High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial


 and
and 
Abstract
1. Introduction
2. Materials and Methods
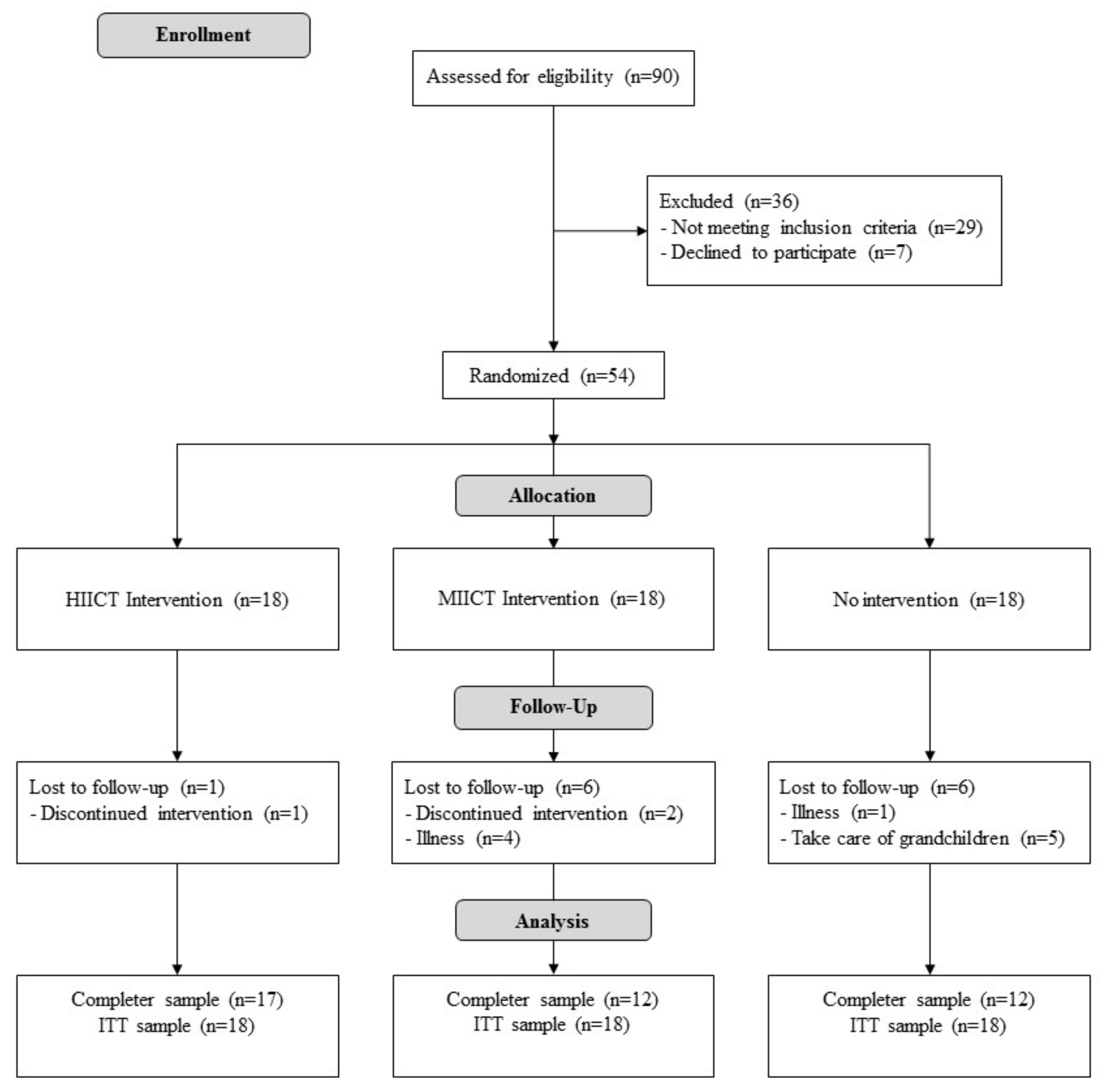
2.1. Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.5. Sample size and Power
2.6. Randomization and Blinding
2.7. Statistical Analysis
3. Results
3.1. Inter-group Results
- For VO2max-ES, HIICT was statistically superior to the CG (dif = 3.4 ml/kg/min, t = −3.73) and MICT was also statistically superior to the CG (dif = 1.9 ml/kg/min, t = −2.65).
