Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study


Abstract
1. Introduction
1.1. Background
1.2. State of the Science
1.3. Legal Context
1.4. Aims
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Source
2.3. Data Collection
2.4. Variables
2.5. Statistical Analysis
3. Results
3.1. Demography
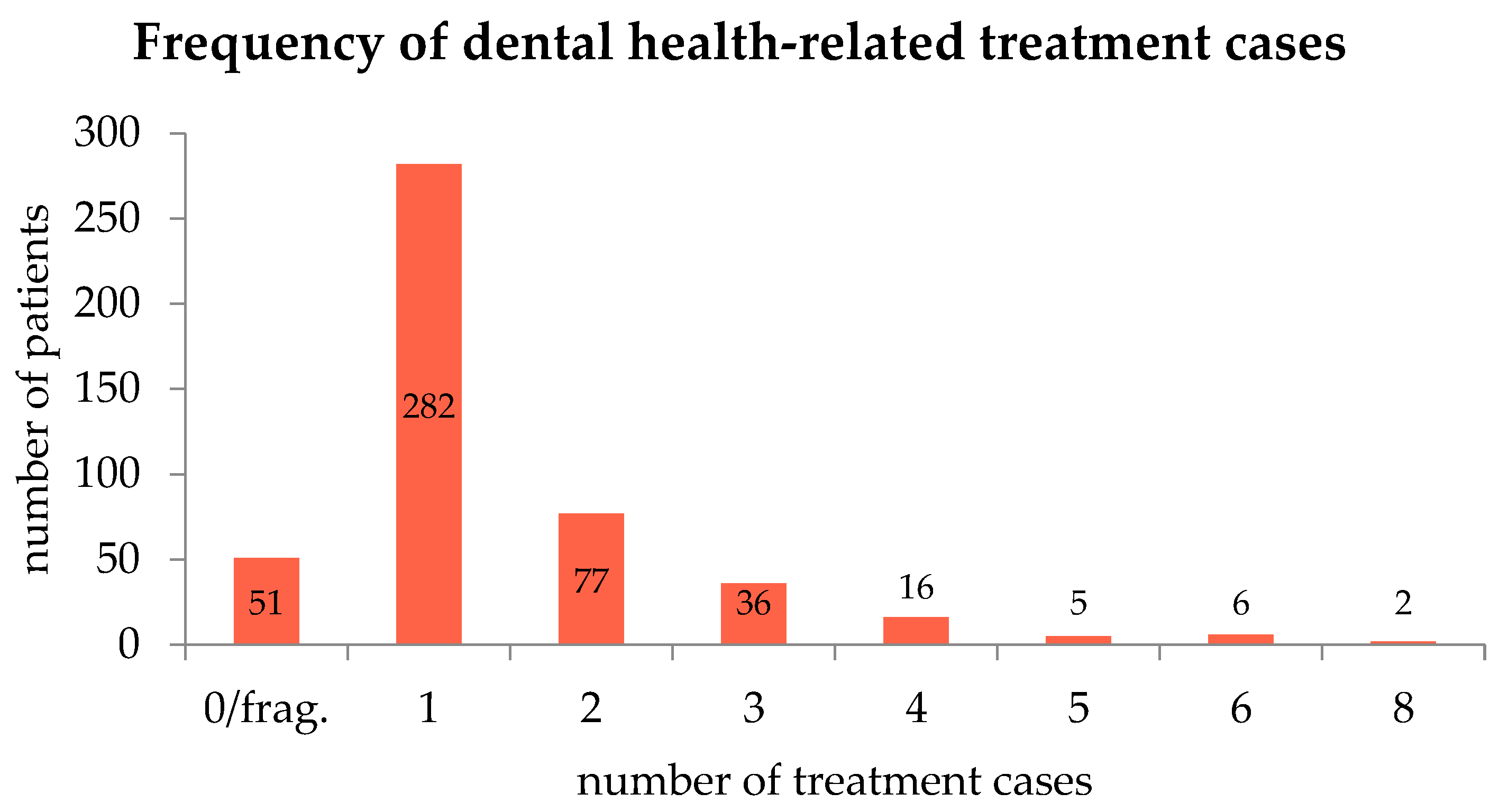
3.2. Dental Health Care Utilization
