Active Commuting and Physical Fitness: A Systematic Review

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Data Extraction and Harmonization
2.4. Study Quality and Risk of Bias
2.5. Synthesis of Results
3. Results
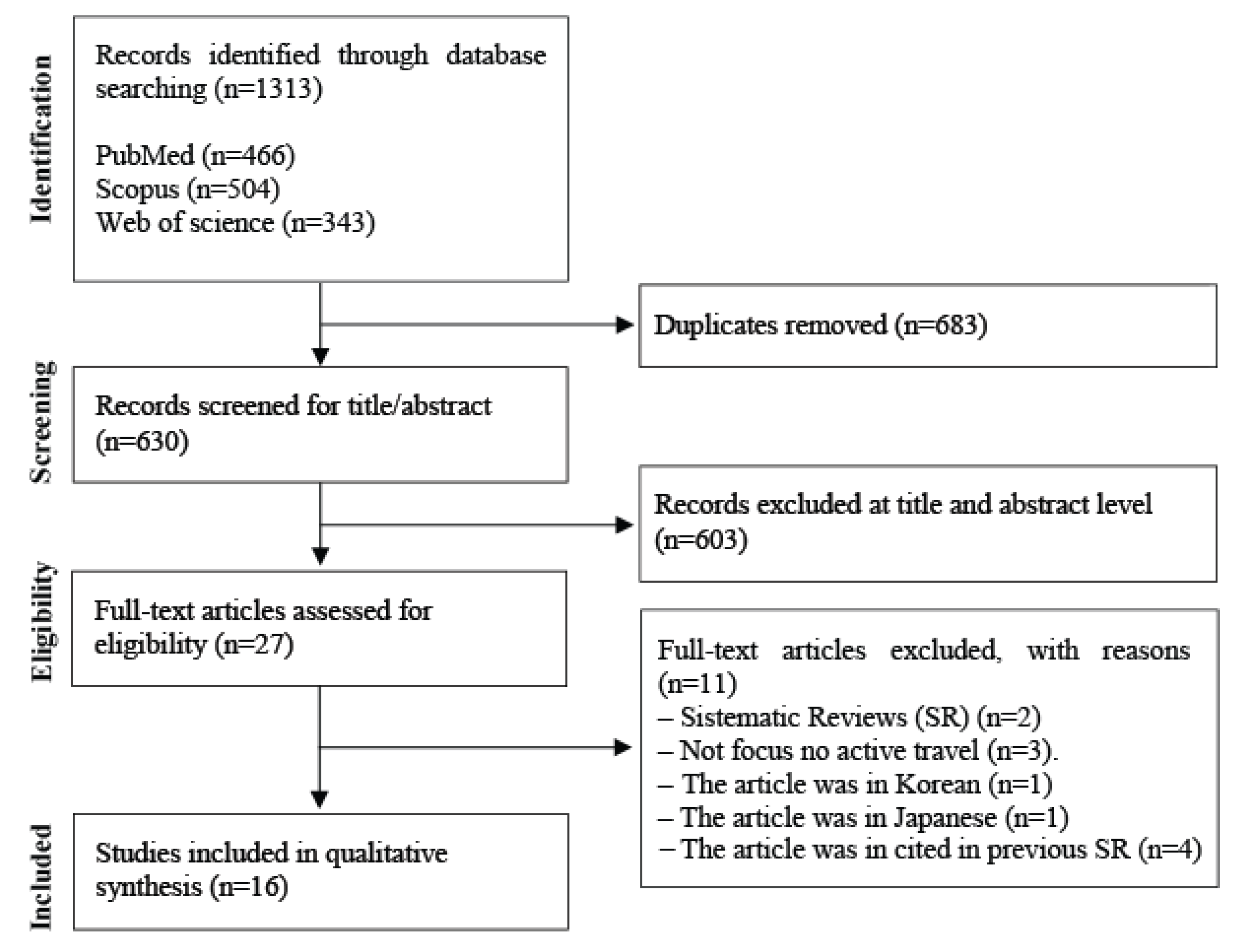
3.1. Search Results
3.2. Investigation Characteristics
3.2.1. Children/Adolescent
3.2.2. Adults
4. Discussion
4.1. Children/Adolescents

{kind=link}
| Author, Year | Study Design | Country | Sample | Physical Fitness Attribute (Measure) | Active Commuting Measure | Observation | Main Results | Study Quality |
|---|---|---|---|---|---|---|---|---|
| Børrestad et al., 2012 [35] | Experimental | Norway | Total n = 204 IG, 26 (10.8 ± 0.7 years), Boys (53.9%) CG, 27 (10.9 ± 0.7 years), boys (51.9%) | CRF: Peak oxygen consumption (VO2peak, mL O2/min/kg), HRpeak (h/min), BMI (kg/m2) | Participants reported how many days a week they traveled to/from school in the last 3 months by walking, cycling, car, or public transport. Distance to school (km). | Active commuting; Cycle ergometer test | Active commuting by cycling in both groups (IG and CG) improves the CRF in children. | Moderate |
| Chillón et al., 2012 [33] | Prospective cohort | Sweden | Total n = 262 120 boys, 142 girls Swedish children who were involved in the European Youth Heart Study (EYHS) | CRF: (VO2max) expressed in absolute terms (L/min); BMI (kg/m2); WC (cm); Skinfolds (mm) | Participants reported how they go to school. Passive: car, bus, train or Active: bicycle or walk (%) | Active commuting; Cycle ergometer test; calipers | Bicycling to school in childhood was related to improvements in fitness 6 years later. Children who became bicyclists in adolescence improved their fitness levels. No changes were observed for fatness. | Moderate |
| Østergaard et al., 2013 [12] | Cross-sectional | Norway | Total n = 1694, aged 9–15 years, 577 Boys, 482 Girls Norwegian who were participated in the Physical Activity among Norwegian Children Study | CRF: (VO2max, mL/kg/min); Functional strength (cm), Muscular endurance (n) (s); BMI (kg/m2); Skinfolds (mm) | Participants reported how they go to school: passively (car/ motorcycle or bus/train) or actively (bicycle or walk). | Active commuting Time of travel (minutes); Cycle ergometer test; Standing jump, Sit-ups, Biering–Sørensen test, Harpenden calipers | Active commuting, especially cycling, is positively associated with body composition, CRF, and MF when compared to passive commuting. | Strong |
| Ropero et al., 2014 [27] | Cross-sectional | England | Total n = 6829, aged 10–16 years; (53% males, age 12.9 ± 1.2 years) English adolescent who participated in the East of England Healthy Hearts Study | Muscular fitness: upper strength (kg), lower strength (cm) and (W·kg−1); BMI (kg/m2) | Participants reported how they go to school: passively (car or public transport) or actively (bicycle or walk. Distance to school (km). | Active commuting: Distance from home to school calculated by Google Maps. MF: Handgrip test, Vertical jump | When compared with passive travelers, cyclists had higher handgrip strength and walkers had higher vertical jump peak power. | Moderate |
