Scapular Dyskinesis: From Basic Science to Ultimate Treatment

 ,
, 
 , ,
, ,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Causes and Effects of SD
4. Clinical Examination
5. Treatment
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lefèvre-Colau, M.M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Recent advances in kinematics of the shoulder complex in healthy people. Ann. Phys. Rehabil. Med. 2018, 61, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Lefèvre-Colau, M.M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications. Ann. Phys. Rehabil. Med. 2018, 61, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Veeger, H.E.; van der Helm, F.C. Shoulder function: The perfect compromise between mobility and stability. J. Biomech. 2007, 40, 2119–2129. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Sciascia, A. The role of the scapula in preventing and treating shoulder instability. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 390–397. [Google Scholar] [CrossRef]
- Huang, T.S.; Huang, H.Y.; Wang, T.G.; Tsai, Y.S.; Lin, J.J. Comprehensive classification test of scapular dyskinesis: A reliability study. Man. Ther. 2015, 20, 427–432. [Google Scholar] [CrossRef]
- Merolla, G.; De Santis, E.; Sperling, J.W.; Campi, F.; Paladini, P.; Porcellini, G. Infraspinatus strength assessment before and after scapular muscles rehabilitation in professional volleyball players with scapular dyskinesis. J. Shoulder Elbow Surg. 2010, 19, 1256–1264. [Google Scholar] [CrossRef]
- Huang, T.S.; Ou, H.L.; Huang, C.Y.; Lin, J.J. Specific kinematics and associated muscle activation in individuals with scapular dyskinesis. J. Shoulder Elbow Surg. 2015, 24, 1227–1234. [Google Scholar] [CrossRef]
- Kibler, W.B.; Ludewig, P.M.; McClure, P.W.; Michener, L.A.; Bak, K.; Sciascia, A.D. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘Scapular Summit’. Br. J. Sports Med. 2013, 47, 877–885. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Berton, A.; Maffulli, N.; Denaro, V. Remplissage, humeral osteochondral grafts, weber osteotomy, and shoulder arthroplasty for the management of humeral bone defects in shoulder instability: Systematic review and quantitative synthesis of the literature. Arthroscopy 2014, 30, 1650–1666. [Google Scholar] [CrossRef]
- Depreli, Ö.; Angın, E. Review of scapular movement disorders among office workers having ergonomic risk. J. Back Musculoskelet. Rehabil. 2018, 31, 371–380. [Google Scholar] [CrossRef]
- Longo, U.G.; Petrillo, S.; Candela, V.; Rizzello, G.; Loppini, M.; Maffulli, N.; Denaro, V. Arthroscopic rotator cuff repair with and without subacromial decompression is safe and effective: A clinical study. BMC Musculoskelet. Disord. 2020, 21, 24. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.; Chen, K.; Ma, Y.; Chen, J.; Huang, M. The Influence of Test Positions on Clinical Assessment for Scapular Dyskinesis. PM R 2017, 9, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Johansson, F.R.; Borms, D.; Maenhout, A. Prevention of shoulder injuries in overhead athletes: A science-based approach. Braz. J. Phys. Ther. 2015, 19, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Warner, J.J.; Micheli, L.J.; Arslanian, L.E.; Kennedy, J.; Kennedy, R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moiré topographic analysis. Clin. Orthop. Relat. Res. 1992, 285, 191–199. [Google Scholar]
- Paletta, G.A.; Warner, J.J.; Warren, R.F.; Deutsch, A.; Altchek, D.W. Shoulder kinematics with two-plane x-ray evaluation in patients with anterior instability or rotator cuff tearing. J. Shoulder Elbow Surg. 1997, 6, 516–527. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. Shoulder injuries in overhead athletes. The “dead arm” revisited. Clin. Sports Med. 2000, 19, 125–158. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A.; Wilkes, T. Scapular dyskinesis and its relation to shoulder injury. J. Am. Acad. Orthop. Surg. 2012, 20, 364–372. [Google Scholar] [CrossRef]
- Kibler, W.B. The scapula in rotator cuff disease. Med. Sport Sci. 2012, 57, 27–40. [Google Scholar]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 546. [Google Scholar] [CrossRef]
- Longo, U.G.; Petrillo, S.; Loppini, M.; Candela, V.; Rizzello, G.; Maffulli, N.; Denaro, V. Metallic versus biodegradable suture anchors for rotator cuff repair: A case control study. BMC Musculoskelet. Disord. 2019, 20, 477. [Google Scholar] [CrossRef]
- Ou, H.L.; Huang, T.S.; Chen, Y.T.; Chen, W.Y.; Chang, Y.L.; Lu, T.W.; Chen, T.H.; Lin, J.J. Alterations of scapular kinematics and associated muscle activation specific to symptomatic dyskinesis type after conscious control. Man. Ther. 2016, 26, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Uhl, T.L.; Kibler, W.B.; Gecewich, B.; Tripp, B.L. Evaluation of clinical assessment methods for scapular dyskinesis. Arthroscopy 2009, 25, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Preziosi Standoli, J.; Fratalocchi, F.; Candela, V.; Preziosi Standoli, T.; Giannicola, G.; Bonifazi, M.; Gumina, S. Scapular Dyskinesis in Young, Asymptomatic Elite Swimmers. Orthop. J. Sports Med. 2018, 6, 2325967117750814. [Google Scholar] [CrossRef] [PubMed]