3.3. Clinical Presentations
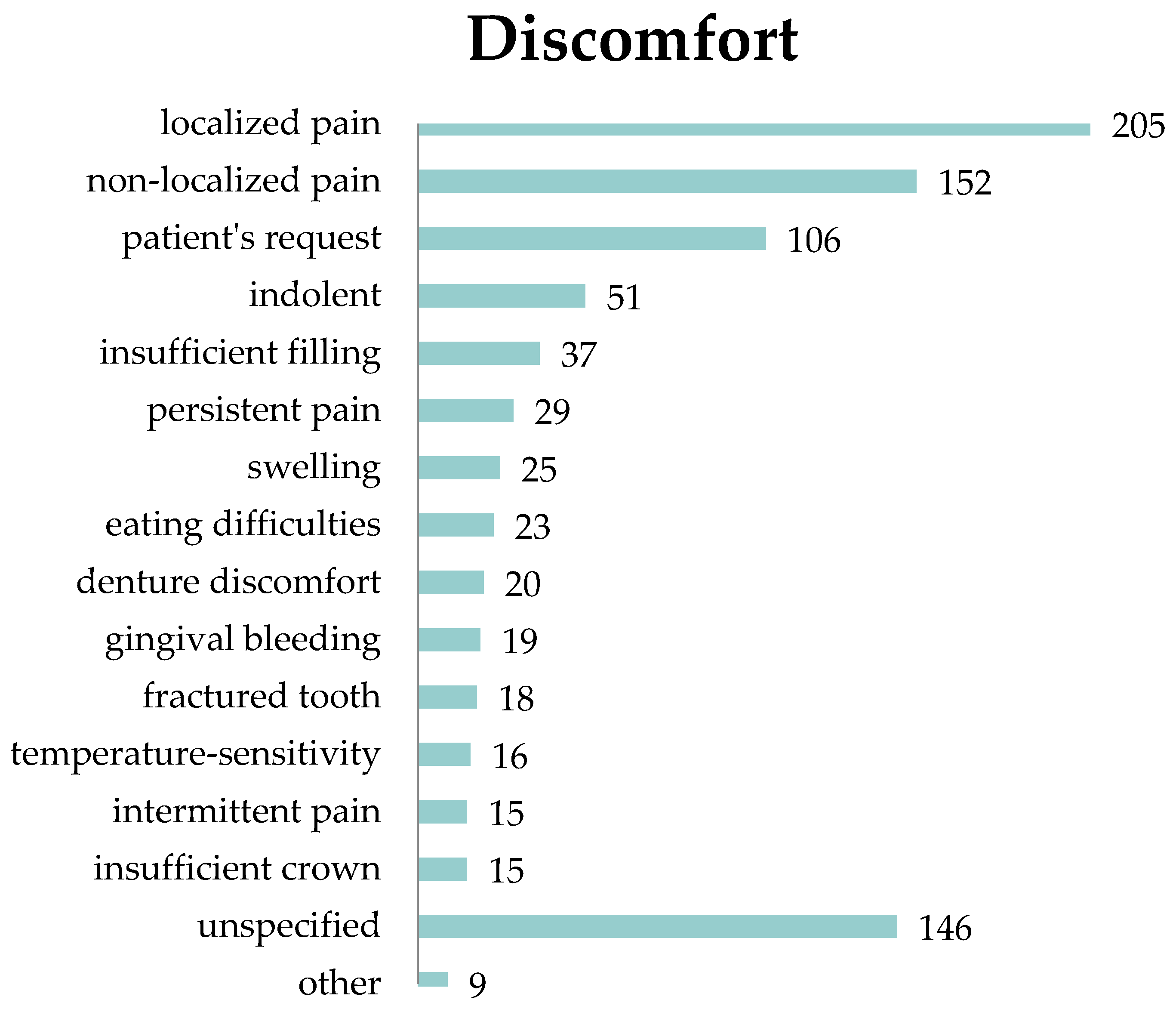
3.3.1. Discomfort
3.3.2. Diagnoses
3.3.3. Treatments
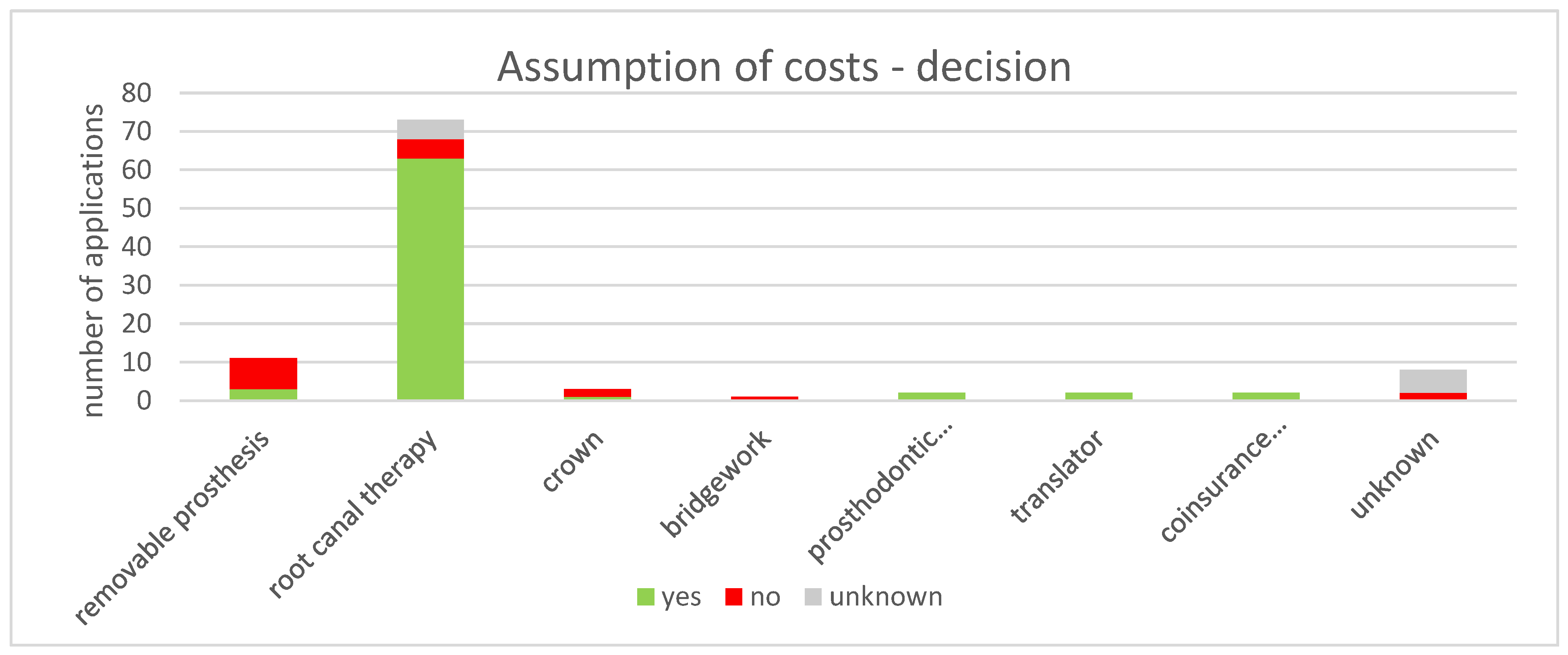
3.4. Assumption of Costs
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brzoska, P.; Razum, O. Herausforderungen einer diversitätssensiblen Versorgung in der medizinischen Rehabilitation. Rehabilitation 2017, 56, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Razum, O.; Geiger, I.; Zeeb, H.; Ronellenfitsch, U. Gesundheitsversorgung von Migranten. Dtsch. Ärzteblatt 2004, 101, 2882–2887. [Google Scholar]
- Dribbusch, B. Interimsprothese statt Brücke. 2. 10. 2015. Available online: https://taz.de/Aerztliche-Versorgung-von-Fluechtlingen/!5233590/ (accessed on 15 April 2019).