| Villa-González et al., 2015 [28] | Cross-sectional | Spain | Total n = 494, aged 8–11 (9.2 ± 0.6) years, 577 Boys (9.3 ± 0.6 years), 229 (9.2 ± 0.6 years) Girls. | CRF (VO2max mL·min–1·kg–1, stage); MF (cm, kg), Agility (s). | Participants reported how they go to school: passively (car or public transport) or actively (bicycle or walk). | Active commuting Weekly frequency: (0–2 active travels vs. 3–7 active travels vs. 8–10 active travels); PACER test, Push-up test, Handgrip test, Standing long jump, Leg extension test. | No associations were found between active commuting with CRF and upper body MF. Positive associations between active commuting with agility and lower body MF in girls and boys. | Weak |
| Noonan et al., 2017 [30] | Cross-sectional | England | Total n = 194, aged 8–11 (9.2 ± 0.6) years, 87 Boys (9.97 ± 0.30 years), 107 Girls (9.95 ± 0.30 years). | CRF (laps); MF: upper strength (kg), lower strength (cm) and (W·kg−1); BMI (kg/m−2) | Participants reported by how they go to the school: passively (scooter, bus, car, train, taxi, other) or actively (bicycle or walk). | Active commuting; distance (km) calculated by Google Maps; PACER test, Push-up test, Handgrip test, Standing long jump, Leg extension test. | Active commuters, who live further away from school had better cardiorespiratory fitness. | Moderate |
| Pires et al., 2017 [31] | Cross-sectional | Brazil | Total n = 751, aged 7–17; 312 Boys and 349 Girls. | MF: upper strength (m), lower strength (m); Speed (s); Agility (s) BMI (kg/m2) | Participants reported how they go to school. Passive: car, bus, train or active- bicycle, walk (%) | Active commuting (%); Medicinal ball throw; Standing long jump; Square test. | Girls who actively commute to school showed better levels of upper limb strength and velocity. No significant difference was observed for the physical fitness between transport groups in boys. | Moderate |
| Villa-González et al., 2017 [34] | Quasi-experimental | Spain | Total n = 251, aged 8–11 (9.2 ± 0.6) years, IG: 73 boys and 68 girls; CG: 54 boys and 56 girls. | CRF (VO2max mL/kg/·min, stage); MF (cm, kg), Agility (s). | Participants reported how they go to school. Passively (car, bus, train) or actively (bicycle, walk). | Weekly frequency (0–2 active travels vs. 3–7 active travels vs. 8–10 active travels); PACER test, Push-up test, Handgrip test, Standing long jump, Leg extension test. | No associations between active commuters and health-related fitness. | Moderate |
