Health Impacts of Ambient Biomass Smoke in Tasmania, Australia

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. PM2.5 Exposure and Identification of WHS and LFS Days
- 1)
- The PM2.5 threshold used to identify LFS summer days (90th vs 99th percentile);
- 2)
- The months considered as start and end of winter; and
- 3)
- The consideration of sources allocated during the transition months (March, April, September, October) through the random forest method.
2.2. Population and Health Data
2.3. Health Impacts
2.4. Health Costs and Assessment
3. Results
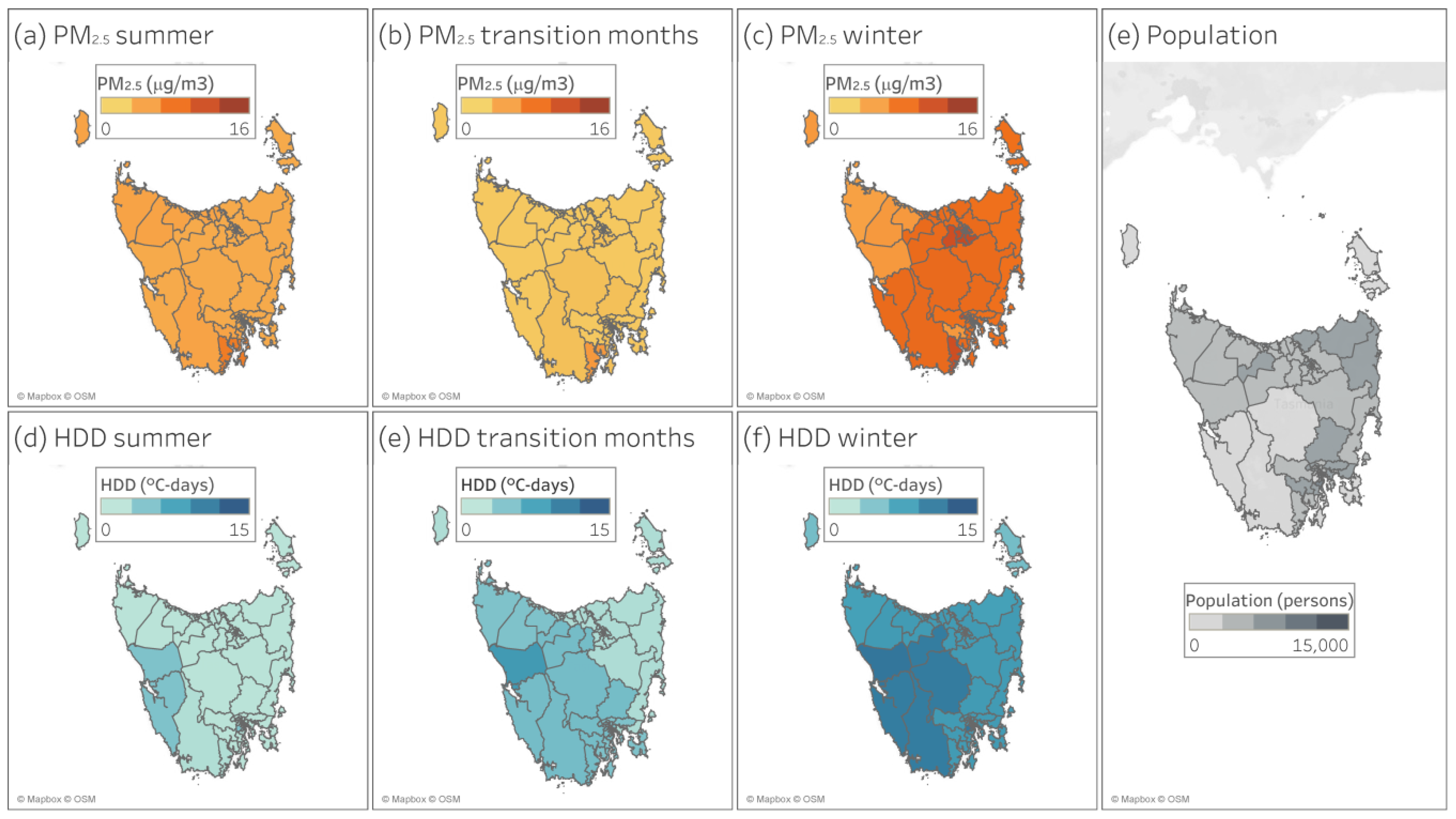
3.1. PM2.5 and HDD
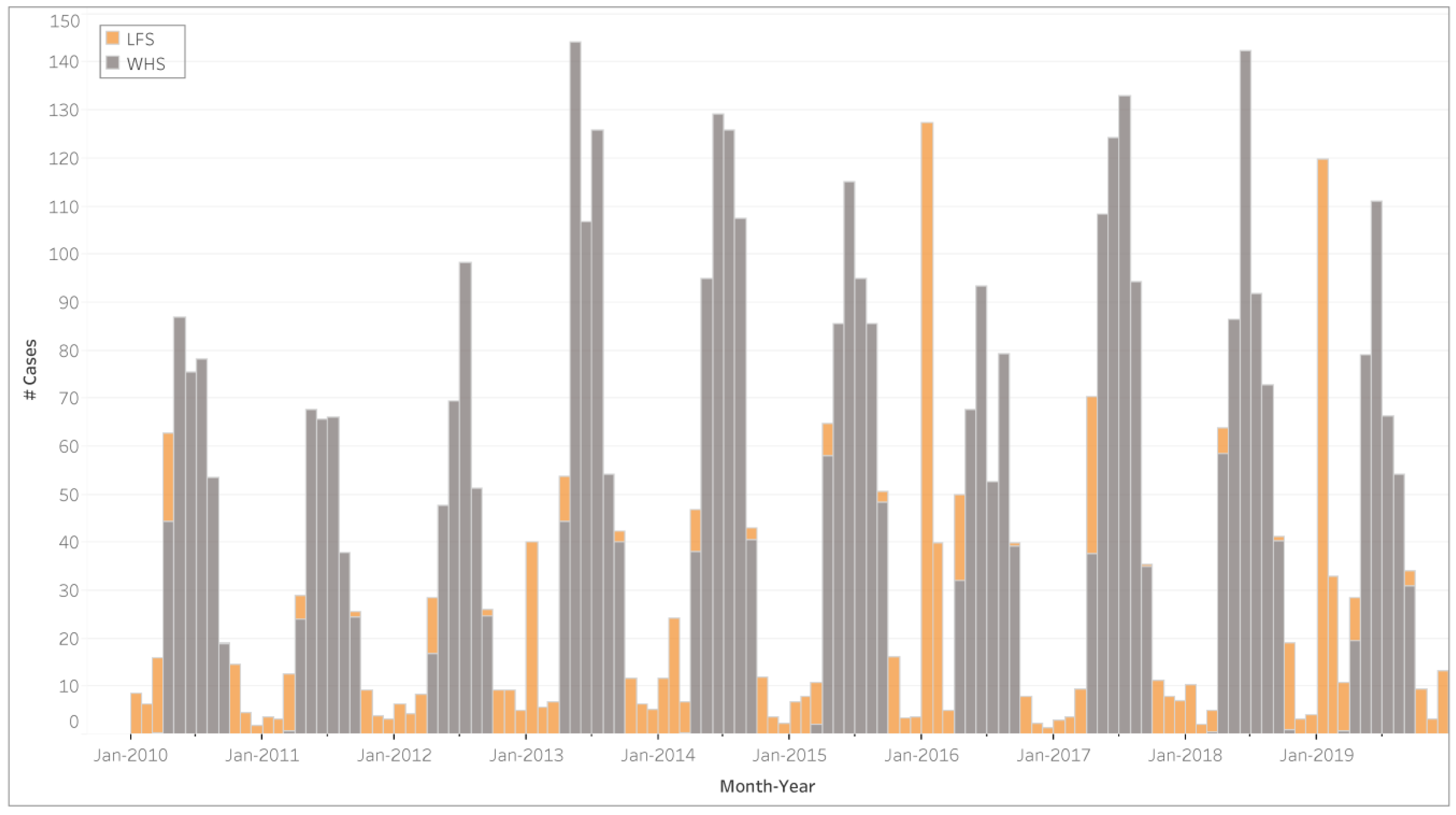
3.2. Health Impacts
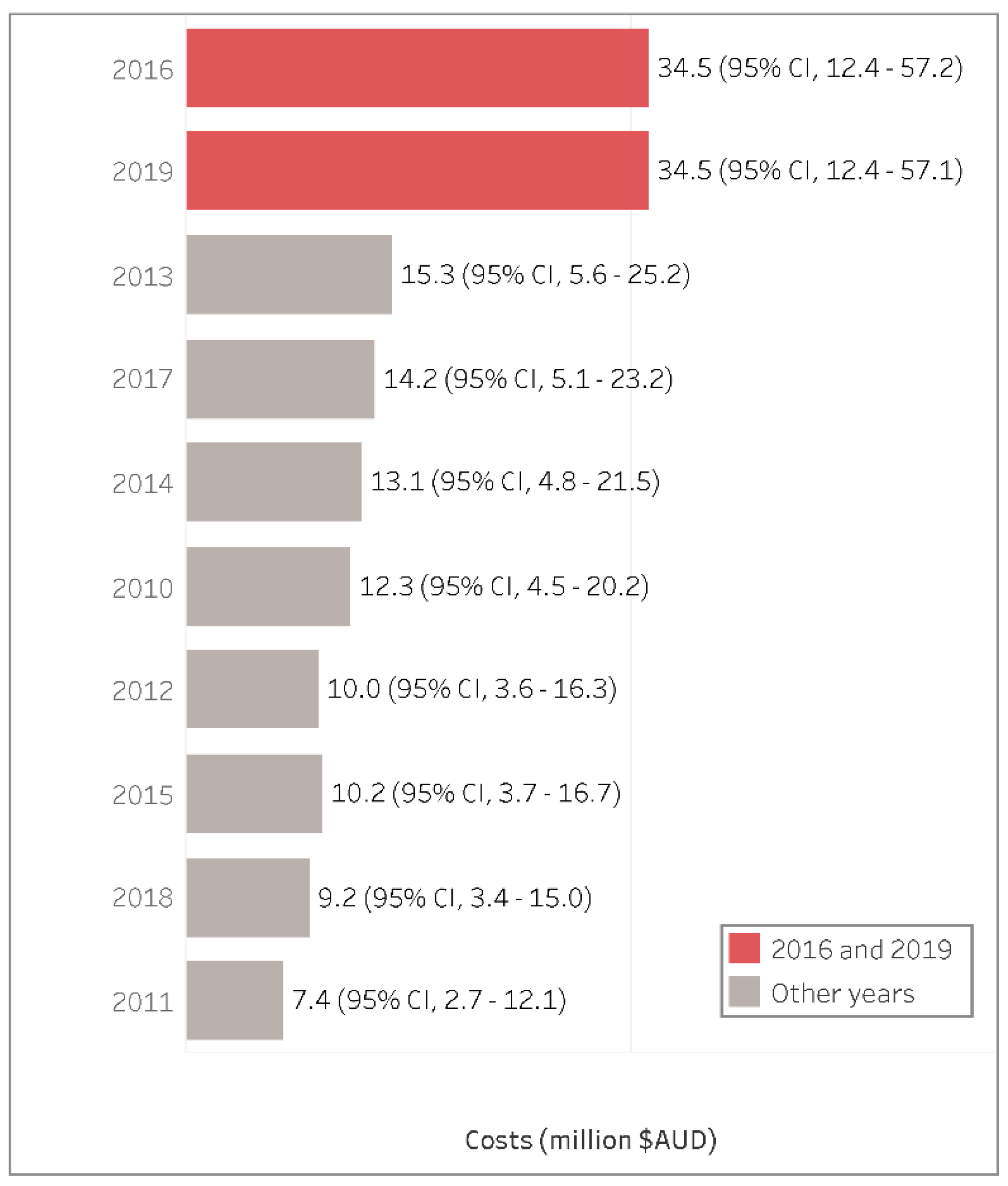
3.3. Health Costs
3.4. Sensitivity Analysis
4. Discussion
4.1. Results in Relation to Other Studies
4.2. Strengths and Limitations
4.3. Policy Implications
4.4. Unanswered Questions and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bhattu, D.; Zotter, P.; Zhou, J.; Stefenelli, G.; Klein, F.; Bertrand, A.; Temime-Roussel, B.; Marchand, N.; Slowik, J.G.; Baltensperger, U.; et al. Effect of Stove Technology and Combustion Conditions on Gas and Particulate Emissions from Residential Biomass Combustion. Environ. Sci. Technol. 2019, 53, 2209–2219. [Google Scholar] [CrossRef]
- Williamson, G.J.; Bowman, D.M.J.S.; Price, O.F.; Henderson, S.B.; Johnston, F.H. A transdisciplinary approach to understanding the health effects of wildfire and prescribed fire smoke regimes. Environ. Res. Lett. 2016, 11, 125009. [Google Scholar] [CrossRef]