- Hickey, D.; Solvig, V.; Cavalheri, V.; Harrold, M.; Mckenna, L. Scapular dyskinesis increases the risk of future shoulder pain by 43% in asymptomatic athletes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Plummer, H.A.; Sum, J.C.; Pozzi, F.; Varghese, R.; Michener, L.A. Observational Scapular Dyskinesis: Known-Groups Validity in Patients With and Without Shoulder Pain. J. Orthop. Sports Phys. Ther. 2017, 47, 530–537. [Google Scholar] [CrossRef]
- Struyf, F.; Nijs, J.; Meeus, M.; Roussel, N.A.; Mottram, S.; Truijen, S.; Meeusen, R. Does scapular positioning predict shoulder pain in recreational overhead athletes? Int. J. Sports Med. 2014, 35, 75–82. [Google Scholar] [CrossRef]
- Miller, A.H.; Evans, K.; Adams, R.; Waddington, G.; Witchalls, J. Shoulder injury in water polo: A systematic review of incidence and intrinsic risk factors. J. Sci. Med. Sport 2018, 21, 368–377. [Google Scholar] [CrossRef]
- Chorley, J.; Eccles, R.E.; Scurfield, A. Care of Shoulder Pain in the Overhead Athlete. Pediatr. Ann. 2017, 46, e112–e113. [Google Scholar] [CrossRef]
- Burn, M.B.; McCulloch, P.C.; Lintner, D.M.; Liberman, S.R.; Harris, J.D. Prevalence of Scapular Dyskinesis in Overhead and Nonoverhead Athletes: A Systematic Review. Orthop. J. Sports Med. 2016, 4, 2325967115627608. [Google Scholar] [CrossRef]
- Andersson, S.H.; Bahr, R.; Clarsen, B.; Myklebust, G. Risk factors for overuse shoulder injuries in a mixed-sex cohort of 329 elite handball players: Previous findings could not be confirmed. Br. J. Sports Med. 2017. [CrossRef]
- Sanchez, H.M.; Sanchez, E.G.; Tavares, L.I. Association Between Scapular Dyskinesia and Shoulder Pain in Young Adults. Acta Ortop. Bras. 2016, 24, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.T.; Moon, J.; Lee, S.H.; Cho, K.H.; Im, S.H.; Kim, M.; Min, K. Changes in Activation of Serratus Anterior, Trapezius and Latissimus Dorsi With Slouched Posture. Ann. Rehabil. Med. 2016, 40, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Amorim, C.S.; Gracitelli, M.E.; Marques, A.P.; Alves, V.L. Effectiveness of global postural reeducation compared to segmental exercises on function, pain, and quality of life of patients with scapular dyskinesis associated with neck pain: A preliminary clinical trial. J. Manip. Physiol. Ther. 2014, 37, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cools, A.; Parlevliet, T.; Cagnie, B. Are chronic neck pain, scapular dyskinesis and altered scapulothoracic muscle activity interrelated?: A case-control study with surface and fine-wire EMG. J. Electromyogr. Kinesiol. 2016, 31, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Salvatore, G.; Rizzello, G.; Berton, A.; Ciuffreda, M.; Candela, V.; Denaro, V. The burden of rotator cuff surgery in Italy: A nationwide registry study. Arch. Orthop. Trauma Surg. 2017, 137, 217–224. [Google Scholar] [CrossRef]
- Cutti, A.G.; Parel, I.; Pellegrini, A.; Paladini, P.; Sacchetti, R.; Porcellini, G.; Merolla, G. The Constant score and the assessment of scapula dyskinesis: Proposal and assessment of an integrated outcome measure. J. Electromyogr. Kinesiol. 2016, 29, 81–89. [Google Scholar] [CrossRef]
- Salvatore, G.; Longo, U.G.; Candela, V.; Berton, A.; Migliorini, F.; Petrillo, S.; Ambrogioni, L.R.; Denaro, V. Epidemiology of rotator cuff surgery in Italy: Regional variation in access to health care. Results from a 14-year nationwide registry. Musculoskelet. Surg. 2019. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Papapietro, N.; Maffulli, N.; Denaro, V. Epidemiology, genetics and biological factors of rotator cuff tears. Med. Sport Sci. 2012, 57, 1–9. [Google Scholar]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. The Roman Bridge: A “double pulley—Suture bridges” technique for rotator cuff repair. BMC Musculoskelet. Disord. 2007, 8, 123. [Google Scholar] [CrossRef]
- Kibler, W.B. Scapular involvement in impingement: Signs and symptoms. Instr. Course. Lect. 2006, 55, 35–43. [Google Scholar]
- Kibler, W.B.; Sciascia, A.; Uhl, T. Medial scapular muscle detachment: Clinical presentation and surgical treatment. J. Shoulder Elbow Surg. 2014, 23, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Ciuffreda, M.; Locher, J.; Buchmann, S.; Maffulli, N.; Denaro, V. The effectiveness of conservative and surgical treatment for shoulder stiffness: A systematic review of current literature. Br. Med. Bull. 2018, 127, 111–143. [Google Scholar] [CrossRef] [PubMed]
- Shitara, H.; Kobayashi, T.; Yamamoto, A.; Shimoyama, D.; Ichinose, T.; Tajika, T.; Osawa, T.; Iizuka, H.; Takagishi, K. Prospective multifactorial analysis of preseason risk factors for shoulder and elbow injuries in high school baseball pitchers. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3303–3310. [Google Scholar] [CrossRef]
- Møller, M.; Nielsen, R.O.; Attermann, J.; Wedderkopp, N.; Lind, M.; Sørensen, H.; Myklebust, G. Handball load and shoulder injury rate: A 31-week cohort study of 679 elite youth handball players. Br. J. Sports Med. 2017, 51, 231–237. [Google Scholar] [CrossRef] [PubMed]
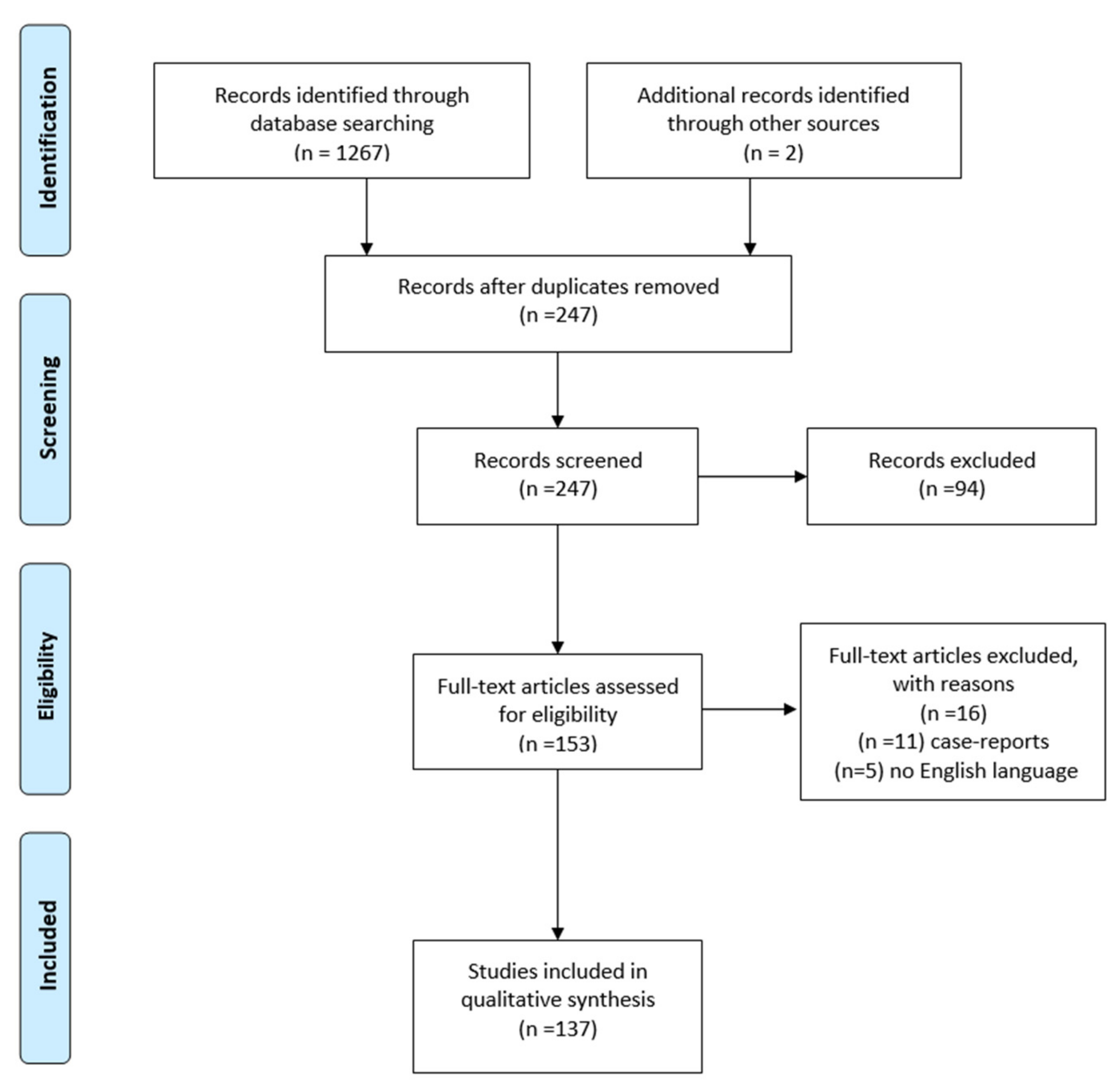
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Otoshi, K.; Takegami, M.; Sekiguchi, M.; Onishi, Y.; Yamazaki, S.; Otani, K.; Shishido, H.; Kikuchi, S.; Konno, S. Association between kyphosis and subacromial impingement syndrome: LOHAS study. J. Shoulder Elbow Surg. 2014, 23, e300–e307. [Google Scholar] [CrossRef]
