Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans

 ,
,  and
and
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population and Inclusion Criteria
- Control (implant placement without graft material), n = 25;
- Test (implant placement with graft material), n = 24.
4.2. Surgical Procedure
4.3. Statistical Analysis
- -
- Initial available bone: Amount of bone measured on a calibrated panoramic radiograph.
- -
- Implant length: The length of the implant used was 8 or 10 mm.
- -
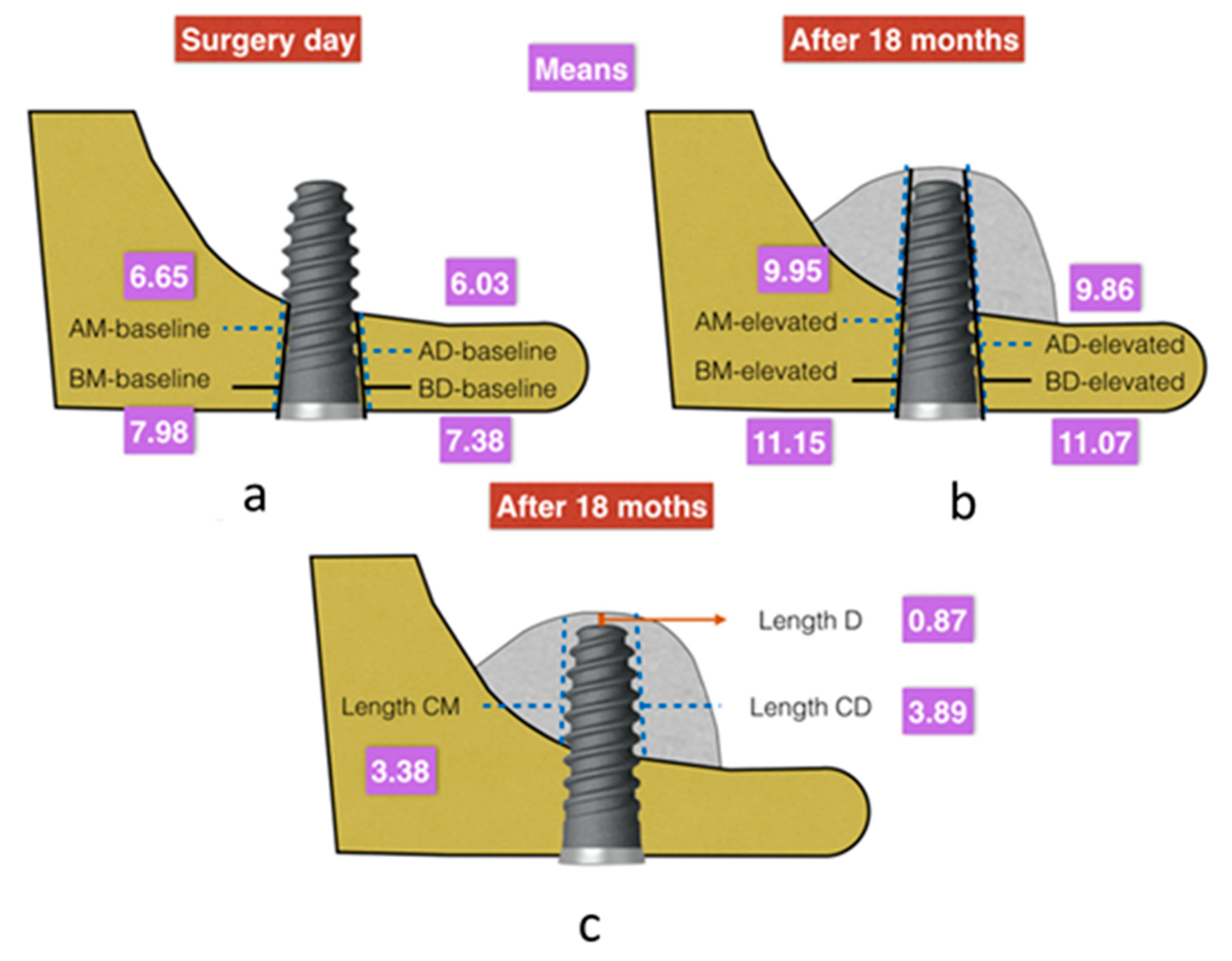
- Postoperative radiography:
