Racial Disparities in Associations between Neighborhood Demographic Polarization and Birth Weight

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Neighborhood Demographic Polarization
2.2. Study Population
2.3. Statistical Analysis
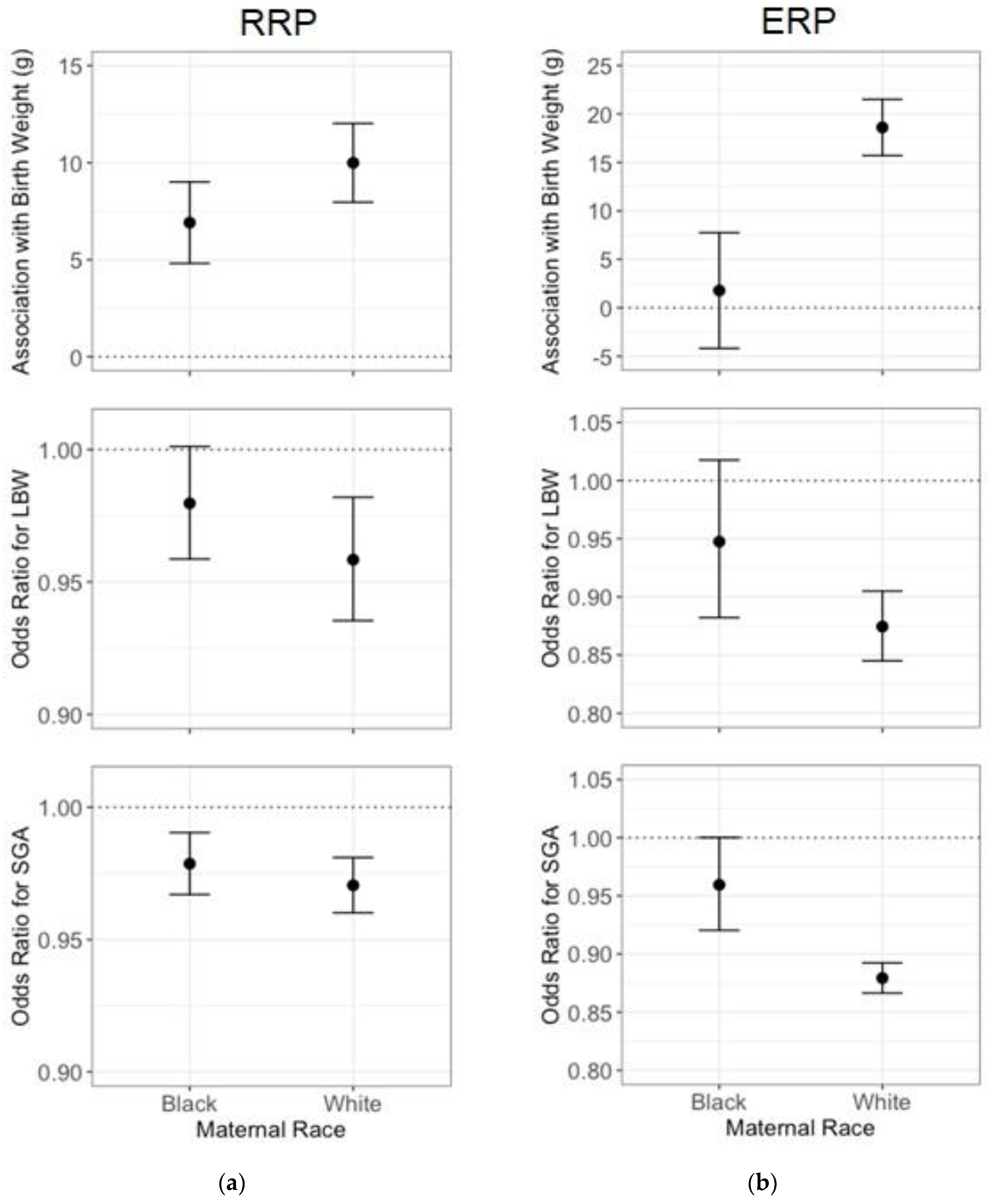
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Massey, D.S. The age of extremes: Concentrated affluence and poverty in the twenty-first century. Demography 1996, 33, 395–412. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Waterman, P.D.; Batra, N.; Murphy, J.S.; Dooley, D.P.; Shah, S.N. Measures of Local Segregation for Monitoring Health Inequities by Local Health Departments. Am. J. Public Health 2017, 107, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Chambers, B.D.; Baer, R.J.; McLemore, M.R.; Jelliffe-Pawlowski, L.L. Using Index of Concentration at the Extremes as Indicators of Structural Racism to Evaluate the Association with Preterm Birth and Infant Mortality-California, 2011–2012. J. Urban Health Bull. N. Y. Acad. Med. 2019, 96, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V. Investigating Neighborhood and Area Effects on Health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Feldman, J.M.; Waterman, P.D.; Coull, B.A.; Krieger, N. Spatial social polarisation: Using the Index of Concentration at the Extremes jointly for income and race/ethnicity to analyse risk of hypertension. J. Epidemiol. Community Health 2015, 69, 1199–1207. [Google Scholar] [CrossRef]
- Lange-Maia, B.S.; Maio, F.D.; Avery, E.F.; Lynch, E.B.; Laflamme, E.M.; Ansell, D.A.; Shah, R.C. Association of community-level inequities and premature mortality: Chicago, 2011–2015. J. Epidemiol. Community Health 2018, 72, 1099–1103. [Google Scholar] [CrossRef]