- For SBPex, HIICT was statistically better than the CG (dif = −6,39 mmHg, t = −0.122).
- For DBPex, HIICT was statistically better than the CG (dif = −5,00 mmHg, t = −3.933) and MICT was also statistically better than the CG (dif = −7,50 mmHg, t = 3.989).
- Finally, for maximal speed reached during treadmill test, HIICT was statistically superior to the CG (dif = 0.2 m/s, t = −1.96) and MICT was also statistically superior to the CG (dif = 0.57 m/s, t = −2.96).
3.2. Intra-group Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blain, H.; Masud, T.; Dargent-Molina, P.; Martin, F.C.; Rosendahl, E.; van der Velde, N.; Bousquet, J.; Benetos, A.; Cooper, C.; Kanis, J.A.; et al. A comprehensive fracture prevention strategy in older adults: The European Union Geriatric Medicine Society (EUGMS) statement. Aging Clin. Exp. Res. 2016, 28, 797–803. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health. Available online: https://population.un.org/wpp/ (accessed on 13 September 2019).
- Murias, J.M.; Paterson, D.H. Slower VO2 Kinetics in Older Individuals: Is It Inevitable? Med. Sci. Sports Exerc. 2015, 47, 2308–2318. [Google Scholar] [CrossRef] [PubMed]
- Amundsen, B.H.; Rognmo, Ø.; Hatlen-Rebhan, G.; Slørdahl, S.A. High-intensity aerobic exercise improves diastolic function in coronary artery disease. Scand. Cardiovasc. J. SCJ. 2008, 42, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Cardozo, G.G.; Oliveira, R.B.; Farinatti, P.T.V. Effects of high intensity interval versus moderate continuous training on markers of ventilatory and cardiac efficiency in coronary heart disease patients. Sci. World J. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guiraud, T.; Juneau, M.; Nigam, A.; Gayda, M.; Meyer, P.; Mehary, S.; Paillard, F.; Bosquet, L. Optimization of high intensity interval exercise in coronary heart disease. Eur. J. Appl. Physiol. 2010, 108, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Madssen, E.; Arbo, I.; Granøien, I.; Walderhaug, L.; Moholdt, T. Peak oxygen uptake after cardiac rehabilitation: A randomized controlled trial of a 12-month maintenance program versus usual care. PLoS ONE 2014, 9, 733–740. [Google Scholar] [CrossRef]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef]
- Hawkins, S.; Wiswell, R. Rate and mechanism of maximal oxygen consumption decline with aging: Implications for exercise training. Sports Med. Auckl. NZ. 2003, 33, 877–888. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet Lond. Engl. 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.M.; Miller, M.E.; et al. A physical activity intervention to treat the frailty syndrome in older persons-results from the LIFE-P study. J. Gerontol. A. Biol. Sci. Med. Sci. 2015, 70, 216–222. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A. Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Laddu, D.R.; Wertheim, B.C.; Garcia, D.O.; Brunner, R.; Groessl, E.; Shadyab, A.H.; Going, S.B.; LaMonte, M.J.; Cannell, B.; LeBroff, M.S.; et al. Associations between self-reported physical activity and physical performance measures over time in postmenopausal women: The women’s health initiative. J. Am. Geriatr. Soc. 2017, 65, 2176–2181. [Google Scholar] [CrossRef] [PubMed]