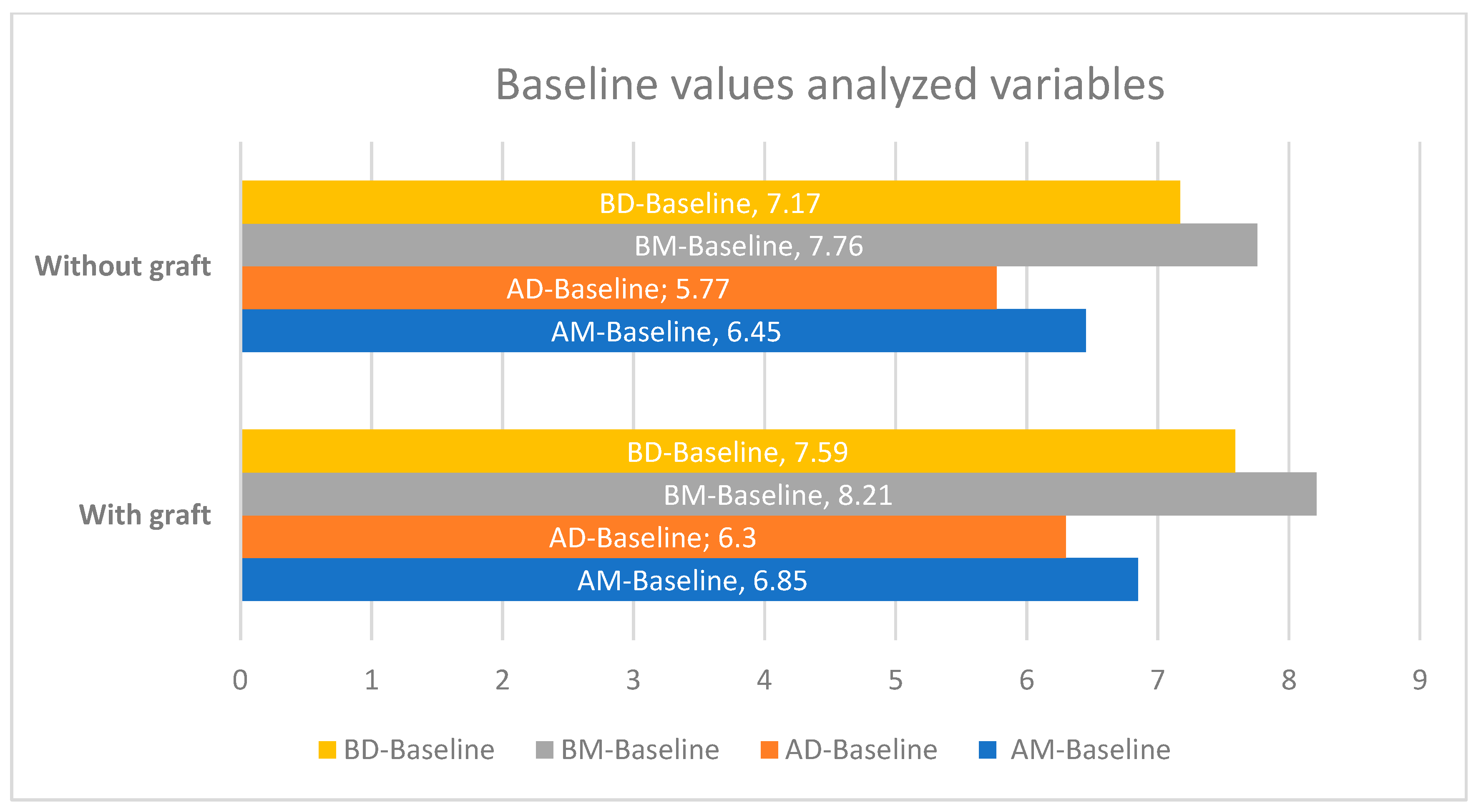
- Length AM-baseline: Distance between the alveolar process and cortical bone of the sinus floor, mesial to the implant.
- Length BM-baseline: Distance between the implant shoulder and the cortical bone of the sinus floor, mesial to the implant.
- Length AD-baseline: Distance between the alveolar process and the cortical bone of the sinus floor, distal to the implant.
- Length BD-baseline: Distance between the implant shoulder and the cortical bone of the sinus floor, distal to the implant.
