Identifying the Roles of Healthcare Leaders in HIT Implementation: A Scoping Review of the Quantitative and Qualitative Evidence



Abstract
1. Introduction
2. The Review
2.1. Design
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
3. Results
3.1. Study Characteristics
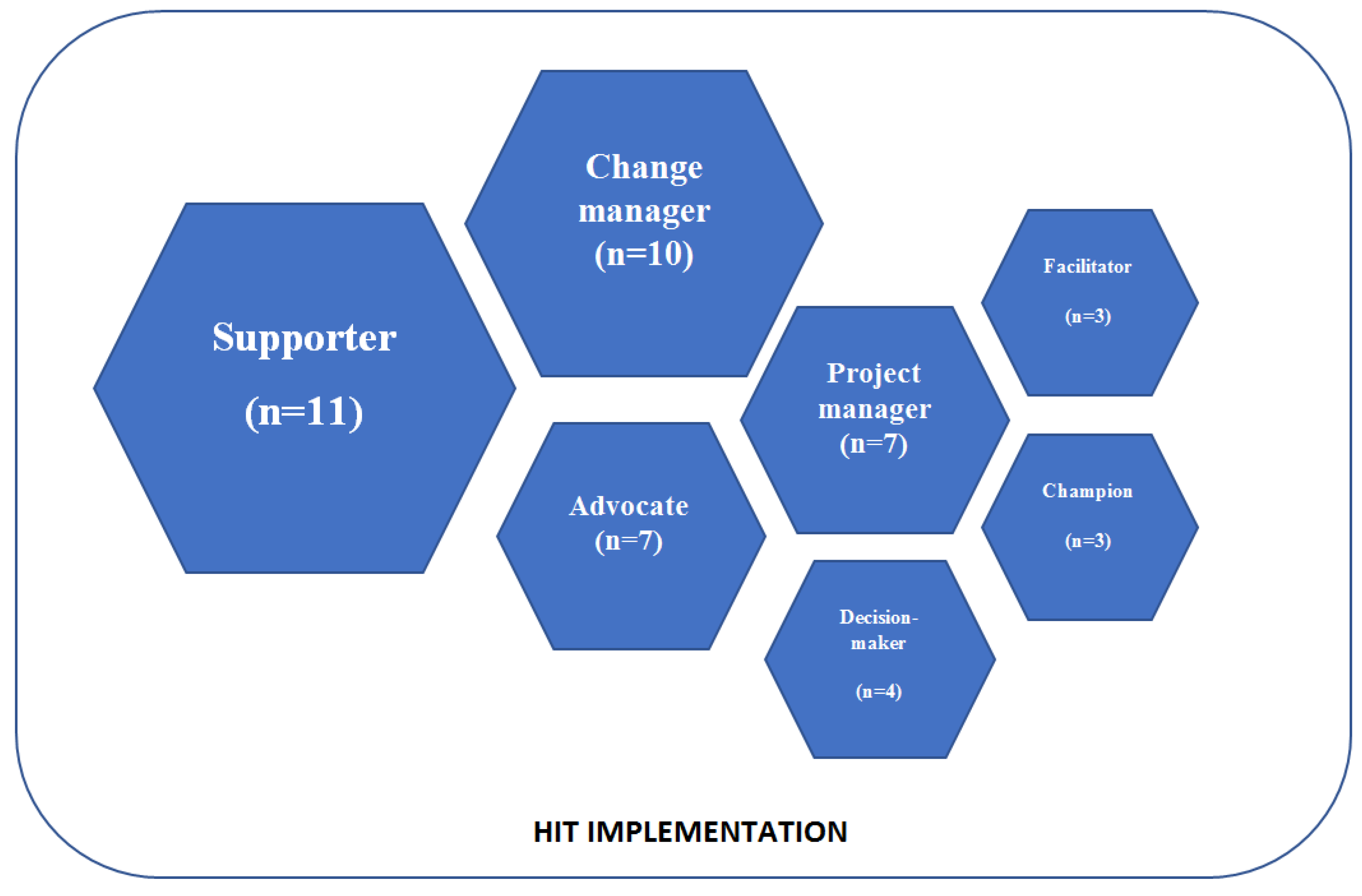
3.2. Healthcare Leaders’ Roles in HIT Implementation
3.2.1. Role of Supporter
3.2.2. Role of Change Manager
3.2.3. Role of Advocate
3.2.4. Role of Project Manager
3.2.5. Role of Decision-Maker
3.2.6. Role of Facilitator
3.2.7. Role of Champion
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HIT | health information technology |
| EMR | electronic medical record |
| HER | electronic health record |
| IT | information technology |
| CIO | chief information officer |
| CPOE | computerised physician order entry |
| DHI | doctorate in health informatics |
References
- Brailer, D.J. Perspective: Presidential Leadership and Health Information Technology. Health Aff. 2009, 28, 392–399. [Google Scholar] [CrossRef] [PubMed]
- European Commission. The Digital Transdormation of Healthcare; European Commission: Brussels, Belgium, 2018; pp. 1–2. [Google Scholar]
- Lluch, M. Healthcare Professionals’ Organisational Barriers to Health Information Technologies-A Literature Review. Int. J. Med. Inform. 2011, 80, 849–862. [Google Scholar] [CrossRef]
- Chen, J.; Ou, L.; Hollis, S.J. A Systematic Review of the Impact of Routine Collection of Patient Reported Outcome Measures on Patients, Providers and Health Organisations in an Oncologic Setting. BMC Health Serv. Res. 2013, 13, 211. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, K.; Sheikh, A. Organizational Issues in the Implementation and Adoption of Health Information Technology Innovations: An Interpretative Review. Int. J. Med. Inform. 2013, 82, e73–e86. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.A.; Foster, J.; de Fatima Marin, H.; Dykes, P.C. Complexity and the Science of Implementation in Health IT-Knowledge Gaps and Future Visions. Int. J. Med. Inform. 2014, 83, e12–e22. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.; Boehme, P.; Mondritzki, T.; Ehlers, J.P.; Kavadias, S.; Truebel, H. Digital Transformation and Disruption of the Health Care Sector: Internet-Based Observational Study. J. Med. Internet Res. 2018, 20, 1–2. [Google Scholar] [CrossRef]
- Glaser, J. More on Management’s Role in IT Project Failures. Healthc. Financ. Manag. 2005, 59, 82–85. [Google Scholar]
- Heeks, R. Health Information Systems: Failure, Success and Improvisation. Int. J. Med. Inform. 2006, 75, 125–137. [Google Scholar] [CrossRef]
- Walsh, M.N.; Rumsfeld, J.S. Leading the Digital Transformation of Healthcare: The ACC Innovation Strategy. J. Am. Coll. Cardiol. 2017, 70, 2719–2722. [Google Scholar] [CrossRef]
- Krause, J.; Van Lieshout, J.; Klomp, R.; Huntink, E.; Aakhus, E.; Flottorp, S.; Jaeger, C.; Steinhaeuser, J.; Godycki-Cwirko, M.; Kowalczyk, A.; et al. Identifying Determinants of Care for Tailoring Implementation in Chronic Diseases: An Evaluation of Different Methods. Implement. Sci. 2014, 9, 102. [Google Scholar] [CrossRef]