- Masley, S.C.; Roetzheim, R.; Clayton, G.; Presby, A.; Sundberg, K.; Masley, L.V. Lifestyle markers predict cognitive function. J. Am. Coll. Nutr. 2017, 36, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Bunout, D.; Barrera, G.; Hirsch, S.; Jimenez, T.; de la Maza, M.P. Association between activity energy expenditure and peak oxygen consumption with sarcopenia. BMC Geriatr. 2018, 18, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Martínez, F.A.; Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Alcaraz, P.E. Effectiveness of resistance circuit-based training for maximum oxygen uptake and upper-body one-repetition maximum improvements: A systematic review and meta-analysis. Sports Med. Auckl. NZ. 2017, 47, 2553–2568. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.L.; Martínez-Guardado, I.; Olcina, G.; Marín-Pagán, C.; Martínez-Noguera, F.J.; Carlos-Vivas, J.; Alcaráz, P.E.; Rubio-Arias, J.Á. Effect of high-intensity resistance circuit-based training in hipoxia on aerobic performance and repeat sprint ability. Scand. J. Med. Sci. Sports 2018, 28, 2135–2143. [Google Scholar] [CrossRef]
- Villelabeitia-Jaureguizar, K.; Vicente-Campos, D.; Senen, A.B.; Jiménez, V.H.; Garrido-Lestache, M.E.B.; López Chicharro, J.L. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int. J. Cardiol. 2017, 244, 17–23. [Google Scholar] [CrossRef]
- Molisz, A.; Schmederer, Z.; Siebert, J.; Kadamani, T.; Glasner, P.; Rosłonkiewicz, K.; Nowicka-Sauer, K.; Gutknecht, P.; Trzeciak, B.; Suchanowski, A. Haemodynamic parameters in postmenopausal women–beneficial effect of moderate continuous exercise training. Ann. Agric. Envirn. Med. 2019, 26, 425–428. [Google Scholar] [CrossRef]
- Huang, G.; Shi, X.; Davis-Brezette, J.A.; Osness, W.H. Resting heart rate changes after endurance training in older adults: A meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 1381–1386. [Google Scholar] [CrossRef]
- Ballesta-García, I.; Rubio Arias, J.Á.; Ramos Campo, D.J.; Martínez González-Moro, I.; Carrasco Poyatos, M. High-intensity interval training dosage for heart failure and coronary artery disease cardiac rehabilitation: A systematic review and meta-analysis. Rev. Espanola Cardiol. Engl. Ed. 2019, 72, 233–243. [Google Scholar] [CrossRef]
- López Chicharro, J.; Vicente Campos, D. HIIT de la teoría a la práctica; Exercise Physiology & Training: Madrid, Spain, 2018. [Google Scholar]
