Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions

 , , ,
, , ,  , ,
, ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
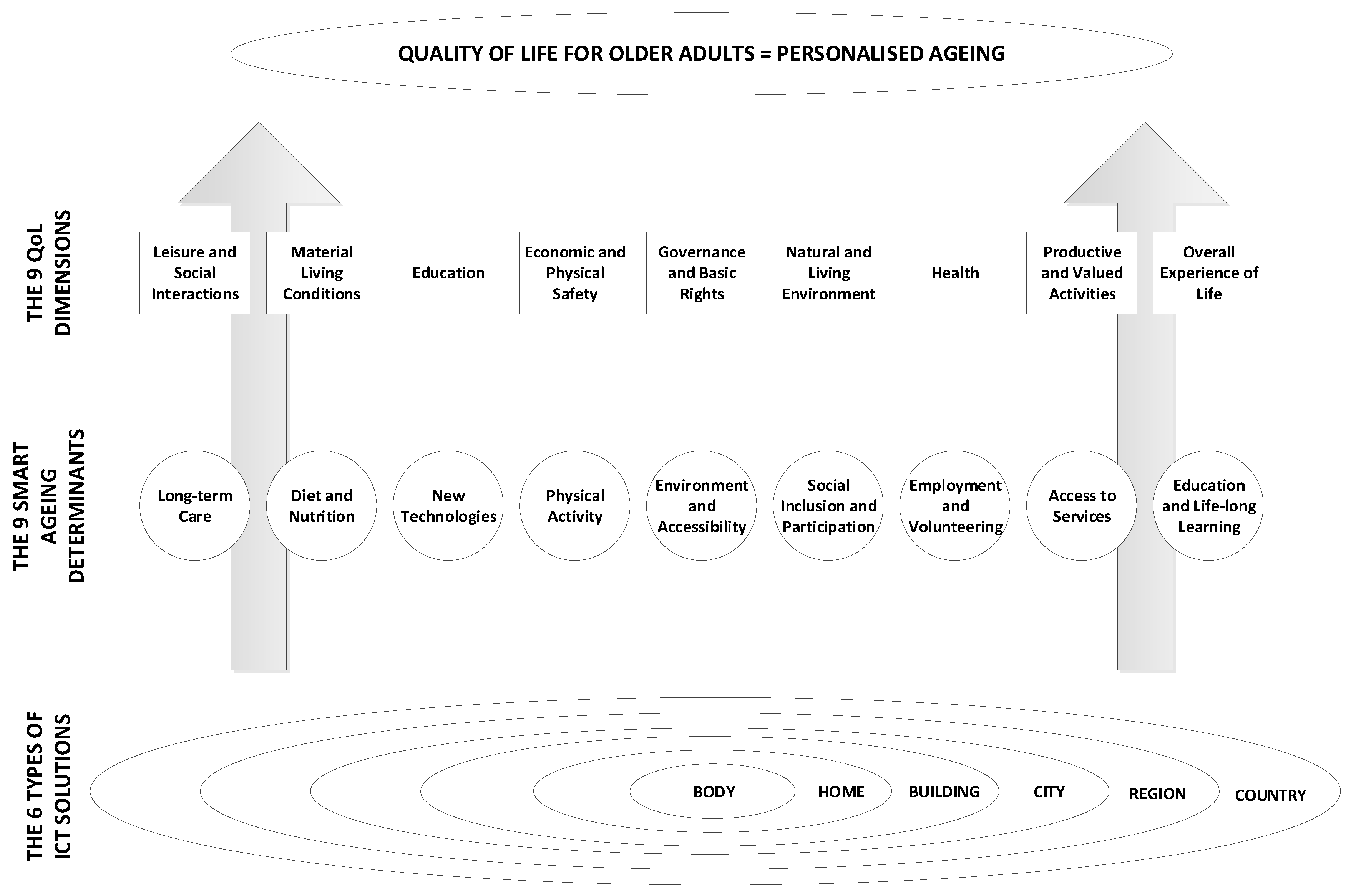
2. The Framework for Quality of Life and Personalised Ageing
2.1. Quality of Life
2.2. Smart Ageing
2.3. The Framework—A Contribution of ICT Solutions
2.3.1. Horizontal Component
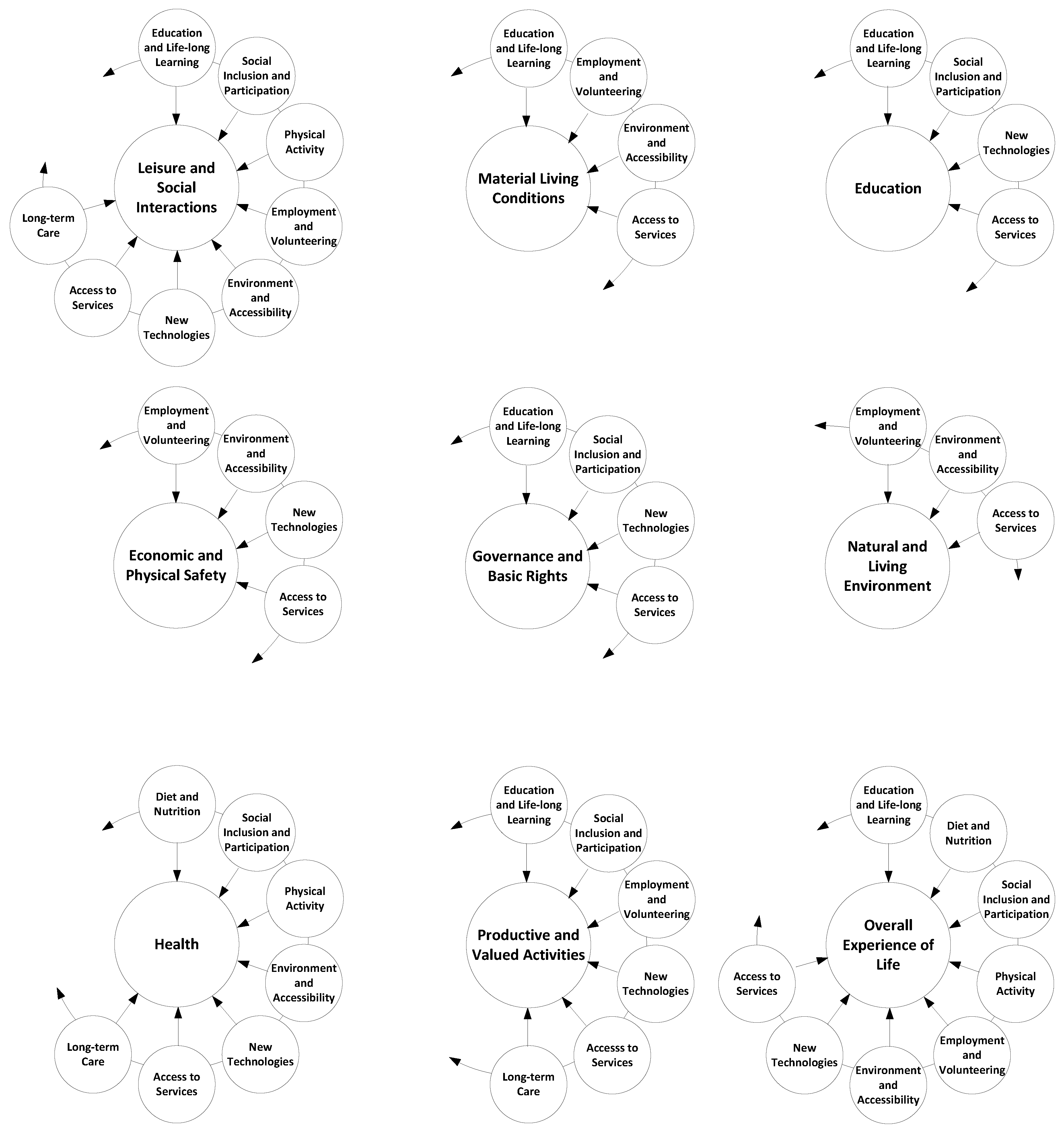
2.3.2. Vertical Component
3. Methodology of the Review
3.1. Data Sources and Search Strategy
3.2. Study Selection Process
3.2.1. Inclusion Criteria
- Articles and patents which included ICT solutions to achieve the QoL for older adults that:
- Addressed ICT solutions in home or supportive care environments for older adults with specific needs regardless of whether the ICT solution was embedded on the human body or in a home, building, city, region, and country;
- Addressed the physical and/or mental needs faced by older adults;
- Involved ICT solutions that have been implemented or deployed in pilot form contributing to the key smart ageing determinants (i.e., long-term care, diet and nutrition, new technologies, physical activity, social inclusion and participation, employment and volunteering, access to services, and education and life-long learning);
- Articles and patents which intend to understand various QoL dimensions (i.e., material living conditions, health, education, productive and valued activities, governance and basic rights, leisure and social interactions, natural and living environment, economic and physical safety, and overall experience of life) in terms of QoL for older adults;
- Articles and patents which are peer-reviewed and published in English within a 20-year period (i.e., 1999–2019).
