The Associations between Individual Factors, eHealth Literacy, and Health Behaviors among College Students


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Statistics and Gender Differences in eHealth Literacy Dietary, Dietary Behaviors, Exercise Habits, Subjective Health Status, Perception of the Importance of Health and Supplements Use
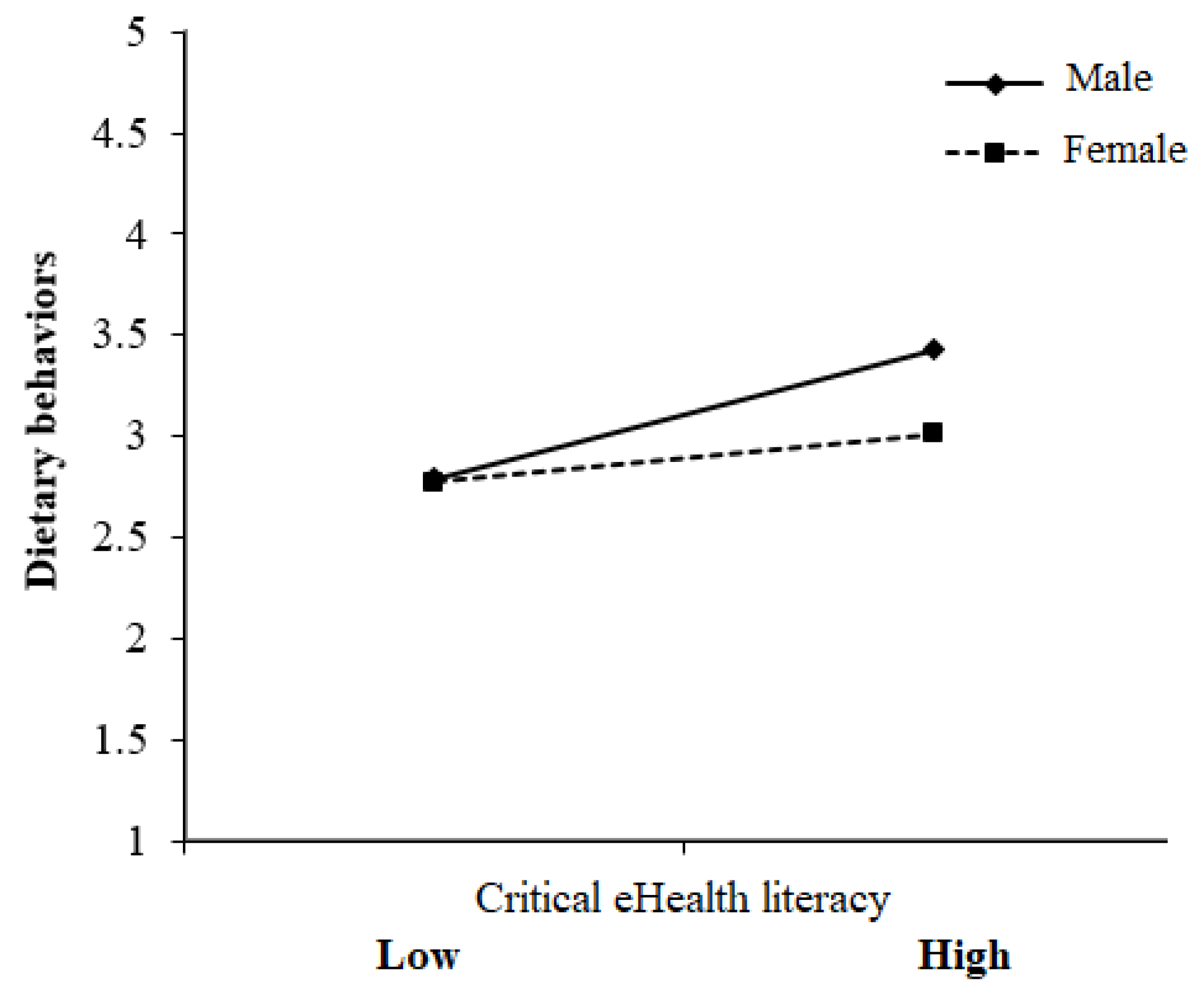
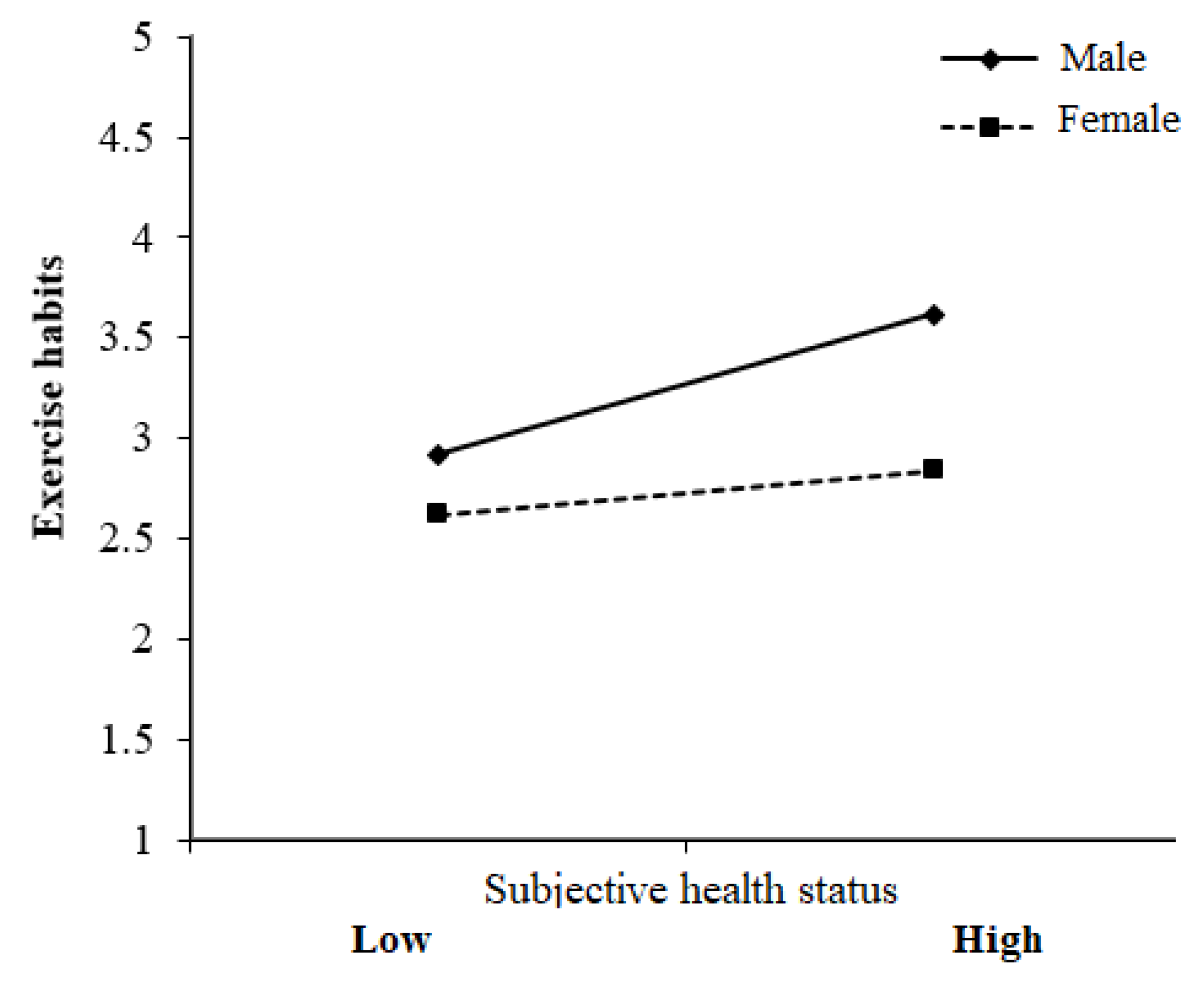
3.2. Regression Analysis of the Predictive Power of the Research Variables on Dietary Behavior and Exercise Habits
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Instruments Used in This Study
- I.