- Bundeszahnärztekammer. Zahnärztliche Behandlung von Asylbewerbern: Rechlicher Kontex; Bundeszahnärztekammer: Berlin, Germany, 2015. [Google Scholar]
- Almerich-Silla, J.M.; Montiel-Company, J.M.; Ruiz-Miravet, A. Caries and dental fluorosis in a western Saharan population of refugee children. Eur. J. Oral Sci. 2008, 116, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Kingsford Smith, D.; Szuster, F. Aspects of tooth decay in recently arrived refugees. Aust. N. Z. J. Public Health 2000, 24, 623–626. [Google Scholar] [CrossRef]
- Macdonald, M.E.; Keboa, M.T.; Nurelhuda, N.M.; Lawrence, H.P.; Carnevale, F.; McNally, M.; Singhal, S.; Ka, K.; Nicolau, B. The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol. Int. J. Environ. Res. Public Health 2019, 16, 542. [Google Scholar] [CrossRef]
- Reza, M.; Amin, M.; Sgro, A.; Abdelaziz, A.; Ito, D.; Main, P.; Azarpazhooh, A.; Amin, M.S. Oral Health Status of Immigrant and Refugee Children in North America: A Scoping Review. J. Can. Dent. Assoc. 2016, 82, 1488–2159. [Google Scholar]
- Strasen, T. Untersuchungen zur Zahngesundheit an Kindern der Würzburger Gemeinschaftsunterkunft für Flüchtlinge und Asylbewerber; Julius-Maximilians-Universität Würzburg: Würzburg, Germany, 2013. [Google Scholar]
- Splieth, C.H.; Takriti, M.; Ali Al-Ani, A.T. Studie Mundgesundheit Fluechtlinge: Flüchtlinge in Deutschland—Mundgesundheit, Versorgungsbedarfe und deren Kosten; DGZMK, KZVBV, BZÄK: Frankfurt, Germany, 2017. [Google Scholar]
- Solyman, M.; Schmidt-Westhausen, A.M. Oral health status among newly arrived refugees in Germany: A cross-sectional study. BMC Oral Health 2018, 18, 1. [Google Scholar] [CrossRef]
- Erdsiek, F.; Waury, D.; Brzoska, P. Oral health behaviour in migrant and non-migrant adults in Germany: The utilization of regular dental check-ups. BMC Oral Health 2017, 17, 84. [Google Scholar] [CrossRef]
- Goetz, K.; Winkelmann, W.; Steinhäuser, J. Assessment of oral health and cost of care for a group of refugees in Germany: A cross-sectional study. BMC Oral Health 2018. [Google Scholar] [CrossRef]
- Laban, C.J.; Gernaat, H.B.P.E.; Komproe, I.H.; de Jong, J.T.V.M. Prevalence and predictors of health service use among Iraqi asylum seekers in the Netherlands. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Toar, M.; O’Brien, K.K.; Fahey, T. Comparison of self-reported health & healthcare utilisation between asylum seekers and refugees: An observational study. BMC Public Health 2009. [Google Scholar] [CrossRef]
- Hadgkiss, E.J.; Renzaho, A.M.N. The physical health status, service utilisation and barriers to accessing care for asylum seekers residing in the community: A systematic review of the literature. Aust. Health Rev. 2014, 38, 142–159. [Google Scholar] [CrossRef]
- Razum, O.; Reiss, K.; Breckenkamp, J.; Kaufner, L.; Brenne, S.; Bozorgmehr, K.; Borde, T.; David, M. Comparing provision and appropriateness of health care between immigrants and non-immigrants in Germany using the example of neuraxial anaesthesia during labour: Crosssectional study. BMJ Open 2017. [Google Scholar] [CrossRef] [PubMed]
- Jäger, F.; Thomé, H. Leitfaden Alg II/Sozialhilfe von A.Z. In Ein praktischer Ratgeber für alle, die Arbeitslosengeld II/Sozialhilfe beziehen müssen und über Ihre Rechte informiert werden wollen; Digitaler Vervielfältigungs-und VerlagsService: Frankfurt, Germany, 2016. [Google Scholar]
- Asylum-Seekers’ Benefits Act, Paragraph 4. Available online: https://www.gesetze-im-internet.de/asylblg/__4.html (accessed on 15 January 2020).
- Asylum-Seekers’ Benefits Act, Paragraph 6. Available online: https://www.gesetze-im-internet.de/asylblg/__6.html (accessed on 15 January 2020).
- Medizinische Flüchtlingshilfe Göttingen E. V. Healthcare Voucher. Available online: http://gesundheit-gefluechtete.info/en/healthcare-voucher/ (accessed on 25 November 2019).