- Mair, F.S.; May, C.; O’Donnell, C.; Finch, T.; Sullivan, F.; Murray, E. Factors That Promote or Inhibit the Implementation of E-Health Systems: An Explanatory Systematic Review. Bull. World Health Organ. 2012, 90, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Kajermo, K.N.; UndéN, M.; Gardulf, A.; Eriksson, L.E.; Orton, M.L.; Arnetz, B.B.; Nordström, G. Predictors of Nurses’ Perceptions of Barriers to Research Utilization. J. Nurs. Manag. 2008, 16, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Aarons, G.A.; Ehrhart, M.G.; Farahnak, L.R.; Sklar, M. Aligning Leadership Across Systems and Organizations to Develop a Strategic Climate for Evidence-Based Practice Implementation. Annu. Rev. Public Health 2014, 35, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Ingebrigtsen, T.; Georgiou, A.; Clay-Williams, R.; Magrabi, F.; Hordern, A.; Prgomet, M.; Li, J.; Westbrook, J.; Braithwaite, J. The Impact of Clinical Leadership on Health Information Technology Adoption: Systematic Review. Int. J. Med. Inform. 2014, 83, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Hinţea, C.; Mora, C.; Ţiclǎu, T. Leadership and Management in the Health Care System: Leadership Perception in Cluj County Children’s Hospital. Transylv. Rev. Adm. Sci. 2009, 5, 89–104. [Google Scholar]
- Ludwick, D.A.; Doucette, J. Adopting Electronic Medical Records in Primary Care: Lessons Learned from Health Information Systems Implementation Experience in Seven Countries. Int. J. Med. Inform. 2009, 78, 22–31. [Google Scholar] [CrossRef]
- Desveaux, L.; Soobiah, C.; Bhatia, R.S.; Shaw, J. Identifying and Overcoming Policy-Level Barriers to the Implementation of Digital Health Innovation: Qualitative Study. J. Med. Internet Res. 2019, 21, e14994. [Google Scholar] [CrossRef]
- Kleinman, C.S. Leadership Roles, Competencies, and Education. J. Nurs. Adm. 2003, 33, 451–455. [Google Scholar] [CrossRef]
- Collins, S.; Yen, P.-Y.; Phillips, A.; Kennedy, M.K. Nursing Informatics Competency Assessment for the Nurse Leader. JONA J. Nurs. Adm. 2017, 47, 212–218. [Google Scholar] [CrossRef]
- Sood, H.; NcNeil, K.; Keogh, B. Chief Clinical Information Officers: Clinical Leadership for a Digital Age: These New Roles Need Autonomy, Authority, and a Fully Accredited Career Path. BMJ 2017, 358, j3295. [Google Scholar] [CrossRef]
- Sandström, B.; Borglin, G.; Nilsson, R.; Willman, A. Promoting the Implementation of Evidence-Based Practice: A Literature Review Focusing on the Role of Nursing Leadership. Worldviews Evid.-Based Nurs. 2011, 8, 212–223. [Google Scholar] [CrossRef]
- Birken, S.A.; Lee, S.Y.D.; Weiner, B.J. Uncovering Middle Managers’ Role in Healthcare Innovation Implementation. Implement. Sci. 2012, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Kimberly, J.; Cook, J.M. Organizational Measurement and the Implementation of Innovations in Mental Health Services. Adm. Policy Ment. Health Ment. Health Serv. Res. 2008, 35, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Birken, S.A.; Lee, S.D.; Weiner, B.J. From Strategy to Action: How Top Managers’ Support Increases Middle Managers’ Commitment to Innovation Implementation in Healthcare Organizations. Health Care Manag. Rev. 2015, 40, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Shortliffe, E.H.; Perreault, L.E. Medical Informatics: Computer Applications in Health Care and Biomedicine; Springer: New York, NY, USA, 2001. [Google Scholar]
- Yusif, S.; Hafeez-Baig, A.; Soar, J. E-Health Readiness Assessment Factors and Measuring Tools: A Systematic Review. Int. J. Med. Inform. 2017, 107, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The Use of Electronic Health Records to Support Population Health: A Systematic Review of the Literature. J. Med. Syst. 2018, 42, 214. [Google Scholar] [CrossRef] [PubMed]
