The TTCYB Study Protocol: A Tailored Print Message Intervention to Improve Cardiovascular Patients’ Lifestyles


 , and
, and
Abstract
1. Introduction
The “Time to Change Your Behavior” (TTCYB) Intervention
- to determine whether tailored materials are perceived as more useful, understandable, and complete compared to non-tailored ones;
- to understand whether the TTCYB intervention is effective in promoting changes in diet, alcohol intake, physical activity, and smoking behavior among patients with CVDs;
- to explore the effects of the TTCYB intervention compared with two control groups (described below) on secondary endpoints, including body mass index and systolic and diastolic blood pressure;
- to evaluate socio-demographic and psychological factors such as self-efficacy, locus of control, and anxiety and depression, which could moderate the effectiveness of the intervention.
2. Materials and Methods
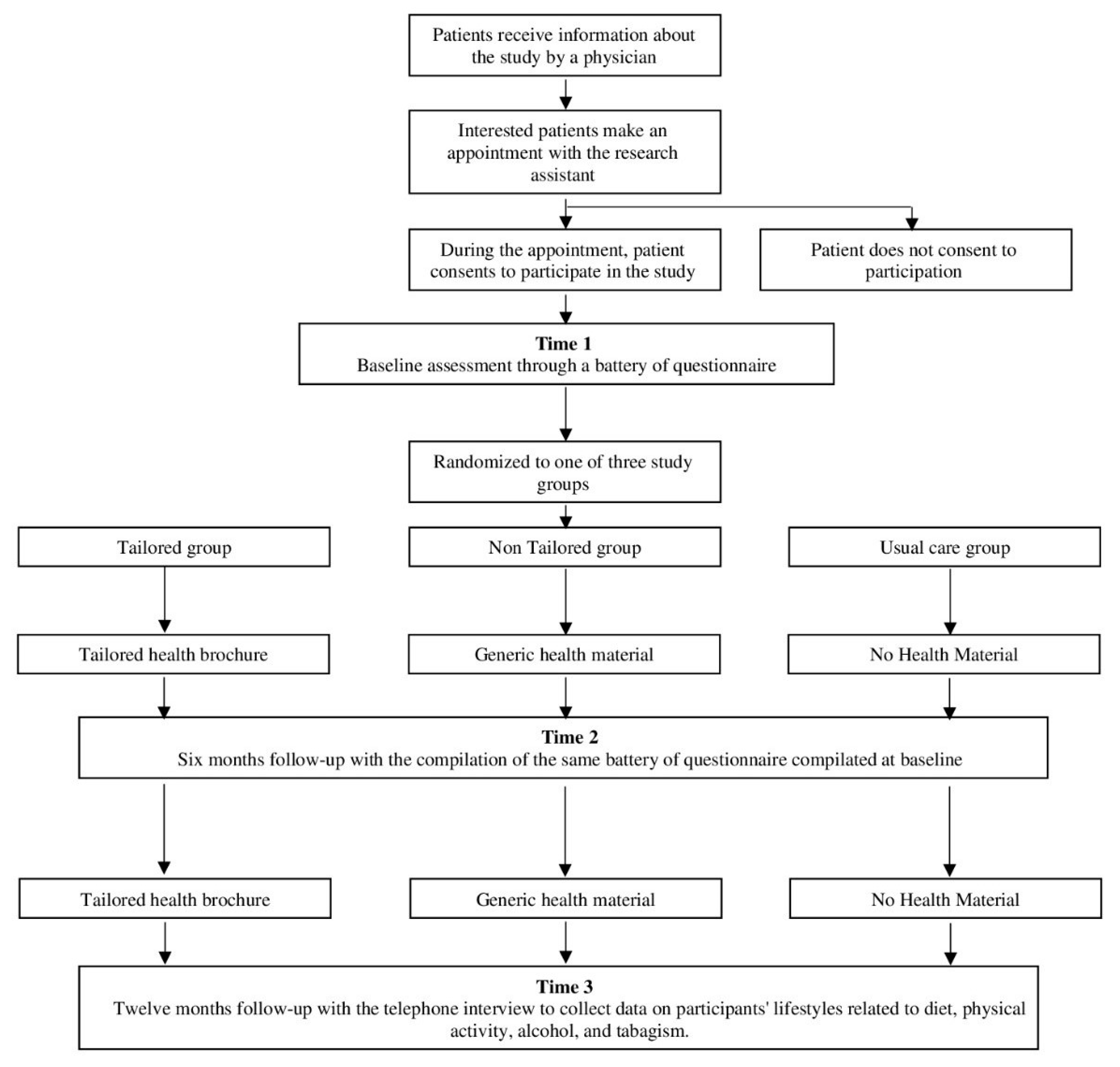
2.1. Design
2.2. Recruitment of Participants
2.3. Eligibility
2.4. Measures
2.4.1. Dietary Behavior
2.4.2. Physical Activity
2.4.3. Alcohol Intake
2.4.4. Smoking Behavior
2.4.5. HAPA Constructs
2.4.6. Illness Perception
2.4.7. Needs for Information
- “Pharmacological Treatment”: typology of drugs, how and when to take them, possible side effects;
- “Knowledge About the Disease”: the anatomical/functional nature connected to the disease (ex. how the blood circulation system functions, what the symptoms connected to the health problem are, and what can be done to manage them);
- “Daily Activities”: information about everyday activities that can be carried out and which ones have to be modified (ex. work, free time, sexual activity);
- “Behavioral Habits”: information on lifestyle, with a focus on smoking, diet, alcohol, and physical activity;
- “Impact of the Disease”: advice on how to manage distress caused by the disease;
- “Risk and Complications”: the risks related to the disease and possible complications (e.g., the possibilities of a heart attack, how to avoid complications, who to call in case of need, etc.).
2.4.8. Medical Adherence
2.5. Intervention
2.5.1. Tailored Group
- Adherence to medical treatment. For example, if a patient answers “yes” to the question “Sometimes if you feel worse when you take the medicine, do you stop taking it?”, he/she will receive a message like “Pay attention, because the treatment for hypertension must not be interrupted without a physician’s approval”.