- Hwang, C.-L.; Yoo, J.-K.; Kim, H.-K.; Hwang, M.-H.; Handberg, E.M.; Petersen, J.W.; Christou, D.D. Novel all-extremity high-intensity interval training improves aerobic fitness, cardiac function and insulin resistance in healthy older adults. Exp. Gerontol. 2016, 82, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in adults with pre- to established hypertension: A systematic review and meta-analysis of randomized trials. Sports Med. Auckl. NZ. 2018, 48, 2127–2142. [Google Scholar] [CrossRef] [PubMed]
- Olea, M.A.; Mancilla, R.; Martínez, S.; Díaz, E. Effects of high intensity interval training on blood pressure in hypertensive subjects. Rev. Med. Chil. 2017, 145, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Grace, F.; Herbert, P.; Elliott, A.D.; Richards, J.; Beaumont, A.; Sculthorpe, N.F. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp. Gerontol. 2018, 109, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; García-Pinillos, F.; Latorre-Román, P.Á. Effects of a 10-week functional training programme on pain, mood state, depression, and sleep in healthy older adults. Psychogeriact. Off. J. Psychigeriatr. Soc. 2018, 18, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; de Feitosa-Neta, M.L.; Brandão, L.H.; Chaves, L.M.; da Silva-Grigoletto, M.E. The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fitness 2019, 59, 380–386. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standarized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Ballesta-García, I.; Martínez-González-Moro, I.; Rubio-Arias, J.Á.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Functional Ability and Body Mass Index in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4205. [Google Scholar] [CrossRef]
- Fielding, R.A.; Frontera, W.R.; Hughes, V.A.; Fisher, E.C.; Evans, W.J. The reproducibility of the Bruce protocol exercise test for the determination of aerobic capacity in older women. Med. Sci. Sports Exerc. 1997, 29, 1109–1113. [Google Scholar] [CrossRef]
- Kenney, W.L.; Humphrey, R.H.; Bryant, C.X.; Mahler, D.A. ACSM’s Guidelines for Exercise Testing and Prescription; Williams & Wilkins: Baltimore, MD, USA, 1995. [Google Scholar]
- Nugent, S.F.; Jung, M.E.; Bourne, J.E.; Loeppky, J.; Arnold, A.; Little, J.P. The influence of high-intensity interval training and moderate-intensity continuous training on sedentary time in overweight and obese adults. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2018, 43, 747–750. [Google Scholar] [CrossRef] [PubMed]
- Dünnwald, T.; Melmer, A.; Gatterer, H.; Salzmann, K.; Ebenbichler, C.; Burtscher, M.; Schobersberger, W.; Grander, W. Supervised Short-term High-intensity Training on Plasma Irisin Concentrations in Type 2 Diabetic Patients. Int. J. Sports Med. 2019, 40, 158–164. [Google Scholar] [CrossRef]