| Ramirez-Veléz et al., 2017 [3] | Cross-sectional | Colombia | Total n = 2877, aged 7–17, 312 boys, 349 girls. | CRF Peak oxygen consumption (VO2peak mL/O2/min/kg); MF: upper strength (kg), lower strength (cm); Flexibility (cm); Agility (s); BMI (kg/m2), WC (cm). | Participants reported how they go to school: by car, public transportation or actively (walking, cycling). | Active commuting (days per week); PACER test; Handgrip test; Standing long jump test; 4 × 10 m shuttle run. | Regular cycling to school may be associated with better physical fitness, especially in girls. | Moderate |
| Muntaner-Mas et al., 2018 [32] | Cross-sectional | Spain | Total n = 2518, aged 10–16 years (13.0 ± 2.1). | CRF (VO2 peak, mL kg min−1); BMI (kg/m2). | Participants reported how they go to school. Passively (car, bus, train) or actively (by bicycle, walk, by riding skate). | Active commuting (%); PACER test. | No relationship between active commuting to school and CRF in children and adolescents. | Moderate |
| Ruiz-Hermosa et al., 2018 [29] | Cross-sectional | Spain | Total n = 2518, aged 4–7 years (13.0 ± 2.1). | CRF (VO2 peak, mL kg min−1); MF: lower strength (cm); BMI (kg/m2), WC (cm), Skinfolds (mm). | Children’s parents reported how they go to school. Passive (car, bus, train) or Active (bicycle, walk) | Active commuting (time); Course-Navette or PACER test; Standing long jump test; Holtain Ltd. Caliper | No relationship between walking to school with adiposity indicators, physical fitness. | Moderate |
| Author, Year | Study Design | Country | Sample | Physical Fitness Attribute (Measure) | Active Commuting Measure | Observation | Main Results | Study Quality |
|---|---|---|---|---|---|---|---|---|
| De Geus et al., 2009 [36] | Experimental | Belgium | Total n = 80 IG, 30 males (43 ± 6 years), 35 females (43 ± 3); CG, 7 males (50 ± 8 years), 8 females (48 ± 6 years) | CRF (Maximal external power [Pmáx (/kg)]; Peak oxygen uptake [VO2peak (/kg)], Absolute maximal external power (Pmáx), Relative peak oxygen uptake (VO2peak/kg), Heart ratio max (beats/min), respiratory exchange ratio (VCO2/VO2) | Participants reported a weekly diary. Distance and the time spend on each trip by car/motorcycle; bus/train; bicycle; walk to work. | Measured the distance and the time spend on each trip; cycle ergometer test. | The maximal external power and peak oxygen uptake increased significantly in IG (Male and Female). Cycling to work has the potential to increase physical performance in an untrained study population. | Moderate |
| Moller et al., 2011 [37] | Experimental | Denmark | Total n = 48 IG 13 males (43 ± 8.9 years), 6 females (44.4 ± 8); CG, 16 males (46.1 ± 9.9 years), 7 females (46 ± 9.1 years | CRF (VO2max ml/kg/min); Heart ratio max (beats/min); Respiratory exchange ratio (VCO2/VO2); BMI (kg/m2); Skinfolds (mm) | Participants used their bicycle and registered the cycling distance | Active commuting was calculated by (Mavic M-Tech 7) Cycle ergometer test; Harpenden calipers | CRF was significantly improved and body fat reduced in 8 weeks of commuter cycling. | Strong |