- Bundesministerium für Gesundheit. Health Guide: For asylum seekers in Germany, 3rd ed.; Task Force Migration und Gesundheit Referat Z24: Berlin, Germany, 2016. [Google Scholar]
- Albaum, C. Pressemitteilung: Klare und flächendeckende Rechtsgrundlagen statt Flickenteppich in der Versorgung; Kassenzahnärztliche Bundesvereinigung: Berlin, Germany, 2015. [Google Scholar]
- Razum, O.; Wenner, J.; Bozorgmehr, K. Wenn Zufall über den Zugang zur Gesundheitsversorgung bestimmt: Geflüchtete in Deutschland. Gesundheitswesen 2016, 78, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a World Beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef]
- Keboa, M.T.; Hiles, N.; Macdonald, M.E. The oral health of refugees and asylum seekers: A scoping review. Glob. Health 2016, 12, 59. [Google Scholar] [CrossRef]
- Ghiabi, E.; Matthews, D.C.; Brillant, M.S. The oral health status of recent immigrants and refugees in Nova Scotia, Canada. J. Immigr. Minor. Health 2014, 16, 95–101. [Google Scholar] [CrossRef]
- Cote, S.; Geltman, P.; Nunn, M.; Lituri, K.; Henshaw, M.; Garcia, R.I. Dental caries of refugee children compared with US children. Pediatrics 2004, 114, e733–e740. [Google Scholar] [CrossRef]
- Zeidan, A.J.; Khatri, U.G.; Munyikwa, M.; Barden, A.; Samuels-Kalow, M. Barriers to Accessing Acute Care for Newly Arrived Refugees. West J. Emerg. Med. 2019, 20, 842–850. [Google Scholar] [CrossRef]
- Van Loenen, T.; Van Den Muijsenbergh, M.; Hofmeester, M.; Dowrick, C.; Van Ginneken, N.; Mechili, E.A.; Angelaki, A.; Ajdukovic, D.; Bakic, H.; Pavlic, D.R.; et al. Primary care for refugees and newly arrived migrants in Europe: A qualitative study on health needs, barriers and wishes. Eur. J. Public Health 2018, 28, 82–87. [Google Scholar] [CrossRef]
- Antonipillai, V.; Baumann, A.; Hunter, A.; Wahoush, O.; O’Shea, T. Impacts of the Interim Federal Health Program reforms: A stakeholder analysis of barriers to health care access and provision for refugees. Can. J. Public Health 2017, 108, e435–e441. [Google Scholar] [CrossRef] [PubMed]
- Scheppers, E.; van Dongen, E.; Dekker, J.; Geertzen, J.; Dekker, J. Potential barriers to the use of health services among ethnic minorities: A review. Fam. Pract. 2006, 23, 325–348. [Google Scholar] [CrossRef] [PubMed]
- Green, M. Language Barriers and Health of Syrian Refugees in Germany. Am. J. Public Health 2017, 107, 486. [Google Scholar] [CrossRef] [PubMed]
- Crocombe, L.A.; Stewart, J.F.; Barnard, P.D.; Slade, G.D.; Roberts-Thomson, K.; Spencer, A.J. Relative oral health outcome trends between people inside and outside capital city areas of Australia. Aust. Dent. J. 2010, 55, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Farmer, P.; Sen, A. Pathologies of Power: Health, Human Rights, and the New War on the Poor; University of California Press: Berkeley, CA, USA, 2009. [Google Scholar]
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Spura, A.; Kleinke, M.; Robra, B.P.; Ladebeck, N. Wie erleben Asylsuchende den Zugang zu medizinischer Versorgung? Bundesgesundheitsbl 2017, 60, 462–470. [Google Scholar] [CrossRef]
- BARMER. Zahnvorsorge bei Erwachsenen—Prävention und Bonuspunkte durch regelmäßige Zahnarztbesuche. 2018. Available online: https://www.barmer.de/unsere-leistungen/leistungen-a-z/praevention-und-vorsorge/zahnvorsorge-bei-erwachsenen-9902 (accessed on 31 January 2020).
- Siemens-Betriebskrankenkasse. Zahnvorsorgeuntersuchungen für Kinder. Available online: https://www.sbk.org/beratung/leistungen/zahngesundheit/zahnvorsorge/zahnvorsorgeuntersuchungen-fuer-kinder/ (accessed on 15 January 2020).