- Illness perception. For example, if a patient answers “For a very short time” to the question “How long do you think your illness will continue?”, he/she will receive a message like “Please note that acute coronary syndrome is a chronic disease; this means that it is a long-lasting condition that can be controlled but not cured and you’ll need to take pharmacological treatment for life”.
- Descriptive feedback on the behavior. For example, “Based on your answers, we determined that your daily consumption of fruits and vegetables is not healthy”. Descriptive feedback is one of the effective strategies used to tailor communication [46], to stimulate patients’ self-referential thought or otherwise focusing attention on specific behaviors related to the outcome of interest.
- HAPA constructs. In line with HAPA, health messages will be customized to the patients’ intention to change. Specific messages will be developed to address the social-cognitive predictors emerging in the different phases. Patients will be divided into five different stages of changes:
- Patients who do not intend to change their behavior (non-intenders). This group will be divided into two subgroups:
- (1)
- Non-intenders A—patients who do not want to change their behaviors because they have the wrong idea about the relationship between lifestyles and illness (patients who answer “I do not believe it will make my health better” or “No particular reasons” to the question “Do you intend to change your behaviors in the next months?”). For non-intenders A, the tailored messages target patients’ outcome expectancies resulting from the change in behavior, focusing on positive effects and reducing negative outcomes.
- (2)
- Non intenders B—patients who do not want to change due to a lack of or low level of self-efficacy (I know I will never manage to do it). For this group, the tailored messages focus on self-efficacy, to improve patients’ perception that they can change and to reduce the cognitive barriers to change.
- Patients who have not (yet) set a goal to act (preintenders), but who might consider changing their behavior. For this group, the tailoring procedure is the same as non-intenders A.
- Patients who have set a goal to change their behavior but who are not yet acting (intenders). In this case, tailored messages present some real plans to implement the change, focusing on those plans the patients declare themselves unable to foresee. The social-cognitive predictors that will be addressed are action planning, which is the subject’s ability to identify real goals to put the change into action, and coping planning, which pertains to the anticipation of barriers that might arise during the acceptance and adoption of new behavior.