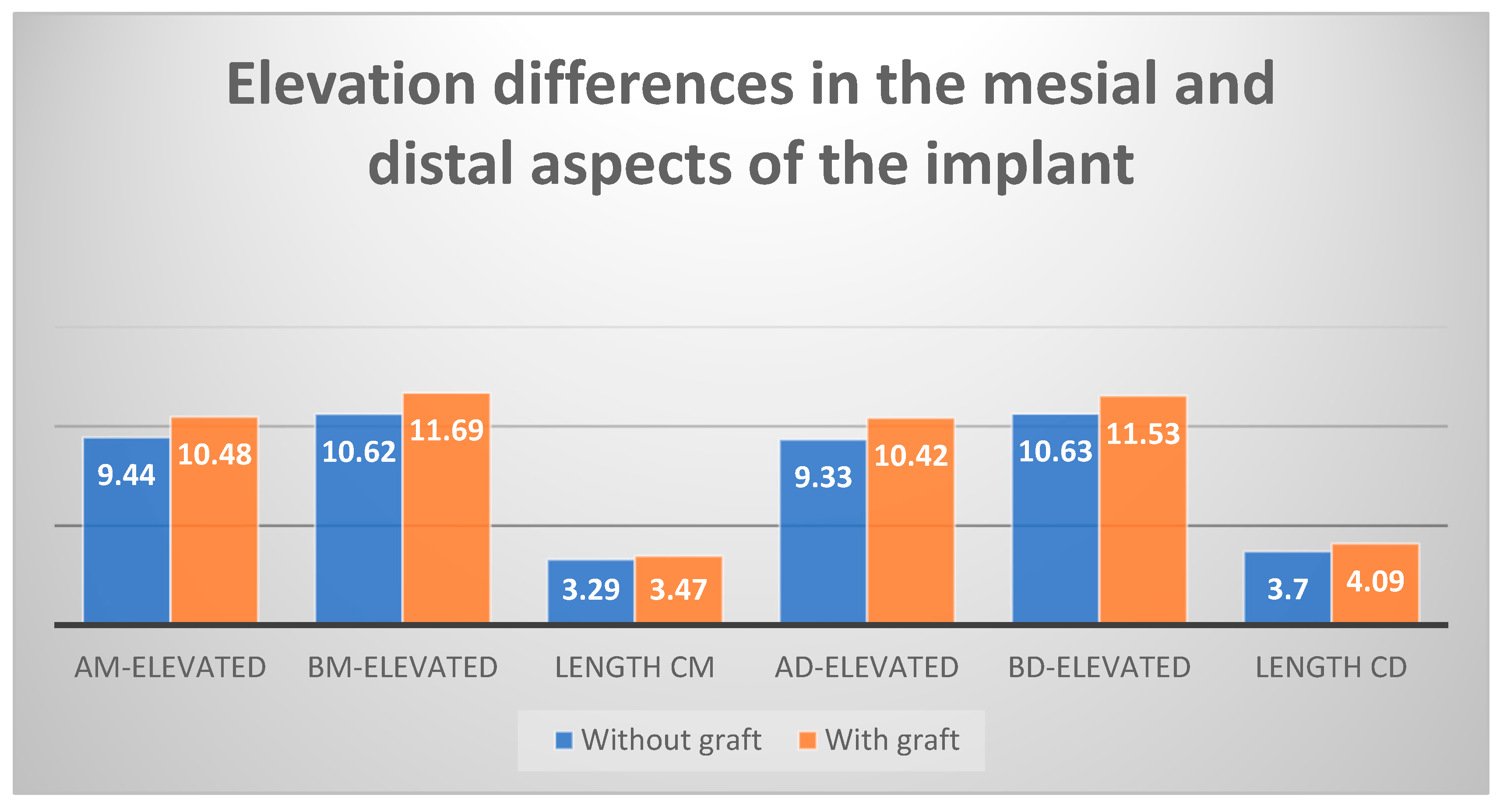
- Length AM-elevated: Distance between the alveolar process and the new sinus cortical bone, mesial to the implant.
- Length BM-elevated: Distance between the implant shoulder and the new sinus cortical bone, mesial to the implant.
- Length AD-elevated: Distance between the alveolar process and the new sinus cortical bone, distal to the implant.
- Length BD-elevated: Distance between the implant shoulder and the new sinus cortical bone, distal to the implant.
