | 39.09 | 159.69 | 194.77 | 21.71 | 158.38 | 193.1 |
| BOYS | ||||||
| Performance Type | 9th Grade | 12th Grade | ||||
| Obese | Overweight | Normal | Obese | Overweight | Normal | |
| run-walk | 22.97 | 129.59 | 200.5 | 27.37 | 165.21 | 195.11 |
| lower limb | 70.74 | 143.93 | 192.39 | 35.53 | 160.86 | 195.38 |
| hip flexor and abdominal muscle | 44.19 | 174.15 | 192.62 | 48.09 | 161.28 | 196.98 |
| shoulder and arm muscle | 75.28 | 159.66 | 188.1 | 54.29 | 159.66 | 192.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrovics, P.; Sandor, B.; Palfi, A.; Szekeres, Z.; Atlasz, T.; Toth, K.; Szabados, E. Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 134. https://doi.org/10.3390/ijerph18010134
Petrovics P, Sandor B, Palfi A, Szekeres Z, Atlasz T, Toth K, Szabados E. Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(1):134. https://doi.org/10.3390/ijerph18010134
Chicago/Turabian StylePetrovics, Peter, Barbara Sandor, Anita Palfi, Zsolt Szekeres, Tamas Atlasz, Kalman Toth, and Eszter Szabados. 2021. "Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents" International Journal of Environmental Research and Public Health 18, no. 1: 134. https://doi.org/10.3390/ijerph18010134
APA StylePetrovics, P., Sandor, B., Palfi, A., Szekeres, Z., Atlasz, T., Toth, K., & Szabados, E. (2021). Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents. International Journal of Environmental Research and Public Health, 18(1), 134. https://doi.org/10.3390/ijerph18010134