- Rädel, M.; Bohm, S.; Priess, H.W.; Walter, M. BARMER Zahnreport 2017: Schriftenreihe zur Gesundheitsanalyse; Asgard Verlagsservice GmbH: Berlin, Germany, 2017. [Google Scholar]
- Hilton, I.V.; Stephen, S.; Barker, J.C.; Weintraub, J.A. Cultural factors and children’s oral health care: A qualitative study of carers of young children. Community Dent. Oral Epidemiol. 2007, 35, 429–438. [Google Scholar] [CrossRef]
- Führer, A. Asylbewerberleistungsgesetz: Abrechnung versus ärztliche Ethik. Dtsch. Ärzteblatt 2016, 113. Available online: https://www.aerzteblatt.de/archiv/178776/Asylbewerberleistungsgesetz-Abrechnung-versus-aerztliche-Ethik (accessed on 10 January 2019).
- Reinke, R. Leitfaden zur medizinischen Versorgung von Flüchtlingen mit Behinderung; Amadeu Antonio Stiftung: Berlin, Germany, 2016. [Google Scholar]
- Epping, B. Medizinische Versorgung von Flüchtlingen: Teure Hürden. Z. Orthopädie Unf. 2017, 155, 129–134. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Emami, E.; Ahmadi, M.; Eilayyan, O.; Abi-Nader, S.; Tamimi, F. Failure rate of single-unit restorations on posterior vital teeth: A systematic review. J. Prosthet. Dent. 2017, 117, 345–353. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Ahmadi, M.; Emami, E.; Abi-Nader, S.; Tamimi, F. Failure of single-unit restorations on root filled posterior teeth: A systematic review. Int. Endod. J. 2017, 50, 951–966. [Google Scholar] [CrossRef] [PubMed]
- Van de Rijt, L.J.M.; Stoop, C.C.; Weijenberg, R.A.F.; de Vries, R.; Feast, A.R.; Sampson, E.L.; Lobbezoo, F. The Influence of Oral Health Factors on the Quality of Life in Older People: A Systematic Review. Gerontologist 2019. [Google Scholar] [CrossRef] [PubMed]
- Rasines Alcaraz, M.G.; Veitz-Keenan, A.; Sahrmann, P.; Schmidlin, P.R.; Davis, D.; Iheozor-Ejiofor, Z. Direct composite resin fillings versus amalgam fillings for permanent or adult posterior teeth. Cochrane Database Syst. Rev. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- Roulet, J.F. Benefits and disadvantages of tooth-coloured alternatives to amalgam. J. Dent. 1997, 25, 459–473. [Google Scholar] [CrossRef]
- Mikhailichenko, N.; Yagami, K.; Chiou, J.Y.; Huang, J.Y.; Wang, Y.H.; Wei, J.C.C.; Lai, T.J. Exposure to Dental Filling Materials and the Risk of Dementia: A Population-Based Nested Case Control Study in Taiwan. Int. J. Environ. Res. Public Health 2019, 16, 3283. [Google Scholar] [CrossRef]
- Umesi, D.C.; Oremosu, O.A.; Makanjuola, J.O. Amalgam phase down: Baseline data preceding implementation in Nigeria. Int. Dent. J. 2019. [Google Scholar] [CrossRef]
- Heidari, E.; Andiappan, M.; Banerjee, A.; Newton, J.T. The oral health of individuals with dental phobia: A multivariate analysis of the Adult Dental Health Survey, 2009. Br. Dent. J. 2017, 222, 595–604. [Google Scholar] [CrossRef]
- Gruber, D. Leistungsverzeichnis für die Leistungsberechtigten nach § 1 AsylbLG; Kassenzahnärztliche Vereinigung Bayerns (KZVB): München, Germany, 2015. [Google Scholar]
- Köber, C. Bayern regelt Zahnmedizin für Flüchtlinge. 09.10.2015. Available online: https://www.zm-online.de/news/politik/bayern-regelt-zahnmedizin-fuer-fluechtlinge/ (accessed on 28 October 2019).