- Patients who already perform the behavior in question (actors). The tailored communication focuses on the possible obstacles that patients believe that they cannot overcome to maintain the new behavior. The social-cognitive predictors that will be addressed are maintenance self-efficacy and recovery self-efficacy. The former is about the subject’s confidence that he/she can maintain a difficult behavior, while recovery self-efficacy is about the subject’s belief he/she can resume a difficult behavior after an interruption.
2.5.2. Non-Tailored Group
2.5.3. Usual Care Group
2.6. Measurement of Outcomes
2.6.1. Change in Lifestyle Habits
2.6.2. Physiological Parameters
2.6.3. Patients’ Judgments about the Material
2.6.4. Potential Moderators of Intervention Efficacy
2.6.5. Locus of Control
2.6.6. Anxiety and Depression
2.6.7. General Self Efficacy
2.7. Sample Size Estimation
2.8. Data Collection Methods and Data Management
2.9. Planned Statistical Analysis
2.10. Ethics
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Trial Registration
References
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, A.C.; Wändell, P.E.; Gigante, B.; Leander, K.; Hellenius, M.; de Faire, U. Seven modifiable lifestyle factors predict reduced risk for ischemic cardiovascular disease and all-cause mortality regardless of body mass index: A cohort study. Int. J. Cardiol. 2013, 168, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, E.; Iso, H.; Tanabe, N.; Wada, Y.; Yatsuya, H.; Kikuchi, S.; Inaba, Y.; Tamakoshi, A. Healthy lifestyle behaviours and cardiovascular mortality among japanese men and women: The japan collaborative cohort study. Eur. Heart J. 2012, 33, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Yatsuya, H.; Nettleton, J.A.; Lutsey, P.L.; Cushman, M.; Rosamond, W.D.; ARIC Study Investigators. Community prevalence of ideal cardiovascular health, by the american heart association definition, and relationship with cardiovascular disease incidence. J. Am. Coll. Cardiol. 2011, 57, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Greenlund, K.J.; Hong, Y. Ideal cardiovascular health and mortality from all causes and diseases of the circulatory system among adults in the United States. Circulation 2012, 125, 987–995. [Google Scholar] [CrossRef]
- Odegaard, A.O.; Koh, W.P.; Gross, M.D.; Yuan, J.M.; Pereira, M.A. Combined lifestyle factors and cardiovascular disease mortality in chinese men and women: The singapore chinese health study. Circulation 2011, 124, 2847–2854. [Google Scholar] [CrossRef]
- Fodor, G.J.; McInnis, N.H.; Helis, E.; Turton, P.; Leenen, F.H. Lifestyle changes and blood pressure control: A Community-Based Cross-Sectional survey (2006 Ontario survey on the prevalence and control of hypertension). J. Clin. Hypertens. 2009, 11, 31–35. [Google Scholar] [CrossRef]
- Gee, M.E.; Bienek, A.; Campbell, N.R.; Bancej, C.M.; Robitaille, C.; Kaczorowski, J.; Joffres, M.; Dai, S.; Gwadry-Sridar, F.; Nolan, R.P. Prevalence of, and barriers to, preventive lifestyle behaviors in hypertension (from a national survey of canadians with hypertension). Am. J. Cardiol. 2012, 109, 570–575. [Google Scholar] [CrossRef]
- Naderi, S.H.; Bestwick, J.P.; Wald, D.S. Adherence to drugs that prevent cardiovascular disease: Meta-analysis on 376,162 patients. Am. J. Med. 2012, 125, 882–887. [Google Scholar] [CrossRef]
- Leung, A.A.; Nerenberg, K.; Daskalopoulou, S.S.; McBrien, K.; Zarnke, K.B.; Dasgupta, K.; Cloutier, L.; Gelfer, M.; Lamarre-Cliche, M.; Milot, A.; et al. Hypertension Canada’s 2016 Canadian hypertension education program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can. J. Cardiol. 2016, 32, 569–588. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Farrell, D.W.; Olevitch, L.R.; Brennan, L.K. Tailoring Health Messages: Customizing Communication with Computer Technology Tailoring Health Messages: Customizing Communication with Computer Technology; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Revere, D.; Dunbar, P.J. Review of computer-generated outpatient health behavior interventions: Clinical encounters “in absentia”. J. Am. Med. Inform. Assoc. 