Analysis of the Components of a Cognitive-Behavioral Intervention for the prevention of Depression Administered via Conference Call to Nonprofessional Caregivers: A Randomized Controlled Trial

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
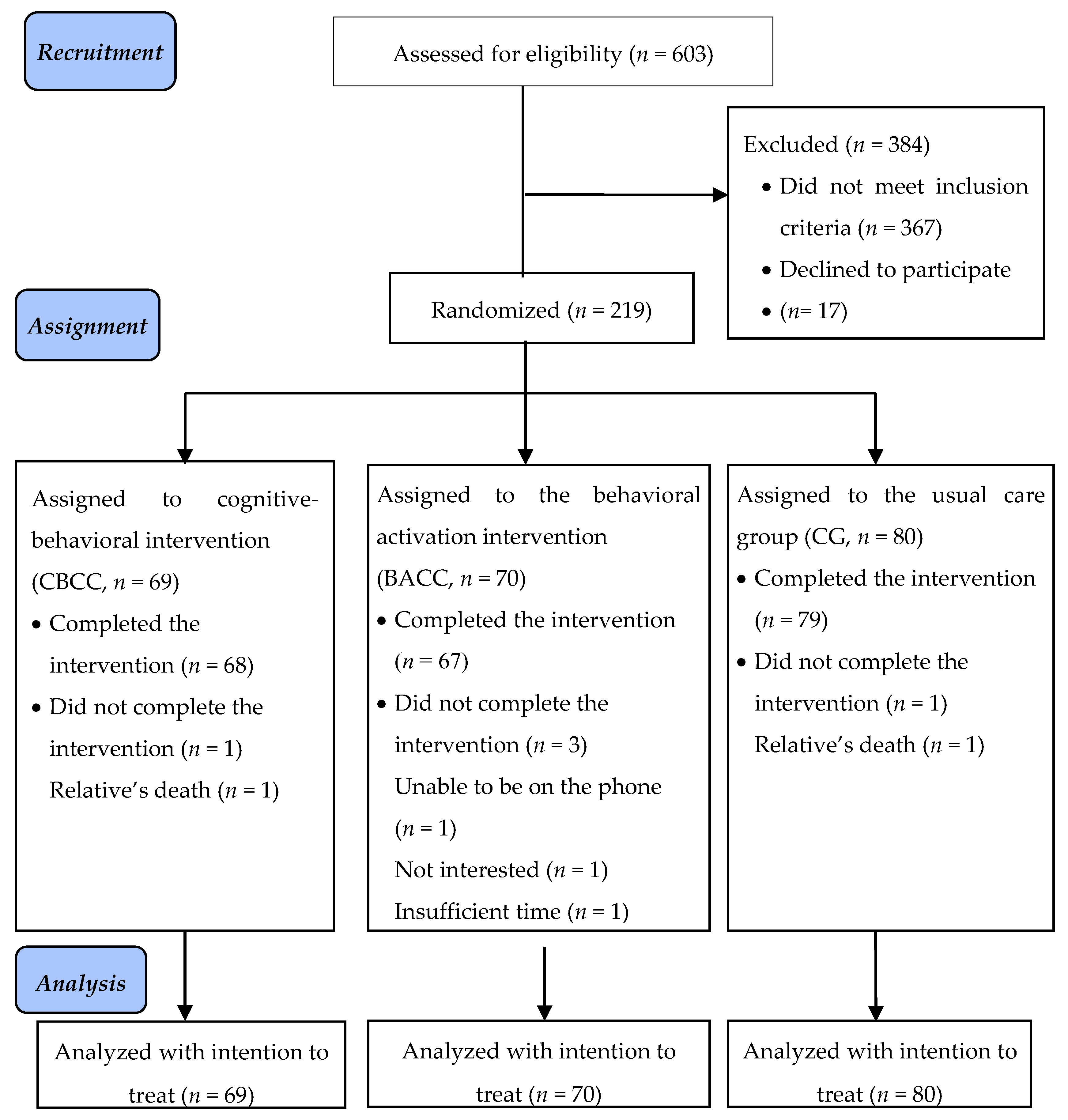
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Intervention and Control Groups
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Incidence of Depression
3.3. Depressive Symptomatology
3.4. Clinically Significant Change
3.5. Acceptability and Satisfaction with the Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Lewinsohn, P.M.; Hoberman, H.; Teri, L.; Hautzinger, M. An integrative theory of depression. In Theoretical Issues in Behaviour Therapy; Reiss, S., Bootzin, R.R., Eds.; Academic Press: New York, NY, USA, 1985; pp. 313–359. [Google Scholar]
- Hasler, G. Pathophysiology of depression: Do we have any solid evidence of interest to clinicians? World Psychiatry 2010, 9, 155–161. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf;jsessionid=AB723912C9867A8AC437F321DB5AACDD?sequence=1 (accessed on 25 January 2020).