- Belbasis, L.; Savvidou, M.D.; Kanu, C.; Evangelou, E.; Tzoulaki, I. Birth weight in relation to health and disease in later life: An umbrella review of systematic reviews and meta-analyses. BMC Med. 2016, 14, 147. [Google Scholar] [CrossRef]
- Boulet, S.L.; Schieve, L.A.; Boyle, C.A. Birth weight and health and developmental outcomes in US children, 1997–2005. Matern. Child Health J. 2011, 15, 836–844. [Google Scholar] [CrossRef]
- Hack, M.; Klein, N.K.; Taylor, H.G. Long-term developmental outcomes of low birth weight infants. Future Child. Cent. Future Child. David Lucile Packard Found. 1995, 5, 176–196. [Google Scholar] [CrossRef]
- Reyes, L.; Mañalich, R. Long-term consequences of low birth weight. Kidney Int. Suppl. 2005, S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Waterman, P.D.; Spasojevic, J.; Li, W.; Maduro, G.; Van Wye, G. Public Health Monitoring of Privilege and Deprivation With the Index of Concentration at the Extremes. Am. J. Public Health 2016, 106, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Pearl, M.; Braveman, P.; Abrams, B. The Relationship of Neighborhood Socioeconomic Characteristics to Birthweight Among 5 Ethnic Groups in California. Am. J. Public Health 2001, 91, 1808–1814. [Google Scholar] [CrossRef] [PubMed]
- Conley, D.; Bennett, N.G. Race and the inheritance of low birth weight. Soc. Biol. 2000, 47, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.W.; David, R.J. Racial disparity in low birth weight and infant mortality. Clin. Perinatol. 2009, 36, 63–73. [Google Scholar] [CrossRef]
- U.S. Census Bureau American Community Survey, 2010 5-Year Estimates. Available online: https://factfinder.census.gov (accessed on 29 November 2017).