2001, 8, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Noar, S.M.; Harrington, N.G. Tailored Communications for Health-Related Decision-Making and Behavior Change. In Handbook of Health Decision Science; Diefenbach, M., Miller-Halegoua, S., Bowen, D., Eds.; Springer: New York, NY, USA, 2016; pp. 251–263. [Google Scholar]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-Analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.; Dockray, S.; Linehan, C. A systematic review of tailored eHealth interventions for weight loss. Digit. Health 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.; Lauver, D.R. The efficacy of tailored interventions. J. Nurs. Scholarsh. 2002, 34, 331–337. [Google Scholar] [CrossRef]
- Sahin, C.; Courtney, K.L.; Naylor, P.J.; Rhodes, R.E. Tailored mobile text messaging interventions targeting type 2 diabetes self-management: A systematic review and a meta-analysis. Digit. Health 2019, 5. [Google Scholar] [CrossRef]
- Skinner, C.S.; Campbell, M.K.; Rimer, B.K.; Curry, S.; Prochaska, J.O. How effective is tailored print communication? Ann. Behav. Med. 1999, 21, 290. [Google Scholar] [CrossRef]
- Sohl, S.J.; Moyer, A. Tailored interventions to promote mammography screening: A meta-analytic review. Prev. Med. 2007, 45, 252–261. [Google Scholar] [CrossRef]
- Gatwood, J.; Balkrishnan, R.; Erickson, S.R.; An, L.C.; Piette, J.D.; Farris, K.B. The impact of tailored text messages on health beliefs and medication adherence in adults with diabetes: A randomized pilot study. Res. Soc. Adm. Pharm. 2016, 12, 130–140. [Google Scholar] [CrossRef]
- Rowley, T.W.; Lenz, E.K.; Swartz, A.M.; Miller, N.E.; Maeda, H.; Strath, S.J. Efficacy of an individually tailored, internet-mediated physical activity intervention in older adults: A randomized controlled trial. J. Appl. Gerontol. 2019, 38, 1011–1022. [Google Scholar] [CrossRef]
- Kroeze, W.; Werkman, A.; Brug, J. A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Ann. Behav. Med. 2006, 31, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Neville, L.M.; O’Hara, B.; Milat, A.J. Computer-tailored dietary behaviour change interventions: A systematic review. Health Educ. Res. 2009, 24, 699–720. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.P.; Pelletier, L.; Guertin, C. Starting off on the Best Foot: A Review of Message Framing and Message Tailoring, and Recommendations for the Comprehensive Messaging Strategy for Sustained Behavior Change. Health Commun. 2018, 33, 1068–1077. [Google Scholar] [CrossRef]
- Reuter, C.; Kaufhold, M.A.; Schmid, S.; Spielhofer, T.; Hahne, A.S. The impact of risk cultures: Citizens’ perception of social media use in emergencies across Europe. Technol. Forecast. Soc. Chang. 2019, 148, 119724. [Google Scholar] [CrossRef]
- Greco, A.; Cappelletti, E.R.; Monzani, D.; Pancani, L.; D’Addario, M.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrigaro, M.; Vecchio, L.; et al. A longitudinal study on the information needs and preferences of patients after an acute coronary syndrome. BMC Fam. Pract. 2016, 17, 136. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a mediterranean diet and survival in a greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.M.B. The Rapid Assessment of Physical Activity (RAPA) among older adults. Prev. Chronic. Dis. 2006, 3, 118. [Google Scholar]
- Keogh, J.W.; Shepherd, D.; Krägeloh, C.U.; Ryan, C.; Masters, J.; Shepherd, G.; MacLeod, R. Predictors of physical activity and quality of life in new zealand prostate cancer survivors undergoing androgen-deprivation therapy. N. Z. Med. J. 2010, 123, 20–29. [Google Scholar]
- Sander, A.P.; Wilson, J.; Izzo, N.; Mountford, S.A.; Hayes, K.W. Factors that affect decisions about physical activity and exercise in survivors of breast cancer: A qualitative study. Phys. Ther. 2012, 92, 525–536. [Google Scholar] [CrossRef]
- von Känel, R.; Mausbach, B.T.; Ancoli-Israel, S.; Dimsdale, J.E.; Mills, P.J.; Patterson, T.L.; Ziegler, M.G.; Roepke, S.K.; Chattillion, E.A.; Allison, M.I.; et al. Sleep in spousal alzheimer caregivers: A longitudinal study with a focus on the effects of major patient transitions on sleep. Sleep 2012, 35, 247–255. [Google Scholar] [CrossRef]