- Kocbach, A.; Pagels, J.; Espen, K.; Barregard, L.; Sallsten, G.; Schwarze, P.E.; Boman, C. Health effects of residential wood smoke particles: The importance of combustion conditions and physicochemical particle properties. Part. Fibre Toxicol. 2009, 6, 29. [Google Scholar] [CrossRef]
- Moeltner, K.; Kim, M.K.; Zhu, E.; Yang, W. Wildfire smoke and health impacts: A closer look at fire attributes and their marginal effects. J. Environ. Econ. Manag. 2013, 66, 476–496. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Health Risks of Air Pollution in Europe–HRAPIE Project: Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Sigsgaard, T.; Forsberg, B.; Annesi-Maesano, I.; Blomberg, A.; Bølling, A.; Boman, C.; Bønløkke, J.; Brauer, M.; Bruce, N.; Héroux, M.-E.; et al. Health impacts of anthropogenic biomass burning in the developed world. Eur. Respir. J. 2015, 46, 1577–1588. [Google Scholar] [CrossRef]
- Mészáros, D.; Markos, J.; FitzGerald, D.G.; Walters, E.H.; Wood-Baker, R. An observational study of PM10 and hospital admissions for acute exacerbations of chronic respiratory disease in Tasmania, Australia 1992–2002. BMJ Open Respir. Res. 2015, 2, e000063. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Adetona, O.; Reinhardt, T.E.; Domitrovich, J.; Broyles, G.; Adetona, A.M.; Kleinman, M.T.; Ottmar, R.D.; Naeher, L.P. Review of the health effects of wildland fire smoke on wildland firefighters and the public. Inhal. Toxicol. 2016, 28, 95–139. [Google Scholar] [CrossRef] [PubMed]
- Cascio, W.E. Wildland fire smoke and human health. Sci. Total Environ. 2018, 624, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Naeher, L.P.; Brauer, M.; Lipsett, M.; Zelikoff, J.T.; Simpson, C.D.; Koenig, J.Q.; Smith, K.R. Woodsmoke health effects: A review. Inhal. Toxicol. 2007, 19, 67–106. [Google Scholar] [CrossRef]