- Gumina, S.; Di Giorgio, G.; Postacchini, F.; Postacchini, R. Subacromial space in adult patients with thoracic hyperkyphosis and in healthy volunteers. Chir. Organi. Mov. 2008, 91, 93–96. [Google Scholar] [CrossRef]
- Berthold, J.B.; Burg, T.M.; Nussbaum, R.P. Long Thoracic Nerve Injury Caused by Overhead Weight Lifting Leading to Scapular Dyskinesis and Medial Scapular Winging. J. Am. Osteopath. Assoc. 2017, 117, 133–137. [Google Scholar] [CrossRef]
- Brown, K.E.; Stickler, L. Shoulder pain and dysfunction secondary to neural injury. Int J. Sports Phys. Ther 2011, 6, 224–233. [Google Scholar]
- Umehara, J.; Nakamura, M.; Nishishita, S.; Tanaka, H.; Kusano, K.; Ichihashi, N. Scapular kinematic alterations during arm elevation with decrease in pectoralis minor stiffness after stretching in healthy individuals. J. Shoulder Elbow Surg. 2018, 27, 1214–1220. [Google Scholar] [CrossRef]
- Provencher, M.T.; Kirby, H.; McDonald, L.S.; Golijanin, P.; Gross, D.; Campbell, K.J.; LeClere, L.; Sanchez, G.; Anthony, S.; Romeo, A.A. Surgical Release of the Pectoralis Minor Tendon for Scapular Dyskinesia and Shoulder Pain. Am. J. Sports Med. 2017, 45, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Yeşilyaprak, S.S.; Yüksel, E.; Kalkan, S. Influence of pectoralis minor and upper trapezius lengths on observable scapular dyskinesis. Phys. Ther. Sport 2016, 19, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Uga, D.; Nakazawa, R.; Sakamoto, M. Strength and muscle activity of shoulder external rotation of subjects with and without scapular dyskinesis. J. Phys. Ther. Sci. 2016, 28, 1100–1105. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pires, E.D.; Camargo, P.R. Analysis of the kinetic chain in asymptomatic individuals with and without scapular dyskinesis. Clin. Biomech. (Bristol, Avon) 2018, 54, 8–15. [Google Scholar] [CrossRef]
- Seitz, A.L.; McClelland, R.I.; Jones, W.J.; Jean, R.A.; Kardouni, J.R. A Comparison Of Change in 3d Scapular Kinematics with Maximal Contractions and Force Production with Scapular Muscle Tests Between Asymptomatic Overhead Athletes with and Without Scapular Dyskinesis. Int. J. Sports Phys. Ther. 2015, 10, 309–318. [Google Scholar]
- Alibazi, R.J.; Moghadam, A.N.; Cools, A.M.; Bakhshi, E.; Ahari, A.A. The Effect of Shoulder Muscle Fatigue on Acromiohumeral Distance and Scapular Dyskinesis in Women with Generalized Joint Hypermobility. J. Appl. Biomech. 2017, 33, 424–430. [Google Scholar] [CrossRef]
- Gaudet, S.; Tremblay, J.; Dal Maso, F. Evolution of muscular fatigue in periscapular and rotator cuff muscles during isokinetic shoulder rotations. J. Sports Sci. 2018, 36, 2121–2128. [Google Scholar] [CrossRef]
- Hannah, D.C.; Scibek, J.S.; Carcia, C.R. Strength Profiles In Healthy Individuals with and without Scapular Dyskinesis. Int. J. Sports Phys. Ther. 2017, 12, 305–313. [Google Scholar]
- Noguchi, M.; Chopp, J.N.; Borgs, S.P.; Dickerson, C.R. Scapular orientation following repetitive prone rowing: Implications for potential subacromial impingement mechanisms. J. Electromyogr. Kinesiol. 2013, 23, 1356–1361. [Google Scholar] [CrossRef]
- Depalma, M.J.; Johnson, E.W. Detecting and treating shoulder impingement syndrome: The role of scapulothoracic dyskinesis. Phys. Sportsmed. 2003, 31, 25–32. [Google Scholar] [CrossRef]
- Savoie, F.H.; O’Brien, M.J. Anterior instability in the throwing shoulder. Sports Med. Arthrosc. Rev. 2014, 22, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, E.W.; Dengerink, D.D. Common conditions in the overhead athlete. Am. Fam. Physician 2014, 89, 537–541. [Google Scholar] [PubMed]
- Murena, L.; Canton, G.; Vulcano, E.; Cherubino, P. Scapular dyskinesis and SICK scapula syndrome following surgical treatment of type III acute acromioclavicular dislocations. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Gumina, S.; Carbone, S.; Postacchini, F. Scapular dyskinesis and SICK scapula syndrome in patients with chronic type III acromioclavicular dislocation. Arthroscopy 2009, 25, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, D.; Jang, Y.; Yeom, J.; Banks, S.A. Effects of short malunion of the clavicle on in vivo scapular kinematics. J. Shoulder Elbow Surg. 2017, 26, e286–e292. [Google Scholar] [CrossRef]
- Cisneros, L.N.; Reiriz, J.S. Management of chronic unstable acromioclavicular joint injuries. J. Orthop. Traumatol. 2017, 18, 305–318. [Google Scholar] [CrossRef]
- Natera-Cisneros, L.; Sarasquete-Reiriz, J.; Escolà-Benet, A.; Rodriguez-Miralles, J. Acute high-grade acromioclavicular joint injuries treatment: Arthroscopic non-rigid coracoclavicular fixation provides better quality of life outcomes than hook plate ORIF. Orthop. Traumatol. Surg. Res. 2016, 102, 31–39. [Google Scholar] [CrossRef]
- Kim, E.; Lee, S.; Jeong, H.J.; Park, J.H.; Park, S.J.; Lee, J.; Kim, W.; Park, H.J.; Lee, S.Y.; Murase, T.; et al. Three-dimensional scapular dyskinesis in hook-plated acromioclavicular dislocation including hook motion. J. Shoulder Elbow Surg. 2018, 27, 1117–1124. [Google Scholar] [CrossRef]
- Osias, W.; Matcuk, G.R.; Skalski, M.R.; Patel, D.B.; Schein, A.J.; Hatch, G.F.R.; White, E.A. Scapulothoracic pathology: Review of anatomy, pathophysiology, imaging findings, and an approach to management. Skeletal. Radiol. 2018, 47, 161–171. [Google Scholar] [CrossRef]