- Glovannucci, E.; Colditz, G.; Stampfer, M.J.; Rimm, E.B.; Litin, L.; Sampson, L.; Willett, W.C. The assessment of alcohol consumption by a simple self-administered questionnaire. Am. J. Epidemiol. 1991, 133, 810–817. [Google Scholar] [CrossRef]
- Steca, P.; D’Addario, M.; Magrin, M.E.; Miglioretti, M.; Monzani, D.; Pancani, L.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Fattirolli, F.; et al. A type A and type D combined personality typology in essential hypertension and acute coronary syndrome patients: Associations with demographic, psychological, clinical, and lifestyle indicators. PLoS ONE 2016, 11, 0161840. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K. The fagerström test for nicotine dependence: A revision of the fagerstrom tolerance questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Renner, B.; Schwarzer, R. Risk and Health Behaviors. Documentation of the Scales of the Research Project: “Risk Appraisal Consequences in Korea”, 2nd ed.; International University Bremen & Freie Universität Berlin: Berlin, Germany, 2005; pp. 1–55. [Google Scholar]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The brief illness perception questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- Cappelletti, E.R.; Greco, A.; Maloberti, A.; Giannattasio, C.; Steca, P.; D’Addario, M. What hypertensive patients want to know [and from whom] about their disease: A two-year longitudinal study. BMC Public Health 2020, 1, 1–10. [Google Scholar] [CrossRef]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; Islam, T.; Webber, L.S.; Re, R.N.; Morisky, D.E.; Muntner, P. New medication adherence scale versus pharmacy fill rates in seniors with hypertension. Am. J. Manag. Care 2009, 15, 59–66. [Google Scholar]
- Schwarzer, R.; Schüz, B.; Ziegelmann, J.P.; Lippke, S.; Luszczynska, A.; Scholz, U. Adoption and maintenance of four health behaviors: Theory-guided longitudinal studies on dental flossing, seat belt use, dietary behavior, and physical activity. Ann. Behav. Med. 2007, 33, 156–166. [Google Scholar] [CrossRef]
- Schwarzer, R.; Renner, B. Social-cognitive predictors of health behavior: Action self-efficacy and coping self-efficacy. Health Psychol. 2000, 19, 487. [Google Scholar] [CrossRef]
- Murgraff, V.; McDermott, M.R.; Walsh, J. Self-Efficacy and behavioral enactment: The application of schwarzer’s health action process approach to the prediction of Low-Risk, Single-Occasion drinking. J. Appl. Soc. Psychol. 2003, 33, 339–361. [Google Scholar] [CrossRef]
- Schwarzer, R.; Luszczynska, A.; Ziegelmann, J.P.; Scholz, U.; Lippke, S. Social-Cognitive Predictors of Physical Exercise Adherence: Three Longitudinal Studies in Rehabilitation. Health Psychol. 2008, 27, S54-63. [Google Scholar] [CrossRef]
- Hawkins, R.P.; Kreuter, M.; Resnicow, K.; Fishbein, M.; Dijkstra, A. Understanding tailoring in communicating about health. Health Educ. Res. 2008, 23, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Saywell, R.M., Jr.; Champion, V.L.; Sugg Skinner, C.; Menon, U.; Daggy, J. A cost-effectiveness comparison of three tailored interventions to increase mammography screening. J. Womens Health 2004, 13, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Wallston, K.A. The validity of the multidimensional health locus of control scales. J. Health Psychol. 2005, 10, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Wallston, K.A.; Stein, M.J.; Smith, C.A. Form C of the MHLC scales: A condition-specific measure of locus of control. J. Pers. Assess. 1994, 63, 534–553. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta. Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. The general self-efficacy scale (GSE). Anxiety Stress Coping 2010, 12, 329–345. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A. G* Power Version 3.1.7 [Computer Software]; Universität Kiel: Kiel, Germany, 2013. [Google Scholar]


{kind=link}
| Baseline | Time 2—Six Months after Baseline | Time 3—12 Months after Baseline | |
|---|---|---|---|
| Lifestyle behaviors | x | x | x |
| HAPA constructs | x | x | |
| Illness perception | x | x | |
| Needs for Information | x | x | |
| Medical adherence | x | x | |
| Locus of control | x | x | |
| Anxiety and depression | x | x | |
| General Self Efficacy | x | x | |