| Vaara, et al., 2014 [13] | Cross-sectional | Finland | Total n = 781, aged 18–90 years (47.1 ± 8.7 years); Male (81.9%) | CRF: VO2max, mL/kg/min. MF: reps/min, kg and N). WC (cm), body fat: bioelectrical impedance. | Participants reported a weekly diary. The time spend per day by bicycle or walk to work | Active commuting was classified by total time. CRF was assessed by cycle ergometer, and VO2max estimated from HR and maximal power. | The high active commuting group showed better results in CRF, some MF tests and WC with other active commuting groups. | Weak |
| Hochsmann et al., 2018 [38] | Experimental | Switzerland | Total n = 32 adults, aged 18–50 years. 28 males and 2 females | CRF: (VO2 peak, mL kg min−1); BMI (kg/m2). | E-bike group and bike group reported a typical route to work. | Active commuting (km and elevation calculated by Google Maps, Google Inc, Mountain View, California). CRF was assessed by cycle ergometer. | A period of 4 weeks of active commuting can lead to improvements in VO2peak in both groups. Moreover, no significant difference in VO2peak and maximal ergometric workload gain. | Weak |
| Blond et al., 2019 [24] | Experimental | Denmark | Total n = 130 adults, aged 20–45 years. CG 18 (male 9, female 9); IG bike 35 (male 16, female 19); IG/MOD 39 (male 19, female 20); IG/VIG 38 (male 20, female 18) | CRF: (VO2 peak, mL kg min−1); BMI (kg/m2). | The daily distance was calculated for participants in bike based on their energy expenditure while cycling from/to work/school. | The active commuting distance was monitored using Polar RC3 GPS (Polar, Finland). CRF was determined using an electronically braked cycle and open circuit indirect respiratory calorimetry. | CRF increased in all exercise active commuting groups compared with non-active commuting. | Strong |
4.2. Adults
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Physical Activity Strategy for the WHO European Region 2016–2025; Europe, R.C.F., Ed.; World Helath Organization: Vilnus, Lithuania, 2015. [Google Scholar]
- Committee, P.A.G.A. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Ramirez-Velez, R.; Correa-Bautista, J.E.; Lobelo, F.; Izquierdo, M.; Alonso-Martinez, A.; Rodriguez-Rodriguez, F.; Cristi-Montero, C. High muscular fitness has a powerful protective cardiometabolic effect in adults: Influence of weight status. BMC Public Health 2016, 16, 1012. [Google Scholar] [CrossRef] [PubMed]
- Australian Sports Commission. Addressing the Decline in Sport Participation in Secondary Schools; Australian Sports Commission: Bruce, Australia, 2017.