- Han, K.J.; Cho, J.H.; Han, S.H.; Hyun, H.S.; Lee, D.H. Subacromial impingement syndrome secondary to scapulothoracic dyskinesia. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1958–1960. [Google Scholar] [CrossRef]
- Buss, D.D.; Freehill, M.Q.; Marra, G. Typical and atypical shoulder impingement syndrome: Diagnosis, treatment, and pitfalls. Instr. Course. Lect. 2009, 58, 447–457. [Google Scholar] [PubMed]
- Navlet, M.G.; Asenjo-Gismero, C.V. Multidirectional Instability: Natural History and Evaluation. Open Orthop. J. 2017, 11, 861–874. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lopes, A.D.; Timmons, M.K.; Grover, M.; Ciconelli, R.M.; Michener, L.A. Visual scapular dyskinesis: Kinematics and muscle activity alterations in patients with subacromial impingement syndrome. Arch. Phys. Med. Rehabil. 2015, 96, 298–306. [Google Scholar] [CrossRef] [PubMed]
- McClure, P.W.; Michener, L.A.; Sennett, B.J.; Karduna, A.R. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J. Shoulder Elbow Surg. 2001, 10, 269–277. [Google Scholar] [CrossRef]
- Shields, E.; Behrend, C.; Beiswenger, T.; Strong, B.; English, C.; Maloney, M.; Voloshin, I. Scapular dyskinesis following displaced fractures of the middle clavicle. J. Shoulder Elbow Surg. 2015, 24, e331–e336. [Google Scholar] [CrossRef]
- Longo, U.G.; Facchinetti, G.; Marchetti, A.; Candela, V.; Risi Ambrogioni, L.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Sleep Disturbance and Rotator Cuff Tears: A Systematic Review. Medicina (Kaunas) 2019, 55, 453. [Google Scholar] [CrossRef]
- Kim, E.; Park, J.H.; Han, B.R.; Park, H.J.; Lee, S.Y.; Murase, T.; Sugamoto, K.; Ikemoto, S.; Park, S.J. In Vivo Analysis of Three-Dimensional Dynamic Scapular Dyskinesis in Scapular or Clavicular Fractures. Acta Med. Okayama 2017, 71, 151–159. [Google Scholar]
- Rubright, J.; Kelleher, P.; Beardsley, C.; Paller, D.; Shackford, S.; Beynnon, B.; Shafritz, A. Long-term clinical outcomes, motion, strength, and function after total claviculectomy. J. Shoulder Elbow Surg. 2014, 23, 236–244. [Google Scholar] [CrossRef]
- Carbone, S.; Moroder, P.; Runer, A.; Resch, H.; Gumina, S.; Hertel, R. Scapular dyskinesis after Latarjet procedure. J. Shoulder Elbow Surg. 2016, 25, 422–427. [Google Scholar] [CrossRef]
- Kolk, A.; de Witte, P.B.; Henseler, J.F.; van Zwet, E.W.; van Arkel, E.R.; van der Zwaal, P.; Nelissen, R.G.; de Groot, J.H. Three-dimensional shoulder kinematics normalize after rotator cuff repair. J. Shoulder Elbow Surg. 2016, 25, 881–889. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Petrillo, S.; Loppini, M.; Maffulli, N.; Denaro, V. Conservative Rehabilitation Provides Superior Clinical Results Compared to Early Aggressive Rehabilitation for Rotator Cuff Repair: A Retrospective Comparative Study. Medicina (Kaunas) 2019, 55, 402. [Google Scholar] [CrossRef] [PubMed]
- Fedoriw, W.W.; Ramkumar, P.; McCulloch, P.C.; Lintner, D.M. Return to play after treatment of superior labral tears in professional baseball players. Am. J. Sports Med. 2014, 42, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.B.; Laudner, K.G.; Pasquale, M.R.; Bradley, J.P.; Lephart, S.M. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am. J. Sports Med. 2006, 34, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Abrams, G.D.; Safran, M.R. Diagnosis and management of superior labrum anterior posterior lesions in overhead athletes. Br. J. Sports Med. 2010, 44, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, C.; Turgut, E.; Baltaci, G. Distal radius fractures result in alterations in scapular kinematics: A three-dimensional motion analysis. Clin. Biomech. (Bristol, Avon) 2015, 30, 296–301. [Google Scholar] [CrossRef]
- Park, S.Y.; Yoo, W.G. Activation of the serratus anterior and upper trapezius in a population with winged and tipped scapulae during push-up-plus and diagonal shoulder-elevation. J. Back Musculoskelet. Rehabil. 2015, 28, 7–12. [Google Scholar] [CrossRef]
- Longo, U.G.; Candela, V.; Berton, A.; Salvatore, G.; Guarnieri, A.; DeAngelis, J.; Nazarian, A.; Denaro, V. Genetic basis of rotator cuff injury: A systematic review. BMC Med. Genet. 2019, 20, 149. [Google Scholar] [CrossRef]
- Kawasaki, T.; Maki, N.; Shimizu, K.; Ota, C.; Urayama, S.; Moriya, S.; Kaketa, T.; Kobayashi, H.; Kaneko, K. Do stingers affect scapular kinematics in rugby players? J. Shoulder Elbow Surg. 2014, 23, e293–e299. [Google Scholar] [CrossRef]
- Kawasaki, T.; Yamakawa, J.; Kaketa, T.; Kobayashi, H.; Kaneko, K. Does scapular dyskinesis affect top rugby players during a game season? J. Shoulder Elbow Surg. 2012, 21, 709–714. [Google Scholar] [CrossRef]
- DiVeta, J.; Walker, M.L.; Skibinski, B. Relationship between performance of selected scapular muscles and scapular abduction in standing subjects. Phys. Ther. 1990, 70, 470–476, discussion 476–479. [Google Scholar] [CrossRef]