- Kim, J.; Shin, W. How to Do Random Allocation (Randomization). Clin. Orthop. Surg. 2014, 6, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Boukabous, I.; Marcotte-Chénard, A.; Amamou, T.; Boulay, P.; Brochu, M.; Tessier, D.; Riesco, E. Low-Volume High-Intensity Interval Training (HIIT) versus Moderate-Intensity Continuous Training on Body Composition, Cardiometabolic Profile and Physical Capacity in Older Women. J. Aging Phys. Act. 2019, 27, 1–34. [Google Scholar]
- Su, L.; Fu, J.; Sun, S.; Zhao, G.; Cheng, W.; Dou, C.; Quan, M. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar] [CrossRef]
- Connolly, L.J.; Bailey, S.J.; Krustrup, P.; Fulford, J.; Smietanka, C.; Jones, A.M. Effects of self-paced interval and continuous training on health markers in women. Eur. J. Appl. Physiol. 2017, 117, 2281–2293. [Google Scholar] [CrossRef]
- Kemi, O.J.; Ellingsen, Ø.; Ceci, M.; Grimaldi, S.; Smith, G.L.; Condorelli, G.; Wisløff, U. Aerobic interval training enhances cardiomyocyte contractility and Ca2+ cycling by phosphorylation of CaMKII and Thr-17 of phospholamban. J. Mol. Cell Cardiol. 2007, 43, 354–361. [Google Scholar] [CrossRef]
- Njemanze, H.; Warren, C.; Eggett, C.; MacGowan, G.A.; Bates, M.G.D.; Siervo, M.; Ivkovic, S.; Trenell, M.I.; Jakovljevic, D.G. Age-related decline in cardiac autonomin function is not attenuated with increased physical activity. Oncotarget 2016, 7, 76390–76397. [Google Scholar] [CrossRef]
- Qiu, Z.; Zheng, K.; Zhang, H.; Feng, J.; Wang, L.; Zhou, H. Physical Exercise and Patients with Chronic Renal Failure: A Meta-Analysis. BioMed Res. Int. 2017, 2017, 7191826. [Google Scholar] [CrossRef] [PubMed]
- Arbit, B.; Azarbal, B.; Hayes, S.W.; Gransar, H.; Germano, G.; Friedman, J.D.; Thomson, L.; Berman, D.S. Prognostic Contribution of Exercise Capacity, Heart Rate Recovery, Chronotropic Incompetence, and Myocardial Perfusion Single-Photon Emission Computerized Tomography in the Prediction of Cardiac Death and All-Cause Mortality. Am. J. Cardiol. 2015, 116, 1678–1684. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, A.; Alpsoy, S.; Akkoyun, D.Ç.; Degirmenci, H.; Güler, N. Heart rate recovery may predict the presence of coronary artery disease. Anadolu. Kardiyol. Derg. 2014, 14, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Bassett, D.R.; Turner, M.J. Exaggerated blood pressure response to maximal exercise in endurance-trained individuals. Am. J. Hypertens 1996, 9, 1099–1103. [Google Scholar] [CrossRef][Green Version]
- Martin, W.H.; Ogawa, T.; Kohrt, W.M.; Malley, M.T.; Korte, E.; Kieffer, P.S.; Schechtman, K.B. Effects of aging, gender, and physical training on peripheral vascular function. Circulation 1991, 84, 654–664. [Google Scholar] [CrossRef]
- Daida, H.; Allison, T.G.; Squires, R.W.; Miller, T.D.; Gau, G.T. Peak exercise blood pressure stratified by age and gender in apparently healthy subjects. Mayo. Clin. Proc. 1996, 71, 445–452. [Google Scholar] [CrossRef]
- López Chicharro, J.L.; Vaquero, A.F. Physiology of Exercise; Editorial Médica Panamericana: Madrid, Spain, 2006. [Google Scholar]