- eHealth Literacy Scale (Five-Point Likert-Type)
- 1.
- I cannot understand the symbols (such as BMI, Body Mass Index) and wording about health information.
- 2.
- I find the online health information difficult to understand.
- 3.
- I find the mathematical formulas provided in online health information difficult to calculate. (e.g., the algorithm of calorie consumption, BMI).
- 4.
- I can locate health information efficiently through search engines.
- 5.
- I pay attention to and obtain new knowledge about online health information.
- 6.
- I know how to get what I need from online health information.
- 7.
- I understand the online health information I have obtained.
- 8.
- I will think about whether the online health information applies to my situation.
- 9.
- I try to find different sources to verify the credibility of health information.
- 10.
- I evaluate the validity and reliability of online health information.
- 11.
- I will browse various discussions and make a decision or action that is good for health.
- 12.
- When I have questions or doubts about online health information, I use other channels to verify the information.
- II.
- Dietary Behaviors (Five-Point Likert-Type)
- 1.
- More than two bowls per day of fruit.
- 2.
- More than three bowls per day of vegetables.
- 3.
- More than five bowls per day of meats and protein.
- 4.
- More than one bowl per day of unrefined whole grains.
- 5.
- More than 1.5 glasses (360 mL) per day of milk.
- III.
- Exercise Habits
- 1.
- Motion frequency of a week(1) none (2) one day (3) two days (4) three days (5) four days (6) five or more days
- 2.
- Exercise duration each time(1) 0−29 min (2) 30−60 min (3) 61−90 min (4) 91−120 min (5) 121 or more min
- 3.
- Average intensity each time(1) 10% (2) 20% (3) 30% (4) 40% (5) 50%(6) 60% (7) 70% (8) 80% (9) 90% (10) 100%
References
- Ruggeri, D.; Seguin, R.A. Impact of point of sale nutritional information and dietary and exercise habits of college students in Missouri. J. Food Nutr. Res. 2016, 4, 195–200. [Google Scholar] [CrossRef]
- Wong, C.A.; Greeno, J.; Perrin, E.; Peterson, E.; Chung, R.; Skinner, A. Young and not so invincible: Health behaviours and patient-reported health outcomes among adolescents and young adults. J. Adolesc. Health 2018, 62, S132. [Google Scholar] [CrossRef]
- Stanziano, D.C.; Butler-Ajibade, P. Differences in health-related behaviours and body mass index risk categories in African American women in college. J. Natl. Med. Assoc. 2011, 103, 4–8. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.; Carey, K.B.; Carey, M.P. Health behaviour and college students: Does Greek affiliation matter? J. Behav. Med. 2008, 31, 61–70. [Google Scholar] [CrossRef]
- Luo, Y.F.; Yang, S.C.; Chiang, C.H.; Lu, C.M. Development and validation of a food literacy self-report inventory and investigation of the relationships between food literacy and dietary behavior among college students. Taiwan J. Public Health 2018, 37, 407–419. [Google Scholar] [CrossRef]
- Yang, S.C.; Luo, Y.F.; Chiang, C.H. Electronic health literacy and dietary behaviors in Taiwanese college students: Cross-sectional study. J. Med. Internet Res. 2019, 21, e13140. [Google Scholar] [CrossRef]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Weight changes, exercise, and dietary patterns during freshman and sophomore years of college. J. Am. Coll. Health 2005, 53, 245–251. [Google Scholar] [CrossRef]