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef]
- ten Have, M.; de Graaf, R.; van Dorsselaer, S.; Tuithof, M.; Kleinjan, M.; Penninx, B.W.J.H. Recurrence and chronicity of major depressive disorder and their risk indicators in a population cohort. Acta Psychiatr. Scand. 2018, 137, 503–515. [Google Scholar] [CrossRef]
- Hardeveld, F.; Spijker, J.; de Graaf, R.; Nolen, W.A.; Beekman, A.T.F. Recurrence of major depressive disorder and its predictors in the general population: Results from The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Psychol. Med. 2013, 43, 39–48. [Google Scholar] [CrossRef]
- Hoertel, N.; Blanco, C.; Oquendo, M.A.; Wall, M.M.; Olfson, M.; Falissard, B.; Franco, S.; Peyre, H.; Lemogne, C.; Limosin, F. A comprehensive model of predictors of persistence and recurrence in adults with major depression: Results from a national 3-year prospective study. J. Psychiatr. Res. 2017, 95, 19–27. [Google Scholar] [CrossRef]
- Kohn, R.; Saxena, S.; Levav, I.; Saraceno, B. The treatment gap in mental health care. Bull. World Health Organ. 2004, 82, 858–866. [Google Scholar] [CrossRef]
- Thornicroft, G.; Chatterji, S.; Evans-Lacko, S.; Gruber, M.; Sampson, N.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.; Borges, G.; et al. Undertreatment of people with major depressive disorder in 21 countries. Br. J. Psychiatry 2017, 210, 119–124. [Google Scholar] [CrossRef]
- van Zoonen, K.; Buntrock, C.; Ebert, D.D.; Smit, F.; Reynolds III, C.F.; Beekman, A.T.F.; Cuijpers, P. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. Int. J. Epidemiol. 2014, 43, 318–329. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Stockings, E.A.; Harris, M.G.; Doi, S.A.R.; Page, I.S.; Davidson, S.K.; Barendregt, J.J. The risk of developing major depression among individuals with subthreshold depression: A systematic review and meta-analysis of longitudinal cohort studies. Psychol. Med. 2019, 49, 92–102. [Google Scholar] [CrossRef]
- Joling, K.J.; Smit, F.; van Marwijk, H.W.J.; van der Horst, H.E.; Scheltens, P.; Schulz, R.; van Hout, H.P. Identifying target groups for the prevention of depression among caregivers of dementia patients. Int. Psychogeriatr. 2012, 24, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Howland, R.H.; Schettler, P.J.; Rapaport, M.H.; Mischoulon, D.; Schneider, T.; Fasiczka, A.; Delrahiem, K.; Maddux, R.; Lightfoot, M.; Nierenberg, A.A. Clinical features and functioning of patients with minor depression. Psychother. Psychosom. 2008, 77, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Smit, F.; Oostenbrink, J.; de Graaf, R.; ten Have, M.; Beekman, A. Economic costs of minor depression: A population based-study. Acta Psychiatr. Scand. 2007, 115, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Vogelzangs, N.; Twisk, J.; Kleiboer, A.; Li, J.; Penninx, B.W. Differential mortality rates in major and subthreshold depression: Meta-analysis of studies that measured both. Br. J. Psychiatry 2013, 202, 22–27. [Google Scholar] [CrossRef]
- Ho, C.S.H.; Jin, A.; Nyunt, M.S.Z.; Feng, L.; Ng, T.P. Mortality rates in major and subthreshold depression: 10-year follow-up of a Singaporean population cohort of older adults. Postgrad. Med. 2016, 128, 642–647. [Google Scholar] [CrossRef]
- Torres, Á.; Blanco, V.; Vázquez, F.L.; Díaz, O.; Otero, P.; Hermida, E. Prevalence of major depressive episodes in non-professional caregivers. Psychiatry Res. 2015, 226, 333–339. [Google Scholar] [CrossRef]
- Givens, J.L.; Mezzacappa, C.; Heeren, T.; Yaffe, K.; Fredman, L. Depressive symptoms among dementia caregivers: Role of mediating factors. Am. J. Geriatr. Psychiatry 2014, 22, 481–488. [Google Scholar] [CrossRef]
- Lee, Y.; Xu, L.; Kim, B.J.; Chen, L. Leisure activity, gender and depressive symptoms among dementia caregivers: Findings from the REACH II. Aging Ment. Health 2019. [Google Scholar] [CrossRef]
- Triantafillou, J.; Naiditch, M.; Repkova, K.; Stiehr, K.; Carretero, S.; Emilsson, T.; Di Santo, P.; Bednarik, R.; Brichtova, L.; Ceruzzi, F.; et al. Informal Care in the Long-Term Care System; European Overview Paper; Interlinks: Athens, Vienna, 2010. [Google Scholar]