- Borchers-Arriagada, N.; Horsley, J.A.; Palmer, A.J.; Morgan, G.G.; Tham, R.; Johnston, F.H. Association between fire smoke fine particulate matter and asthma-related outcomes: Systematic review and meta-analysis. Environ. Res. 2019, 179, 108777. [Google Scholar] [CrossRef]
- Borchers Arriagada, N.; Palmer, A.J.; Bowman, D.M.; Morgan, G.G.; Jalaludin, B.B.; Johnston, F.H. Unprecedented smoke-related health burden associated with the 2019–20 bushfires in eastern Australia. Med. J. Aust. 2020, 2, 50545. [Google Scholar] [CrossRef] [PubMed]
- Bowman, D.M.J.S.; Moreira-Muñoz, A.; Kolden, C.A.; Chávez, R.O.; Muñoz, A.A.; Salinas, F.; González-Reyes, Á.; Rocco, R.; de la Barrera, F.; Williamson, G.J.; et al. Human-environmental drivers and impacts of the globally extreme 2017 Chilean fires. Ambio 2018, 48, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Fann, N.; Alman, B.; Broome, R.A.; Morgan, G.G.; Johnston, F.H.; Pouliot, G.; Rappold, A.G. The health impacts and economic value of wildland fire episodes in the U.S.: 2008–2012. Sci. Total Environ. 2017, 610, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Sarigiannis, D.A.; Karakitsios, S.P.; Kermenidou, M.V. Health impact and monetary cost of exposure to particulate matter emitted from biomass burning in large cities. Sci. Total Environ. 2015, 524, 319–330. [Google Scholar] [CrossRef]
- Robinson, D.L. Australian wood heaters currently increase global warming and health costs. Atmos. Pollut. Res. 2011, 2, 267–274. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. ERP by SA2 (ASGS 2016), Age and Sex, 2001 Onwards. Available online: http://stat.data.abs.gov.au/Index.aspx?DataSetCode=ABS_ERP_ASGS2016 (accessed on 15 November 2018).