- Gray, S.C.; Edwards, S.E.; Schultz, B.D.; Miranda, M.L. Assessing the impact of race, social factors and air pollution on birth outcomes: A population-based study. Environ. Health Glob. Access Sci. Source 2014, 13, 4. [Google Scholar] [CrossRef]
- Shmool, J.L.C.; Bobb, J.F.; Ito, K.; Elston, B.; Savitz, D.A.; Ross, Z.; Matte, T.D.; Johnson, S.; Dominici, F.; Clougherty, J.E. Area-level socioeconomic deprivation, nitrogen dioxide exposure, and term birth weight in New York City. Environ. Res. 2015, 142, 624–632. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Chen, J.T.; Rehkopf, D.H.; Waterman, P.D.; Krieger, N. Comparing individual- and area-based socioeconomic measures for the surveillance of health disparities: A multilevel analysis of Massachusetts births, 1989–1991. Am. J. Epidemiol. 2006, 164, 823–834. [Google Scholar] [CrossRef]
- Kessner, D.M.; Singer, J.; Kalk, C.W.; Shlesinger, E.R. Chapter 2. In Infant Death: An Analysis by Maternal Risk and Health Care; Institute of Medicine and National Academy of Sciences: Washington, DC, USA, 1973. [Google Scholar]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef]
- Sun, X.; Luo, X.; Zhao, C.; Zhang, B.; Tao, J.; Yang, Z.; Ma, W.; Liu, T. The associations between birth weight and exposure to fine particulate matter (PM2.5) and its chemical constituents during pregnancy: A meta-analysis. Environ. Pollut. Barking Essex 1987 2016, 211, 38–47. [Google Scholar] [CrossRef]
- Kloog, I.; Chudnovsky, A.A.; Just, A.C.; Nordio, F.; Koutrakis, P.; Coull, B.A.; Lyapustin, A.; Wang, Y.; Schwartz, J. A new hybrid spatio-temporal model for estimating daily multi-year PM2.5 concentrations across northeastern USA using high resolution aerosol optical depth data. Atmos. Environ. 2014, 95, 581–590. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; Wong, D.W.S. The Modifiable Areal Unit Problem in Multivariate Statistical Analysis. Environ. Plan. Econ. Space 1991, 23, 1025–1044. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Zeka, A.; Melly, S.J.; Schwartz, J. The effects of socioeconomic status and indices of physical environment on reduced birth weight and preterm births in Eastern Massachusetts. Environ. Health Glob. Access Sci. Source 2008, 7, 60. [Google Scholar] [CrossRef] [PubMed]
- Casciano, R.; Massey, D.S. Neighborhood disorder and anxiety symptoms: New evidence from a quasi-experimental study. Health Place 2012, 18, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Finch, B.K.; Phuong Do, D.; Heron, M.; Bird, C.; Seeman, T.; Lurie, N. Neighborhood effects on health: Concentrated advantage and disadvantage. Health Place 2010, 16, 1058–1060. [Google Scholar] [CrossRef]
- Ncube, C.N.; Enquobahrie, D.A.; Albert, S.M.; Herrick, A.L.; Burke, J.G. Association of neighborhood context with offspring risk of preterm birth and low birthweight: A systematic review and meta-analysis of population-based studies. Soc. Sci. Med. 1982 2016, 153, 156–164. [Google Scholar] [CrossRef]
- Huynh, M.; Spasojevic, J.; Li, W.; Maduro, G.; Van Wye, G.; Waterman, P.D.; Krieger, N. Spatial social polarization and birth outcomes: Preterm birth and infant mortality—New York City, 2010–2014. Scand. J. Public Health 2018, 46, 157–166. [Google Scholar] [CrossRef]
- Shrimali, B.P.; Pearl, M.; Karasek, D.; Reid, C.; Abrams, B.; Mujahid, M. Neighborhood Privilege, Preterm Delivery, and Related Racial/Ethnic Disparities: An Intergenerational Application of the Index of Concentration at the Extremes. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Luo, Z.-C.; Wilkins, R.; Kramer, M.S. Effect of neighbourhood income and maternal education on birth outcomes: A population-based study. CMAJ Can. Med. Assoc. J. 2006, 174, 1415–1420. [Google Scholar] [CrossRef]
- Orchard, J.; Price, J. County-level racial prejudice and the black-white gap in infant health outcomes. Soc. Sci. Med. 1982 2017, 181, 191–198. [Google Scholar] [CrossRef]
