Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol

 , and
, and
Abstract
1. Introduction
Research Objectives
- Identify adaptations to improve the content and structure of the study protocol in cooperative consensus processes with expert clinicians and researchers in the area of memory assessment.
- Identify possibilities for refinement of the assessment procedures based on investigations of uncertainties concerning the interplay between TUGdt administration and participants’ responses to the assessment instructions by the use of video-recorded test performances.
- Explore potentially useful TUGdt outcome measures based on TUGdt assessments of a small sample of individuals attending a specialist clinic for memory assessment.
2. Material and Methods
2.1. Study Design
2.2. Ethical Approval and Patients’ Consent to Participate
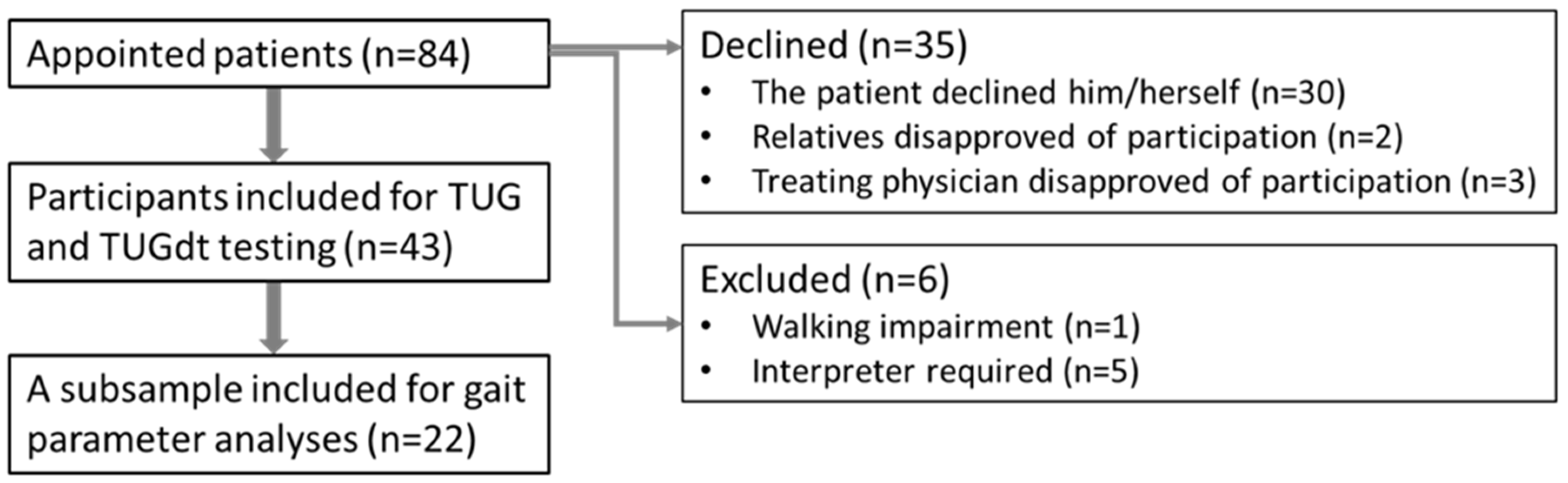
2.3. Pilot Setting and Participating Patients
2.4. Pilot Test Procedures, Data Collection and Analyses
2.5.1. Timed Up-and-Go and Timed Up-and-Go dual-task tests
2.5.2. Analyses
2.5.3. Statistical Analyses
3. Results
3.1. Identification of Possible Refinements of the Study Protocol and Assessment Procedures
3.2. Explorations of the TUGdt Outcome Measures
3.3. Interpretations of Pilot Results and Development of the UDDGait Protocol
3.3.1. The Refined Protocol for the Large-Scale UDDGait Study
3.3.2. Statistical Power Calculation for the UDDGait-Protocol
4. Discussion
5. Study Limitations and Strengths
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Data Collection of Timed Up-and-Go (TUG) and Two Types of TUG Dual Task (TUGdt): TUGdt Animals and TUGdt Months
Appendix A.1.1. TUG and TUGdt Tests
Appendix A.1.2. Two TUGdt Tests
Appendix A.1.3. TUG Test
- Pre-trial: The participant performs the TUG test once without timing: “You can try now”. If necessary, supplementary instructions are given while the participant is performing the trial test.
- TUG single-task (timed): The following instructions are given to the participant immediately before the test is performed: “When I say start, you should rise up, walk towards the line, cross the line, turn back, walk back and sit down in the chair. You should walk normally, as you usually do, at your own pace. Are you ready?” After an affirmative answer, the assessor says: “You can start now”. Timing starts when the participant’s back leaves the chair back and ends when the participant’s posterior touches the seat. Oral clues are provided if necessary and noted in the minutes (see below: IMPORTANT).
- TUG dual-task (Animals): The following instructions are given to the participant “You should do what you just did, but at the same time as you walk, please name different animals aloud. You can choose any animals you want. If you get stuck and cannot think of any animals, just keep walking like you just did now”.Answer any questions.Ask the question: “Are you ready?”. After an affirmative answer, the assessor says: “You can start now”. The assessor times the performance. (The number of different animals is extracted from the video recordings).
- TUG dual-task (Months): The following instructions are given to the participant “You should do what you just did, but at the same time as you walk, please recite the months of the year in reverse order. So you should start with the last month. If you get stuck and do not know what month to say, just keep walking like you just did now. You don’t have to recite all of the months”.Answer any questions.Ask the question: “Are you ready?”. After an affirmative answer, the assessor says: “You can start now”. The assessor times the performance. (The number of months in correct order is extracted from the video recordings).