- Johnson, M.P.; McClure, P.W.; Karduna, A.R. New method to assess scapular upward rotation in subjects with shoulder pathology. J. Orthop. Sports Phys. Ther. 2001, 31, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Odom, C.J.; Taylor, A.B.; Hurd, C.E.; Denegar, C.R. Measurement of scapular asymetry and assessment of shoulder dysfunction using the Lateral Scapular Slide Test: A reliability and validity study. Phys. Ther. 2001, 81, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.E.; Blankenship, K.R.; Robb, J.B.; Walker, M.J.; Bryan, J.M.; Stetts, D.M.; Mincey, L.M.; Simmons, G.E. Investigation of the validity and reliability of four objective techniques for measuring forward shoulder posture. J. Orthop. Sports Phys. Ther. 1997, 25, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Balster, S.M.; Finch, C.; Dalziel, R. Measurement of scapula upward rotation: A reliable clinical procedure. Br. J. Sports Med. 2005, 39, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Du, W.Y.; Huang, T.S.; Hsu, K.C.; Lin, J.J. Measurement of scapular medial border and inferior angle prominence using a novel scapulometer: A reliability and validity study. Musculoskelet. Sci. Pract. 2017, 32, 120–126. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.; McCaffrey, N.; Whyte, E.; Moran, K. The Development and Reliability of a Simple Field-Based Screening Tool to Assess for Scapular Dyskinesis. J. Sport Rehabil. 2016, 25. [Google Scholar] [CrossRef]
- van den Noort, J.C.; Wiertsema, S.H.; Hekman, K.M.C.; Schönhuth, C.P.; Dekker, J.; Harlaar, J. Reliability and precision of 3D wireless measurement of scapular kinematics. Med. Biol. Eng. Comput. 2014, 52, 921–931. [Google Scholar] [CrossRef]
- Shadmehr, A.; Bagheri, H.; Ansari, N.N.; Sarafraz, H. The reliability measurements of lateral scapular slide test at three different degrees of shoulder joint abduction. Br. J. Sports Med. 2010, 44, 289–293. [Google Scholar] [CrossRef]
- Kopkow, C.; Lange, T.; Schmitt, J.; Kasten, P. Interrater reliability of the modified scapular assistance test with and without handheld weights. Man. Ther. 2015, 20, 868–874. [Google Scholar] [CrossRef]
- Baumgarten, K.M.; Osborn, R.; Schweinle, W.E.; Eidsness, J.; Schelhaas, D. A novel technique for determining scapulohumeral translation: A case-control and inter-rater reliability study. Int. J. Sports Phys. Ther. 2012, 7, 39–48. [Google Scholar]
- Ludewig, P.M.; Phadke, V.; Braman, J.P.; Hassett, D.R.; Cieminski, C.J.; LaPrade, R.F. Motion of the shoulder complex during multiplanar humeral elevation. J. Bone Joint Surg. Am. 2009, 91, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.M.; Juul-Kristensen, B.; Lund, H.; Søgaard, K. Measurement properties of existing clinical assessment methods evaluating scapular positioning and function. A systematic review. Physiother. Theory Pract. 2014, 30, 453–482. [Google Scholar] [CrossRef] [PubMed]
- Ellenbecker, T.S.; Kibler, W.B.; Bailie, D.S.; Caplinger, R.; Davies, G.J.; Riemann, B.L. Reliability of scapular classification in examination of professional baseball players. Clin. Orthop. Relat. Res. 2012, 470, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Barnes, M.J.; Leddon, C.E.; Van Ryssegem, G.; Alamar, B. Reliability of the sitting hand press-up test for identifying and quantifying the level of scapular medial border posterior displacement in overhead athletes. Int. J. Sports Phys. Ther. 2011, 6, 306–311. [Google Scholar]
- Miachiro, N.Y.; Camarini, P.M.; Tucci, H.T.; McQuade, K.J.; Oliveira, A.S. Can clinical observation differentiate individuals with and without scapular dyskinesis? Braz. J. Phys. Ther. 2014, 18, 282–289. [Google Scholar] [CrossRef]
- Chen, K.; Deng, S.; Ma, Y.; Yao, Y.; Chen, J.; Zhang, Y. A preliminary exploration of plain-film radiography in scapular dyskinesis evaluation. J. Shoulder Elbow Surg. 2018, 27, e210–e218. [Google Scholar] [CrossRef]
- Huang, T.S.; Lin, J.J.; Ou, H.L.; Chen, Y.T. Movement Pattern of Scapular Dyskinesis in Symptomatic Overhead Athletes. Sci. Rep. 2017, 7, 6621. [Google Scholar] [CrossRef]
- Park, J.Y.; Noh, Y.M.; Chung, S.W.; Moon, S.G.; Ha, D.H.; Lee, K.S. Bennett lesions in baseball players detected by magnetic resonance imaging: Assessment of association factors. J. Shoulder Elbow Surg. 2016, 25, 730–738. [Google Scholar] [CrossRef]
- Bell, S.N.; Troupis, J.M.; Miller, D.; Alta, T.D.; Coghlan, J.A.; Wijeratna, M.D. Four-dimensional computed tomography scans facilitate preoperative planning in snapping scapula syndrome. J. Shoulder Elbow Surg. 2015, 24, e83–e90. [Google Scholar] [CrossRef]
- Morita, W.; Nozaki, T.; Tasaki, A. MRI for the diagnosis of scapular dyskinesis: A report of two cases. Skeletal. Radiol. 2017, 46, 249–252. [Google Scholar] [CrossRef]
- Park, J.Y.; Hwang, J.T.; Kim, K.M.; Makkar, D.; Moon, S.G.; Han, K.J. How to assess scapular dyskinesis precisely: 3-dimensional wing computer tomography—A new diagnostic modality. J. Shoulder Elbow Surg. 2013, 22, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Rossi, D.M.; Pedroni, C.R.; Martins, J.; de Oliveira, A.S. Intrarater and interrater reliability of three classifications for scapular dyskinesis in athletes. PLoS ONE 2017, 12, e0181518. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Wassinger, C.A.; Frank, M.; Michener, L.A.; Hegedus, E.J. Diagnostic accuracy of scapular physical examination tests for shoulder disorders: A systematic review. Br. J. Sports Med. 2013, 47, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, D.H.; Møller, A.D.; Vestergaard, J.M.; Mose, S.; Maribo, T. The scapular dyskinesis test: Reliability, agreement, and predictive value in patients with subacromial impingement syndrome. J. Hand Ther. 2017, 30, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Tsuruike, M.; Ellenbecker, T.S. Adaptation of muscle activity in scapular dyskinesis test for collegiate baseball players. J. Shoulder Elbow Surg. 2016, 25, 1583–1591. [Google Scholar] [CrossRef]