- Articles that used any kind of research methodology with positive/negative results.
3.2.2. Exclusion Criteria
- Articles and patents written in a language other than English;
- Articles and patents that were unavailable or available with an abstract;
- Articles covering theoretical reviews, narrative reviews, meta-analyses, conference notes, and other types of literature reviews;
- Articles and patents that are about technology which differs from ICT for older people;
- Research published in conference proceedings, books, book chapters, and master’s and doctoral theses;
- Articles and patents that consider ICT solutions contributing to smart concepts other than smart ageing and QoL for older adults;
- Articles and patents on assistive devices such as canes, wheeled walkers, hearing aids, etc.;
- Studies published before 1999;
- Research which focuses on ICT solutions contributing to the concept of smart ageing in developing countries, which are under different conditions to developed countries;
- Research with a focus on industry and production of ICT solutions;
- Research materials on telemonitoring, telemedicine or telehealth programs which include self-monitoring using low-complexity technologies;
- Research materials that reported combined interventions;
- Articles that did not provide enough information for categorising the data source.
3.3. Publications Review and Data Extraction
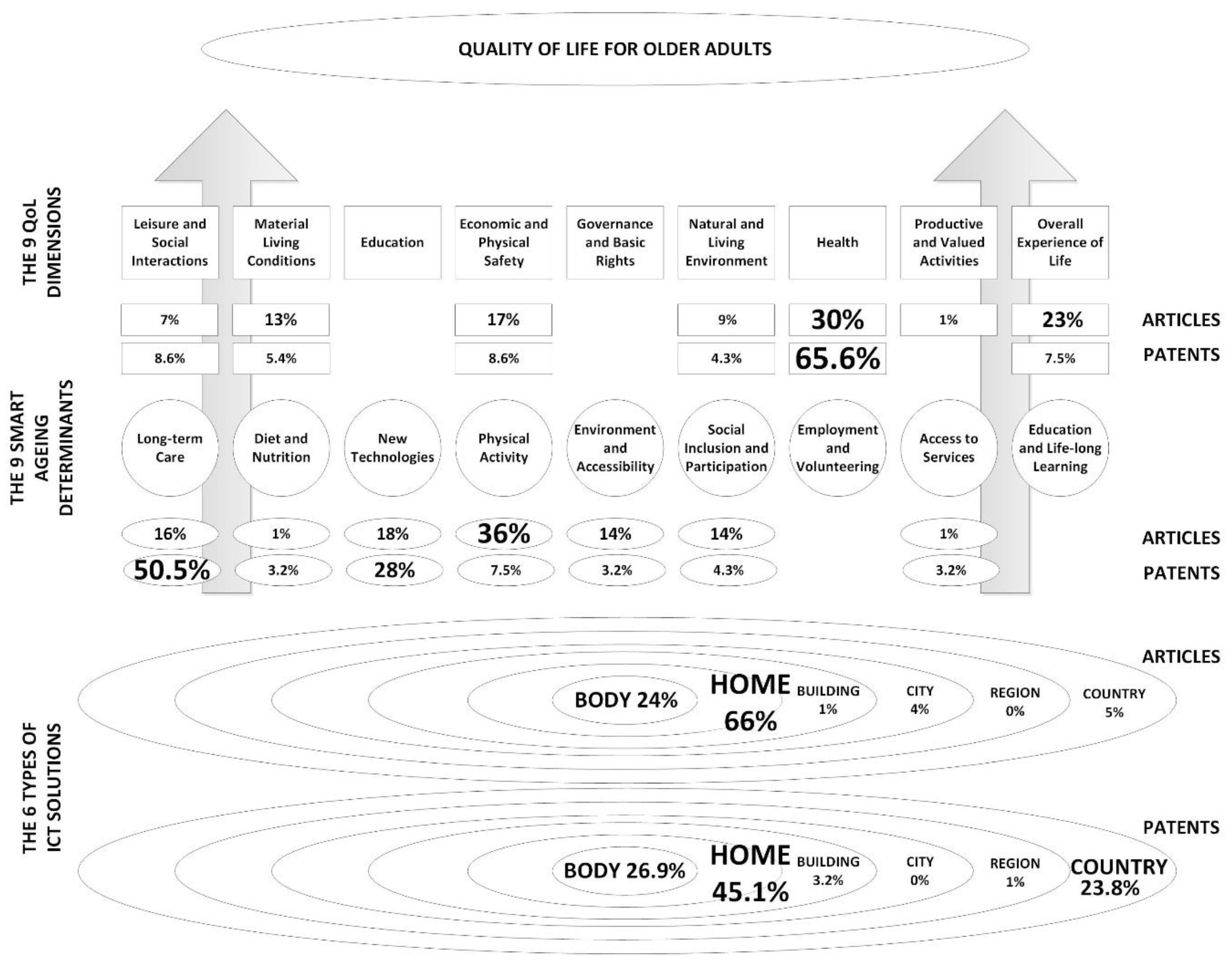
4. Results
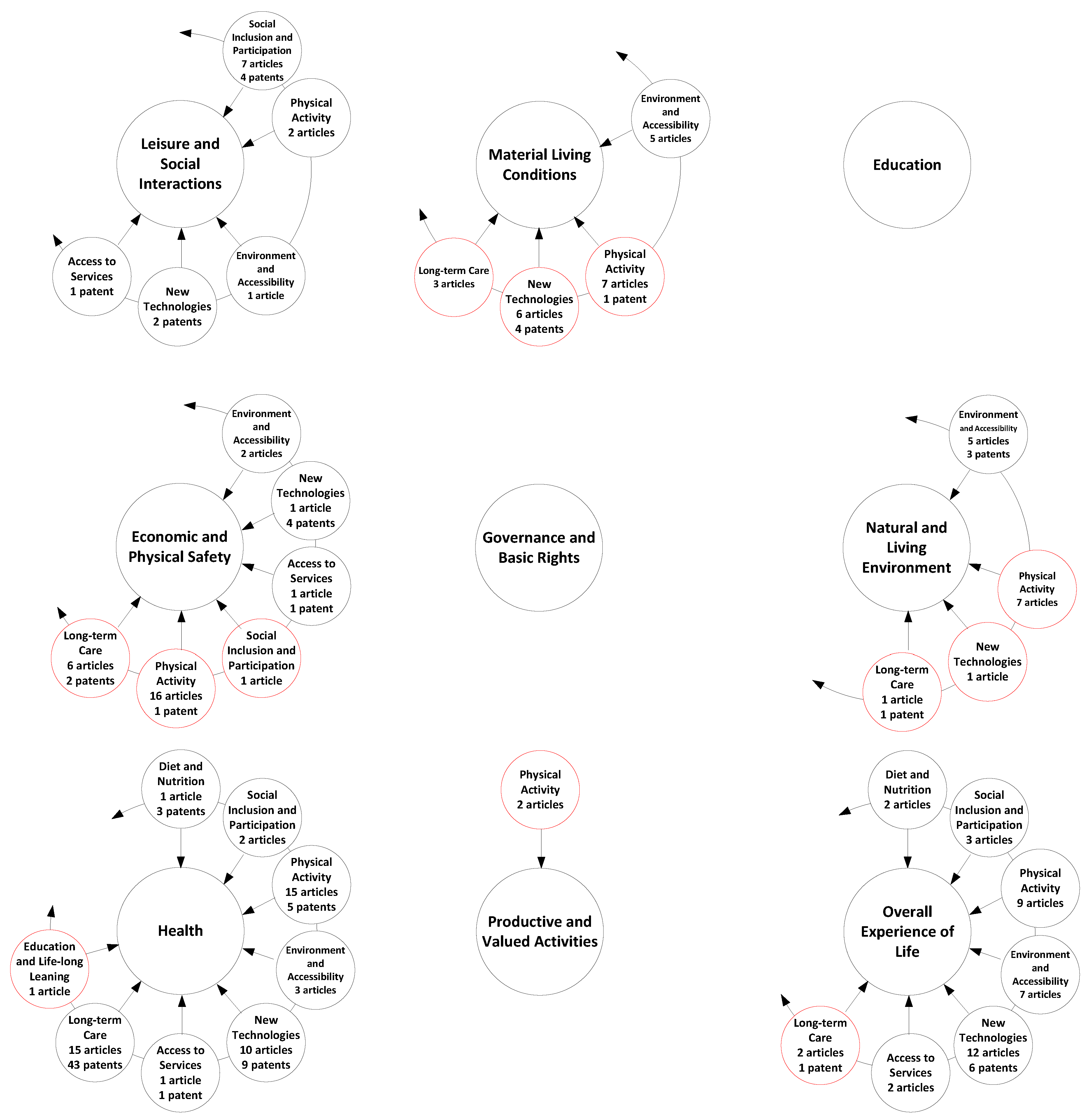
4.1. Literature Analysis
4.2. Patent Analysis
5. Discussion
5.1. Horizontal Component
5.2. Vertical Component
5.3. Study Flaws and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- World Health Organization: 10 Facts on Ageing and Ealth. Available online: http://www.who.int/features/factfiles/ageing/en/ (accessed on 4 April 2020).
