1. Introduction
Cardiovascular disorders are the most common cause of mortality worldwide, including Poland and most European countries [
1]. Seasonal peaks in acute myocardial infarction incidence have been widely reported. Weather has been postulated to be one of the elements greatly contributing to this association [
2]. However, it is difficult to clearly establish relationships between meteorological or synoptic factors and decline in people’s mood or well-being. The reasons for that may lie, e.g., in varied responses to weather related stimuli, or in synergistic effects produced by various meteorological factors. Due to this, results obtained by various researchers frequently cannot be compared because of the different methodologies applied in studies. Nevertheless, in order to get better understanding of health-related effects produced by various environmental factors, there is a need for further research focusing on possible links between specific medical conditions and selected weather phenomena.
The term “föhn” is used with reference to a type of strong and turbulent wind blowing down from mountain crests towards the lee side and bringing dry and warm air to the surface. Foehn events rather frequently occur in the Alps, or more specifically on the northern side of the mountains, and constitute a significant challenge in weather forecasting for the Alpine valleys, inhabited by many people. The northern Alpine foehn is frequently observed in the prefrontal environment. The foehn clearance reflects the leeward range of the foehn in the mountains, i.e., a region with no clouds where dry and warm air occurs at the surface, just as in the foehn region but with no strong winds. This meteorological phenomenon is not unique to the Alps, and it can be observed over other high mountains worldwide [
3].
A local variety of foehn, “halny” wind, is produced by violent flow of air masses from the southern side of the Carpathians or the Sudetes. This happens when Poland is approached from the west by a deep cyclone (low-pressure area), while the anticyclone centre (high-pressure) is in Ukraine [
3,
4]. In addition to an abrupt change in temperature and its large speed, there are also other consequences of halny wind. The first involves rapid pressure drop, and a second is linked with increased condensation of positive ions in the air as a result of which microscopic particles of gases and aerosols, including harmful elements and chemical compounds, can easily penetrate organisms [
3,
4]. Halny wind frequently leads to considerable increase in the temperature and decrease in humidity on the leeward side of the mountains. The strong abrupt gusts of wind at times reach a speed typical of a hurricane and are accompanied with characteristic calm intervals. The foehn winds are observed in the Tatras rather frequently, particularly during the cold seasons. The criteria commonly applied by Polish researchers investigating foehn winds occurring in the mountainous areas include: direction (usually 90–270°) and wind speed (>4 m/s, commonly ≥10 m/s, at times increasing to even 60 m/s), occurrence of strong gusts and calm intervals, sudden rise in the air temperature (by several degrees in a short time) and decrease in the humidity (commonly ≤70%), and changes in atmospheric pressure and/or certain types of cloud. In foothill and lowland areas, the wind is dry and warm [
4].
It is believed that foehn wind may lead to increased aggressiveness, more severe depressive states, emotional crises ending with suicide attempts, agitation, anxiety, fatigue, weariness, muscle and joint pain, problems with concentration, sleep disorders, migraine, and headaches [
4,
5,
6,
7].
People with high sensitivity to weather changes are referred to as meteoropaths. They present increased tension towards the vegetative system and poor adaptative responses. Effects of weather fronts, in particular cold fronts, include decrease in the temperature and increase in the atmospheric pressure, responses to which include vasoconstriction, potentially posing a burden for the circulatory system [
8,
9,
10]. Nowadays, it is estimated that the number of meteoropaths is consistently growing. According to the data from the Institute of Meteorology and Water Management, as many as 50–70% of Poles respond to weather changes [
11]. Similar statistics have been published in other countries, e.g., in Germany 54.5% of the population is weather sensitive and in Canada the relevant rate amounts to 61% [
12]. It is also believed that meteoropathy is a “disease” of affluence, caused by stress, work overload, and unhealthy lifestyles, since meteoropaths are mainly residents of urban areas, whose immunity is affected by the long time spent in the artificial microclimates of their homes and offices, by a lack of exercise and by polluted air. It has also been pointed out that meteoropathy is most commonly observed in individuals affected by coronary disease, hypertension and ulcer disease [
8,
9,
10,
13].