- Vázquez, F.L.; Otero, P.; Torres, Á.; Hermida, E.; Blanco, V.; Díaz, O. A brief problem-solving indicated-prevention intervention for prevention of depression in nonprofessional caregivers. Psicothema 2013, 25, 87–92. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Hermida, E.; Torres, Á.; Otero, P.; Blanco, V.; Díaz, O. Eficacia de una intervención preventiva cognitivo conductual en cuidadores con síntomas depresivos elevados. [Efficacy of a brief cognitive-behavioral intervention in caregivers with high depressive symptoms]. Behav. Psychol. 2014, 22, 79–96. [Google Scholar]
- Brenes, G.A.; Ingram, C.W.; Danhauer, S.C. Benefits and challenges of conducting psychotherapy by telephone. Prof. Psychol. Res. Pract. 2011, 42, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.; Gili, M.; Ricci-Cabello, I.; Roca, M.; Gilbody, S.; Pérez-Ara, M.Á.; Seguí, A.; McMillan, D. Effectiveness and adherence of telephone-administered psychotherapy for depression: A systematic review and meta-analysis. J. Affect. Disord. 2019, 260, 514–526. [Google Scholar] [CrossRef]
- Smith, T.L.; Toseland, R.W. The effectiveness of a telephone support program for caregivers of frail older adults. Gerontologist 2006, 46, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Tremont, G.; David, J.D.; Papandonatos, G.D.; Ott, B.R.; Fortinsky, R.H.; Gozalo, P.; Yue, M.S.; Bryant, K.; Grover, C.; Bishop, D.S. Psychosocial telephone intervention for dementia caregivers: A randomized, controlled trial. Alzheimers Dement. 2015, 11, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, K.; Beische, D.; Hautzinger, M.; Berry, J.W.; Wengert, J.; Hoffrichter, R.; Becker, C.; van Schayck, R.; Elliott, T.R. Telephone-based problem-solving intervention for family caregivers of stroke survivors: A randomized controlled trial. J. Consult. Clin. Psychol. 2014, 82, 628–643. [Google Scholar] [CrossRef]
- Wilz, G.; Reder, M.; Meichsner, F.; Soellner, R. The Tele.TAnDem Intervention: Telephone-based CBT for family caregivers of people with Dementia. Gerontologist 2018, 58, e118–e129. [Google Scholar] [CrossRef]
- Papa, A.; Follete, W.C. Dismantling studies of psychotherapy. In The Encyclopedia of Clinical Psychology, 1st ed.; Cautin, R.L., Lilienfeld, S.O., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Dimidjian, S.; Hollon, S.D.; Dobson, K.S.; Schmaling, K.B.; Kolenberg, R.J.; Addis, M.E.; Gallop, R.; McGlinchey, J.B.; Markley, D.K.; Gollan, J.K.; et al. Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression. J. Consult. Clin. Psychol. 2006, 74, 658–670. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Dobson, K.S.; Truax, P.A.; Addis, M.E.; Koerner, K.; Gollan, J.K.; Gortner, E.; Prince, S.E. A component analysis of cognitive-behavioral treatment of depression. J. Consult. Clin. Psychol. 1996, 64, 295–304. [Google Scholar] [CrossRef]
- Kazdin, A.E. Research Design in Clinical Psychology, 3rd ed.; Allyn and Bacon: Boston, MA, USA, 2002. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Blanco, V.; López, M. An adaptation of the Center for Epidemiologic Studies Depression Scale for use in non-psychiatric Spanish populations. Psychiatry Res. 2007, 149, 247–252. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Blanco, V.; Otero, P.; Díaz, O.; Ferraces, M.J. Long-term follow-up of a randomized clinical trial assessing the efficacy of a brief cognitive-behavioral depression prevention intervention for caregivers with elevated depressive symptoms. Am. J. Geriatr. Psychiatry 2016, 24, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, F.L.; Torres, Á.; Otero, P.; Blanco, V.; Díaz, O.; Estévez, L.E. Analysis of the components of a cognitive-behavioral intervention administered via conference call for preventing depression among non-professional caregivers: A pilot study. Aging Ment. Health 2017, 21, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Grady, D.; Cummings, S.R.; Hulley, S.B. Alternative clinical trial designs and implementation issues. In Designing Clinical Research, 4th ed.; Hulley, S.B., Cummings, S.R., Browner, W.S., Grady, D.G., Newman, T.B., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 151–170. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5® Disorders: Clinical Version (SCID-5-CV); American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2015. [Google Scholar]