- Öberg, U.; Orre, C.J.; Isaksson, U.; Schimmer, R.; Larsson, H.; Hörnsten, Å. Swedish Primary Healthcare Nurses’ Perceptions of Using Digital EHealth Services in Support of Patient Self-Management. Scand. J. Caring Sci. 2018, 32, 961–970. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for Conducting Systematic Scoping Reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Denzin, N.; Lincoln, Y. Handbook of Qualitative Research; SAGE: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Boddy, D.; King, G.; Clark, J.S.; Heaney, D.; Mair, F. The Influence of Context and Process When Implementing E-Health. BMC Med. Inform. Decis. Mak. 2009, 9, 9. [Google Scholar] [CrossRef]
- Deokar, A.V.; Sarnikar, S. Understanding Process Change Management in Electronic Health Record Implementations. Inf. Sys. E-Bus. Manag. 2016, 14, 733–766. [Google Scholar] [CrossRef]
- Dugstad, J.; Eide, T.; Nilsen, E.R.; Eide, H. Towards Successful Digital Transformation through Co-Creation: A Longitudinal Study of a Four-Year Implementation of Digital Monitoring Technology in Residential Care for Persons with Dementia. BMC Health Serv. Res. 2019, 19, 366. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Wilson, C.B.; Stanmore, E.; Todd, C. Implementing Monitoring Technologies in Care Homes for People with Dementia: A Qualitative Exploration Using Normalization Process Theory. Int. J. Nurs. Stud. 2017, 72, 60–70. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Odonnell, C.; Boddy, D.; Smith, F.; Heaney, D.; Mair, F.S. Boundaries and E-Health Implementation in Health and Social Care. BMC Med. Inform. Decis. Mak. 2012, 12, 100. [Google Scholar] [CrossRef] [PubMed]
- Kujala, S.; Hörhammer, I.; Ervast, M.; Kolanen, H.; Rauhala, M. Johtamisen Hyvät Käytännöt Sähköisten Omahoitopalveluiden Käyttöönotossa. Finn. J. eHealth eWelfare 2018, 10, 221–235. [Google Scholar] [CrossRef]
- Kujala, S.; Heponiemi, T.; Hilama, P. Clinical Leaders’ Self-Perceived EHealth Competencies in the Implementation of New EHealth Services. Stud. Health Technol. Inform. 2019, 264, 1253–1257. [Google Scholar] [CrossRef]
- Kujala, S.; Hörhammer, I.; Heponiemi, T.; Josefsson, K. The Role of Frontline Leaders in Building Health Professional Support for a New Patient Portal: Survey Study. J. Med. Internet Res. 2019, 21, e11413. [Google Scholar] [CrossRef]
- Mason, P.; Mayer, R.; Chien, W.W.; Monestime, J.P. Overcoming Barriers to Implementing Electronic Health Records in Rural Primary Care Clinics. Qual. Rep. 2017, 22, 2943–2955. [Google Scholar]
- McAlearney, A.S.; Hefner, J.L.; Sieck, C.; Rizer, M.; Huerta, T.R. Evidence-Based Management of Ambulatory Electronic Health Record System Implementation: An Assessment of Conceptual Support and Qualitative Evidence. Int. J. Med. Inform. 2014, 83, 484–494. [Google Scholar] [CrossRef]
- Nilsen, E.R.; Dugstad, J.; Eide, H.; Gullslett, M.K.; Eide, T. Exploring Resistance to Implementation of Welfare Technology in Municipal Healthcare Services—A Longitudinal Case Study. BMC Health Serv. Res. 2016, 16, 657. [Google Scholar] [CrossRef]
- Øvretveit, J.; Scott, T.; Rundall, T.G.; Shortell, S.M.; Brommels, M. Improving Quality through Effective Implementation of Information Technology in Healthcare. Int. J. Qual. Health Care 2007, 19, 259–266. [Google Scholar] [CrossRef]
- Poon, E.G.; Blumenthal, D.; Jaggi, T.; Honour, M.M.; Bates, D.W.; Kaushal, R. Overcoming Barriers to Adopting and Implementing Computerized Physician Order Entry Systems in U.S. Hospitals. Health Aff. 2004, 23, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, L.; Ball, S.; Haverhals, L.M.; Aron, D.C.; Lowery, J. Evaluation of a National Telemedicine Initiative in the Veterans Health Administration: Factors Associated with Successful Implementation. J. Telemed. Telecare 2018, 24, 168–178. [Google Scholar] [CrossRef]