- Canada, P.H.A.O. A Common Vision for Increasing Physical Activity and Reducing Sedentary Living in Canada; Federal, P.A.T.G., Ed.; Diabetes Action Canada: Toronto, ON, Canada, 2018. [Google Scholar]
- Page, N.C.; Nilsson, V.O. Active Commuting: Workplace Health Promotion for Improved Employee Well-Being and Organizational Behavior. Front. Psychol. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Aparicio-Ugarriza, R.; Mielgo-Ayuso, J.; Ruiz, E.; Ávila, J.M.; Aranceta-Bartrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; González-Gross, M. Active Commuting, Physical Activity, and Sedentary Behaviors in Children and Adolescents from Spain: Findings from the ANIBES Study. Int. J. Environ. Res. Public Health 2020, 17, 668. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, A.N.; Ribeiro, J.C.; Marques, E.A.; Mota, J.; Santos, M.P. Is walking to school associated with improved metabolic health? Int. J. Behav. Nutr. Phys. Act. 2013, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hermoso, A.; Quintero, A.P.; Hernandez, E.; Correa-Bautista, J.E.; Izquierdo, M.; Tordecilla-Sanders, A.; Prieto-Benavides, D.; Sandoval-Cuellar, C.; Gonzalez-Ruiz, K.; Villa-Gonzalez, E.; et al. Active commuting to and from university, obesity and metabolic syndrome among Colombian university students. BMC Public Health 2018, 18, 523. [Google Scholar] [CrossRef] [PubMed]
- Steell, L.; Garrido-Mendez, A.; Petermann, F.; Diaz-Martinez, X.; Martinez, M.A.; Leiva, A.M.; Salas-Bravo, C.; Alvarez, C.; Ramirez-Campillo, R.; Cristi-Montero, C.; et al. Active commuting is associated with a lower risk of obesity, diabetes and metabolic syndrome in Chilean adults. J. Public Health 2018, 40, 508–516. [Google Scholar] [CrossRef]
- Cooper, A.R.; Wedderkopp, N.; Jago, R.; Kristensen, P.L.; Moller, N.C.; Froberg, K.; Page, A.S.; Andersen, L.B. Longitudinal associations of cycling to school with adolescent fitness. Prev. Med. 2008, 47, 324–328. [Google Scholar] [CrossRef]
- Ostergaard, L.; Kolle, E.; Steene-Johannessen, J.; Anderssen, S.A.; Andersen, L.B. Cross sectional analysis of the association between mode of school transportation and physical fitness in children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 91. [Google Scholar] [CrossRef]
- Vaara, J.P.; Kyrolainen, H.; Fogelholm, M.; Santtila, M.; Hakkinen, A.; Hakkinen, K.; Vasankari, T. Associations of leisure time, commuting, and occupational physical activity with physical fitness and cardiovascular risk factors in young men. J. Phys. Act. Health 2014, 11, 1482–1491. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjostrom, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Bouchard, C.; Blair, S.N.; Haskell, W. Physical Activity and Health, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Lee, M.C.; Orenstein, M.R.; Richardson, M.J. Systematic Review of Active Commuting to School and Children’s Physical Activity and Weight. J. Phys. Act. Health 2008, 5, 930–949. [Google Scholar] [CrossRef]
- Faulkner, G.E.J.; Buliung, R.N.; Flora, P.K.; Fusco, C. Active school transport, physical activity levels and body weight of children and youth: A systematic review. Prev. Med. 2009, 48, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Boreham, C.A.; Kelly, P.; Foster, C.E. The relationship between active travel to school and health-related fitness in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 5. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Saunders, T.J.; Faulkner, G.; Colley, R.; Tremblay, M. Associations between active school transport and physical activity, body composition, and cardiovascular fitness: A systematic review of 68 studies. J. Phys. Act. Health 2014, 11, 206–227. [Google Scholar] [CrossRef]
- Gordon-Larsen, P.; Nelson, M.C.; Beam, K. Associations among Active Transportation, Physical Activity, and Weight Status in Young Adults. Obes. Res. 2005, 13, 868–875. [Google Scholar] [CrossRef]
- Cooper, A.R.; Wedderkopp, N.; Wang, H.A.N.; Andersen, L.B.; Froberg, K.; Page, A.S. Active Travel to School and Cardiovascular Fitness in Danish Children and Adolescents. Med. Sci. Sports Exerc. 2006, 38, 1724–1731. [Google Scholar] [CrossRef]
- Andersen, L.B.; Lawlor, D.A.; Cooper, A.R.; Froberg, K.; Anderssen, S.A. Physical fitness in relation to transport to school in adolescents: The Danish youth and sports study. Scand. J. Med. Sci. Sports 2009, 19, 406–411. [Google Scholar] [CrossRef]
- Hoehner, C.M.; Barlow, C.E.; Allen, P.; Schootman, M. Commuting distance, cardiorespiratory fitness, and metabolic risk. Am. J. Prev. Med. 2012, 42, 571–578. [Google Scholar] [CrossRef]
- Blond, M.B.; Rosenkilde, M.; Gram, A.S.; Tindborg, M.; Christensen, A.N.; Quist, J.S.; Stallknecht, B.M. How does 6 months of active bike commuting or leisure-time exercise affect insulin sensitivity, cardiorespiratory fitness and intra-abdominal fat? A randomised controlled trial in individuals with overweight and obesity. Br. J. Sports Med. 2019, 53, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Tools, N.C.C.f.M.A. Quality Assessment Tool for Quantitative Studies Method. 2008. Available online: http://www.nccmt.ca/resources/search/14 (accessed on 1 July 2016).