- Bermúdez, C. Valoración de la presión arterial en la ergometría. Rev. Urug. Cardiol. 2012, 27, 399–404. [Google Scholar]
- Le, V.-V.; Mitiku, T.; Sungar, G.; Myers, J.; Froelicher, V. The blood pressure response to dynamic exercise testing: A systematic review. Prog. Cardiovasc. Dis. 2008, 51, 135–160. [Google Scholar] [CrossRef]
- Ayabe, M.; Aoki, J.; Kumahara, H.; Ishii, K.; Yonei, Y.; Tanaka, H. Effects of Age and Body Mass Index on Accuracy of Simple Moderate Vigorous Physical Activity Monitor Under Controlled Condition. Anti Aging Med. 2011, 8, 31–47. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Group | n | Mean | SD | Min | Max | p |
|---|---|---|---|---|---|---|
| Age (years) | ||||||
| CG | 18 | 67.4 | 5.71 | 59 | 75 | 0.370 |
| MICT | 18 | 70 | 8.76 | 55 | 86 | |
| HIICT | 18 | 66.3 | 5.44 | 57 | 76 | |
| Body Mass Index (kg/m2) | ||||||
| CG | 18 | 31.2 | 4.89 | 20.9 | 38.4 | 0.689 |
| MICT | 18 | 30.1 | 3.08 | 24.3 | 35.9 | |
| HIICT | 18 | 30.4 | 4.13 | 35.2 | 37.7 | |
| Maximal Oxygen Consumption estimated (ml/kg/min) | ||||||
| CG | 18 | 26.8 | 5.17 | 15.5 | 39.0 | 0.065 |
| MICT | 18 | 25.0 | 5.57 | 15.5 | 33.1 | |
| HIICT | 18 | 26.1 | 5.63 | 18.4 | 36.1 | |
| Heart Rate peak (bpm) | ||||||
| CG | 18 | 144.94 | 15.4 | 108 | 170 | 0.719 |
| MICT | 18 | 150.78 | 22.6 | 119 | 193 | |
| HIICT | 18 | 148.83 | 17.7 | 93 | 173 | |
| Heart Rate recovery (bpm) | ||||||
| CG | 18 | 79.5 | 8.1 | 68.2 | 91.3 | <0.001 |
| MICT | 18 | 85 | 14.3 | 60.5 | 121 | |
| HIICT | 18 | 100 | 53.0 | 54.8 | 296 | |
| Systolic Blood Pressure exercise (mmHg) | ||||||
| CG | 18 | 184 | 23.50 | 146 | 210 | 0.008 |
| MICT | 18 | 185 | 10.80 | 170 | 210 | |
| HIICT | 18 | 179 | 9.67 | 160 | 200 | |
| Diastolic Blood Pressure exercise (mmHg) | ||||||
| CG | 18 | 76.9 | 13.2 | 50 | 95 | 0.003 |
| MICT | 18 | 56.9 | 9.3 | 40 | 75 | |
| HIICT | 18 | 58.3 | 6.9 | 50 | 75 | |
| Systolic Blood Pressure recovery (mmHg) | ||||||
| CG | 18 | 152 | 16.2 | 120 | 175 | 0.042 |
| MICT | 18 | 156 | 13.6 | 140 | 190 | |
| HIICT | 18 | 151 | 11.7 | 135 | 180 | |
| Diastolic Blood Pressure recovery (mmHg) | ||||||
| CG | 18 | 73.3 | 7.28 | 65 | 90 | 0.001 |
| MICT | 18 | 73.9 | 7.19 | 60 | 85 | |
| HIICT | 18 | 73.9 | 5.02 | 65 | 80 | |
| Maximal speed reached during treadmill test (m/s) | ||||||
| CG | 18 | 4.94 | 0.809 | 3.2 | 6.7 | 0.054 |
| MICT | 18 | 4.66 | 0.899 | 3.2 | 5.9 | |
| HIICT | 18 | 4.86 | 0.910 | 3.7 | 6.4 | |
| Group | Increment | ANCOVA interactions (F, p, ES η²) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (ITT) | n (treated) | Mean | SD | Training x Group | Training x Baseline | Training x Age | |||||||
| F | p | ES η² | F | p | ES η² | F | p | ES η² | |||||
| Maximal Oxygen Consumption estimated (ml/kg/min) | |||||||||||||
| CG | 18 | 12 | −0.80 | −0.31 | 7.36 | 0.002 1,2 | 0.224 | 13.60 | <0.001 | 0.171 | 0.11 | 0.742 | 0.002 |
