Selection of Policy Instruments on Integrated Care in China: Based on Documents Content Analysis

Abstract
1. Introduction
2. Literature Review
2.1. Integrated Care
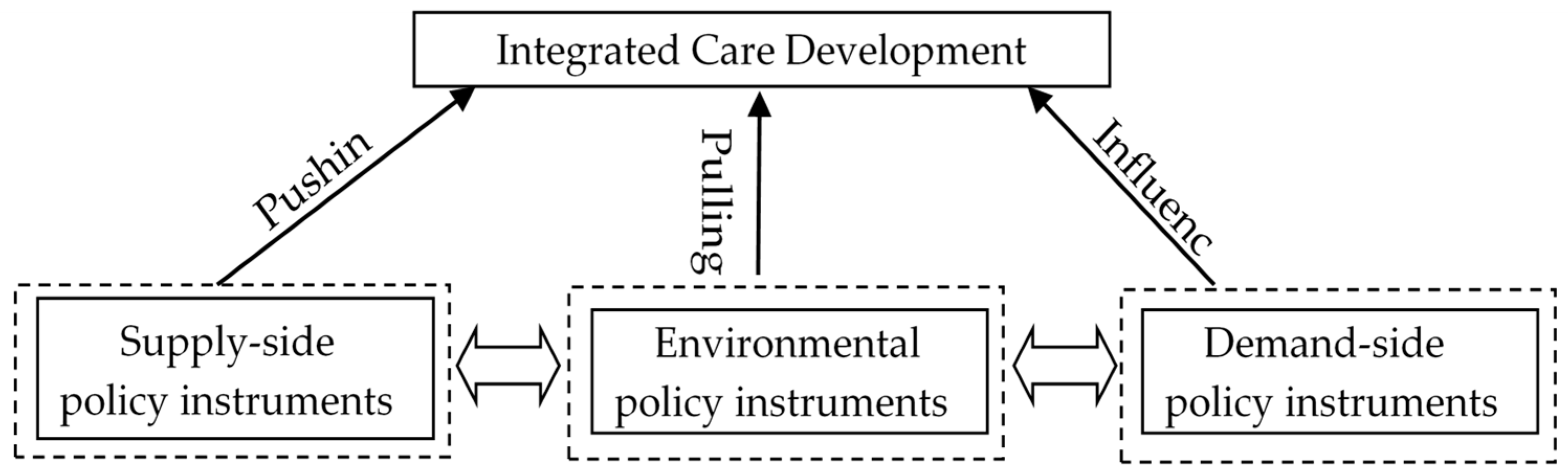
2.2. Policy Instruments
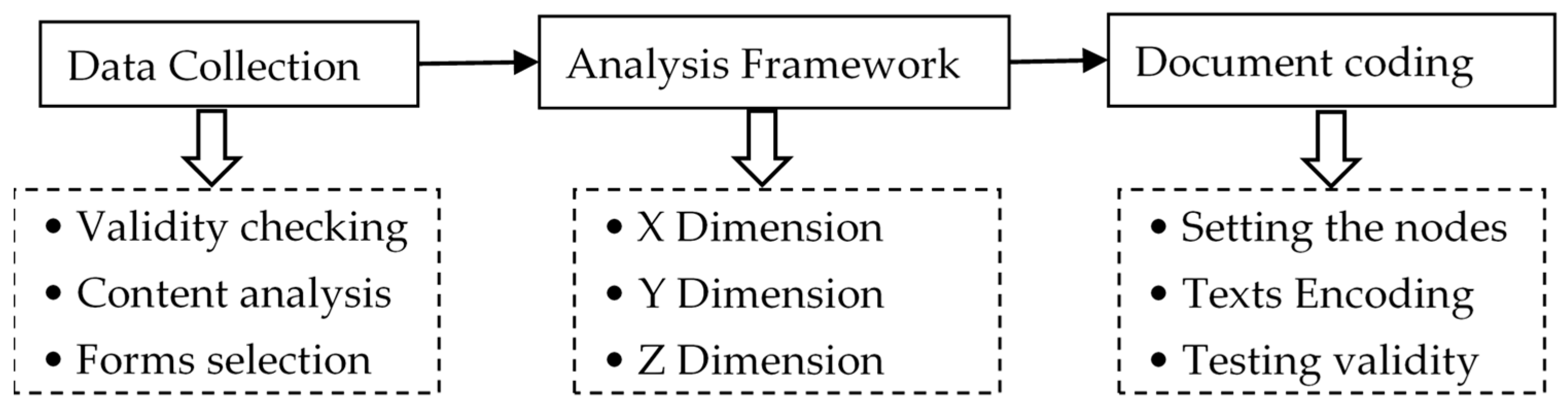
3. Methods
3.1. Data Collection
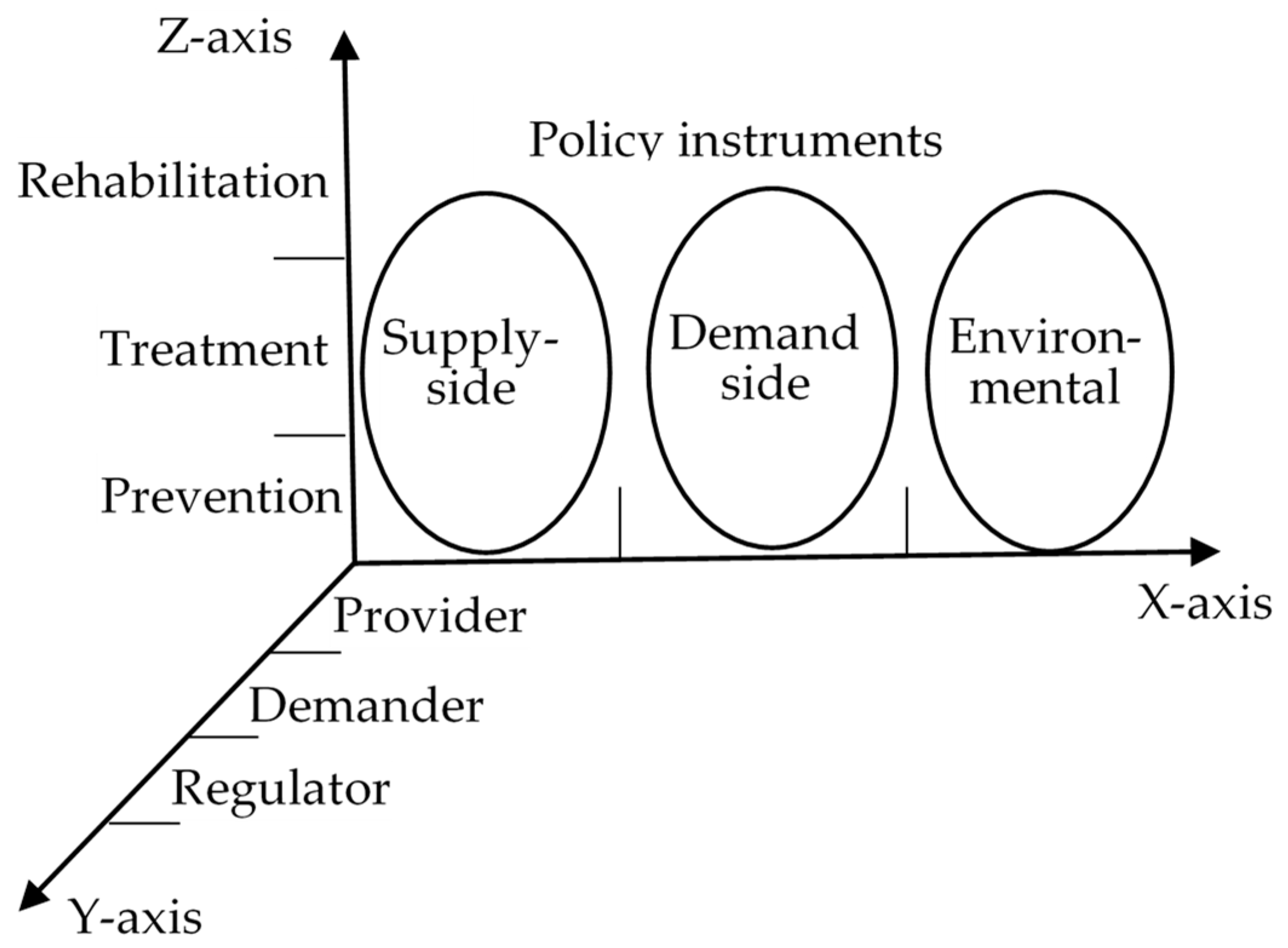
3.2. An Analytical Framework
3.2.1. X Dimension: The Basic Policy Instrument
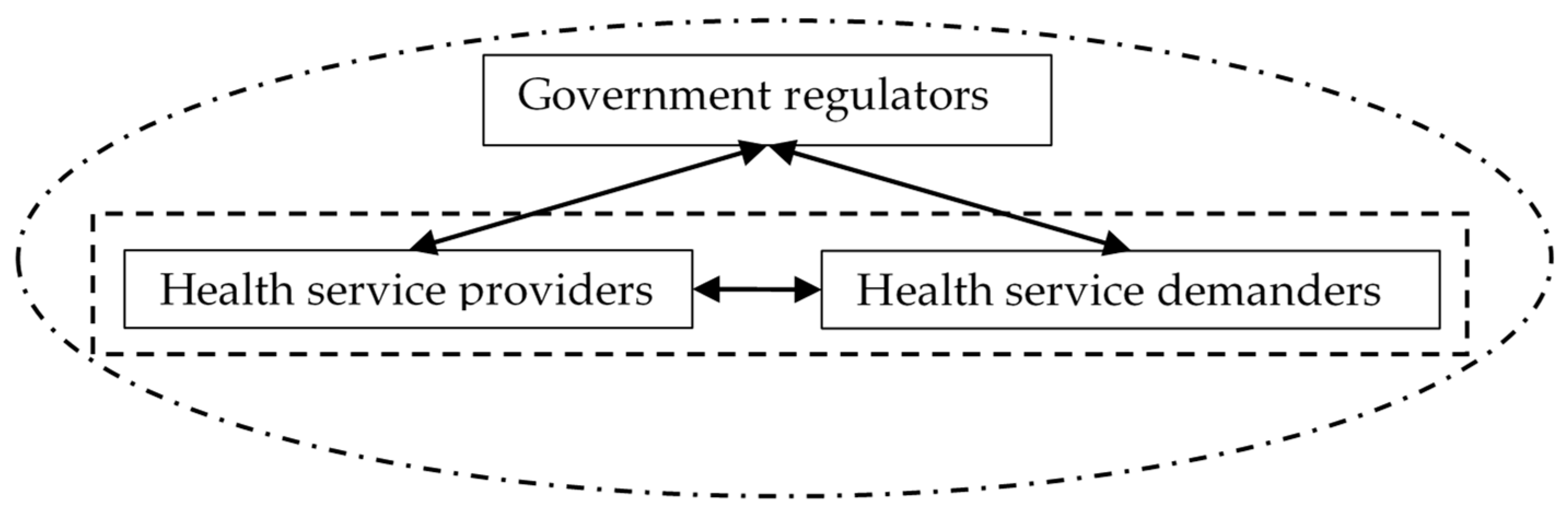
3.2.2. Y Dimension: Stakeholders
3.2.3. Z Dimension: Health Service Supply Chains
3.3. Document Coding Process
4. Results
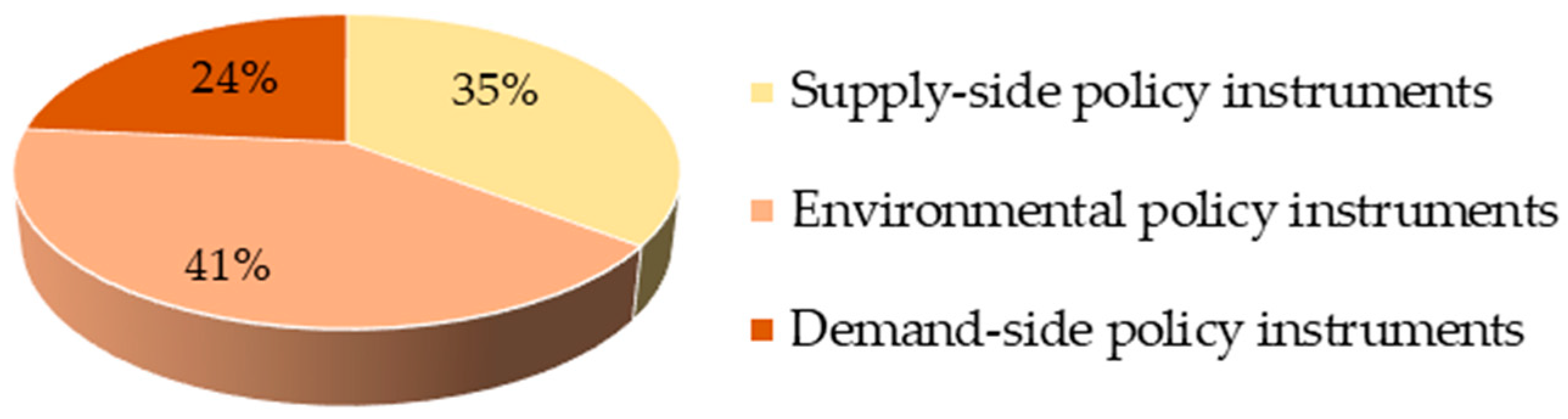
4.1. Overall Analysis of Policy Instruments
4.2. Policy Instruments Used in Stakeholders Dimension
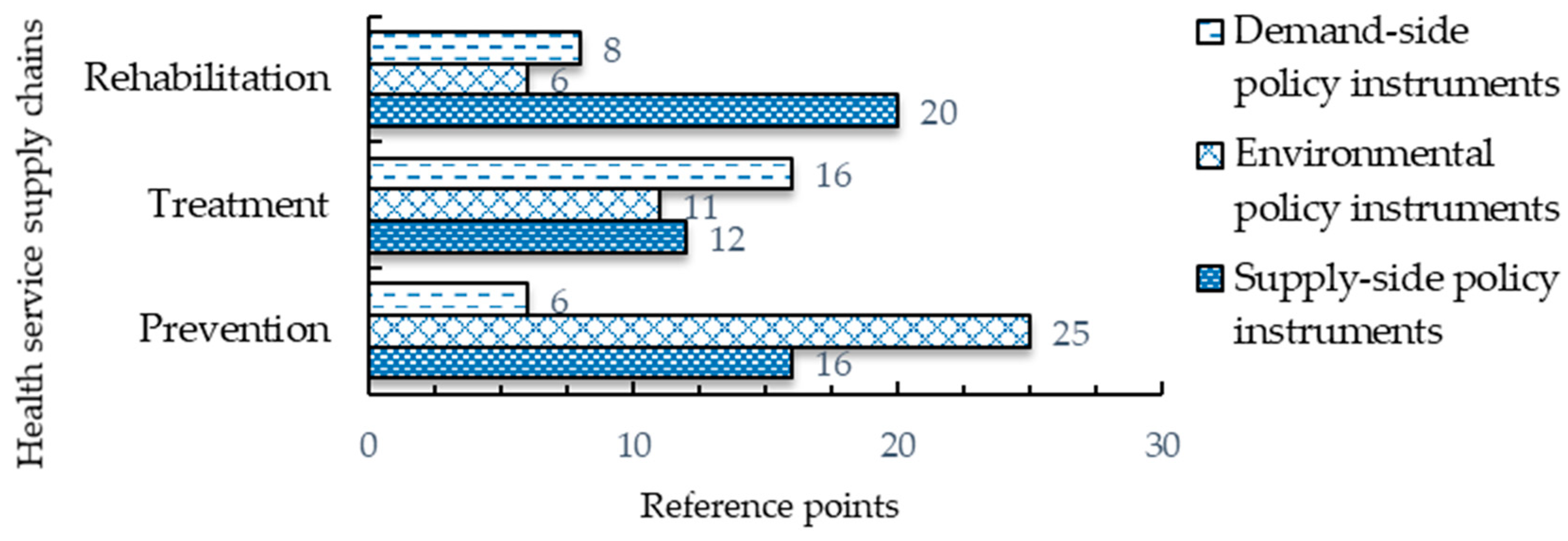
4.3. Policy Instruments Used in Health Service Supply Chains Dimention
5. Discussion
5.1. The Using of Supply-Side Policy Instruments
5.2. The Using of Demand-Side Policy Instruments
5.3. The Use of Environmental Policy Instruments
5.4. The Use of Policy Instruments by Different Stakeholders
5.5. The Using of Policy Instruments in Health Service Supply Chains
5.6. Limitation and Further Research Directions
6. Conclusions and Suggestions
6.1. Conclusions
6.2. Policy Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Woolcott, G.; Keast, R.; Tsasis, P.; Lipina, S.; Chamberlain, D. Reconceptualising person-centered service models as social ecology networks in supporting integrated care. Int. J. Integr. Care 2019, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Shortell, S.M.; Gillies, R.R.; Anderson, D.A.; Mitchell, J.B.; Morgan, K.L. Creating organized delivery systems: The barriers and facilitators. Hosp. Health Serv. Adm. 1993, 38, 447–466. [Google Scholar] [PubMed]
- Shortell, S.M.; Gillies, R.R.; Anderson, D.A. The new world of managed care: Creating organized delivery systems. Health Aff. (Millwood) 1994, 13, 46–64. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.L.; Chiang, C.Y. The effects of strategic hospital alliances on hospital efficiency. Serv. Ind. J. 2013, 33, 624–635. [Google Scholar] [CrossRef]