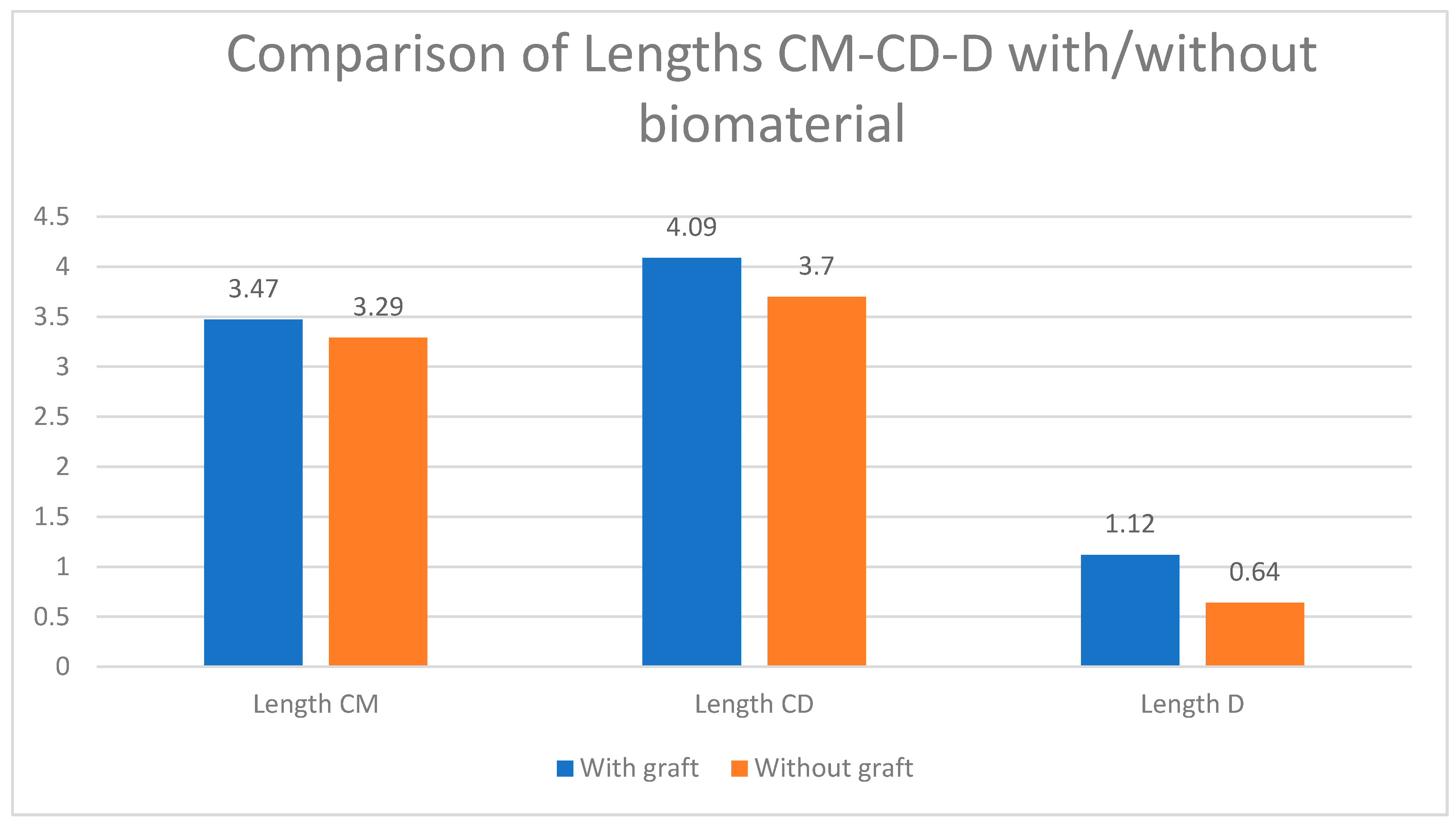
- Length CM: Distance between the initial sinus cortical bone and the new cortical bone, mesial to the implant.
- Length CD: Distance between the initial sinus cortical bone and the new cortical bone, distal to the implant.