- Szydlowski, S.; Smith, C. Perspectives From Nurse Leaders And Chief Information Officers Implementation. Hosp. Top. 2008, 87, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Varsi, C.; Ekstedt, M.; Gammon, D.; Børøsund, E.; Ruland, C.M. Middle Managers’ Experiences and Role in Implementing an Interactive Tailored Patient Assessment EHealth Intervention in Clinical Practice. CIN Comput. Inform. Nurs. 2015, 33, 249–257. [Google Scholar] [CrossRef]
- Nilsson, L.; Eriksén, S.; Borg, C. The Influence of Social Challenges When Implementing Information Systems in a Swedish Health-Care Organisation. J. Nurs. Manag. 2016, 24, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Hsia, T.L.; Chiang, A.J.; Wu, J.H.; Teng, N.N.H.; Rubin, A.D. What Drives E-Health Usage? Integrated Institutional Forces and Top Management Perspectives. Comput. Hum. Behav. 2019, 97, 260–270. [Google Scholar] [CrossRef]
- Shea, C.M.; Belden, C.M. What Is the Extent of Research on the Characteristics, Behaviors, and Impacts of Health Information Technology Champions? A Scoping Review. BMC Med. Inform. Decis. Mak. 2015, 16, 2. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Velasco, F.; Classen, D.; Raddemann, R.J. Reducing Clinical Costs with an EHR: Investments in Performance Management Are Essential to Realizing the Full Benefits of an EHR System--Including Reduced Costs and Improved Quality of Care. Healthc. Financ. Manag. 2010, 64, 106–112. [Google Scholar]
- Blachowicz, D.; Christiansen, J.H.; Ranginani, A.; Sinimunich, K.L. How to Determine Future EHR ROI. Agent-Based Modeling and Simulation Offers a New Alternative to Traditional Techniques. J. Healthc. Inf. Manag. 2008, 22, 39–45. [Google Scholar] [CrossRef]
- Edwards, C. Nursing Leaders Serving as a Foundation for the Electronic Medical Record. Leadersh. Dev. J. TRAUMA Nurs. 2012, 19, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Delpha, D. Nurse Leaders Guide to a Large-Scale Information Technology Implementation. Nurse Lead. 2014, 12, 74–78. [Google Scholar] [CrossRef]
- Yen, P.-Y.; McAlearney, A.S.; Sieck, C.J.; Hefner, J.L.; Huerta, T.R. Health Information Technology (HIT) Adaptation: Refocusing on the Journey to Successful HIT Implementation. JMIR Med. Inform. 2017, 5, e28. [Google Scholar] [CrossRef] [PubMed]
- Fenton, S.H.; Ross, A.; Simmons, D. Training Leaders in Health Informatics. Stud. Health Technol. Inform. 2019, 264, 1184–1188. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Keywords | Database |
|---|---|
| Strategy I | |
| TI (“health services” OR “health care” OR healthcare OR hospital* OR care) AND TI (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND (leader* OR manage* OR administrat*) | CINAHL (EBSCO) Business Source Complete (EBSCO) |
| ti (“health services” OR “health care” OR healthcare OR hospital* OR care) AND ti (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND noft (leader* OR manage* OR administrat*) | ProQuest |
| TITLE (“health services” OR “health care” OR healthcare OR hospital* OR care) AND TITLE (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND TITLE-ABS-KEY (leader* OR manage* OR administrat*) | Scopus |
| TITLE: (“health services” OR “health care” OR healthcare OR hospital* OR care) AND TITLE: (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND TOPIC: (leader* OR manage* OR administrat*) | Web of Science |
| Strategy II | |
| TI (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND TI (leader* OR manage* OR administrat*) AND (“health services” OR “health care” OR healthcare OR hospital* OR care) | CINAHL (EBSCO) Business Source Complete (EBSCO) |