- Lomi, A.; Mascia, D.; Vu, D.Q.; Pallotti, F.; Conaldi, G.; Iwashyna, T.J. Quality of care and interhospital collaboration: A study of patient transfers in Italy. Med. Care 2014, 52, 407–414. [Google Scholar] [CrossRef]
- Saddique, A.A. Integrated delivery systems (IDSs) as a means of reducing costs and improving healthcare delivery. J. Health Commun. 2017, 3, 1–4. [Google Scholar] [CrossRef]
- Wu, X.B.; Li, S.H.; Xu, N.; Wu, D.; Zhang, X.L. Establishing a balanced scorecard measurement system for integrated care organizations in China. Int. J. Health Plan. Manag. 2019, 34, 672–692. [Google Scholar] [CrossRef]
- Mur-Veeman, I.; Van Raak, A.; Paulus, A. Comparing integrated care policy in Europe: Does policy matter? Health Policy 2008, 85, 172–183. [Google Scholar] [CrossRef]
- Schussele Filliettaz, S.; Berchtold, P.; Kohler, D.; Peytremann-Bridevaux, I. Integrated care in Switzerland: Results from the first nationwide survey. Health Policy 2018, 122, 568–576. [Google Scholar] [CrossRef]
- Sun, X.; Tang, W.; Ye, T.; Zhang, Y.; Wen, B.; Zhang, L. Integrated care: A comprehensive bibliometric analysis and literature review. Int. J. Integr. Care 2014, 14, e017. [Google Scholar] [CrossRef]
- Ma, J.; Lu, M.; Quan, H. From a national, centrally planned health system to a system based on the market: Lessons from China. Health Aff. (Millwood) 2008, 27, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Stange, K.C. The paradox of the parts and the whole in understanding and improving general practice. Int. J. Qual. Health Care 2002, 14, 267–268. [Google Scholar] [CrossRef] [PubMed][Green Version]
- National Burean of Statistics of China. China Statistical Yearbook 2019; China Statistics Press: Beijing, China, 2019; p. 33. [Google Scholar]
- Montenegro, H.; Holder, R.; Ramagem, C.; Urrutia, S.; Fabrega, R.; Tasca, R.; Alfaro, G.; Salgado, O.; Gomes, M.A. Combating health care fragmentation through integrated health service delivery networks in the Americas: Lessons learned. J. Integr. Care 2011, 19, 5–16. [Google Scholar] [CrossRef]
- Huang, C.; Yang, C.; Su, J. Policy change analysis based on “policy target–policy instrument” patterns: A case study of China’s nuclear energy policy. Scientometrics 2018, 117, 1081–1114. [Google Scholar] [CrossRef]