- Shankman, S.A.; Funkhouser, C.J.; Klein, D.N.; Davila, J.; Lerner, D.; Hee, D. Reliability and validity of severity dimensions of psychopathology assessed using the Structured Clinical Interview for DSM-5 (SCID). Int. J. Methods Psychiatr. Res. 2018, 27, e1590. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of client/patient satisfaction: Development of a general scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, A.; Otero, P.; Blanco, V.; Attkisson, C.C. Psychometric properties of the Castilian Spanish version of the Client Satisfaction Questionnaire (CSQ-8). Curr. Psychol. 2019, 38, 829–835. [Google Scholar] [CrossRef]
- van-der Hofstadt, C.J. El Libro de las Habilidades de Comunicación [The Book of Communication Skills], 2nd ed.; Díaz de Santos: Madrid, Spain, 2008. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org (accessed on 25 January 2020).
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Honaker, J.; King, G. What to do about missing values in time series cross-section data. AJPS 2010, 54, 561–581. [Google Scholar] [CrossRef]
- Honaker, J.; King, G.; Blackwell, M. Amelia II: A Program for Missing Data. J. Stat. Softw. 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Van Buuren, S. Flexible Imputation of Missing Data, 2nd ed.; Chapman & Hall: Boca Raton, FL, USA, 2018. [Google Scholar]
- Robitzsch, A.; Grund, S.; Henke, T. Miceadds: Some Additional Multiple Imputation Functions, Especially for Mice; R Package Version 2.12-24. 2018. Available online: https://CRAN.R-project.org/package=miceadds (accessed on 25 January 2020).
- Guyatt, G.H.; Sackett, D.L.; Cook, D.J. Users’ guides to the medical literature, II. How to use an article about therapy or prevention. What were the results and will they help me in caring for my patients? JAMA 1994, 271, 59–63. [Google Scholar] [CrossRef]
- Jiang, J. Linear and Generalized Linear Mixed Models and Their Applications; Springer: New York, NY, USA, 2007. [Google Scholar]
- Pinheiro, J.C.; Bates, D.M. Mixed-Effects Models in S and S-PLUS; Springer: New York, NY, USA, 2000. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Lenth, R. Emmeans: Estimated Marginal Means, aka Least-Squares Means. R Package Version 1.4.2. 2019. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 24 January 2020).
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Follette, W.C.; Revenstorf, D. Psychotherapy outcome research: Methods for reporting variability and evaluating clinical significance. Behav. Ther. 1984, 15, 336–352. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Roberts, L.J.; Berns, S.B.; McGlinchey, J.B. Methods for defining and determining the clinical significance of treatment effects: Description, application, and alternatives. J. Consult. Clin. Psychol. 1999, 67, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Blanco, V.; Otero, P.; López, L.; Torres, Á.; Vázquez, F.L. Predictores del cambio clínicamente significativo en una intervención de prevención de la depresión [Clinically significant predictors of change in an intervention for the prevention of depression]. Rev. Iberoam. Psicol. Salud 2017, 8, 9–20. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Warmerdam, L. Behavioral activation treatments of depression: A meta-analysis. Clin. Psychol. Rev. 2007, 27, 318–326. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Depression in Adults: Recognition and Management. 2018. Available online: https://www.nice.org.uk/guidance/cg90/ifp/chapter/treatments-for-mild-to-moderate-depression (accessed on 27 January 2020).