| Ti (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND ti (leader* OR manage* OR administrat*) AND noft(“health services” OR “health care” OR healthcare OR hospital* OR care) | ProQuest |
| TITLE (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND TITLE (leader* OR manage* OR administrat*) AND TITLE-ABS-KEY (“health services” OR “health care” OR healthcare OR hospital* OR care) | Scopus |
| TITLE: (“information technology” OR digi* OR “e-health” OR ehealth OR mhealth OR electronic OR telemedicine) AND TITLE: (leader* OR manage* OR administrat*) AND TOPIC: (“health services” OR “health care” OR healthcare OR hospital* OR care) | Web of Science |
| The Author(s) (Year) and the Journal | Country of Origin | The Aim of the Study | Data and Methods (Data Collection; Informants; Analysis Method(s)) | Key Findings Related to the Research Question |
|---|---|---|---|---|
| Boddy et al. (2009) [33] | UK | To identify to what extent generic management practices are evident in e-health projects, and to use that knowledge to develop a theoretical model of e-health implementation. | Semi-structured interviews with managers and health professionals (n = 18). Nvivo used for analysis. | Senior manager supported e-health implementation and made it essential to the working practices of senior managers. |
| Deokar & Sarnikar (2016) [34] | US | To describe how process change issues relate to implementation of large IT projects in healthcare settings. | Data consisted of application reports. Qualitative content analysis. | Management support is critical in EHR implementation. Strong physician and clinical leadership in implementation team were critical in communicating and supporting the goals and vision. Top organisation leaders served on the Leadership Council as well as different project implementation teams. Project implementation team leadership resolved conflicts. |
| Dugstad et al. (2019) [35] | Norway | To identify the facilitators and barriers for implementation of digital monitoring technology in residential care for persons with dementia and wandering behaviour, and to explore co-creation as an implementation strategy and practice. | Longitudinal case study, interviews (n = 23), strategic documents, participatory observations and process data from workshops (n = 7), observations of local training sessions and numerous meetings. Content analysis. | Healthcare leaders are responsible for developing new routines, roles and responsibilities. In addition, allocating sufficient time and resources across roles and professions for workshops and other implementation strategies proved to be a facilitator. The leaders’ priority was operating the service. Project managers provided technical support and filled the role of implementation champions. |
| Hall et al. (2017) [36] | UK | To explore facilitators and barriers to the implementation of monitoring technologies in care homes. | Semi-structured interviews of staff, relatives and residents (n = 36), observation, resident care record view. Framework analysis. | Senior management made decisions to implement HIT. |
| King et al. (2012) [37] | UK | To explore the way in which structural, professional and geographical boundaries have affected e-health implementation in health and social care. | Interviews of health and social care professionals (n = 30) and telephone interviews (n = 11). Framework analysis. | Managers made the decision to make SSA a necessary part of the referral process, when healthcare professionals were reluctant to use it. |