- United Nations: World Population Ageing. 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Report.pdf (accessed on 23 April 2020).
- Van Hoof, J.; Demiris, G.; Wouters, E.J. Handbook of Smart Homes, Health Care and Well-Being; Springer Science and Business Media LLC: Berlin, Germany, 2017. [Google Scholar]
- Van Hoof, J.; Kolmer, D.M.B.G.; De Vlugt, E.; De Vries, S.I. Quality of Life: The Interplay between Human Behaviour, Technology and the Environment. Int. J. Environ. Res. Public Health 2019, 16, 5106. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.B. Personalized Aging: One Size Doesn’t Fit All. In The Upside of Ageing: How Long Life is Changing the World of Health, Work, Innovation, Policy and Purpose; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 19–34. [Google Scholar]
- Peek, S.T.M.; Luijkx, K.; Rijnaard, M.D.; Nieboer, M.E.; Van Der Voort, C.S.; Aarts, S.; Van Hoof, J.; Vrijhoef, H.J.M.; Wouters, E. Older Adults’ Reasons for Using Technology while Aging in Place. Gerontology 2015, 62, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Marston, H.R.; van Hoof, J. "Who Doesn’t Think about Technology When Designing Urban Environments for Older People?" A Case Study Approach to a Proposed Extension of the WHO’s Age-friendly Cities Model. Int. J. Environ. Res. Public Health 2019, 16, 3525. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The Challenges of Urban Ageing: Making Cities Age-Friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar] [CrossRef]
- van Hoof, J.; Kazak, J.K. Urban Ageing. Indoor Built Environ. 2018, 27, 538–586. [Google Scholar] [CrossRef]
- Husic, J.B.; Baraković, S.; Dinarević, E.C. Smart Ageing: Are We Succeeding? In Proceedings of the World Congress on Medical Physics and Biomedical Engineering 2006; Springer Science and Business Media LLC: Banja Luka, Bosnia and Herzegovina, 2019; pp. 387–393. [Google Scholar]
- The Whoqol Group Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [CrossRef]
- Gotay, C.C.; Moore, T.D. Assessing quality of life in head and neck cancer. Qual. Life Res. 1992, 1, 5–17. [Google Scholar] [CrossRef]
- Hörnquist, J.O. The Concept of Quality of Life. Scand. J. Soc. Med. 1982, 10, 57–61. [Google Scholar] [CrossRef]
- Theofilou, P. Quality of Life: Definition and Measurement. Eur. J. Psychol. 2013, 9, 150–162. [Google Scholar] [CrossRef]
- Eurostat. Quality of Life (QoL). Available online: https://ec.europa.eu/eurostat/web/gdp-and-beyond/quality-of-life/data (accessed on 4 April 2020).
- EuroHealthNet. Healthy Ageing. Available online: http://www.healthyageing.eu/sites/www.healthyageing.eu/files/featured/Healthy%20and%20Active%20Ageing.pdf (accessed on 4 April 2020).
- Yang, Q.; Shen, Z. Active Aging in the Workplace and the Role of Intelligent Technologies. In Proceedings of the 2015 IEEE/WIC/ACM International Conference on Web Intelligence and Intelligent Agent Technology (WI-IAT), Singapore, 6–9 December 2015; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2015; Volume 2, pp. 391–394. [Google Scholar]
- Department of the Taoiseach. Programme of Actions for Smart Ageing. Available online: https://www.taoiseach.gov.ie/eng/Publications/Publica-tions_2016/Programme_of_Actions_for_Smart_Ageing.pdf (accessed on 4 April 2020).