- Al-Gelban, K.S. Dietary habits and exercise practices among the students of a Saudi teachers’ training college. Saudi Med. J. 2008, 29, 754. [Google Scholar]
- Cutilli, C.C.; Bennett, I.M. Understanding the health literacy of America results of the national assessment of adult literacy. Orthop. Nurs. 2009, 28, 27. [Google Scholar] [CrossRef]
- Karnoe, A.; Kayser, L. How is eHealth literacy measured and what do the measurements tell us? A systematic review. Knowl. Manag. E Learn. Int. J. 2015, 7, 576–600. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. eHealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef]
- Mitsutake, S.; Shibata, A.; Ishii, K.; Oka, K. Associations of eHealth literacy with health behavior among adult internet users. J. Med. Internet Res. 2016, 18, e192. [Google Scholar] [CrossRef]
- Hsu, W.C.; Chiang, C.H.; Yang, S.C. The effect of individual factors on health behaviours among college students: The mediating effects of eHealth literacy. J. Med. Internet Res. 2014, 16, e287. [Google Scholar] [CrossRef]
- Chiang, C.H.; Yang, S.C.; Hsu, W.C. Development and validation of the e-health literacy scale and investigation of the relationships between e-health literacy and healthy behavior among undergraduate students in Taiwan. Formosa J. Ment. Health 2015, 28, 389–420. [Google Scholar]
- Yang, S.H.; Lou, Y.F.; Chiang, C.H. The associations among individual factors, eHealth literacy and health-promoting lifestyles among college students. J. Med. Internet Res. 2017, 19, e15. [Google Scholar] [CrossRef]
- Neter, E.; Brainin, E. Association between health literacy, eHealth literacy, and health outcomes among patients with long-term conditions. Eur. Psychol. 2019, 24, 68–81. [Google Scholar] [CrossRef]
- Peltzer, K. Health behaviour among black and white South Africans. J. R. Soc. Promot. Health 2002, 122, 187–193. [Google Scholar] [CrossRef]
- Greene, G.W.; Schembre, S.M.; White, A.A.; Hoerr, S.L.; Lohse, B.; Shoff, S.; Horacek, T.; Riebe, D.; Patterson, J.; Phillips, B.W.; et al. Identifying clusters of college students at elevated health risk based on eating and exercise behaviors and psychosocial determinants of body weight. J. Am. Diet. Assoc. 2011, 111, 394–400. [Google Scholar] [CrossRef]
- Whatnall, M.C.; Patterson, A.J.; Chiu, S.; Oldmeadow, C.; Hutchesson, M.J. Determinants of eating behaviours in Australian university students: A cross-sectional analysis. Nutr. Diet. 2019, 3. [Google Scholar] [CrossRef]
- Mello Rodrigues, V.; Bray, J.; Fernandes, A.C.; Luci Bernardo, G.; Hartwell, H.; Secchi Martinelli, S.; Lazzarin Uggioni, P.; Barletto Cavalli, S.; Proença, R.P.D.C. Vegetable consumption and factors associated with increased intake among college students: A scoping review of the last 10 years. Nutrients 2019, 11, 1634. [Google Scholar] [CrossRef]
- Beşer, A.; Bahar, Z.; Büyükkaya, D. Health promoting behaviors and factors related to lifestyle among Turkish workers and occupational health nurses’ responsibilities in their health promoting activities. Ind. Health 2007, 45, 151–159. [Google Scholar] [CrossRef]