| MICT | 18 | 12 | 1.90 | −0.85 | |||||||||
| HIICT | 18 | 17 | 3.40 | 0.12 | |||||||||
| Heart Rate peak (bpm) | |||||||||||||
| CG | 18 | 12 | −4.33 | −0.06 | 3.26 | 0.474 | 0.002 | 2.56 | 0.115 | 0.043 | 8.18 | 0.006 | 0.070 |
| MICT | 18 | 12 | −0.72 | −4.70 | |||||||||
| HIICT | 18 | 17 | −4.72 | 2.61 | |||||||||
| Heart Rate recovery (bpm) | |||||||||||||
| CG | 18 | 12 | 0.81 | 0.00 | 1.92 | 0.156 | 0.070 | 37.844 | <0.001 | 0.426 | 0.039 | 0.844 | 0.001 |
| MICT | 18 | 12 | −0.34 | −3.65 | |||||||||
| HIICT | 18 | 17 | −19.85 | −40.18 | |||||||||
| Systolic Blood Pressure exercise (mmHg) | |||||||||||||
| CG | 18 | 12 | −15.40 | −7.75 | 3.48 | 0.038 2 | 0.120 | 37.66 | <0.001 | 0.394 | 6.24 | 0.016 | 0.098 |
| MICT | 18 | 12 | −6.39 | 0.24 | |||||||||
| HIICT | 18 | 17 | −3.06 | −3.52 | |||||||||
| Diastolic Blood Pressure exercise (mmHg) | |||||||||||||
| CG | 18 | 12 | −12.78 | −5.10 | 17.4 | <0.001 1,2 | 0.405 | 8.37 | <0.001 | 0.086 | 1.19 | 0.281 | 0.014 |
| MICT | 18 | 12 | 7.50 | 0.28 | |||||||||
| HIICT | 18 | 17 | 5.00 | −0.68 | |||||||||
| Systolic Blood Pressure recovery (mmHg) | |||||||||||||
| CG | 18 | 12 | −6.39 | −4.70 | 0.0587 | 0.943 | 0.002 | 76.01 | <0.001 | 0.589 | 13.332 | <0.001 | 0.207 |
| MICT | 18 | 12 | −5.84 | −6.86 | |||||||||
| HIICT | 18 | 17 | −6.95 | −6.21 | |||||||||
| Diastolic Blood Pressure recovery (mmHg) | |||||||||||||
| CG | 18 | 12 | 1.39 | −2.00 | 0.0540 | 0.947 | 0.002 | 73.137 | <0.001 | 0.592 | 5.3698 | 0.025 | 0.097 |
| MICT | 18 | 12 | 1.11 | −2.04 | |||||||||
| HIICT | 18 | 17 | 2.22 | −0.30 | |||||||||
| Maximal speed reached during treadmill test (m/s) | |||||||||||||
| CG | 18 | 12 | −0.08 | −0.01 | 7.68 | 0.001 1,2 | 0.231 | 10.28 | 0.023 | 0.134 | 0.317 | 0.575 | 0.005 |
| MICT | 18 | 12 | 0.51 | −0.14 | |||||||||
| HIICT | 18 | 17 | 0.20 | 0.07 | |||||||||
| Body Mass Index (kg/m2) | |||||||||||||
| CG | 18 | 12 | 0.30 | −0.05 | 6.99 | 0.002 2 | 0.215 | 3.02 | 0.088 | 0.046 | 0.217 | 0.643 | 0.003 |
| MICT | 18 | 12 | −0.10 | 1.47 | |||||||||
| HIICT | 18 | 17 | −0.30 | 0.47 | |||||||||
| Variables | Pre-training | Post-Training | p | 95% CI for MD | Cohen’s d | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | Lower | Upper | |||
| Maximal Oxygen Consumption estimated (mL/kg/min) | ||||||||||
| CG | 18 | 26.8 | 5.17 | 12 | 26.00 | 4.86 | 0.288 | −0.753 | 2.386 | 0.14 |
| MICT | 18 | 25.0 | 5.57 | 12 | 26.90 | 4.72 | 0.010 | −3.378 | −0.541 | 0.32 |
| HIICT | 18 | 26.1 | 5.63 | 17 | 29.50 | 5.75 | <0.001 | −3.968 | −0.441 | 0.58 |
| Heart Rate peak (bpm) | ||||||||||
| CG | 18 | 144.94 | 15.41 | 12 | 140.61 | 15.35 | 0.066 | −0.316 | 8.983 | 0.26 |
| MICT | 18 | 150.78 | 22.64 | 12 | 150.06 | 17.94 | 0.770 | −4.408 | 5.853 | 0.03 |
| HIICT | 18 | 148.83 | 17.76 | 17 | 144.11 | 20.37 | 0.125 | −1.444 | 10.888 | 0.25 |
| Heart Rate recovery (bpm) | ||||||||||