- Innis, J. Overview of the BLANkET Smoke Monitoring Network: Development and Operation 2009–2015; Technical Report No. 31; Environment Protection Authority Tasmania: Hobart, Australia, 2015.
- Environment Protection Authority Tasmania. Spatial Distribution of Wood Heaters and Open Fires in Tasmania; EPA: Hobart, Australia, 2017.
- Reisen, F.; Meyer, C.P.M.; Keywood, M.D. Impact of biomass burning sources on seasonal aerosol air quality. Atmos. Environ. 2013, 67, 437–447. [Google Scholar] [CrossRef]
- Meyer, C.P.; Reisen, F.; Keywood, M.; Crumeyrolle, S. Impacts of Smoke from Regeneration Burning on Air Quality in the Huon Valley, Tasmania; CSIRO: Hobart, Australia, 2011.
- Bennett, C.M.; Dharmage, S.C.; Matheson, M.; Gras, J.L.; Markos, J.; Mészáros, D.; Hopper, J.; Walters, E.H.; Abramson, M.J. Ambient wood smoke exposure and respiratory symptoms in Tasmania, Australia. Sci. Total Environ. 2010, 409, 294–299. [Google Scholar] [CrossRef]
- Johnston, F.H.; Hanigan, I.C.; Henderson, S.B.; Morgan, G.G. Evaluation of interventions to reduce air pollution from biomass smoke on mortality in Launceston, Australia: Retrospective analysis of daily mortality, 1994–2007. BMJ 2013, 346, e8446. [Google Scholar] [CrossRef]
- Keywood, M.D.; Ayers, G.P.; Gras, J.L.; Gillett, R.W.; Cohen, D.D. Size distribution and sources of aerosol in Launceston, Australia, during winter 1997. J. Air Waste Manag. Assoc. 2000, 50, 418–427. [Google Scholar] [CrossRef][Green Version]
- CSIRO. Woodheaters in Launceston—Impacts on Air Quality; CSIRO: Hobart, Australia, 2005.