- A Mapping of Smart Ageing Activity in Ireland and an Assessment of the Potential Smart Ageing Opportunity Areas. Available online: https://www.dcu.ie/sites/default/files/agefriendly/SmartAgingExecutiveSummary.pdf (accessed on 23 April 2020).
- Song, I.-Y.; Song, M.; Timakum, T.; Ryu, S.-R.; Lee, H. The landscape of smart aging: Topics, applications, and agenda. Data Knowl. Eng. 2018, 115, 68–79. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity and Adults. Available online: http://www9.who.int/dietphysicalactivity/factsheet_adults/en/ (accessed on 4 April 2020).
- Ogita, M.; Okura, M.; Yamamoto, M.; Nakai, T.; Numata, T.; Arai, H. P101: Social participation is associated with physical frailty in Japanese older adults. Eur. Geriatr. Med. 2014, 5, S114. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Marx, M.S.; Werner, P. Agitation in Elderly Persons: An Integrative Report of Findings in a Nursing Home. Int. Psychogeriatrics 1992, 4, 221–240. [Google Scholar] [CrossRef] [PubMed]
- Buettner, L.L.; Fitzsimmons, S.; Atav, A.S.; Buettner, L.; Fitzsimmons, S.; Atav, S. Predicting Outcomes of Therapeutic Recreation Interventions for Older Adults with Dementia and Behavioral Symptoms. Ther. Recreat. J. 2006, 40, 12–14. Available online: http://libres.uncg.edu/ir/uncg/f/L_Buettner_Predicting_2006.pdf (accessed on 24 April 2020).
- Granic, A.; Mendonça, N.; Hill, T.R.; Jagger, C.; Stevenson, E.J.; Mathers, J.C.; Sayer, A.A. Nutrition in the Very Old. Nutrition 2018, 10, 269. [Google Scholar] [CrossRef]
- Volkert, D. Nutrition and lifestyle of the elderly in Europe. J. Public Health 2005, 13, 56–61. [Google Scholar] [CrossRef]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Ríos-Rincón, A.M. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Haghi, M.; Thurow, K.; Stoll, R. Wearable Devices in Medical Internet of Things: Scientific Research and Commercially Available Devices. Healthc. Inform. Res. 2017, 23, 4–15. [Google Scholar] [CrossRef]
- Yin, Y.; Zeng, Y.; Chen, X.; Fan, Y. The internet of things in healthcare: An overview. J. Ind. Inf. Integr. 2016, 1, 3–13. [Google Scholar] [CrossRef]
- Van Hoof, J.; De Kort, H.; Markopoulos, P.; Soede, M. Ambient intelligence, ethics and privacy. Gerontechnology 2007, 6, 155–163. [Google Scholar] [CrossRef]
- Van Hoof, J.; Verboor, J.; Weernink, C.O.; Sponselee, A.-M.A.-M.G.; Sturm, J.; Kazak, J.K.; Govers, G.; Van Zaalen, Y. Real-Time Location Systems for Asset Management in Nursing Homes: An Explorative Study of Ethical Aspects. Information 2018, 9, 80. [Google Scholar] [CrossRef]
- Weernink, C.O.; Felix, E.; Verkuijlen, P.; Daele, A.D.-V.; Kazak, J.K.; Van Hoof, J. Real-time location systems in nursing homes: state of the art and future applications. J. Enabling Technol. 2018, 12, 45–56. [Google Scholar] [CrossRef]
- Maresova, P.; Javanmardi, E.; Barakovic, S.; Husic, J.B.; Tomsone, S.; Krejcar, O.; Ramalho, T.C. Consequences of chronic diseases and other limitations associated with old age - a scoping review. BMC Public Health 2019, 19, 1431. [Google Scholar] [CrossRef] [PubMed]
- Maresova, P.; Krejcar, O.; Baraković, S.; Baraković Husić, J.; Lemeski, P.; Zdravevski, E.; Chorbev, I.; Trajkovik, V. Health-Related ICT Solutions of Smart Environments for Elderly – Systematic Review. IEEE Access. 2020, 8, 54574–54600. [Google Scholar] [CrossRef]
- Krejcar, O.; Maresova, P.; Selamat, A.; Melero, F.J.; Frischer, R.; Kuca, K.; Baraković, S.; Baraković Husić, J. Smart Furniture Definition and Specification. IEEE Access 2019, 7, 94822–94839. [Google Scholar] [CrossRef]
- Frischer, R.; Krejcar, O.; Maresova, P.; Fadeyi, O.; Selamat, A.; Kuča, K.; Tomsone, S.; Teixeira, J.P.; Madureira, J.; Melero, F.J. Commercial ICT Smart Solutions for the Elderly: State of the Art and Future Challenges in the Smart Furniture Sector. Electronics 2020, 9, 149. [Google Scholar] [CrossRef]