A large body of evidence reported in the literature shows there is an association between wind- related environmental variables and cardiovascular or cerebrovascular events, with impact observed also on the preceding days [
14,
15,
16,
17,
18,
19,
20,
21,
22,
23]. Boussoussou et al. have reported positive significant association between acute cardiovascular diseases and a cold front effect lagged by one day [
14]. Mohammad et al. demonstrated that incidence of myocardial infarction increased with higher wind velocity, lower air temperature, lower atmospheric air pressure, and shorter sunshine duration [
15]. Similarly, Honda et al. found that increased incidence of acute myocardial infarction corresponds to lower minimum temperature occurring on the second day preceding the onset of wind [
17]. Radišauskas et al. established that myocardial infarction morbidity is directly correlated to wind speed and atmospheric pressure and inversely correlated to atmospheric temperatures and rainfall level [
16]. Goerre et al. reported that the incidence of myocardial infarctions is significantly affected by wind activity, ambient pressure, and pressure gradient [
15]. Vencloviene et al. showed that prognostic factors for the risk of acute coronary syndromes include such environmental variables as wind speed, daily air temperature, and barometric pressure on the day of the onset and on the two days preceding the ambulance call [
18]. Likewise, Ezekowitz et al. showed relationships between the likelihood of an acute coronary event and rapid changes in weather conditions (including excessively frequent increases in wind speed) [
19]. Hensel et al. showed that increasing wind speed corresponds to greater likelihood of out-of-hospital cardiac arrest of presumed cardiac aetiology [
20]. Vencloviene et al. demonstrated that increased risk of paroxysmal atrial fibrillation occurring at night was linked with wind speed above the median (lag 2–4 days) [
21]. Tamasauskiene et al. pointed out that a greater risk of ischemic stroke in older patients was associated with high wind speed on the day of the incident [
22]. Similarly, Kim et al. showed that the odds ratios for wind speed, daily wind speed range, and wind chill for patients with ischemic stroke were slightly greater than in the total sample [
23].
Effects of seasonal changes in environmental variables have also been pointed out. According to Gallerani et al., it is possible to observe six-month-period regularities in the incidence of subarachnoid haemorrhage, spring and autumn being the peak seasons. The authors propose an explanation that during these transitional seasons the arterial wall is exposed to frequent stress episodes due to typical changes in temperature and that may result in aneurysmal rupture occurring more frequently than, e.g., during the more stable periods of winter cold [
24]. Investigators from the International Worldwide Registry reported that the high incidence of acute aortic dissection in winter is observed in various climate settings (both cold and temperate), which seems to suggest that the major mechanistic factors contributing to the phenomenon include the relative change in temperature, rather than absolute temperature, and/or circannual rhythms [
25].
Clinical studies provide evidence that some meteorological factors, and most importantly weather changes occurring rapidly, e.g., in one day, may play an important role in inducing subjectively perceived indisposition in healthy individuals and in promoting disease symptoms in patients. Notably, the same weather changes may induce completely different bodily responses. As an example, a large drop in barometric pressure will induce a decrease in blood pressure in some individuals and an increase in other people [
2,
26,
27,
28,
29]. Due to this no uniform recommendations for dealing with sudden changes in weather can be addressed, e.g., to all patients with cardiovascular problems.
It has been shown that meteorotropic responses in both healthy people and individuals affected by medical conditions may be observed more in advance of specific changes in weather; in extreme cases these may be “sensed” up to 48 h before they actually happen. Such sensitivity may result from the changes in the electric field of the atmosphere, preceding arrival of a weather front [
30,
31,
32]. It has also been reported that changes in atmospheric pressure produce adverse effects in the human body, possibly also leading to cardiac incidents [
33,
34,
35,
36].
As early as 1953, it was suggested by Petersen that the human organism may be stimulated by specific relationships between weather fronts [
6]. Cardiovascular problems are most frequently listed among meteorotropic diseases. In Poland the earliest studies focusing on impact of weather on functioning of the cardio-vascular system were carried out in the mid-1800s [
6]. Research shows impact of short-term weather changes on intensity of ischemic heart disease symptoms, increased oscillations in arterial blood pressure, and higher incidence of acute myocardial infarction. Over 34% of fatal cases of myocardial infarction co-occur with a passage of weather fronts, compared to only 6% observed during periods of calm weather linked with high pressure [
37]. A survey conducted by Baranowska showed that in the respondents’ opinion, meteoropaths are adversely affected by weather transitions from highs to lows [
6]. In a study conducted by Höppe, individuals sensitive to weather, living in northern Germany, negatively assessed stormy weather (30%) and influx of cold air (29%). On the other hand, inhabitants of southern Germany experienced mood decline accompanying influx of warm (30%) rather than cold air (18%). This difference may be associated with the quite frequent foehn winds in southern Germany [
38]. Mackensen et al. investigated effects of weather in the sense of well-being observed in people living in Germany and in Canada. The authors reported weather sensitivity in 54.5% of the subjects representing the German population while in Canada the rate amounted to 61% [
12]. Likewise, Shiue et al. found a relationship between weather conditions, including wind speed, and hospital admissions due to heart disease in Germany [
39]. The same relationship was shown by studies conducted in Switzerland [
40] and Lithuania [
16].