- Luhar, A.K.; Galbally, I.E.; Keywood, M. Modelling PM10 concentrations and carrying capacity associated with woodheater emissions in Launceston, Tasmania. Atmos. Environ. 2006, 40, 5543–5557. [Google Scholar] [CrossRef]
- EPA Tasmania. Base Line Air Network of EPA Tasmania (BLANkET). Available online: https://epa.tas.gov.au/epa/air/monitoring-air-pollution/real-time-air-quality-data-for-tasmania/about-blanket (accessed on 1 February 2020).
- Bureau of Meteorology. Climate Data Online. Available online: http://www.bom.gov.au/climate/data/ (accessed on 15 November 2018).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS). Available online: https://www.abs.gov.au/websitedbs/D3310114.nsf/home/Australian+Statistical+Geography+Standard+(ASGS) (accessed on 5 December 2019).
- Xie, X.; Semanjski, I.; Gautama, S.; Tsiligianni, E.; Deligiannis, N.; Rajan, R.; Pasveer, F.; Philips, W. A Review of Urban Air Pollution Monitoring and Exposure Assessment Methods. ISPRS Int. J. Geo-Inf. 2017, 6, 389. [Google Scholar] [CrossRef]
- Martin, K.L.; Hanigan, I.C.; Morgan, G.G.; Henderson, S.B.; Johnston, F.H. Air pollution from bushfires and their association with hospital admissions in Sydney, Newcastle and Wollongong, Australia 1994–2007. Aust. N. Z. J. Public Health 2013, 37, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.; Hanigan, I.; Henderson, S.; Morgan, G.; Bowman, D. Extreme air pollution events from bushfires and dust storms and their association with mortality in Sydney, Australia 1994–2007. Environ. Res. 2011, 111, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Horsley, J.A.; Broome, R.A.; Johnston, F.H.; Cope, M.; Morgan, G.G. Health burden associated with fire smoke in Sydney, 2001–2013. Med. J. Aust. 2018, 208, 309–310. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Deaths, Year of Occurrence, Age at Death, Age-Specific Death Rates, Sex, States, Territories and Australia. Available online: http://stat.data.abs.gov.au/Index.aspx?DataSetCode=DEATHS_AGESPECIFIC_OCCURENCEYEAR (accessed on 15 November 2018).
- Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework. Available online: https://www.aihw.gov.au/reports/indigenous-health-welfare/health-performance-framework-new/contents/tier-1-health-status-outcomes (accessed on 15 November 2018).
- Australian Institute of Health and Welfare. Emergency Department Care 2014–15: Australian Hospital Statistics; Heatlh services series no. 65. Cat. no. HSE 168; AIHW: Canberra, Australia, 2015.
- Australian Institute of Health and Welfare. Emergency Department Care 2015–16: Australian Hospital Statistics; Heatlh services series no. 72. Cat. no. HSE 182; AIHW: Canberra, Australia, 2016.
- Australian Institute of Health and Welfare. Emergency Department Care 2016–17: Australian Hospital Statistics; Heatlh services series no. 80. Cat. no. HSE 194; AIHW: Canberra, Australia, 2017.
- Fann, N.; Lamson, A.D.; Anenberg, S.C.; Wesson, K.; Risley, D.; Hubbell, B.J. Estimating the National Public Health Burden Associated with Exposure to Ambient PM2.5 and Ozone. Risk Anal. 2012, 32, 81–95. [Google Scholar] [CrossRef]
- Johnston, F.H.; Henderson, S.B.; Chen, Y.; Randerson, J.T.; Marlier, M.; DeFries, R.S.; Kinney, P.L.; Bowman, D.M.J.S.; Brauer, M. Estimated global mortality attributable to smoke from landscape fires. Environ. Health Perspect. 2012, 120, 695–701. [Google Scholar] [CrossRef]
- Fan, J.; Li, S.; Fan, C.; Bai, Z.; Yang, K. The impact of PM2.5 on asthma emergency department visits: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. 2016, 23, 843–850. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Health Risk Assessment of Air Pollution—General Principles; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Science for Environmental Policy. What Are the Health Costs of Environmental Pollution? Future Brief 21. Brief produced for the European Commission DG Environment by the Science Communication Unit, UWE, Bristol. Publications Office of the European Union: Luxembourg, 2018. Available online: http://ec.europa.eu/science-environment-policy (accessed on 6 May 2020).
- Office of the Best Practice Regulation. Best Practice Regulation Note—Value of Statistical Life; Australian Government, Department of the Prime Minister and Cabinet: Canberra, Australia, 2014.
- The Independent Hospital Pricing Authority. National Hospital Cost Data Collection, Public Hospitals Cost Report, Round 20 (Financial Year 2015–16); IHPA: Darlinghurst, Australia, 2018.
- Australian Bureau of Statistics. Average Weekly Earnings, Australia. May 2018. Available online: http://www.abs.gov.au/ausstats/abs@.nsf/mf/6302.0 (accessed on 12 December 2018).