- Rocha, N.P.; Dias, A.; Santinha, G.; Rodrigues, M.; Queirós, A.; Rodrigues, C. A Systematic Review of Smart Cities’ Applications to Support Active Ageing. Procedia Comput. Sci. 2019, 160, 306–313. [Google Scholar] [CrossRef]
- Na Lee, L.; Kim, M.J. A Critical Review of Smart Residential Environments for Older Adults with a Focus on Pleasurable Experience. Front. Psychol. 2020, 10, 3080. [Google Scholar] [CrossRef]
- Maskeliūnas, R.; Damasevicius, R.; Segal, S. A Review of Internet of Things Technologies for Ambient Assisted Living Environments. Futur. Internet 2019, 11, 259. [Google Scholar] [CrossRef]
- Yang, P.; Lin, S.J. Digital Aging as an Essential Component of Active Aging: A Literature review. Int. J. Lib. Arts Soc. Sci. 2019, 7, 113–132. [Google Scholar]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Vegesna, A.; Tran, M.; Angelaccio, M.; Arcona, S. Remote Patient Monitoring via Non-Invasive Digital Technologies: A Systematic Review. Telemed. e-Health 2016, 23, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Ye, B.; Taati, B.; Mihailidis, A. Detecting agitation and aggression in people with dementia using sensors-A systematic review. Alzheimer’s Dement. 2018, 14, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Van Bronswijk, J.; Bouma, H.; Fozard, J. Technology for quality of life: an enriched taxonomy. Gerontechnology 2002, 2, 169–172. [Google Scholar] [CrossRef]
- Genoe, R.; Kulczycki, C.; Marston, H.R.; Freeman, S.; Musselwhite, C.; Rutherford, H. E-Leisure and Older Adults: Findings from an International Exploratory Study. Ther. Recreat. J. 2018, 52, 1–18. [Google Scholar] [CrossRef]
- Marston, H.R.; Genoe, R.; Freeman, S.; Kulczycki, C.; Musselwhite, C. Older Adults’ Perceptions of ICT: Main Findings from the Technology In Later Life (TILL) Study. Healthcare 2019, 7, 86. [Google Scholar] [CrossRef]
- World Health Organization. Global Age-Friendly Cities: A Guide. Available online: https://www.who.int/ageing/publications/Global_age_friendly_cities_Guide_English.pdf (accessed on 23 April 2020).
- Peek, S.T.M.; Wouters, E.J.; Van Hoof, J.; Luijkx, K.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef]
- Van Hoof, J.; Dikken, J.; Buttiġieġ, S.C.; Hoven, R.F.M.V.D.; Kroon, E.; Marston, H.R. Age-friendly cities in the Netherlands: An explorative study of facilitators and hindrances in the built environment and ageism in design. Indoor Built Environ. 2019, 29, 417–437. [Google Scholar] [CrossRef]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baraković, S.; Baraković Husić, J.; van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. Int. J. Environ. Res. Public Health 2020, 17, 2940. https://doi.org/10.3390/ijerph17082940
Baraković S, Baraković Husić J, van Hoof J, Krejcar O, Maresova P, Akhtar Z, Melero FJ. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. International Journal of Environmental Research and Public Health. 2020; 17(8):2940. https://doi.org/10.3390/ijerph17082940
Chicago/Turabian StyleBaraković, Sabina, Jasmina Baraković Husić, Joost van Hoof, Ondrej Krejcar, Petra Maresova, Zahid Akhtar, and Francisco Jose Melero. 2020. "Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions" International Journal of Environmental Research and Public Health 17, no. 8: 2940. https://doi.org/10.3390/ijerph17082940
APA StyleBaraković, S., Baraković Husić, J., van Hoof, J., Krejcar, O., Maresova, P., Akhtar, Z., & Melero, F. J. (2020). Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. International Journal of Environmental Research and Public Health, 17(8), 2940. https://doi.org/10.3390/ijerph17082940