The foehn wind known as “halny”, occurring in southern Poland, has as equally bad a reputation as the foehn winds blowing in other parts of Europe and the world. The aim of this study was to examine the impact of the foehn wind and the related environmental variables on the incidence of cardiac events in the population inhabiting a region affected by halny wind. We also decided to determine whether the environmental changes coincide with or predate the event examined.
4. Discussion
Based on a review of the literature it can be concluded that many researchers are investigating the association between wind-related environmental variables, and cardio- or cerebrovascular events, including the impact observed on days preceding onset of such weather conditions [
14,
15,
16,
17,
18,
19,
20,
21,
22,
23].
The current study was an attempt to collect evidence related to the impact of foehn wind and the related environmental variables on the incidence of cardiac events. The basic meteotropic factor adopted in the study was defined as halny wind and the accompanying change from cold to warm weather front.
Contrary to the findings reported by other researchers [
14,
15,
16,
17,
18,
19,
20,
21,
22,
23], the current study did not confirm effects of environmental factors investigated, i.e., air temperature, atmospheric humidity, speed of wind, pressure and total daily precipitation in the incidence of cardiac events, either on halny days or on days preceding the onset of halny, as well as throughout the whole year in the consecutive months from January 2011 to December 2011. The findings showed no statistically significant correlations between the environmental variables and the number of cardiac events in any of the periods analysed (i.e., days with halny, days preceding halny onset, total days with and preceding halny, other days, all the days combined.) This may be linked with the fact that the data acquired in the current study may be treated as preliminary, and in fact we are planning to carry out further study where we want to acquire more comprehensive data from other hospitals. However, it should be remembered that some of the hospitals may be located further away than others from the Tatra Mountains. Hence, it may be difficult to compare the acquired results. Likewise, Honda et al. explained that their study focused on the association between meteorological factors and frequency of acute myocardial infarction in patients residing in a small, strictly defined region, because the potential variations in weather conditions that are likely to occur in a larger area would have adversely affected their analyses [
17]. In view of the above, in our study we have collected evidence on the effects of halny wind in this particular territory. Nevertheless, it is necessary to conduct further research which will take into account other factors, such as air pollution, individuals’ socioeconomic status, lifestyle, body mass index, physical activity, etc. because, based on our findings it may be hypothesised that since there are no correlations between the environmental variables and the number of cardiac events, incidence of myocardial infarction may be linked with other factors rather than weather. These issues will be investigated in our future studies. Other researchers also point out that it is necessary to assess other risk factors that may influence the relationships of environmental variables and the incidence of cardiac events [
14,
20,
21,
22].
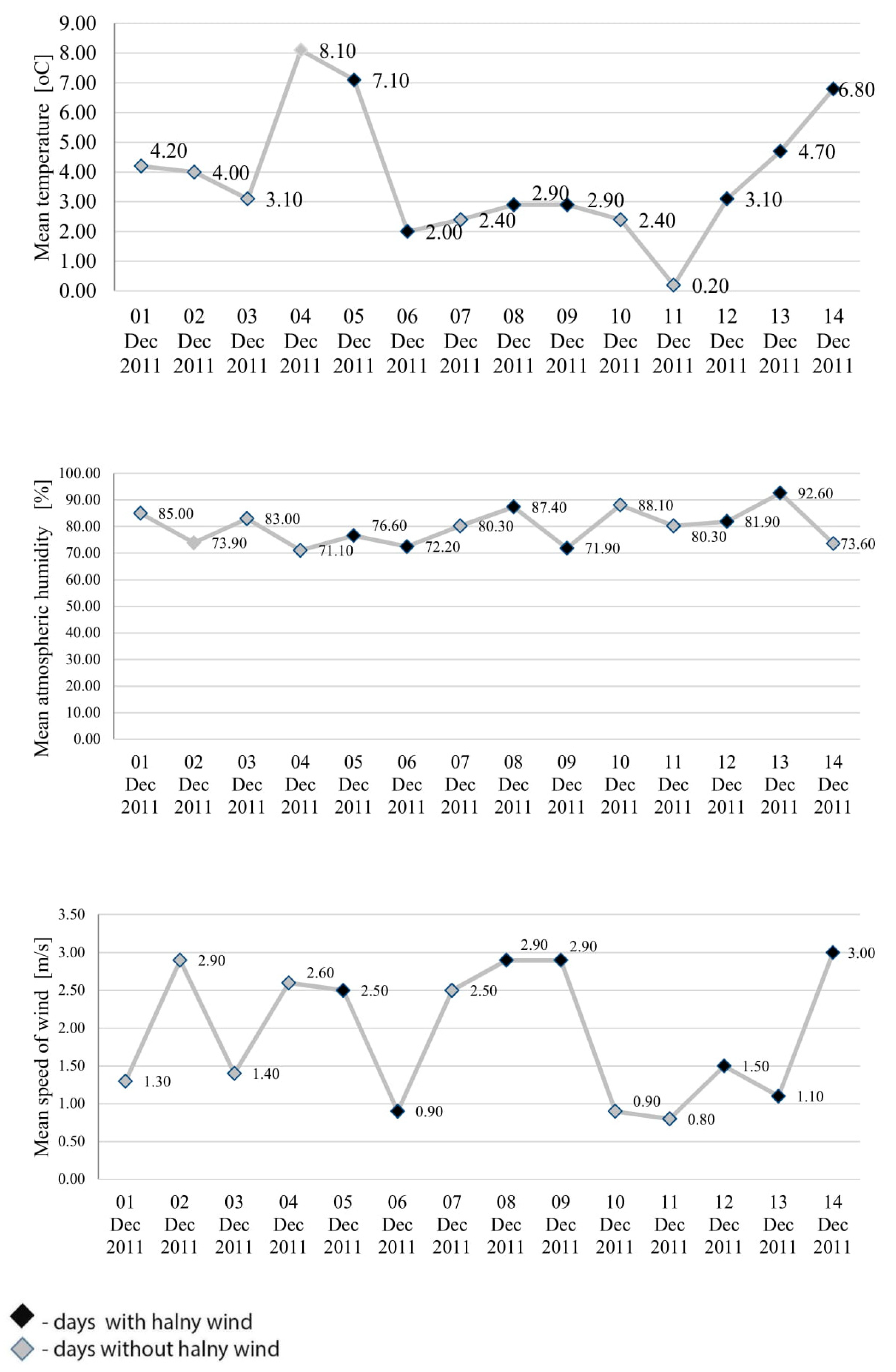