- Dyremyhr, A.E.; Diaz, E.; Meland, E. How adolescent subjective health and satisfaction with weight and body shape are related to participation in sports. J. Environ. Public Health 2014, 2014, 851932. [Google Scholar] [CrossRef]
- Kwak, H.K.; Lee, M.Y.; Kim, M.J. Comparisons of body image perception, health related lifestyle and dietary behavior based on the self-rated health of university students in Seoul. Korean J. Commun. Nutr. 2011, 16, 672–682. [Google Scholar] [CrossRef]
- Bishwajit, G.; Tang, S.; Yaya, S.; He, Z.; Feng, Z. Lifestyle behaviors, subjective health, and quality of life among Chinese men living with type 2 diabetes. Am. J. Men Health 2017, 11, 357–364. [Google Scholar] [CrossRef]
- Chiou, W.B.; Yang, C.C.; Wan, C.S. Ironic effects of dietary supplementation: Illusory invulnerability created by taking dietary supplements licenses health-risk behaviors. Psychol. Sci. 2011, 22, 1081–1086. [Google Scholar] [CrossRef]
- van der Horst, K.; Siegrist, M. Vitamin and mineral supplement users. Do they have healthy or unhealthy dietary behaviours? Appetite 2011, 57, 758–764. [Google Scholar] [CrossRef]
- Harrison, R.A.; Holt, D.; Pattison, D.J.; Elton, P.J. Are those in need taking dietary supplements? A survey of 21923 adults. Br. J. Nutr. 2004, 91, 617–623. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef]
- Bora, J.K.; Saikia, N. Gender differentials in self-rated health and self-reported disability among adults in India. PLoS ONE 2015, 10, e0141953. [Google Scholar] [CrossRef]
- El-Ansari, W.; Stock, C. Gender differences in self-rated health among university students in England, Wales and Northern Ireland: Do confounding variables matter? Glob. J. Health Sci. 2016, 8, 168–177. [Google Scholar] [CrossRef]
- Jerdén, L.; Burell, G.; Stenlund, H.; Weinehall, L.; Bergström, E. Gender differences and predictors of self-rated health development among Swedish adolescents. J. Adolesc. Health 2011, 48, 143–150. [Google Scholar] [CrossRef]
- de Jong, N.; Ocké, M.C.; Branderhorst, H.A.; Friele, R. Demographic and lifestyle characteristics of functional food consumers and dietary supplement users. Br. J. Nutr. 2003, 89, 273–281. [Google Scholar] [CrossRef]
- Baron-Epel, O.; Balin, L.; Daniely, Z.; Eidelman, S. Validation of a Hebrew health literacy test. Patient Educ. Couns. 2007, 67, 235–239. [Google Scholar] [CrossRef]
- Javadzade, S.H.; Sharifirad, G.; Radjati, F.; Mostafavi, F.; Reisi, M.; Hasanzade, A. Relationship between health literacy, health status, and healthy behaviors among older adults in Isfahan, Iran. J. Educ. Health Promot. 2012, 1, 31. [Google Scholar] [CrossRef]
- New Nutritional Guidelines. Available online: https://www.hpa.gov.tw/Pages/EBook.aspx?nodeid=1208 (accessed on 14 January 2019).
- Peng, H.Y. The study of recreational sport participation and learning achievement of physical education of Taipei young people. TPEC Press 2008, 16, 193–205. [Google Scholar]
- Yu, C.T.; Chao, C.M.; Cheng, B.W. Effects of personality traits on the degree of exercise participation, physical self-description and social physique anxiety of hospital employees. J. Appl. Sci. 2014, 14, 3555–3562. [Google Scholar]
- Chen, Y.C.; Ting, C.Y.; Tseng, M.S.; Pan, W.H. Pattern and purpose of dietary supplements use in Taiwan. J. Chin. Nutr. Soc. 2001, 26, 193–202. [Google Scholar]