- Cuijpers, P.; Cristea, I.A.; Karyotaki, E.; Reijnders, M.; Hollon, S.D. Component studies of psychological treatments of adult depression: A systematic review and meta-analysis. Psychother. Res. 2019, 29, 15–29. [Google Scholar] [CrossRef]
- Otero, P.; Vázquez, F.L.; Hermida, E.; Díaz, O.; Torres, Á. Relationship of cognitive behavioral therapy effects and homework in an indicated prevention of depression intervention for non-professional caregivers. Psychol. Rep. 2015, 116, 841–854. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, A.; Blanco, V.; Otero, P.; Hermida, E. Intervenciones psicológicas administradas por teléfono para la depresión: Una revisión sistemática y meta-análisis [Telephone-administered psychological interventions for depression: A systematic review and meta-analysis]. Rev. Iberoam. de Psicol. y Salud 2015, 6, 39–52. [Google Scholar] [CrossRef]
- Kazdin, A.E. Mediators and mechanisms of change in psychotherapy research. Annu. Rev. Clin. Psychol. 2007, 3, 1–27. [Google Scholar] [CrossRef]
- Colombo, F.; Llena-Nozal, A.; Mercier, J.; Tjadens, F. Help Wanted? Providing and Paying for Long-Term Care; OECD Publishing, OECD Health Policy Studies: Paris, France, 2011. [Google Scholar]


{kind=link}
| Variables | Total | CBCC | BACC | CG | ||||
|---|---|---|---|---|---|---|---|---|
| N = 219 | % | n = 69 | % | n = 70 | % | n = 80 | % | |
| Sex | ||||||||
| Men | 20 | 9.1 | 7 | 10.1 | 3 | 4.3 | 10 | 12.5 |
| Women | 199 | 90.9 | 62 | 89.9 | 67 | 95.7 | 70 | 87.5 |
| Age | ||||||||
| M | 54.0 | 54.8 | 54.5 | 52.9 | ||||
| SD | 10.8 | 10.7 | 11.0 | 10.7 | ||||
| Range | 25–76 | 34–75 | 32–74 | 25–76 | ||||
| Marital status | ||||||||
| Single | 25 | 11.4 | 7 | 10.2 | 9 | 12.9 | 9 | 11.2 |
| Married, lives as a couple | 157 | 71.7 | 51 | 73.9 | 52 | 74.2 | 54 | 67.5 |
| Separated, divorced, widowed | 37 | 16.9 | 11 | 15.9 | 9 | 12.9 | 17 | 21.3 |
| Social class | ||||||||
| Low/lower middle | 114 | 52.1 | 36 | 52.2 | 39 | 55.7 | 39 | 48.7 |
| Middle/upper middle | 105 | 47.9 | 33 | 47.8 | 31 | 44.3 | 41 | 51.3 |
| Level of education | ||||||||
| Can read and write | 27 | 12.3 | 5 | 7.3 | 12 | 17.1 | 10 | 12.5 |
| Primary | 123 | 56.2 | 39 | 56.5 | 38 | 54.3 | 46 | 57.5 |
| Secondary/University | 69 | 31.5 | 25 | 36.2 | 20 | 28.6 | 24 | 30.0 |
| Primary activity | ||||||||
| Active worker | 46 | 21.0 | 11 | 15.9 | 16 | 22.9 | 19 | 23.7 |
| Unemployed/retired | 173 | 79.0 | 58 | 84.1 | 54 | 77.1 | 61 | 76.3 |
| Care recipient sex | ||||||||
| Male | 85 | 38.8 | 28 | 40.6 | 28 | 40.0 | 29 | 36.2 |
| Female | 134 | 61.2 | 41 | 59.4 | 42 | 60.0 | 51 | 63.8 |
| Care recipient age | ||||||||
| M | 60.8 | 59.9 | 67.6 | 55.5 | ||||
| SD | 33.1 | 32.7 | 30.0 | 35.2 | ||||
| Range | 1–100 | 1–99 | 3–98 | 3–100 | ||||
| Relationship | ||||||||
| Father/mother | 86 | 39.3 | 27 | 39.1 | 32 | 45.7 | 27 | 33.7 |
| Spouse/partner | 12 | 5.5 | 2 | 3.0 | 4 | 5.7 | 6 | 7.5 |
| Son/daughter | 75 | 34.2 | 27 | 39.1 | 17 | 24.3 | 31 | 38.8 |