- Fehmel, T. Entscheidungsspielräume im Sozialleistungsrecht—Konsequenzen für die Soziale Arbeit. Z. Soz. 2017. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients n = 475 | All Asylum-Seekers n = 4107 | |
|---|---|---|---|
| Gender, n (%) | Female | 134 (28.2) | 1103 (26.9) |
| Male | 341 (71.8) | 3004 (73.1) | |
| Country of origin, n (%) | Syria | 187 (39.4) | 1957 (47.7) |
| Afghanistan | 46 (9.7) | 354 (8.6) | |
| Iran | 38 (8.0) | 180 (4.4) | |
| Somalia | 29 (6.1) | 173 (4.2) | |
| Guinea-Bissau | 21 (4.4) | 116 (2.8) | |
| Russian Federation | 21 (4.4) | 98 (2.4) | |
| Eritrea | 18 (3.8) | 83 (2.0) | |
| India | 14 (3.0) | 121 (2.9) | |
| Kosovo | 14 (3.0) | 88 (2.1) | |
| Benin | 11 (2.3) | 168 (4.1) | |
| unknown | 4 (0.8) | 28 (0.7) | |
| others | 72 (15.2) | 741 (18.0) | |
| Age group in years, n (%) | 0 ≤ 5 | 6 (1.3) | 322 (7.9) |
| 5 ≤ 10 | 25 (5.3) | 238 (5.8) | |
| 10 ≤ 15 | 14 (3.0) | 171 (4.2) | |
| 15 ≤ 20 | 41 (8.6) | 467 (11.4) | |
| 20 ≤ 25 | 86 (18.1) | 795 (19.4) | |
| 25 ≤ 30 | 99 (20.8) | 746 (18.2) | |
| 30 ≤ 35 | 71 (15.0) | 535 (13.0) | |
| 35 ≤ 40 | 55 (11.6) | 340 (8.3) | |
| 40 ≤ 45 | 28 (5.9) | 195 (4.8) | |
| 45 ≤ 50 | 29 (6.1) | 147 (3.6) | |
| > 50 | 21 (4.4) | 151 (3.7) | |
| Diagnosis | Subgroup | Absolute Frequency | Proportion in All Patients [%] (95%-CI) | Proportion in All Asylum–Seekers [%] (95%-CI) |
|---|---|---|---|---|
| Caries | 469 | 98.7 (97.7–99.7) | 11.4 (8.5–14.3) | |
| Primary caries | 100 | 21.1 (17.4–24.8) | 2.4 (1.0–3.8) | |
| Secondary caries | 51 | 10.7 (7.9–13.5) | 1.2 (0.2–2.2) | |
| Incipient caries | 2 | 0.4 (0–1.0) | 0.1 (0–0.4) | |
| Carious lesion | 101 | 21.3 (17.6–25.0) | 2.5 (1.1–3.9) | |
| Moderate caries | 12 | 2.5 (1.1–3.9) | 0.3 (0–0.8) | |
| Deep caries | 107 | 22.5 (18.7–26.3) | 2.6 (1.2–4.0) | |
| Deep complicated caries | 96 | 20.2 (16.6–23.8) | 2.3 (1.0–3.6) | |
| Periodontitis 1 | 115 | 24.2 (20.3–28.1) | 2.8 (1.3–4.3) | |
| Apical periodontitis | 80 | 16.8 (13.4–20.2) | 2.0 (0.7–3.3) | |
| Marginal periodontitis | 25 | 5.3 (3.3–7.3) | 0.6 (0–1.3) | |
| Periodontitis (unclassified) | 10 | 2.1 (0.8–3.4) | 0.2 (0–0.6) | |
| Pulpitis | 67 | 14.1 (11.0–17.2) | 1.6 (0.5–2.7) | |
| Irreversible pulpitis | 64 | 13.5 (10.4–16.6) | 1.6 (0.5–2.7) | |
| Reversible pulpitis | 3 | 0.6 (0–1.3) | 0.1 (0–0.4) | |
| Gingivitis | 37 | 7.8 (5.4–10.2) | 0.9 (0.1–1.7) | |
| Defective restorations | 108 | 22.7 (18.9–26.5) | 2.6 (1.2–4.0) | |
| Root canal prepared | 102 | 21.5 (17.8–25.2) | 2.5 (1.1–3.9) | |
| Poor teeth conditions | 275 | 57.9 (53.5–62.3) | 6.7 (4.5–8.9) | |
| Teeth not worthy of preserving 2 | 139 | 29.3 (25.2–33.4) | 3.4 (1.8–5.0) | |
| Retained/Remnant root | 74 | 15.6 (12.3–18.9) | 1.8 (0.6–3.0) | |
| Insufficient dentition | 38 | 8.0 (5.6–10.4) | 0.9 (0.1–1.7) | |