- Kodner, D.L.; Spreeuwenberg, C. Integrated care: Meaning, logic, applications, and implications—A discussion paper. Int. J. Integr. Care 2002, 2, e12. [Google Scholar] [CrossRef]
- Gillies, R.R.; Shortell, S.M.; Anderson, D.A.; Mitchell, J.B.; Morgan, K.L. Conceptualizing and measuring integration: Findings from the Health Systems Integration study. Hosp. Health Serv. Adm. 1993, 38, 467–477. [Google Scholar]
- Sheiman, I.; Shevski, V. Evaluation of health care delivery integration: The case of the Russian Federation. Health Policy 2014, 115, 128–137. [Google Scholar] [CrossRef]
- Ouwens, M.; Wollersheim, H.; Hermens, R.; Hulscher, M.; Grol, R. Integrated care programmes for chronically ill patients: A review of systematic reviews. Int. J. Qual. Health Care 2005, 17, 141–146. [Google Scholar] [CrossRef]
- Glendinning, C. Breaking down barriers: Integrating health and care services for older people in England. Health Policy 2003, 65, 139–151. [Google Scholar] [CrossRef]
- Kodner, D.L. All together now: A conceptual exploration of integrated care. Healthc. Q. 2009, 13, 6–15. [Google Scholar] [CrossRef]
- Nurjono, M.; Valentijn, P.P.; Bautista, M.A.C.; Wei, L.Y.; Vrijhoef, H.J.M. A prospective validation study of a rainbow model of integrated care measurement tool in Singapore. Int. J. Integr. Care 2016, 16. [Google Scholar] [CrossRef]
- Devers, K.J.; Shortell, S.M.; Gillies, R.R.; Anderson, D.A.; Mitchell, J.B.; Erickson, K.L. Implementing organized delivery systems: An integration scorecard. Health Care Manag. Rev. 1994, 19, 7–20. [Google Scholar] [CrossRef]
- Burns, L.R. Polarity management: The key challenge for integrated health systems. J. Healthc. Manag. 1999, 44, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Maruthappu, M.; Hasan, A.; Zeltner, T. Enablers and barriers in implementing integrated care. Health Syst. Reform 2015, 1, 250–256. [Google Scholar] [CrossRef]