- Mehra, R.; Boyd, L.M.; Ickovics, J.R. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Soc. Sci. Med. 1982 2017, 191, 237–250. [Google Scholar] [CrossRef]
- Fang, J.; Madhavan, S.; Alderman, M.H. Low birth weight: Race and maternal nativity--impact of community income. Pediatrics 1999, 103, E5. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.C.; Kloog, I.; Coull, B.A.; Koutrakis, P.; Laden, F.; Schwartz, J.D.; James, P. Residential Greenness and Birthweight in the State of Massachusetts, USA. Int. J. Environ. Res. Public. Health 2018, 15, 1248. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Overall |
|---|---|
| Total Births (n) | 629,675 |
| Continuous Variables (median ± interquartile range) | |
| Birthweight in Grams | 3459 ± 623 |
| Average PM2.5 over entire Pregnancy (µg/m3) | 10.2 ± 2.3 |
| Clinical Gestational Age in Weeks | 39 ± 1 |
| Maternal Age in Years | 31 ± 8.2 |
| Racial Residential Polarization (RRP) | |
| at Census Block Group | 0.88 ± 0.27 |
| at Census Tract | 0.86 ± 0.24 |
| Economic Residential Polarization (ERP) | |
| at Census Block Group | 0.12 ± 0.43 |
| at Census Tract | 0.12 ± 0.37 |
| Binary and Categorical Variables (%) | |
| Infant Sex = Female | 49.1 |
| Maternal Marital Status = Married | 72.0 |
| Medicaid Status = Yes | 28.2 |
| Smoking During or Prior to Pregnancy | 15.2 |
| Gestational Diabetes | 3.7 |
| Other Diabetes | 0.8 |
| High Blood Pressure during Pregnancy | 3.6 |
| Chronic High Blood Pressure | 1.3 |
| Parity: First-Pregnancy | 45.2 |
| Mode of Delivery | |
| Vaginal | 64.9 |
| Forceps | 0.6 |
| Vacuum | 3.5 |
| First Caesarian Birth | 17.1 |
| Repeat Caesarian | 12.4 |
| Vaginal Birth after Previous Caesarean Birth | 1.5 |
| Maternal Race | |
| White | 89.5 |
| Black | 10.5 |
| Kessner Index for Adequacy of Prenatal Care | |
| Adequate | 80.3 |
| Intermediate | 15.6 |
| Inadequate | 3.0 |
| No Prenatal Care | 1.2 |
| Maternal Education | |
| Less than High School | 7.4 |
| High School | 22.8 |
| Some College | 23.7 |
| College | 28.5 |
| Advanced Degree | 17.6 |
| Outcome | ||||
|---|---|---|---|---|
| - | - | Birth Weight (g) | LBW (OR) 1 | SGA (OR) |
| Unadjusted | RRP 2 | 134.3 (130.6, 137.9) 3 | 0.86 (0.85, 0.87) | 0.94 (0.93, 0.94) |
| ERP | 175.1 (170.8, 179.3) | 0.68 (0.67, 0.70) | 0.76 (0.75, 0.77) | |
| Full Model 4 | RRP | 8.7 (7.4, 10.0) | 0.96 (0.94, 0.98) | 0.97 (0.96, 0.98) |
| ERP | 17.0 (14.1, 19.8) | 0.88 (0.86, 0.91) | 0.88 (0.87, 0.89) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, K.C.; Yitshak-Sade, M.; Lane, K.J.; Fabian, M.P.; Kloog, I.; Schwartz, J.D.; Coull, B.A.; Koutrakis, P.; Hart, J.E.; Laden, F.; et al. Racial Disparities in Associations between Neighborhood Demographic Polarization and Birth Weight. Int. J. Environ. Res. Public Health 2020, 17, 3076. https://doi.org/10.3390/ijerph17093076
Fong KC, Yitshak-Sade M, Lane KJ, Fabian MP, Kloog I, Schwartz JD, Coull BA, Koutrakis P, Hart JE, Laden F, et al. Racial Disparities in Associations between Neighborhood Demographic Polarization and Birth Weight. International Journal of Environmental Research and Public Health. 2020; 17(9):3076. https://doi.org/10.3390/ijerph17093076
Chicago/Turabian StyleFong, Kelvin C., Maayan Yitshak-Sade, Kevin J. Lane, M. Patricia Fabian, Itai Kloog, Joel D. Schwartz, Brent A. Coull, Petros Koutrakis, Jaime E. Hart, Francine Laden, and et al. 2020. "Racial Disparities in Associations between Neighborhood Demographic Polarization and Birth Weight" International Journal of Environmental Research and Public Health 17, no. 9: 3076. https://doi.org/10.3390/ijerph17093076
APA StyleFong, K. C., Yitshak-Sade, M., Lane, K. J., Fabian, M. P., Kloog, I., Schwartz, J. D., Coull, B. A., Koutrakis, P., Hart, J. E., Laden, F., & Zanobetti, A. (2020). Racial Disparities in Associations between Neighborhood Demographic Polarization and Birth Weight. International Journal of Environmental Research and Public Health, 17(9), 3076. https://doi.org/10.3390/ijerph17093076