- Longo, U.G.; Margiotti, K.; Petrillo, S.; Rizzello, G.; Fusilli, C.; Maffulli, N.; De Luca, A.; Denaro, V. Genetics of rotator cuff tears: No association of col5a1 gene in a case-control study. BMC Med. Genet. 2018, 19, 217. [Google Scholar] [CrossRef]
- Yoo, W.G. Effect of the dual-wall pushup plus exercise in patients with scapular dyskinesis with a winged or tipped scapula. J. Phys. Ther. Sci. 2015, 27, 2661–2662. [Google Scholar] [CrossRef][Green Version]
- Lee, J.H.; Cynn, H.S.; Choi, W.J.; Jeong, H.J.; Yoon, T.L. Reliability of levator scapulae index in subjects with and without scapular downward rotation syndrome. Phys. Ther. Sport 2016, 19, 1–6. [Google Scholar] [CrossRef]
- Basar, S.; Citaker, S.; Kanatli, U.; Ozturk, B.Y.; Kilickap, S.; Kafa, N.K. Assessment of function in patients with rotator cuff tears: Functional test versus self-reported questionnaire. Int. J. Shoulder Surg. 2014, 8, 107–113. [Google Scholar] [CrossRef]
- Merolla, G.; De Santis, E.; Campi, F.; Paladini, P.; Porcellini, G. Infraspinatus scapular retraction test: A reliable and practical method to assess infraspinatus strength in overhead athletes with scapular dyskinesis. J. Orthop. Traumatol. 2010, 11, 105–110. [Google Scholar] [CrossRef]
- Juul-Kristensen, B.; Hilt, K.; Enoch, F.; Remvig, L.; Sjøgaard, G. Scapular dyskinesis in trapezius myalgia and intraexaminer reproducibility of clinical tests. Physiother. Theory Pract. 2011, 27, 492–502. [Google Scholar] [CrossRef]
- van den Noort, J.C.; Wiertsema, S.H.; Hekman, K.M.; Schönhuth, C.P.; Dekker, J.; Harlaar, J. Measurement of scapular dyskinesis using wireless inertial and magnetic sensors: Importance of scapula calibration. J. Biomech. 2015, 48, 3460–3468. [Google Scholar] [CrossRef]
- Haik, M.N.; Alburquerque-Sendín, F.; Camargo, P.R. Reliability and minimal detectable change of 3-dimensional scapular orientation in individuals with and without shoulder impingement. J. Orthop. Sports Phys. Ther. 2014, 44, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Rapp, E.A.; Richardson, R.T.; Russo, S.A.; Rose, W.C.; Richards, J.G. A comparison of two non-invasive methods for measuring scapular orientation in functional positions. J. Biomech. 2017, 61, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Maor, M.B.; Ronin, T.; Kalichman, L. Scapular dyskinesis among competitive swimmers. J. Bodyw. Mov. Ther. 2017, 21, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Rich, R.L.; Struminger, A.H.; Tucker, W.S.; Munkasy, B.A.; Joyner, A.B.; Buckley, T.A. Scapular Upward-Rotation Deficits After Acute Fatigue in Tennis Players. J. Athl. Train. 2016, 51, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Rogowski, I.; Creveaux, T.; Chèze, L.; Dumas, R. Scapulothoracic kinematics during tennis forehand drive. Sports Biomech. 2014, 13, 166–175. [Google Scholar] [CrossRef]
- Silva, R.T.; Hartmann, L.G.; Laurino, C.F.; Biló, J.P. Clinical and ultrasonographic correlation between scapular dyskinesia and subacromial space measurement among junior elite tennis players. Br. J. Sports Med. 2010, 44, 407–410. [Google Scholar] [CrossRef]
- Matzkin, E.; Suslavich, K.; Wes, D. Swimmer’s Shoulder: Painful Shoulder in the Competitive Swimmer. J. Am. Acad. Orthop. Surg. 2016, 24, 527–536. [Google Scholar] [CrossRef]
- Seitz, A.L.; McClure, P.W.; Lynch, S.S.; Ketchum, J.M.; Michener, L.A. Effects of scapular dyskinesis and scapular assistance test on subacromial space during static arm elevation. J. Shoulder Elbow Surg. 2012, 21, 631–640. [Google Scholar] [CrossRef]
- Kibler, W.B.; McMullen, J. Scapular dyskinesis and its relation to shoulder pain. J. Am. Acad. Orthop. Surg. 2003, 11, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B. The role of the scapula in athletic shoulder function. Am. J. Sports Med. 1998, 26, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Umehara, J.; Nakamura, M.; Fujita, K.; Kusano, K.; Nishishita, S.; Araki, K.; Tanaka, H.; Yanase, K.; Ichihashi, N. Shoulder horizontal abduction stretching effectively increases shear elastic modulus of pectoralis minor muscle. J. Shoulder Elbow Surg. 2017, 26, 1159–1165. [Google Scholar] [CrossRef]
- Morais, N.; Cruz, J. The pectoralis minor muscle and shoulder movement-related impairments and pain: Rationale, assessment and management. Phys. Ther. Sport 2016, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Başkurt, Z.; Başkurt, F.; Gelecek, N.; Özkan, M.H. The effectiveness of scapular stabilization exercise in the patients with subacromial impingement syndrome. J. Back Musculoskelet. Rehabil. 2011, 24, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Turgut, E.; Duzgun, I.; Baltaci, G. Effects of Scapular Stabilization Exercise Training on Scapular Kinematics, Disability, and Pain in Subacromial Impingement: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 10, 1915–1923. [Google Scholar] [CrossRef]