- Australian Bureau of Statistics. Labour Force, Australia. October 2018. Available online: http://www.abs.gov.au/AUSSTATS/abs@.nsf/allprimarymainfeatures/8A84F3F8AE60BF39CA2583690004C6D1?opendocument (accessed on 12 December 2018).
- Health Policy Analysis. Emergency Care Costing and Classification Project: Cost Report; Independent Hospital Pricing Authority: Sydney, Australia, 2017.
- Reserve Bank of Australia. Inflation Calculator. Available online: https://www.rba.gov.au/calculator/ (accessed on 25 September 2019).
- Australian Bureau of Statistics. Census of Population and Housing: Mesh Block Counts, Australia (2074.0). 2016. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/mf/2074.0 (accessed on 15 January 2019).
- Chafe, Z.; Brauer, M.; Héroux, M.; Klimont, Z.; Lanki, T.; Salonen, R.; Smith, K. Residential Heating with Wood and Coal: Health Impacts and Policy Options in Europe and North America; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Borchers Arriagada, N.; Palmer, A.J.; Bowman, D.M.; Johnston, F.H. Exceedances of national air quality standards for particulate matter in Western Australia: Sources and health-related impacts. Med. J. Aust. 2020, 2, 50547. [Google Scholar] [CrossRef]
- Department of the Environment and Energy. Air Quality Standards. Available online: http://www.environment.gov.au/protection/air-quality/air-quality-standards#air (accessed on 15 February 2020).
- Ford, B.; Val Martin, M.; Zelasky, S.E.; Fischer, E.V.; Anenberg, S.C.; Heald, C.L.; Pierce, J.R. Future Fire Impacts on Smoke Concentrations, Visibility, and Health in the Contiguous United States. GeoHealth 2018, 2, 229–247. [Google Scholar] [CrossRef]
- Broome, R.A.; Johnston, F.H.; Horsley, J.; Morgan, G.G. A rapid assessment of the impact of hazard reduction burning around Sydney, May 2016. Med. J. Aust. 2016, 205, 407–408. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.A.; Hammitt, J.K.; O’Keeffe, L. Valuing Mortality Risk Reductions in Global Benefit-Cost Analysis. J. Benefit-Cost Anal. 2019, 10, 15–50. [Google Scholar] [CrossRef]
- Hammitt, J.K.; Morfeld, P.; Tuomisto, J.T.; Erren, T.C. Premature Deaths, Statistical Lives, and Years of Life Lost: Identification, Quantification, and Valuation of Mortality Risks. Risk Anal. 2019, 40, 674–695. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Final Regulatory Impact Analysis (RIA) for the NO2 National Ambient Air Quality Standards (NAAQS); Office of Air Quality Planning and Standards: Research Triangle Park, NC, USA, 2010.
- Council, N.R. Estimating Mortality Risk Reduction and Economic Benefits from Controlling Ozone Air Pollution; The National Academies Press: Washington, DC, USA, 2008; ISBN 978-0-309-11994-8. [Google Scholar]
- Martinez, G.S.; Spadaro, J.V.; Chapizanis, D.; Kendrovski, V.; Kochubovski, M.; Mudu, P. Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje. Int. J. Environ. Res. Public Health 2018, 15, 626. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H. Understanding and managing the health impacts of poor air quality from landscape fires. Med. J. Aust. 2017, 207, 229–230. [Google Scholar] [CrossRef]
- Forest Practices Authority. Forest Industry Standard for Prescribed Silvicultural Burning Practice 2009; FPA: Hobart, Australia, 2009. [Google Scholar]
- Bowman, D.M.J.S.; Daniels, L.; Johnston, F.; Williamson, G.; Jolly, W.; Magzamen, S.; Rappold, A.; Brauer, M.; Henderson, S. Can Air Quality Management Drive Sustainable Fuels Management at the Temperate Wildland–Urban Interface? Fire 2018, 1, 27. [Google Scholar] [CrossRef]