| Kujala et al. (2018) [38] | Finland | To identify good implementation practices and understand their use. | Survey-based data from supervisors and leaders (n = 478). Interviews with four project managers or coordinators. Descriptive statistics and content analysis. | The identified good practices were communicating clear leadership support, informing about the service implementation and its benefits, and user participation in planning. |
| Kujala et al. (2019) [39] | Finland | To evaluate clinical leaders’ eHealth competencies and training needs in two public healthcare organisations in Finland. | Online survey of clinical leaders (n = 98). Descriptive statistics and content analysis. | Clinical leader had critical role in supporting healthcare professionals and avoiding resistance to change. |
| Kujala et al. (2019) [40] | Finland | To examine whether frontline leaders’ positive expectations of a patient portal and perceptions of its implementation were associated with their support of the portal. To explore whether leaders’ positive perceptions influenced the same unit’s health professional support for the portal. | Online survey of 2067 health professionals and 401 frontline leaders. Several descriptive statistics and reliability analyses. | Healthcare leaders participated in the planning of patient portal service. Leaders’ clear vision of the patient portal was moderately associated with their support for the portal. |
| Mason et al. (2017) [41] | UK | To explore rural primary care physicians and physician assistants’ experiences regarding overcoming barriers to implementing electronic health records. | Interviews with physicians and physician assistants (n = 21). Phenomenological research analysis and narrative segments. | EHR implementation struggles when managers do not support it. The collaboration between healthcare leaders and providers might enhance the degree of operational, technological, clinical and financial success. |
| McAlearney et al. (2014) [42] | USA | To comprehensively study and synthesise best practices for managing ambulatory EHR system implementation in healthcare organisations, highlighting applicable management theories and successful strategies. | Interviews (n = 45) with key informants and six focus groups comprised of 37 physicians. Both deductive and inductive analysis methods. | Five factors that appear to facilitate successful management of HIT implementation were characterised: (1) commitment; (2) convincing/converting; (3) communication; (4) coordination; and (5) change management. |
| Nilsen et al. (2016) [43] | Norway | To identify and describe forms of resistance that emerged in five municipalities during a technology implementation project as part of the care for older people. | Data from interviews with focus groups (21 individuals, both healthcare providers and technology developers) and participatory observation (about 50 individuals, including five researchers). Kvale’s description of the bricolage approach and research triangulation. | Project managers and healthcare professionals experienced a lack of interest and support from middle managers, unit leaders and ward nurses. The need for training was recognised by project leaders and other participants, but responsible leaders did not arrange this. |