- Ropero, A.B.; Nadal, A.; Mora, C.; Cohen, D.; Ogunleye, A.A.; Taylor, M.; Voss, C.; Micklewright, D.; Sandercock, G.R. Association between habitual school travel and muscular fitness in youth. Prev. Med. 2014, 67, 216–220. [Google Scholar] [CrossRef]
- Villa-Gonzalez, E.; Ruiz, J.R.; Chillon, P. Associations between Active Commuting to School and Health-Related Physical Fitness in Spanish School-Aged Children: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2015, 12, 10362–10373. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Hermosa, A.; Martinez-Vizcaino, V.; Alvarez-Bueno, C.; Garcia-Prieto, J.C.; Pardo-Guijarro, M.J.; Sanchez-Lopez, M. No Association Between Active Commuting to School, Adiposity, Fitness, and Cognition in Spanish Children: The MOVI-KIDS Study. J. Sch. Health 2018, 88, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Boddy, L.M.; Knowles, Z.R.; Fairclough, S.J. Fitness, fatness and active school commuting among liverpool schoolchildren. Int. J. Environ. Res. Public Health 2017, 14, 995. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.L.; Soares, S.S.; Welser, L.; da Silva, C.F.; Sehn, A.P.; Kern, D.G.; Valim, A.; Reuter, C.P.; Burgos, M.S. Association between commuting to school and physical fitness related to motor performance in schoolchildren. Rev. Epidemiol. Control. Infecc. 2017, 7, 9. [Google Scholar]
- Muntaner-Mas, A.; Herrador-Colmenero, M.; Borras, P.A.; Chillon, P. Physical activity, but not active commuting to school, is associated with cardiorespiratory fitness levels in young people. J. Transp. Health 2018, 10, 297–303. [Google Scholar] [CrossRef]
- Chillon, P.; Ortega, F.B.; Ruiz, J.R.; Evenson, K.R.; Labayen, I.; Martinez-Vizcaino, V.; Hurtig-Wennlof, A.; Veidebaum, T.; Sjostrom, M. Bicycling to school is associated with improvements in physical fitness over a 6-year follow-up period in Swedish children. Prev. Med. 2012, 55, 108–112. [Google Scholar] [CrossRef]
- Villa-Gonzalez, E.; Ruiz, J.R.; Mendoza, J.A.; Chillon, P. Effects of a school-based intervention on active commuting to school and health-related fitness. BMC Public Health 2017, 17, 20. [Google Scholar] [CrossRef]
- Borrestad, L.A.; Ostergaard, L.; Andersen, L.B.; Bere, E. Experiences from a randomised, controlled trial on cycling to school: Does cycling increase cardiorespiratory fitness? Scand. J. Public Health 2012, 40, 245–252. [Google Scholar] [CrossRef]
- de Geus, B.; Joncheere, J.; Meeusen, R. Commuter cycling: Effect on physical performance in untrained men and women in Flanders: Minimum dose to improve indexes of fitness. Scand. J. Med. Sci. Sports 2009, 19, 179–187. [Google Scholar] [CrossRef]
- Moller, N.C.; Ostergaard, L.; Gade, J.R.; Nielsen, J.L.; Andersen, L.B. The effect on cardiorespiratory fitness after an 8-week period of commuter cycling—a randomized controlled study in adults. Prev. Med. 2011, 53, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Hochsmann, C.; Meister, S.; Gehrig, D.; Gordon, E.; Li, Y.; Nussbaumer, M.; Rossmeissl, A.; Schafer, J.; Hanssen, H.; Schmidt-Trucksass, A. Effect of E-Bike Versus Bike Commuting on Cardiorespiratory Fitness in Overweight Adults: A 4-Week Randomized Pilot Study. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2018, 28, 255–265. [Google Scholar] [CrossRef]