- Chinn, D.; McCarthy, C. All Aspects of Health Literacy Scale (AAHLS): Developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ. Couns. 2013, 90, 247–253. [Google Scholar] [CrossRef]
- Waldrop-Valverde, D.; Jones, D.L.; Jayaweera, D.; Gonzalez, P.; Romero, J.; Ownby, R.L. Gender differences in medication management capacity in HIV infection: The role of health literacy and numeracy. AIDS Behav. 2009, 13, 13–46. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Tehrani Banihashemi, A.; Asgharifard, H.; Bahramian, M.; Baradaran, H.R.; Khamseh, M.E. Health literacy and its influencing factors in Iranian diabetic patients. Med. J. Islam. Repub. Iran 2015, 29, 230. [Google Scholar]
- Cai, D.L.; Geng, S.S. Security of fat-soluble vitamins. Amino Acids Biot. Resour. 2006, 28, 67–71. [Google Scholar]
- Fu, A.H.; Jien, J.J. Correlation among college students' body shape, dietary habits, and dietary behaviors. Nutr. Sci. J. 2008, 33, 55–65. [Google Scholar]
- Wansink, B.; Cheney, M.M.; Chan, N. Exploring comfort food preferences across age and gender. Physiol. Behav. 2003, 79, 739–747. [Google Scholar] [CrossRef]
- Grogan, S.C.; Bell, R.; Conner, M. Eating sweet snacks: Gender differences in attitudes and behavior. Appetite 1997, 28, 19–31. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory: An agentic perspective. Ann. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef]
- Joseph, R.P.; Ainsworth, B.E.; Keller, C.; Dodgson, J.E. Barriers to physical activity among African American women: An integrative review of the literature. Women Health 2015, 55, 679–699. [Google Scholar] [CrossRef]
- Osuji, T.; Lovegreen, S.; Elliott, M.; Brownson, R.C. Barriers to physical activity among women in the rural Midwest. Women Health 2006, 44, 41–55. [Google Scholar] [CrossRef]
- Sykes, S.; Wills, J. Challenges and opportunities in building critical health literacy. Glob. Health Promot. 2015, 25, 48–56. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Whole population | Male | Female | t | p | d | ||
| M (SD) | |||||||
| eHealth literacy (three levels) | |||||||
| functional | 3.94 (0.77) | 4.04 (0.77) | 3.81 (0.76) | 3.84 | <0.001 | 0.30 | |
| interactive | 3.66 (0.74) | 3.65 (0.75) | 3.67 (0.72) | −0.254 | 0.799 | −0.03 | |
| critical | 3.78 (0.79) | 3.77 (0.83) | 3.79 (0.72) | −0.201 | 0.841 | −0.03 | |
| Dietary behaviors | 2.94 (0.65) | 3.01 (0.64) | 2.85 (0.65) | 3.35 | 0.001 | 0.25 | |
| Exercise habits | 9.16 (6.77) | 11.02 (7.33) | 6.65 (4.92) | 9.26 | <0.001 | 0.70 | |
| Whole population | Male | Female | x2 | p | |||
| N (%) | |||||||
| Subjective health status (five status) | 34.17 | <0.001 | |||||
| very good | 44 (6.50) | 36 (9.30) | 8 (2.80) | ||||
| good | 248 (36.80) | 164 (42.30) | 84 (29.40) | ||||
| neutral | 296 (43.90) | 154 (39.70) | 142 (49.70) | ||||
| bad | 79 (11.70) | 30 (7.70) | 49 (17.10) | ||||
| very bad | 7 (1.00) | 4 (1.00) | 3 (1.00) | ||||
| Perception of the importance of health (five conditions) | 5.66 | 0.226 | |||||
| very important | 59 (8.80) | 41 (10.60) | 18 (6.30) | ||||
| important | 265 (39.40) | 151 (38.90) | 114 (40.00) | ||||
| neutral | 312 (46.40) | 178 (45.90) | 134 (47.00) | ||||
| not important | 31 (4.60) | 14 (3.60) | 17 (6.00) | ||||
| not at all important | 6 (0.90) | 4 (1.00) | 2 (0.07) | ||||
| Dietary supplement use (two conditions) | 8.41 | 0.005 | |||||