- Length D: Distance from the apex of the implant to the new cortical bone.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Axelsson, P.; Lindhe, J. The significance of maintenance care in the treatment of periodontal disease. J. Clin. Periodontol. 1981, 8, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Oliphant, T.H.; McHugh, R.B. Molar and nonmolar teeth compared over 6½ years following two methods of periodontal therapy. J. Periodontol. 1984, 55, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Kalkwarf, K.L.; Kaldahl, W.B.; Patil, K.D. Evaluation of furcation region response to periodontal therapy. J. Periodontol. 1988, 59, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, L.; Wasserman, B. A long-term survey of tooth loss in 600 treated periodontal patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef]
- Frost, H.M. Bone’s mechanostat: A 2003 update. Anat. Rec. 2003, 275, 1081–1101. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “mass” and the “mechanostat”: A proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Wiskott, H.W.A.; Belser, U.C. Lack of integration of smooth titanium surfaces: A working hypothesis based on strains generated in the surrounding bone. Clin. Oral Implant. Res. 1999, 10, 429–444. [Google Scholar] [CrossRef]
- Misch, C.E. Maxillary sinus augmentation for endosteal implants: Organized alternative treatment plans. Int. J. Oral Implant.. 1987, 4, 49–58. [Google Scholar]
- Jensen, O.T.; Shulman, L.B.; Block, M.S.; Iacono, V.J. Report of the sinus consensus conference of 1996. Int. J. Oral Maxillofac. Implant. 1998, 13, 11–45. [Google Scholar]
- Cardaropoli, G.; Araujo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef]
- Botticelli, D.; Berglundh, T.; Persson, L.G.; Lindhe, J. Bone regeneration at implants with turned or rough surfaces in self-contained defects. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Zarb, G.A.; Zarb, F.L. Tissue integrated dental prostheses. Quintessence Int. 1985, 16, 39–42. [Google Scholar] [PubMed]
- Tatum, H. Maxillary and sinus implant reconstructions. Dent. Clin. North Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar]
- Rosen, P.S.; Summers, R.; Mellado, J.R.; Salkin, L.M.; Shanaman, R.H.; Marks, M.H.; Fugazzotto, P.A. The bone-added osteotome sinus floor elevation technique: Multicenter retrospective report of consecutively treated patients. Int. J. Oral Maxillofac. Implant 1999, 14, 853–858. [Google Scholar]
- Summers, R.B. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994, 15, 154–156. [Google Scholar]
- Summers, R.B. The osteotome technique: Part 2—The ridge expansion osteotomy (REO) procedure. Compendium 1994, 15, 422, 424, 426, passim; quiz 436. [Google Scholar]
- Summers, R.B. The osteotome technique: Part 3—Less invasive methods of elevating the sinus floor. Compendium 1994, 15, 694–702. [Google Scholar]
- Emmerich, D.; Att, W.; Stappert, C. Sinus floor elevation using osteotomes: A systematic review and meta-analysis. J. Periodontol. 2005, 76, 1237–1251. [Google Scholar] [CrossRef]
- Shalabi, M.M.; Manders, P.; Mulder, J.; Jansen, J.A.; Creugers, N.H. A meta-analysis of clinical studies to estimate the 4.5-year survival rate of implants placed with the osteotome technique. Int. J. Oral Maxillofac. Implant. 2007, 22, 110–116. [Google Scholar]
- Tong, D.C.; Rioux, K.; Drangsholt, M.; Beirne, O.R. A review of survival rates for implants placed in grafted maxillary sinuses using meta-analysis. Int. J. Oral Maxillofac. Implant. 1998, 13, 175–182. [Google Scholar]
- Nedir, R.; Nurdin, N.; Abi Najm, S.; El Hage, M.; Bischof, M. Short implants placed with or without grafting into atrophic sinuses: The 5-year results of a prospective randomized controlled study. Clin. Oral Implant. Res. 2017, 28, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Nurdin, N.; Khoury, P.; Perneger, T.; Hage, M.E.; Bernard, J.P.; Bischof, M. Osteotome sinus floor elevation with and without grafting material in the severely atrophic maxilla. A 1-year prospective randomized controlled study. Clin. Oral Implant. Res. 2013, 24, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Nurdin, N.; Khoury, P.; Bischof, M. Short implants placed with or without grafting in atrophic sinuses: The 3-year results of a prospective randomized controlled study. Clin. Implant Dent. Relat. Res. 2016, 18, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Patini, R.; Gallenzi, P.; Spagnuolo, G.; Cordaro, M.; Cantiani, M.; Amalfitano, A.; Arcovito, A.; Callà, C.; Mingrone, G.; Nocca, G. Correlation between metabolic syndrome, periodontitis and reactive oxygen species production. A pilot study. Open Dent. J. 2017, 11, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Martellaci, L.; Quaranta, G.; Patini, R.; Isola, G.; Gallenzi, P.; Masucci, L. A literature review of metagenomics and culturomics of the peri-implant microbiome: Current evidence and future perspectives. Materials 2019, 12, 3010. [Google Scholar] [CrossRef]