| Other | 46 | 21.0 | 13 | 18.8 | 17 | 24.3 | 16 | 20.0 |
| Care recipient diagnosis | ||||||||
| -Diseases of the skeletomuscular/connective tissue/cardiovascular/respiratory systems | 53 | 24.2 | 13 | 18.8 | 18 | 25.7 | 22 | 27.5 |
| -Chromosomal/congenital/perinatal abnormalities | 39 | 17.8 | 11 | 15.9 | 13 | 18.6 | 15 | 18.8 |
| -Mental/neurological disorders/brain damage | 62 | 28.3 | 21 | 30.5 | 16 | 22.8 | 25 | 31.2 |
| -Dementias | 65 | 29.7 | 24 | 34.8 | 23 | 32.9 | 18 | 22.5 |
| Care duration (years) | ||||||||
| M | 12.8 | 13.9 | 12.8 | 11.9 | ||||
| SD | 9.1 | 9.8 | 9.0 | 8.5 | ||||
| Range | 1–47 | 1–47 | 2–47 | 2–46 | ||||
| Daily hours of care | ||||||||
| M | 15.8 | 15.3 | 16.2 | 15.9 | ||||
| SD | 4.1 | 4.4 | 3.8 | 4.0 | ||||
| Range | 1–20 | 3–20 | 1–18 | 5–20 | ||||
| Group | PRE | POST | t | SE | p | Effect Size | 95% CI | |
|---|---|---|---|---|---|---|---|---|
| M (SE) | M (SE) | Min | Max | |||||
| CBCC | 22.3 (0.86) | 11.3 (0.87) | 11.044 | 0.989 | <0.001 | 1.53 | 1.24 | 1.83 |
| BACC | 22.7 (0.86) | 10.4 (0.88) | 12.280 | 0.999 | <0.001 | 1.72 | 1.42 | 2.02 |
| CG | 23.1 (0.80) | 19.6 (0.81) | 3.815 | 0.920 | <0.001 | 0.49 | 0.24 | 0.75 |
| Comparison | t | SE | p | Effect Size | 95% CI | |
|---|---|---|---|---|---|---|
| Min | Max | |||||
| CBCC vs. CG | 6.963 | 1.188 | <0.001 | 1.16 | 0.82 | 1.50 |
| BACC vs. CG | 7.724 | 1.192 | <0.001 | 1.29 | 0.95 | 1.63 |
| CBCC vs. BACC | −0.760 | 1.237 | 1.000 | −0.13 | −0.47 | 0.21 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez, F.L.; López, L.; Torres, Á.J.; Otero, P.; Blanco, V.; Díaz, O.; Páramo, M. Analysis of the Components of a Cognitive-Behavioral Intervention for the prevention of Depression Administered via Conference Call to Nonprofessional Caregivers: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 2067. https://doi.org/10.3390/ijerph17062067
Vázquez FL, López L, Torres ÁJ, Otero P, Blanco V, Díaz O, Páramo M. Analysis of the Components of a Cognitive-Behavioral Intervention for the prevention of Depression Administered via Conference Call to Nonprofessional Caregivers: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(6):2067. https://doi.org/10.3390/ijerph17062067
Chicago/Turabian StyleVázquez, Fernando L., Lara López, Ángela J. Torres, Patricia Otero, Vanessa Blanco, Olga Díaz, and Mario Páramo. 2020. "Analysis of the Components of a Cognitive-Behavioral Intervention for the prevention of Depression Administered via Conference Call to Nonprofessional Caregivers: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 6: 2067. https://doi.org/10.3390/ijerph17062067
APA StyleVázquez, F. L., López, L., Torres, Á. J., Otero, P., Blanco, V., Díaz, O., & Páramo, M. (2020). Analysis of the Components of a Cognitive-Behavioral Intervention for the prevention of Depression Administered via Conference Call to Nonprofessional Caregivers: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(6), 2067. https://doi.org/10.3390/ijerph17062067