| user | 380 (56.50) | 201 (51.80) | 179 (63.00) | ||||
| nonuser | 292 (43.50) | 187 (48.20) | 105 (37.00) | ||||
| Dietary Behaviors (n = 674) | ||||
|---|---|---|---|---|
| B | SE | Beta | p | |
| Gender (0 = Male, 1 = Female) | −0.07 | 0.03 | −0.11 | 0.003 |
| Dietary supplement use (0 = Nonuser, 1 = User) | 0.08 | 0.02 | 0.12 | 0.001 |
| Subjective health status | 0.05 | 0.03 | 0.08 | 0.051 |
| Perception of the importance of health | 0.08 | 0.03 | 0.13 | 0.004 |
| Functional eHealth literacy | 0.02 | 0.03 | 0.04 | 0.357 |
| Interactive eHealth literacy | 0.00 | 0.03 | 0.00 | 0.943 |
| Critical eHealth literacy | 0.14 | 0.03 | 0.22 | <0.001 |
| Gender × Dietary supplement use | −0.01 | 0.02 | −0.01 | 0.720 |
| Gender × Subjective health status | −0.02 | 0.03 | −0.03 | 0.546 |
| Gender × Perception of the importance of health | 0.02 | 0.03 | 0.03 | 0.428 |
| Gender × Functional eHealth literacy | 0.02 | 0.03 | 0.03 | 0.407 |
| Gender × Interactive eHealth literacy | 0.06 | 0.03 | 0.09 | 0.090 |
| Gender × Critical eHealth literacy | −0.07 | 0.03 | −0.10 | 0.038 |
| Adjusted R2 = 0.13, F = 8.91, p < 0.001 | ||||
| Exercise Habits (n = 674) | ||||
|---|---|---|---|---|
| B | SE | Beta | p | |
| Gender (0 = Male, 1 = Female) | −1.84 | 0.25 | −0.27 | <0.001 |
| Dietary supplement use (0 = Nonuser, 1 = User) | −0.01 | 0.24 | −0.00 | 0.967 |
| Subjective health status | 1.57 | 0.29 | 0.23 | <0.001 |
| Perception of the importance of health | 0.03 | 0.29 | 0.01 | 0.912 |
| Functional eHealth literacy | 0.27 | 0.26 | 0.04 | 0.300 |
| Interactive eHealth literacy | −0.04 | 0.34 | −0.01 | 0.909 |
| Critical eHealth literacy | 0.38 | 0.33 | 0.06 | 0.258 |
| Gender × Dietary supplement use | −0.09 | 0.25 | −0.01 | 0.719 |
| Gender × Subjective health status | −0.84 | 0.28 | −0.12 | 0.003 |
| Gender × Perception of the importance of health | 0.47 | 0.29 | 0.07 | 0.104 |
| Gender × Functional eHealth literacy | −0.05 | 0.26 | −0.01 | 0.843 |
| Gender × Interactive eHealth literacy | 0.15 | 0.34 | 0.02 | 0.659 |
| Gender × Critical eHealth literacy | −0.33 | 0.34 | −0.05 | 0.336 |
| Adjusted R2 = 0.16, F = 10.86, p < 0.001 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.L.; Yang, S.-C.; Chiang, C.-H. The Associations between Individual Factors, eHealth Literacy, and Health Behaviors among College Students. Int. J. Environ. Res. Public Health 2020, 17, 2108. https://doi.org/10.3390/ijerph17062108
Huang CL, Yang S-C, Chiang C-H. The Associations between Individual Factors, eHealth Literacy, and Health Behaviors among College Students. International Journal of Environmental Research and Public Health. 2020; 17(6):2108. https://doi.org/10.3390/ijerph17062108
Chicago/Turabian StyleHuang, Chiao Ling, Shu-Ching Yang, and Chia-Hsun Chiang. 2020. "The Associations between Individual Factors, eHealth Literacy, and Health Behaviors among College Students" International Journal of Environmental Research and Public Health 17, no. 6: 2108. https://doi.org/10.3390/ijerph17062108
APA StyleHuang, C. L., Yang, S.-C., & Chiang, C.-H. (2020). The Associations between Individual Factors, eHealth Literacy, and Health Behaviors among College Students. International Journal of Environmental Research and Public Health, 17(6), 2108. https://doi.org/10.3390/ijerph17062108