- Markovic, A.; Misic, T.; Calvo-Guirado, J.L.; Delgado-Ruiz, R.A.; Janjic, B.; Abboud, M. Two-center prospective, randomized, clinical, and radiographic study comparing osteotome sinus floor elevation with or without bone graft and simultaneous implant placement. Clin. Implant Dent. Relat. Res. 2016, 18, 873–882. [Google Scholar] [CrossRef]
- Yang, J.; Xia, T.; Fang, J.; Shi, B. Radiological changes associated with new bone formation following osteotome sinus floor elevation (OSFE): A retrospective study of 40 patients with 18-month follow-up. Med. Sci. Monit. 2018, 24, 4641–4648. [Google Scholar] [CrossRef]
- Chen, M.H.; Shi, J.Y. Clinical and radiological outcomes of implants in osteotome sinus floor elevation with and without grafting: A systematic review and a meta-analysis. J. Prosthodont. 2018, 27, 394–401. [Google Scholar] [CrossRef]
- Aludden, H.; Mordenfeld, A.; Hallman, M.; Christensen, A.E.; Starch-Jensen, T. Osteotome-mediated sinus floor elevation with or without a grafting material: A systematic review and meta-analysis of long-term studies (>/=5-Years). Implant Dent. 2018, 27, 488–497. [Google Scholar] [CrossRef]
- Caban, J.; Fermergard, R.; Abtahi, J. Long-term evaluation of osteotome sinus floor elevation and simultaneous placement of implants without bone grafts: 10-year radiographic and clinical follow-up. Clin. Implant Dent. Relat. Res. 2017, 19, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Nurdin, N.; Vazquez, L.; Abi Najm, S.; Bischof, M. Osteotome sinus floor elevation without grafting: A 10-year prospective study. Clin. Implant Dent. Relat. Res. 2016, 18, 609–617. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DISTANCES AT CRESTA ALVEOLAR LEVEL | Gain (mm) | |||
|---|---|---|---|---|
| Without Biomaterial | With Biomaterial | p | Confidence Interval 95% | |
| intercortical bone, mesial | 2.98 | 3.62 | 0.001 | 0.42/1.66 |
| intercortical bone, distal | 3.56 | 4.12 | 0.005 | 0.39/1.83 |
| from implant neck to floor, mesial | 2.86 | 3.48 | 0.001 | 0.48/1.65 |
| from implant neck to floor, distal soil | 3.47 | 3.94 | 0.006 | 0.66/1.54 |
| floor elevation, mesial | 3.28 | 3.47 | 0.591 * | −0.49/0.85 |
| floor elevation, distal | 3.70 | 4.09 | 0.225 * | −0.25/1.02 |
| bone above implant | 0.63 | 1.12 | <0.0005 | 0.27/0.77 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maximiano Millán, A.; Bravo Álvarez, R.; Plana Montori, M.; Guerrero González, M.; Saura García-Martín, D.; Ríos-Carrasco, B.; Monticelli, F.; Ríos-Santos, J.V.; Fernández-Palacín, A. Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans. Int. J. Environ. Res. Public Health 2020, 17, 1888. https://doi.org/10.3390/ijerph17061888
Maximiano Millán A, Bravo Álvarez R, Plana Montori M, Guerrero González M, Saura García-Martín D, Ríos-Carrasco B, Monticelli F, Ríos-Santos JV, Fernández-Palacín A. Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans. International Journal of Environmental Research and Public Health. 2020; 17(6):1888. https://doi.org/10.3390/ijerph17061888
Chicago/Turabian StyleMaximiano Millán, Adrián, Rocío Bravo Álvarez, Miguel Plana Montori, María Guerrero González, David Saura García-Martín, Blanca Ríos-Carrasco, Francesca Monticelli, José Vicente Ríos-Santos, and Ana Fernández-Palacín. 2020. "Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans" International Journal of Environmental Research and Public Health 17, no. 6: 1888. https://doi.org/10.3390/ijerph17061888
APA StyleMaximiano Millán, A., Bravo Álvarez, R., Plana Montori, M., Guerrero González, M., Saura García-Martín, D., Ríos-Carrasco, B., Monticelli, F., Ríos-Santos, J. V., & Fernández-Palacín, A. (2020). Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans. International Journal of Environmental Research and Public Health, 17(6), 1888. https://doi.org/10.3390/ijerph17061888