- De Mey, K.; Danneels, L.; Cagnie, B.; Borms, D.; T’Jonck, Z.; Van Damme, E.; Cools, A.M. Shoulder muscle activation levels during four closed kinetic chain exercises with and without Redcord slings. J. Strength Cond. Res. 2014, 28, 1626–1635. [Google Scholar] [CrossRef]
- Pirauá, A.L.T.; Pitangui, A.C.R.; Silva, J.P.; dos Passos, M.H.P.; de Oliveira, V.M.A.; Batista, L.D.S.P.; de Araújo, R.C. Electromyographic analysis of the serratus anterior and trapezius muscles during push-ups on stable and unstable bases in subjects with scapular dyskinesis. J. Electromyogr. Kinesiol. 2014, 24, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Pizzari, T.; Wickham, J.; Balster, S.; Ganderton, C.; Watson, L. Modifying a shrug exercise can facilitate the upward rotator muscles of the scapula. Clin. Biomech. (Bristol, Avon) 2014, 29, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Cynn, H.S.; Choi, W.J.; Jeong, H.J.; Yoon, T.L. Various shrug exercises can change scapular kinematics and scapular rotator muscle activities in subjects with scapular downward rotation syndrome. Hum. Mov. Sci. 2016, 45, 119–129. [Google Scholar] [CrossRef]
- Walker, D.L.; Hickey, C.J.; Tregoning, M.B. The Effect Of Electrical Stimulation Versus Sham Cueing on Scapular Position During Exercise in Patients with Scapular Dyskinesis. Int. J. Sports Phys. Ther. 2017, 12, 425–436. [Google Scholar]
- Carbone, S.; Postacchini, R.; Gumina, S. Scapular dyskinesis and SICK syndrome in patients with a chronic type III acromioclavicular dislocation. Results of rehabilitation. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1473–1480. [Google Scholar] [CrossRef]
- Rasmont, Q.; Delloye, C.; Bigare, E.; Van Isacker, T. Is conservative treatment still defensible in grade III acromioclavicular dislocation? Are there predictive factors of poor outcome? Acta Orthop. Belg. 2015, 81, 107–114. [Google Scholar] [PubMed]
- Huang, T.S.; Ou, H.L.; Lin, J.J. Effects of trapezius kinesio taping on scapular kinematics and associated muscular activation in subjects with scapular dyskinesis. J. Hand Ther. 2017, 32, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Intelangelo, L.; Bordachar, D.; Barbosa, A.W. Effects of scapular taping in young adults with shoulder pain and scapular dyskinesis. J. Bodyw. Mov. Ther. 2016, 20, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Wellmann, M.; Pastor, M.F.; Smith, T. Diagnostics and treatment of posterior shoulder instability. Unfallchirurg 2018, 121, 134–141. [Google Scholar] [CrossRef]
- Keramat, K.U. Conservative treatment preferences and the plausible mechanism of Neer’s stage 1 of shoulder impingement in younger people. J. Pak. Med. Assoc. 2015, 65, 542–547. [Google Scholar]
- Pekyavas, N.O.; Ergun, N. Comparison of virtual reality exergaming and home exercise programs in patients with subacromial impingement syndrome and scapular dyskinesis: Short term effect. Acta Orthop. Traumatol. Turc. 2017, 51, 238–242. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U. Conservative management for tendinopathy: Is there enough scientific evidence? Rheumatology 2008, 47, 390–391. [Google Scholar] [CrossRef]
- Kolk, A.; Henseler, J.F.; de Witte, P.B.; van Arkel, E.R.; Visser, C.P.; Nagels, J.; Nelissen, R.G.; de Groot, J.H. Subacromial anaesthetics increase asymmetry of scapular kinematics in patients with subacromial pain syndrome. Man. Ther. 2016, 26, 31–37. [Google Scholar] [CrossRef]
- Pellegrini, A.; Pogliacomi, F.; Costantino, C.; Desimoni, S.; Giovanelli, M.; Golz, A.; Tonino, P.; Ceccarelli, F. Does scapula stabilizing t-shirt help over-head athletes in shoulder discomfort? A randomized control study. Acta Biomed. 2016, 87, 84–89. [Google Scholar] [PubMed]
- Thomas, S.J.; Swanik, K.A.; Swanik, C.B.; Kelly, J.D. Internal rotation and scapular position differences: A comparison of collegiate and high school baseball players. J. Athl. Train. 2010, 45, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.J.; Visco, C.J.; Press, J. Current concepts for shoulder training in the overhead athlete. Curr. Sports Med. Rep. 2009, 8, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Konda, S.; Yanai, T.; Sakurai, S. Configuration of the Shoulder Complex During the Arm-Cocking Phase in Baseball Pitching. Am. J. Sports Med. 2015, 43, 2445–2451. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.G.; Moline, M.T.; Meister, K. The relationship between forward scapular posture and posterior shoulder tightness among baseball players. Am. J. Sports Med. 2010, 38, 2106–2112. [Google Scholar] [CrossRef] [PubMed]
- Bak, K. The practical management of swimmer’s painful shoulder: Etiology, diagnosis, and treatment. Clin. J. Sport Med. 2010, 20, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Corpus, K.T.; Camp, C.L.; Dines, D.M.; Altchek, D.W.; Dines, J.S. Evaluation and treatment of internal impingement of the shoulder in overhead athletes. World J. Orthop. 2016, 7, 776–784. [Google Scholar] [CrossRef]
- Pellegrini, A.; Tonino, P.; Salazar, D.; Hendrix, K.; Parel, I.; Cutti, A.; Paladini, P.; Ceccarelli, F.; Porcellini, G. Can posterior capsular stretching rehabilitation protocol change scapula kinematics in asymptomatic baseball pitchers? Musculoskelet. Surg. 2016, 100, 39–43. [Google Scholar] [CrossRef]