- Ovretveit, J. Digital technologies supporting person-centered integrated care—A perspective. Int. J. Integr. Care 2017, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Howlett, M. Policy instruments, policy styles, and policy implementation—National approaches to theories of instrument choice. Policy Stud. J. 1991, 19, 1–21. [Google Scholar] [CrossRef]
- Bemelmans-Videc, M.L.; Rist, R.C.; Vedung, E.O. (Eds.) Carrots, Sticks, and Sermons: Policy Instruments and Their Evaluation; Transaction Publishers: New Brunswick, NJ, USA; London, UK, 1998; pp. 21–77. [Google Scholar]
- Taylor, C.M.; Gallagher, E.A.; Pollard, S.J.T.; Rocks, S.A.; Smith, H.M.; Leinster, P.; Angus, A.J. Environmental regulation in transition: Policy officials’ views of regulatory instruments and their mapping to environmental risks. Sci. Total Environ. 2019, 646, 811–820. [Google Scholar] [CrossRef]
- Feiock, R.C.; Tavares, A.F.; Lubell, M. Policy instrument choices for growth management and land use regulation. Policy Stud. J. 2008, 36, 461–480. [Google Scholar] [CrossRef]
- Weiss, J.A.; Tschirhart, M. Public information campaigns as policy instruments. J. Policy Anal. Manag. 1994, 13, 82–119. [Google Scholar] [CrossRef]
- Georghiou, L.; Edler, J.; Uyarra, E.; Yeow, J. Policy instruments for public procurement of innovation: Choice, design and assessment. Technol. Forecast. Soc. Chang. 2014, 86, 1–12. [Google Scholar] [CrossRef]
- Hemels, S. Tax incentives as a creative industries policy instrument. In Tax Incentives for the Creative Industries; Springer: Singapore, 2017; pp. 33–64. [Google Scholar] [CrossRef]
- Azevedo, T.C.; Portella, A.A. Green tax incentives as an instrument to support urban policy: A study on the “IPTU VERDE” in Brazilian municipalities. Holos 2019, 1, 1–18. [Google Scholar] [CrossRef]
- Chen, Z. Introduction to Government Tools; Peking University Press: Beijing, China, 2009; pp. 23–34. [Google Scholar]
- Flanagan, K.; Uyarra, E.; Laranja, M. Reconceptualising the ‘policy mix’ for innovation. Res. Policy 2011, 40, 702–713. [Google Scholar] [CrossRef]
- Cai, Y.; Li, L.; Elahi, E.; Qiu, Y. Selection of policies on typhoon and rainstorm disasters in China: A content analysis perspective. Sustainability 2018, 10, 387. [Google Scholar] [CrossRef]