| Lack of oral hygiene | 24 | 5.1 (3.1–7.1) | 0.6 (0–1.3) | |
| Prosthetic replacement | 17 | 3.6 (1.9–5.3) | 0.4 (0–1.0) | |
| inflammation | 32 | 6.7 (4.5–8.9) | 0.8 (0–1.6) | |
| Gumboil | 11 | 2.3 (1.0–3.6) | 0.3 (0–0.8) | |
| Cyst | 6 | 1.3 (0.3–2.3) | 0.2 (0–0.6) | |
| Deep periodontal pocket | 7 | 1.5 (0.4–2.6) | 0.2 (0–0.6) | |
| fistula | 8 | 1.7 (0.5–2.9) | 0.2 (0–0.6) | |
| Accretion | 50 | 10.5 (7.7–13.3) | 1.2 (0.2–2.2) | |
| Plaque | 24 | 5.1 (3.1–7.1) | 0.6 (0–1.3) | |
| Calculus | 26 | 5.5 (3.4–7.6) | 0.6 (0–1.3) | |
| Miscellaneous | 311 | 65.5 (61.2–69.8) | 7.6 (5.2–10.0) | |
| Aftertreatment | 138 | 29.1 (25.0–33.2) | 3.4 (1.8–5.0) | |
| Uncomplaining | 61 | 12.8 (9.8–15.8) | 1.5 (0.4–2.6) | |
| Unspecified | 26 | 5.5 (3.4–7.6) | 0.6 (0–1.3) | |
| No communication possible | 25 | 5.2 (3.2–7.2) | 0.6 (0–1.3) | |
| Other | 61 | 12.8 (9.8–15.8) | 1.5 (0.4–2.6) |
| Absolute | All Patients (%) | All Asylum-Seekers (%) | |||||
|---|---|---|---|---|---|---|---|
| Male | Female | Total | Total | Male | Female | Total | |
| Clinical examination and consultation | 310 | 125 | 435 | 91.6 | 10.3 | 11.3 | 10.6 |
| Radiography | 198 | 59 | 257 | 54.1 | 6.6 | 5.4 | 6.3 |
| Prophylaxis (all) | 55 | 35 | 90 | 19.0 | 1.8 | 3.2 | 2.2 |
| Prophylaxis (age 6–17 years) | 14 | 9 | 23 | 51.1 | 4.3 | 4.5 | 4.4 |
| Tooth preparation and filling | 108 | 59 | 167 | 35.2 | 3.6 | 5.4 | 4.1 |
| Pulp and root canal treatment | 122 | 47 | 169 | 35.6 | 4.1 | 4.3 | 4.1 |
| Extraction | 100 | 34 | 134 | 28.2 | 3.3 | 3.1 | 3.3 |
| Surgical intervention | 84 | 27 | 111 | 23.4 | 2.8 | 2.5 | 2.7 |
| Minimal intervention | 45 | 22 | 67 | 14.1 | 1.5 | 2.0 | 1.6 |
| Anaesthesia | 203 | 71 | 274 | 57.7 | 6.8 | 6.4 | 6.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freiberg, A.; Wienke, A.; Bauer, L.; Niedermaier, A.; Führer, A. Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 2672. https://doi.org/10.3390/ijerph17082672
Freiberg A, Wienke A, Bauer L, Niedermaier A, Führer A. Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study. International Journal of Environmental Research and Public Health. 2020; 17(8):2672. https://doi.org/10.3390/ijerph17082672
Chicago/Turabian StyleFreiberg, Anna, Andreas Wienke, Lena Bauer, Andreas Niedermaier, and Amand Führer. 2020. "Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study" International Journal of Environmental Research and Public Health 17, no. 8: 2672. https://doi.org/10.3390/ijerph17082672
APA StyleFreiberg, A., Wienke, A., Bauer, L., Niedermaier, A., & Führer, A. (2020). Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study. International Journal of Environmental Research and Public Health, 17(8), 2672. https://doi.org/10.3390/ijerph17082672