- Nicholls, D.; Halbrook, J.; Benedum, M.; Han, H.-S.; Lowell, E.; Becker, D.; Barbour, R. Socioeconomic Constraints to Biomass Removal from Forest Lands for Fire Risk Reduction in the Western U.S. Forests 2018, 9, 264. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effect | Cause | Age Group | Type of Smoke | Exposure | Beta | Standard Error | Increase per 10 (μg/m3) | Reference |
|---|---|---|---|---|---|---|---|---|
| Premature Mortality | All-cause | 30+ | WHS | Annual PM2.5 | 0.006015 | 0.001034 | 6.2% | [5] |
| All | LFS | 24-h PM2.5 | 0.001222 | 0.000393 | 1.2% | |||
| Hospital Admissions | CVD | All | WHS/LFS | 24-h PM2.5 | 0.000906 | 0.000377 | 0.9% | [5] |
| RSP | All | WHS/LFS | 24-h PM2.5 | 0.001882 | 0.001051 | 1.9% | ||
| ED visits | Asthma | 0–17 | WHS | 24-h PM2.5 | 0.003537 | 0.000862 | 3.6% | [42] |
| 18–64 | WHS | 24-h PM2.5 | 0.001686 | 0.000527 | 1.7% | |||
| 0–17 | LFS | 24-h PM2.5 | 0.003811 | 0.001865 | 3.9% | [11] | ||
| 18–64 | LFS | 24-h PM2.5 | 0.007071 | 0.001586 | 7.3% | |||
| 64+ | LFS | 24-h PM2.5 | 0.013994 | 0.002356 | 15% |
| Day Type | Average Days per Year (number) | Average Days per Year (%) | Mean (μg/m3) | SD (μg/m3) | Max (μg/m3) |
|---|---|---|---|---|---|
| Unpolluted | 95 | 26% | 1.4 | 0.4 | 3 |
| LFS | 111.8 | 30.6% | 4.2 | 6.3 | 313 |
| WHS | 158.3 | 43.4% | 7.7 | 5.4 | 168 |
| Source Type | Health Outcome | Estimated # of Cases | Estimated # of Cases per Year |
|---|---|---|---|
| LFS | All-cause Mortality | 36 (95% CI: 13–58) | 4 (95% CI: 1–6) |
| Asthma ED Visits | 76 (95% CI: 39–121) | 8 (95% CI: 4–12) | |
| CVD Hospital Admissions | 70 (95% CI: 13–128) | 7 (95% CI: 1–13) | |
| RSP Hospital Admissions | 112 (95% CI: 0–240) | 11 (95% CI: 0–24) | |
| WHS | All-cause Mortality | 653 (95% CI: 420–874) | 65 (95% CI: 42–87) |
| Asthma ED Visits | 72 (95% CI: 36–108) | 7 (95% CI: 4–11) | |
| CVD Hospital Admissions | 259 (95% CI: 49–474) | 26 (95% CI: 5–47) | |
| RSP Hospital Admissions | 416 (95% CI: 0–882) | 42 (95% CI: 0–88) | |
| Total | All-cause Mortality | 688 (95% CI: 433–932) | 69 (95% CI: 43–93) |
| Asthma ED Visits | 148 (95% CI: 74–229) | 15 (95% CI: 7–23) | |
| CVD Hospital Admissions | 329 (95% CI: 62–602) | 33 (95% CI: 6–60) | |
| RSP Hospital Admissions | 528 (95% CI: 0–1123) | 53 (95% CI: 0–112) |
| Health Outcome | 2016 | 2019 | Average for All Other Years |
|---|---|---|---|
| All-cause Mortality | 8 (95% CI: 3–13) | 8 (95% CI: 3–13) | 3 (95% CI: 1–4) |
| Asthma ED Visits | 18 (95% CI: 9–31) | 18 (95% CI: 9–30) | 5 (95% CI: 3–8) |
| CVD Hospital Admissions | 15 (95% CI: 3–28) | 15 (95% CI: 3–28) | 5 (95% CI: 1–9) |
| RSP Hospital Admissions | 24 (95% CI: 0–52) | 24 (95% CI: 0–52) | 8 (95% CI: 0–17) |
| Source Type | Health Outcome | Total Cost (AUD$ *) | Yearly Cost (AUD$/Year *) |
|---|---|---|---|
| LFS | All-cause Mortality (**) | 159 (95% CI: 58–262) million | 16 (95% CI: 6–26) million |
| Asthma ED Visits | 55,949 (95% CI: 28,370–88,766) | 5595 (95% CI: 2837–8877) | |
| CVD Hospital Admissions | 521,552 (95% CI: 97,075–957,899) | 52,155 (95% CI: 9708–95,790) | |
| RSP Hospital Admissions | 845,972 (95% CI: 0–1,817,405) | 84,597 (95% CI: 0–181,741) | |
| WHS | All-cause Mortality (**) | 2929 (95% CI: 1885–3920) million | 293 (95% CI: 189–392) million |
| Asthma ED Visits | 52,508 (95% CI: 26,071–79,259) | 5251 (95% CI: 2607–7926) | |
| CVD Hospital Admissions | 1,937,594 (95% CI: 362,145–3,542,801) | 193,759 (95% CI: 36,215–354,280) | |
| RSP Hospital Admissions | 3,149,178 (95% CI: 0–6,674,047) | 314,918 (95% CI: 0–667,405) | |
| Total | All-cause Mortality (**) | 3088 (95% CI: 1943–4181) million | 309 (95% CI: 194–418) million |
| Asthma ED Visits | 108,457 (95% CI: 54,441–168,025) | 10,846 (95% CI: 5444–16,803) | |