- Lenetsky, S.; Brughelli, M.; Harris, N.K. Shoulder function and scapular position in boxers. Phys. Ther. Sport 2015, 16, 355–360. [Google Scholar] [CrossRef]
- Merolla, G.; De Santis, E.; Campi, F.; Paladini, P.; Porcellini, G. Supraspinatus and infraspinatus weakness in overhead athletes with scapular dyskinesis: Strength assessment before and after restoration of scapular musculature balance. Musculoskelet. Surg. 2010, 94, 119–125. [Google Scholar] [CrossRef]
- Kim, J.T.; Kim, S.Y.; Oh, D.W. An 8-week scapular stabilization exercise program in an elite archer with scapular dyskinesis presenting joint noise: A case report with one-year follow-up. Physiother. Theory Pract. 2018, 35, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.J.; Hung, C.J.; Yang, C.C.; Chen, H.Y.; Chou, F.C.; Lu, T.W. Activation and tremor of the shoulder muscles to the demands of an archery task. J. Sports Sci. 2010, 28, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.H.; Bahr, R.; Clarsen, B.; Myklebust, G. Preventing overuse shoulder injuries among throwing athletes: A cluster-randomised controlled trial in 660 elite handball players. Br. J. Sports Med. 2017, 51, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Bahr, R.; Andersson, S.H.; Munk, R.; Myklebust, G. Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: A prospective cohort study. Br. J. Sports Med. 2014, 48, 1327–1333. [Google Scholar] [CrossRef]
- Thomas, S.J.; Swanik, K.A.; Swanik, C.; Huxel, K.C. Glenohumeral rotation and scapular position adaptations after a single high school female sports season. J. Athl. Train. 2009, 44, 230–237. [Google Scholar] [CrossRef]
- Tate, A.; Turner, G.N.; Knab, S.E.; Jorgensen, C.; Strittmatter, A.; Michener, L.A. Risk factors associated with shoulder pain and disability across the lifespan of competitive swimmers. J. Athl. Train. 2012, 47, 149–158. [Google Scholar] [CrossRef]
- Madsen, P.H.; Bak, K.; Jensen, S.; Welter, U. Training induces scapular dyskinesis in pain-free competitive swimmers: A reliability and observational study. Clin. J. Sport Med. 2011, 21, 109–113. [Google Scholar] [CrossRef]
- Cools, A.M.; Declercq, G.; Cagnie, B.; Cambier, D.; Witvrouw, E. Internal impingement in the tennis player: rehabilitation guidelines. Br. J. Sports Med. 2008, 42, 165–171. [Google Scholar] [CrossRef]
- Werner, C.M.; Ruckstuhl, T.; Zingg, P.; Lindenmeyer, B.; Klammer, G.; Gerber, C. Correlation of psychomotor findings and the outcome of a physical therapy program to treat scapular dyskinesis. J. Shoulder Elbow Surg. 2011, 20, 69–72. [Google Scholar] [CrossRef]
- Tonin, K.; Stražar, K.; Burger, H.; Vidmar, G. Adaptive changes in the dominant shoulders of female professional overhead athletes: Mutual association and relation to shoulder injury. Int. J. Rehabil. Res. 2013, 36, 228–235. [Google Scholar] [CrossRef]
- Longo, U.G.; Ciuffreda, M.; Rizzello, G.; Mannering, N.; Maffulli, N.; Denaro, V. Surgical versus conservative management of Type III acromioclavicular dislocation: A systematic review. Br. Med. Bull. 2017, 122, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Boutsiadis, A.; Baverel, L.; Lenoir, H.; Delsol, P.; Barth, J. Arthroscopic-assisted Acromioclavicular and Coracoclavicular Ligaments Reconstruction for Chronic Acromioclavicular Dislocations: Surgical Technique. Tech. Hand Up Extrem. Surg. 2016, 20, 172–178. [Google Scholar] [CrossRef]
- Groh, G.I.; Mighell, M.A.; Basamania, C.J.; Kibler, W.B. All Things Clavicle: From Acromioclavicular to Sternoclavicular and All Points in Between. Instr. Course. Lect. 2016, 65, 181–196. [Google Scholar] [PubMed]
- Oki, S.; Matsumura, N.; Iwamoto, W.; Ikegami, H.; Kiriyama, Y.; Nakamura, T.; Toyama, Y.; Nagura, T. The function of the acromioclavicular and coracoclavicular ligaments in shoulder motion: A whole-cadaver study. Am. J. Sports Med. 2012, 40, 2617–2626. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuseppe, L.U.; Laura, R.A.; Berton, A.; Candela, V.; Massaroni, C.; Carnevale, A.; Stelitano, G.; Schena, E.; Nazarian, A.; DeAngelis, J.; et al. Scapular Dyskinesis: From Basic Science to Ultimate Treatment. Int. J. Environ. Res. Public Health 2020, 17, 2974. https://doi.org/10.3390/ijerph17082974
Giuseppe LU, Laura RA, Berton A, Candela V, Massaroni C, Carnevale A, Stelitano G, Schena E, Nazarian A, DeAngelis J, et al. Scapular Dyskinesis: From Basic Science to Ultimate Treatment. International Journal of Environmental Research and Public Health. 2020; 17(8):2974. https://doi.org/10.3390/ijerph17082974
Chicago/Turabian StyleGiuseppe, Longo Umile, Risi Ambrogioni Laura, Alessandra Berton, Vincenzo Candela, Carlo Massaroni, Arianna Carnevale, Giovanna Stelitano, Emiliano Schena, Ara Nazarian, Joseph DeAngelis, and et al. 2020. "Scapular Dyskinesis: From Basic Science to Ultimate Treatment" International Journal of Environmental Research and Public Health 17, no. 8: 2974. https://doi.org/10.3390/ijerph17082974
APA StyleGiuseppe, L. U., Laura, R. A., Berton, A., Candela, V., Massaroni, C., Carnevale, A., Stelitano, G., Schena, E., Nazarian, A., DeAngelis, J., & Denaro, V. (2020). Scapular Dyskinesis: From Basic Science to Ultimate Treatment. International Journal of Environmental Research and Public Health, 17(8), 2974. https://doi.org/10.3390/ijerph17082974