- Armstrong, N.; Welsman, J. Youth cardiorespiratory fitness: Evidence, myths and misconceptions. Bull. World Health Organ. 2019, 97, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Welsman, J.; Armstrong, N. The 20 m shuttle run is not a valid test of cardiorespiratory fitness in boys aged 11–14 years. BMJ Open Sport Exerc. Med. 2019, 5, e000627. [Google Scholar] [CrossRef] [PubMed]
- Marta, C.C.; Marinho, D.A.; Barbosa, T.M.; Izquierdo, M.; Marques, M.C. Physical Fitness Differences Between Prepubescent Boys and Girls. J. Strength Cond. Res. 2012, 26, 1756–1766. [Google Scholar] [CrossRef] [PubMed]
- Buchowski, M.; Telford, R.M.; Telford, R.D.; Olive, L.S.; Cochrane, T.; Davey, R. Why Are Girls Less Physically Active than Boys? Findings from the LOOK Longitudinal Study. PLoS ONE 2016, 11, e0150041. [Google Scholar] [CrossRef]
- Aires, L.; Mendonça, D.; Silva, G.; Gaya, A.R.; Santos, M.P.; Ribeiro, J.C.; Mota, J. A 3-Year Longitudinal Analysis of Changes in Body Mass Index. Int. J. Sports Med. 2009, 31, 133–137. [Google Scholar] [CrossRef]
- Pabayo, R.; Gauvin, L.; Barnett, T.A.; Nikiéma, B.; Séguin, L. Sustained Active Transportation is associated with a favorable body mass index trajectory across the early school years: Findings from the Quebec Longitudinal Study of Child Development birth cohort. Prev. Med. 2010, 50, S59–S64. [Google Scholar] [CrossRef]
- Ross, R.; Hudson, R.; Stotz, P.J.; Lam, M. Effects of Exercise Amount and Intensity on Abdominal Obesity and Glucose Tolerance in Obese Adults. Ann. Intern. Med. 2015, 162, 325. [Google Scholar] [CrossRef]
- Wen, D.; Utesch, T.; Wu, J.; Robertson, S.; Liu, J.; Hu, G.; Chen, H. Effects of different protocols of high intensity interval training for VO2max improvements in adults: A meta-analysis of randomised controlled trials. J. Sci. Med. Sport 2019, 22, 941–947. [Google Scholar] [CrossRef]
- Verheggen, R.J.H.M.; Maessen, M.F.H.; Green, D.J.; Hermus, A.R.M.M.; Hopman, M.T.E.; Thijssen, D.H.T. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henriques-Neto, D.; Peralta, M.; Garradas, S.; Pelegrini, A.; Pinto, A.A.; Sánchez-Miguel, P.A.; Marques, A. Active Commuting and Physical Fitness: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2721. https://doi.org/10.3390/ijerph17082721
Henriques-Neto D, Peralta M, Garradas S, Pelegrini A, Pinto AA, Sánchez-Miguel PA, Marques A. Active Commuting and Physical Fitness: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(8):2721. https://doi.org/10.3390/ijerph17082721
Chicago/Turabian StyleHenriques-Neto, Duarte, Miguel Peralta, Susana Garradas, Andreia Pelegrini, André Araújo Pinto, Pedro António Sánchez-Miguel, and Adilson Marques. 2020. "Active Commuting and Physical Fitness: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 8: 2721. https://doi.org/10.3390/ijerph17082721
APA StyleHenriques-Neto, D., Peralta, M., Garradas, S., Pelegrini, A., Pinto, A. A., Sánchez-Miguel, P. A., & Marques, A. (2020). Active Commuting and Physical Fitness: A Systematic Review. International Journal of Environmental Research and Public Health, 17(8), 2721. https://doi.org/10.3390/ijerph17082721