| Øvretveit et al. (2007) [44] | Sweden | To describe an implementation of one information technology system in one hospital, the perceived impact, the factors thought to help and hinder implementation, and the success of the system, comparing this with theories of effective IT implementation. | Qualitative case study using semi-structured interviews (n = 30) and documentation. Participants: senior clinicians, managers, project team members, doctors and nurses. Thematic analysis. | Top leadership was responsible for making a timetable and managing project tightly. Senior leaders set their date for implementation. Senior managers and heads of the clinics felt that HIT implementation was their highest priority. Hospital management group pointed out the importance of the project. |
| Poon et al. (2004) [45] | USA | N/A | Semi-structured interviews of senior managers (n = 52). Grounded-theory approach. | Overcoming resistance requires strong leadership. Healthcare leaders had to be firm believers of CPOE and they need to be able to manage changes that come with implementation. Some managers were among the first to adopt CPOE. |
| Stevenson et al. (2018) [46] | USA | To provide guidance and support for the implementation and spread of SCAN-ECHO. | Mixed-methods approach involving two quantitative surveys and qualitative interviews (n = 52). A consensual qualitative analysis. | Leaders provided technical support and gave resources for training session. |
| Szydlowski & Smith (2009) [47] | USA | To examine the trends of healthcare leadership and management with regard to implementation and management of IT in a hospital setting. | Interviews (n = 12) with CIOs and nurse managers. Comparative analysis. | Nurse managers thought that chief executive officer’s leadership and support of the HIT process increase the probability of efficient and effective HIT implementation. |
| Varsi et al. (2015) [48] | Norway | To examine the perceptions of nurse and physician managers regarding facilitators, barriers, management role, responsibility, and action taken in the implementation of an eHealth intervention called Choice into clinical practice. | A qualitative study with descriptive design based on individual interviews with nurse (n = 6) and physician managers (n = 3). Content analysis. | Managers supported the implementation, established collaboration between different actors and took the initiative to arrange training sessions. Managers also had Choice regularly on the agenda for their management meetings and managers spent time reminding nurses to use Choice and recommended it to colleagues. Managers felt it was their responsibility to ensure the implementation. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laukka, E.; Huhtakangas, M.; Heponiemi, T.; Kanste, O. Identifying the Roles of Healthcare Leaders in HIT Implementation: A Scoping Review of the Quantitative and Qualitative Evidence. Int. J. Environ. Res. Public Health 2020, 17, 2865. https://doi.org/10.3390/ijerph17082865
Laukka E, Huhtakangas M, Heponiemi T, Kanste O. Identifying the Roles of Healthcare Leaders in HIT Implementation: A Scoping Review of the Quantitative and Qualitative Evidence. International Journal of Environmental Research and Public Health. 2020; 17(8):2865. https://doi.org/10.3390/ijerph17082865
Chicago/Turabian StyleLaukka, Elina, Moona Huhtakangas, Tarja Heponiemi, and Outi Kanste. 2020. "Identifying the Roles of Healthcare Leaders in HIT Implementation: A Scoping Review of the Quantitative and Qualitative Evidence" International Journal of Environmental Research and Public Health 17, no. 8: 2865. https://doi.org/10.3390/ijerph17082865
APA StyleLaukka, E., Huhtakangas, M., Heponiemi, T., & Kanste, O. (2020). Identifying the Roles of Healthcare Leaders in HIT Implementation: A Scoping Review of the Quantitative and Qualitative Evidence. International Journal of Environmental Research and Public Health, 17(8), 2865. https://doi.org/10.3390/ijerph17082865