| Clinical evaluation | x | x |
| Patients’ Intention to Change Stage | Social-Cognitive Predictor | Example of a Tailored Message |
|---|---|---|
| Non intender a | Outcome Expectancy | “You reported that in changing your diet you are afraid about the difficulty to buy the right products. Don’t be afraid of this, because, especially in recent years, there is growing attention towards a healthy diet. The greater transparency that has been reached in the communication properties of the food will certainly help you to choose the best groceries. You have to always remember to BRING ON YOUR TABLE ONLY FOOD THAT ALLOWS YOU TO FEEL GOOD”. |
| Non intender b | Self-Efficacy | “When you answered the questionnaire, you declared that don’t want to change your diet because you thought you would not be able to do so. Trying to change your nutrition is not so difficult as it sounds. Try to make one change at a time; it is not necessary to change everything at once. Start, for example, by some very simple things, maybe planning the day in which to start your diet and mark it on the calendar. You can also start by searching for a nutrition specialist, who could give you important advice”. |
| Preintender | Outcome Expectancy | |
| Intender | Action Planning | Planning how to start changing your diet is the first step to actualize the intention to change. From the answers at the questionnaire, it emerged that you have no plan on how to manage the situation in which is difficult to maintain the change (e.g., the lunch at work). Try to organize your lunch by preparing it at home in order to avoid buying unhealthy stuff. |
| Actor | Maintenance and Recovery Self-Efficacy | Do not worry if your partner and/or your family would not change their eating habits with you. It is not necessary that everyone in the family changes habits. Probably when they will see the positive outcomes that you will achieve with your diet, they will ask you for advice and suggestion to eat like you! |
| Questions on a Five-Point Likert Scale (1 = not at All; 2 = Few; 3 = on Average; 4 = Sufficiently; 5 = Very | Dichotomous Question (Yes/No) |
|---|---|
| The material was attractive? | Have you read the material? |
| The material was easy to understand? | Have you stored the material? |
| The material encouraged your reflection? | Have you shown the material to others? |
| The material increased your knowledge about hypertension? | Would you read the material again in the future? |
| The material was personalized on your specific situation? | Was the information in the material new? |
| The material contained information pertinent to your specific situation? | Do you think it would be useful to receive this kind of material again in the future? |
| The material was complete? | |
| Would you make behavioral changes based on the material (specific for diet, physical activity, alcohol intake, and smoking behavior)? |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Addario, M.; Cappelletti, E.R.; Sarini, M.; Greco, A.; Steca, P. The TTCYB Study Protocol: A Tailored Print Message Intervention to Improve Cardiovascular Patients’ Lifestyles. Int. J. Environ. Res. Public Health 2020, 17, 2919. https://doi.org/10.3390/ijerph17082919
D’Addario M, Cappelletti ER, Sarini M, Greco A, Steca P. The TTCYB Study Protocol: A Tailored Print Message Intervention to Improve Cardiovascular Patients’ Lifestyles. International Journal of Environmental Research and Public Health. 2020; 17(8):2919. https://doi.org/10.3390/ijerph17082919
Chicago/Turabian StyleD’Addario, Marco, Erika Rosa Cappelletti, Marcello Sarini, Andrea Greco, and Patrizia Steca. 2020. "The TTCYB Study Protocol: A Tailored Print Message Intervention to Improve Cardiovascular Patients’ Lifestyles" International Journal of Environmental Research and Public Health 17, no. 8: 2919. https://doi.org/10.3390/ijerph17082919
APA StyleD’Addario, M., Cappelletti, E. R., Sarini, M., Greco, A., & Steca, P. (2020). The TTCYB Study Protocol: A Tailored Print Message Intervention to Improve Cardiovascular Patients’ Lifestyles. International Journal of Environmental Research and Public Health, 17(8), 2919. https://doi.org/10.3390/ijerph17082919