- Salamon, L.M. The Tools of Government: A Guide to the New Governance; Oxford University Press: New York, NY, USA, 2002; pp. 1–47. [Google Scholar]
- Chen, Z. Policy Science; China Renmin University Press: Beijing, China, 2004; pp. 380–420. [Google Scholar]
- Howlett, M.; Ramesh, M. Studying Public Policy: Policy Cycles and Policy Subsystems; Oxford University Press: Toronto, ON, Canada, 1995; pp. 239–241. [Google Scholar]
- Rothwell, R.; Zegveld, W. Reindustrialization and Technology; M. E. Sharpe, Inc.: New York, NY, USA, 1985; pp. 282–284. [Google Scholar]
- Zhang, H.; Deng, T.; Wang, M.; Chen, X. Content analysis of talent policy on promoting sustainable development of talent: Taking Sichuan Province as an example. Sustainability 2019, 11, 2508. [Google Scholar] [CrossRef]
- Cardno, C. Policy document analysis: A practical educational leadership tool and a qualitative research method. Educ. Adm. Theory Pract. 2019, 24. [Google Scholar] [CrossRef]
- Bowen, G.A. Document analysis as a qualitative research method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef]
- Takach, M.; Townley, C.; Yalowich, R.; Kinsler, S. Making multipayer reform work: What can be learned from medical home initiatives. Health Aff. (Millwood) 2015, 34, 662–672. [Google Scholar] [CrossRef]
- Rajkumar, R.; Conway, P.H.; Tavenner, M. CMS—Engaging multiple payers in payment reform. JAMA 2014, 311, 1967–1968. [Google Scholar] [CrossRef]
- Wang, Q.; Hu, J.; Dai, T. Analysis on the impetus and resistance to tiered health care system: Based on the stakeholders theory. Chin. J. Health Policy 2016, 9, 9–15. [Google Scholar]
- Ramesh, M.; Wu, X.; He, A.J. Health governance and healthcare reforms in China. Health Policy Plan. 2014, 29, 663–672. [Google Scholar] [CrossRef]
- Wendimagegn, N.F.; Bezuidenhout, M. The integrated health service model: The approach to restrain the vicious cycle to chronic diseases. BMC Health Serv. Res. 2019, 19, 347. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; Singh, S.R.; Srivastava, A.; Chuah, F.L.H.; Koh, G.C.H.; Seng, C.K.; Perel, P.; Legido-Quigley, H. Community involvement in the development and implementation of chronic condition programmes across the continuum of care in high- and upper-middle income countries: A systematic review. Health Policy 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Lang, P.J.; Sugimoto, D.; Micheli, L.J. Prevention, treatment, and rehabilitation of anterior cruciate ligament injuries in children. Open Access J. Sports Med. 2017, 8, 133–141. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Johnstone, R.; Quinlan, M.; Walters, D. Regulating supply chains to improve health and safety. Ind. Law J. 2007, 36, 163–187. [Google Scholar] [CrossRef]
- Brennan, C.D. Integrating the healthcare supply chain. Healthc. Financ. Manag. 1998, 52, 31–34. [Google Scholar]
- Foley, G.; Timonen, V. Using grounded theory method to capture and analyze health care experiences. Health Serv. Res. 2015, 50, 1195–1210. [Google Scholar] [CrossRef]
- Chute, C.; French, T. Introducing Care 4.0: An integrated care paradigm built on industry 4.0 capabilities. Int. J. Environ. Res. Public Health 2019, 16, 2247. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Z.; Qian, D.; Ni, J. Effects of changes in health insurance reimbursement level on outpatient service utilization of rural diabetics: Evidence from Jiangsu Province, China. BMC Health Serv. Res. 2014, 14, 185. [Google Scholar] [CrossRef]
- Homer, J.B.; Hirsch, G.B. System dynamics modeling for public health: Background and opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef]
- Peters, B.G.; Van Nispen, F.K. (Eds.) Public Policy Instruments: Evaluating the Tools of Public Administration; Edward Elgar Publishing: Cheltenham, UK, 1998; pp. 132–139. [Google Scholar]
- Borrás, S.; Edquist, C. The choice of innovation policy instruments. Forecast. Soc. Chang. 2013, 80, 1513–1522. [Google Scholar] [CrossRef]
- Wang, X.; Sun, X.; Gong, F.; Huang, Y.; Chen, L.; Zhang, Y.; Birch, S. The Luohu model: A template for integrated urban healthcare systems in China. Int. J. Integr. Care 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Phillips, W.R.; Haynes, D.G. The domain of family practice: Scope, pole, and function. Fam. Med. 2001, 33, 273–277. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Policy type | Instrument name | Description |