| CVD Hospital Admissions | 2,459,146 (95% CI: 459,220–4,500,700) | 245,915 (95% CI: 45,922–450,070) | |
| RSP Hospital Admissions | 3,995,150 (95% CI: 0–8,491,452) | 399,515 (95% CI: 0–849,145) |
| SA4 | Population | LFS | WHS | |||
|---|---|---|---|---|---|---|
| Persons | % | AUD$ | % | AUD$ | % | |
| Hobart | 229,088 | 44% | 63,119,001 | 39% | 1,161,808,071 | 40% |
| Launceston and North–East | 143,752 | 28% | 48,045,137 | 30% | 1,093,171,538 | 37% |
| West and North–West | 111,259 | 21% | 36,536,828 | 23% | 473,598,790 | 16% |
| South–East | 38,053 | 7% | 13,016,748 | 8% | 205,218,190 | 7% |
| Total | 522,152 | 100% | 160,717,714 | 100% | 2,933,796,590 | 100% |
| Source | Indicator | All-Cause Mortality | Asthma ED Visits | CVD Hospital Admissions | RSP Hospital Admissions | TOTAL |
|---|---|---|---|---|---|---|
| WHS | Total Cost (AUD$) | 2,928,657,309 | 52,508 | 1,937,594 | 3,149,178 | 2,933,796,590 |
| Cost per day (AUD$/WHS-day) | 1,566,127 | 28 | 1036 | 1684 | 1,568,875 | |
| Cost per year (AUD$/year) | 292,865,731 | 5251 | 193,759 | 314,918 | 293,379,659 | |
| Cost per woodstove-year (AUD$/woodstove-year) | 4225 | 0 | 3 | 5 | 4232 | |
| LFS | Total Cost (AUD$) | 159,294,240 | 55,949 | 521,552 | 845,972 | 160,717,714 |
| Cost per day (AUD$/LFS-day) | 75,281 | 26 | 246 | 400 | 75,954 | |
| Cost per year (AUD$/year) | 15,929,424 | 5595 | 52,155 | 84,597 | 16,071,771 |
| Months Included | Source | Indicator | Main Scenario | Range |
|---|---|---|---|---|
| All months | WHS | Total Cost (AUD$) | 2934 million | 2458–3189 million |
| Cost per day (AUD$/WHS-day) | 1.6 million | 1.4–1.7 million | ||
| Cost per year (AUD$/year) | 293.4 million | 245.8–318.9 million | ||
| Cost per woodstove-year (AUD$/woodstove-year) | 4232 | 3545–4601 | ||
| LFS | Total Cost (AUD$) | 160.7 million | 138.2–270.3 million | |
| Cost per day (AUD$/LFS-day) | 76 thousand | 64–109 thousand | ||
| Cost per year (AUD$/year) | 16.1 million | 13.8–27 million | ||
| Excluding months with predicted biomass smoke source | WHS | Total Cost (AUD$) | 2438 million | 1294–2615 million |
| Cost per day (AUD$/WHS-day) | 1.98 million | 1.9–2.4 million | ||
| Cost per year (AUD$/year) | 243.8 million | 129.4–261.5 million | ||
| Cost per woodstove-year (AUD$/woodstove-year) | 3518 | 1867–3773 | ||
| LFS | Total Cost (AUD$) | 97.3 million | 86–117.3 million | |
| Cost per day (AUD$/LFS-day) | 81 thousand | 71.5–97.6 thousand | ||
| Cost per year (AUD$/year) | 9.7 million | 8.6–11.7 million |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borchers-Arriagada, N.; Palmer, A.J.; Bowman, D.M.J.S.; Williamson, G.J.; Johnston, F.H. Health Impacts of Ambient Biomass Smoke in Tasmania, Australia. Int. J. Environ. Res. Public Health 2020, 17, 3264. https://doi.org/10.3390/ijerph17093264
Borchers-Arriagada N, Palmer AJ, Bowman DMJS, Williamson GJ, Johnston FH. Health Impacts of Ambient Biomass Smoke in Tasmania, Australia. International Journal of Environmental Research and Public Health. 2020; 17(9):3264. https://doi.org/10.3390/ijerph17093264
Chicago/Turabian StyleBorchers-Arriagada, Nicolas, Andrew J. Palmer, David M.J.S. Bowman, Grant J. Williamson, and Fay H. Johnston. 2020. "Health Impacts of Ambient Biomass Smoke in Tasmania, Australia" International Journal of Environmental Research and Public Health 17, no. 9: 3264. https://doi.org/10.3390/ijerph17093264
APA StyleBorchers-Arriagada, N., Palmer, A. J., Bowman, D. M. J. S., Williamson, G. J., & Johnston, F. H. (2020). Health Impacts of Ambient Biomass Smoke in Tasmania, Australia. International Journal of Environmental Research and Public Health, 17(9), 3264. https://doi.org/10.3390/ijerph17093264