Although the findings covering the relevant period of time do not show significantly higher number of cardiac events on halny days, a greater number of the related hospital admissions was identified in the case of days immediately preceding occurrence of halny. On the days preceding halny wind onset, the incidence of cardiac events was higher than on the remaining days. However, the findings showed no statistically significant correlation between environmental variables and the number of cardiac events observed during this time. Halny wind frequently leads to a considerable increase in the temperature and decrease in humidity on the leeward side of the mountains. The strong abrupt gusts of wind at times reach a speed typical of a hurricane [
4]. Despite the fact that no significant correlations were observed between environmental variables and cardiac events on days immediately preceding halny onset, the graphs in
Figure 1 and
Figure 2 clearly show that on the consecutive days from 1 to 14 December, which included seven days with halny, the mean temperature in most cases was lower on the day preceding halny, compared to the day with halny onset; atmospheric humidity in most cases was lower on the day preceding halny compared to the day with halny onset; similarly speed of wind on the days preceding halny in most cases was higher than or equal to the speed of wind on the day with halny onset. Hence, it appears that the weather conditions observed on the days preceding halny onset may exacerbate the risk of myocardial infarction, a conclusion which is consistent with opinions presented by other researchers. For example, Honda et al. found that increased incidence of acute myocardial infarction corresponds to lower minimum temperature occurring on the second day preceding the onset of wind [
17]. Similarly, Vencloviene et al. showed that prognostic factors for the risk of acute coronary syndromes include such environmental variables as wind speed, daily air temperature, and barometric pressure on the day of the onset and on the two days preceding the ambulance call [
18]. Furthermore, Delyukov et al. and Głuszak et al. suggest that similar synchronicities can be observed during a period ranging from 3 to 24 h prior to an arrival of a weather front [
30,
31]. Analysis of the mean pressure and the number of cardiac events in the consecutive days from 1 to 14 December, including seven days with halny, shows that in most cases pressure was higher on the days preceding halny, compared to the days with halny onset, and the number of cardiac events was higher on the days preceding halny in six cases and only in one case was lower than on the day of halny onset. It can be speculated that the greater number of cardiac incidents identified in our study 24 h before onset of halny wind may be associated with the fact that indeed the wind is only an effect of earlier turbulent changes in atmospheric pressure systems. The factor of key importance here may be the drop in atmospheric pressure, since onset of halny is determined by co-occurrence of high pressure on the southern side and low pressure on the northern side of the Tatra mountains. Other published studies confirm that changes in atmospheric pressure produce adverse effects in the human body, possibly also leading to cardiac incidents [
33,
34,
35,
36]. However, our study did not demonstrate statistically significant correlations between cardiac events and pressure, which may result from the short period of the observations. Therefore, in order to establish a cause-and-effect relationship and some temporal patterns, it is necessary to conduct a more comprehensive study taking into account more data from a larger number of hospitals and related to a longer period of time. By expanding the research to include additional years of data it may be possible to increase these numbers and further determine what role temporal effects play.

 ,
, 



{kind=link}
{kind=link}