|---|---|---|
| Supply-side policy instruments | Talent support (TS) | Formulating long-term talent development policies for promoting integrated care development, which include increasing the number of primary care practitioners and improving the skills of medical staff. |
| Technology information support (TIS) | Providing public scientific and technological support and information services for integrated care development. | |
| Capital investment (CI) | The government directly provides financial resources for integrated care development. | |
| Infrastructure construction (IC) | Updating basic public health infrastructures and expanding health service facilities. | |
| Demand-side policy instruments | Family doctor engagement (FDE) | Providing basic healthcare to the whole population, helping manage health and medical costs. |
| Medicare reimbursement (MR) | Expanding the insurance coverage and widening the gap of reimbursement rates among different institutions. | |
| Government procurement (GP) | Priority to purchase basic public health services and centralized drug purchasing with public funds is provided by public institutions and organizations. | |
| Social sector support (SSS) | Encouraging qualified private actors and social organizations to provide or serve the health services. | |
| Environmental policy instruments | Target planning (TP) | A component of the integrated care policies by setting a timetable and determining a plan to achieve the policy goal. |
| Performance appraisal and rewards (PAR) | Evaluating achievements and rewarding for high performance. | |
| Regulation control (RC) | The government enacts a series of laws and regulations to restrict or maintain health services market behavior and to create a favorable environment for people. | |
| Policy advocacy (PA) | The government publicize integrated care policies and improve the cognition of the masses through various channels and in various ways. |
| Node | Sub-Node/Instrument Name | Coded References | Percentage |
|---|---|---|---|
| Supply-side policy instruments | Talent support (TS) | 36 | 10.6% |