| CG | 18 | 79.54 | 8.13 | 12 | 80.35 | 8.13 | 0.669 | −4.737 | 3.117 | 0.09 |
| MICT | 18 | 85.01 | 14.32 | 12 | 84.67 | 10.67 | 0.916 | −6.204 | 6.871 | 0.02 |
| HIICT | 18 | 100.16 | 52.98 | 17 | 80.31 | 12.80 | 0.105 | −4.629 | 44.327 | 0.36 |
| Systolic Blood Pressure exercise (mmHg) | ||||||||||
| CG | 18 | 184.28 | 23.52 | 12 | 168.88 | 15.77 | 0.002 | 6.335 | 24.442 | 0.58 |
| MICT | 18 | 185.00 | 10.84 | 12 | 178.61 | 11.08 | 0.015 | 1.430 | 11.347 | 0.55 |
| HIICT | 18 | 178.61 | 9.67 | 17 | 175.55 | 6.15 | 0.213 | −1.927 | 8.038 | 0.30 |
| Diastolic Blood Pressure exercise (mmHg) | ||||||||||
| CG | 18 | 76.94 | 13.18 | 12 | 64.16 | 8.08 | 0.002 | 5.186 | 20.368 | 0.90 |
| MICT | 18 | 56.94 | 9.25 | 12 | 64.44 | 9.53 | 0.002 | −11.699 | −3.300 | 0.75 |
| HIICT | 18 | 58.33 | 6.86 | 17 | 63.33 | 6.18 | 0.003 | −8.075 | −1.925 | 0.69 |
| Systolic Blood Pressure recovery (mmHg) | ||||||||||
| CG | 18 | 151.94 | 16.19 | 12 | 145.55 | 11.49 | 0.020 | 1.145 | 11.632 | 0.37 |
| MICT | 18 | 155.56 | 13.60 | 12 | 149.72 | 6.74 | 0.019 | 1.065 | 10.600 | 0.40 |
| HIICT | 18 | 151.11 | 11.70 | 17 | 144.16 | 5.49 | 0.028 | 0.845 | 13.043 | 0.57 |
| Diastolic Blood Pressure recovery (mmHg) | ||||||||||
| CG | 18 | 73.33 | 7.27 | 12 | 74.72 | 5.27 | 0.462 | −5.279 | 2.501 | 0.18 |
| MICT | 18 | 73.89 | 7.18 | 12 | 75.00 | 5.14 | 0.570 | −2.258 | 2.703 | 0.14 |
| HIICT | 18 | 73.89 | 5.01 | 17 | 76.11 | 4.71 | 0.215 | −5.862 | 1.418 | 0.42 |
| Maximal speed reached during treadmill test (m/s) | ||||||||||
| CG | 18 | 4.94 | 0.80 | 12 | 4.86 | 0.79 | 0.448 | −0.143 | 0.309 | 0.09 |
| MICT | 18 | 4.47 | 0.90 | 12 | 4.98 | 0.77 | 0.015 | −0.544 | −0.067 | 0.53 |
| HIICT | 18 | 5.21 | 0.82 | 17 | 5.41 | 0.89 | 0.001 | −0.685 | −0.203 | 0.23 |
| Body Mass Index (kg/m2) | ||||||||||
| CG | 18 | 31.2 | 4.89 | 12 | 31.5 | 5.05 | 0.019 | −0.52 | −0.53 | 0.06 |
| MICT | 18 | 30.1 | 3.08 | 12 | 30.0 | 3.15 | 0.140 | −0.02 | 0.29 | 0.03 |
| HIICT | 18 | 30.4 | 4.13 | 17 | 30.1 | 4.24 | 0.035 | 0.02 | 0.60 | 0.07 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballesta-García, I.; Martínez-González-Moro, I.; Ramos-Campo, D.J.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1805. https://doi.org/10.3390/ijerph17051805
Ballesta-García I, Martínez-González-Moro I, Ramos-Campo DJ, Carrasco-Poyatos M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(5):1805. https://doi.org/10.3390/ijerph17051805
Chicago/Turabian StyleBallesta-García, Ismael, Ignacio Martínez-González-Moro, Domingo J Ramos-Campo, and María Carrasco-Poyatos. 2020. "High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 5: 1805. https://doi.org/10.3390/ijerph17051805
APA StyleBallesta-García, I., Martínez-González-Moro, I., Ramos-Campo, D. J., & Carrasco-Poyatos, M. (2020). High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(5), 1805. https://doi.org/10.3390/ijerph17051805