| Technology information support (TIS) | 38 | 11.2% | |
| Capital investment (CI) | 29 | 8.6% | |
| Infrastructure construction (IC) | 17 | 5.0% | |
| Demand-side policy instruments | Family doctor engagement (FDE) | 13 | 3.8% |
| Medicare reimbursement (MR) | 27 | 8.0% | |
| Government procurement (GP) | 16 | 4.7% | |
| Social sector support (SSS) | 24 | 7.1% | |
| Environmental policy instruments | Target planning (TP) | 22 | 6.5% |
| Performance appraisal and rewards (PAR) | 38 | 11.2% | |
| Regulation control (RC) | 48 | 14.2% | |
| Policy advocacy (PA) | 31 | 9.1% |
| Stakeholders | Policy Instruments | Coded References | Total Coded References |
|---|---|---|---|
| Demanders | Supply-side policy instruments | 39 | 64 |
| Environmental policy instruments | 45 | ||
| Demand-side policy instruments | 14 | ||
| Providers | Supply-side policy instruments | 39 | 98 |
| Environmental policy instruments | 45 | ||
| Demand-side policy instruments | 14 | ||
| Regulators | Supply-side policy instruments | 15 | 67 |
| Environmental policy instruments | 37 | ||
| Demand-side policy instruments | 15 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yue, X.; Mu, K.; Liu, L. Selection of Policy Instruments on Integrated Care in China: Based on Documents Content Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2327. https://doi.org/10.3390/ijerph17072327
Yue X, Mu K, Liu L. Selection of Policy Instruments on Integrated Care in China: Based on Documents Content Analysis. International Journal of Environmental Research and Public Health. 2020; 17(7):2327. https://doi.org/10.3390/ijerph17072327
Chicago/Turabian StyleYue, Xin, Kaining Mu, and Lihang Liu. 2020. "Selection of Policy Instruments on Integrated Care in China: Based on Documents Content Analysis" International Journal of Environmental Research and Public Health 17, no. 7: 2327. https://doi.org/10.3390/ijerph17072327
APA StyleYue, X., Mu, K., & Liu, L. (2020). Selection of Policy Instruments on Integrated Care in China: Based on Documents Content Analysis. International Journal of Environmental Research and Public Health, 17(7), 2327. https://doi.org/10.3390/ijerph17072327