Appendix A.2. Important Considerations
- Briefly answer questions about the execution.
- Give the instruction “turn”, if the person does not turn when passing the floor marking but walks straight ahead towards the camera in front.
- Give the instruction “sit down” if the person on the way back stops next to the chair and remains standing.
- If the participant slows down or makes short stops (≤10 s) at other times during the test, no encouraging instructions are given.
- In cases where the person has obviously forgotten what to do, or expresses that s/he cannot perform the test, encouragement to continue walking is given.
References
- Saxena, S.; Wortmann, M. Dementia: A Public Health Priority; World Health Organization and Alzheimer’s Disease International, WHO Press: Geneva, Switzerland, 2012; p. 103. Available online: https://www.who.int/mental_health/publications/dementia_report_2012/en/ (accessed on 20 December 2019).
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, M.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Garcia-Ptacek, S.; Eriksdotter, M.; Jelic, V.; Porta-Etessam, J.; Kåreholt, I.; Manzano Palomo, S. Subjective cognitive impairment: Towards early identification of Alzheimer disease. Neurologia 2016, 31, 562–571. [Google Scholar] [CrossRef]
- Shim, H.; Kim, M.; Won, C.W. Motoric cognitive risk syndrome is associated with processing speed and executive function, but not delayed free recall memory: The Korean frailty and aging cohort study (KFACS). Arch. Gerontol. Geriatr. 2019, 87, 103990. [Google Scholar] [CrossRef]
- Verghese, J.; Ayers, E.; Barzilai, N.; Bennett, D.A.; Buchman, A.S.; Holtzer, R.; Katz, M.J.; Lipton, R.B.; Wang, C. Motoric cognitive risk syndrome: Multicenter incidence study. Neurology 2014, 83, 2278–2284. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Bryce, R.; Ferri, C. World Alzheimer Report 2011. The Benefit of Eraly Diagnos and Intervention; Alzheimer’s Deasease International, King’s College: London, UK, 2011; Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2011.pdf (accessed on 20 December 2019).
- Lin, J.S.; O’Connor, E.; Rossom, R.C.; Perdue, L.A.; Eckstrom, E. Screening for cognitive impairment in older adults: A systematic review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2013, 159, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lee, S.J.; Seo, H.J.; Lee, D.Y.; Moon, S.H. Effects of a Dementia Screening Program on Healthcare Utilization in South Korea: A Difference-In-Difference Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3837. [Google Scholar] [CrossRef]
- Nieuwenhuis-Mark, R.E. The death knoll for the MMSE: Has it outlived its purpose? J. Geriatr. Psychiatry Neurol. 2010, 23, 151–157. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué I Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015, 3, CD010783. [Google Scholar]
- Allali, G.; Annweiler, C.; Blumen, H.M.; Callisaya, M.L.; De Cock, A.M.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.P.; Verghese, J.; Beauchet, O. Gait phenotype from mild cognitive impairment to moderate dementia: Results from the GOOD initiative. Eur. J. Neurol. 2016, 23, 527–541. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Verghese, J.; Beauchet, O.; Hausdorff, J.M. Gait and cognition: A complementary approach to understanding brain function and the risk of falling. J. Am. Geriatr. Soc. 2012, 60, 2127–2136. [Google Scholar] [CrossRef] [PubMed]
- Valkanova, V.; Ebmeier, K.P. What can gait tell us about dementia? Review of epidemiological and neuropsychological evidence. Gait Posture 2017, 53, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Kikkert, L.H.J.; Vuillerme, N.; van Campen, J.P.; Hortobágyi, T.; Lamoth, C.J. Walking ability to predict future cognitive decline in old adults: A scoping review. Ageing Res. Rev. 2016, 27, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Katsumata, Y.; Todoriki, H.; Yasura, S.; Dodge, H.H. Timed up and go test predicts cognitive decline in healthy adults aged 80 and older in Okinawa: Keys to Optimal Cognitive Aging (KOCOA) Project. J. Am. Geriatr. Soc. 2011, 59, 2188–2189. [Google Scholar] [CrossRef]
- McGough, E.L.; Kelly, V.E.; Logsdon, R.G.; McCurry, S.M.; Cochrane, B.B.; Engel, J.M.; Teri, L. Associations between physical performance and executive function in older adults with mild cognitive impairment: Gait speed and the timed “up & go” test. Phys. Ther. 2011, 91, 1198–1207. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Ries, J.D.; Echternach, J.L.; Nof, L.; Gagnon Blodgett, M. Test-retest reliability and minimal detectable change scores for the timed “up & go” test, the six-minute walk test, and gait speed in people with Alzheimer disease. Phys. Ther. 2009, 89, 569–579. [Google Scholar]
- Bridenbaugh, S.A.; Kressig, R.W. Quantitative gait disturbances in older adults with cognitive impairments. Curr. Pharm. Des. 2014, 20, 3165–3172. [Google Scholar] [CrossRef]
- Cedervall, Y.; Halvorsen, K.; Aberg, A.C. A longitudinal study of gait function and characteristics of gait disturbance in individuals with Alzheimer’s disease. Gait Posture 2014, 39, 1022–1027. [Google Scholar] [CrossRef]
- Theill, N.; Martin, M.; Schumacher, V.; Bridenbaugh, S.A.; Kressig, R.W. Simultaneously measuring gait and cognitive performance in cognitively healthy and cognitively impaired older adults: The Basel motor-cognition dual-task paradigm. J. Am. Geriatr. Soc. 2011, 59, 1012–1018. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Almeida, Q.J.; Bherer, L.; Burhan, A.M.; Camicioli, R.; Doyon, J.; Fraser, S.; Muir-Hunter, S.; Li, K.Z.H.; Liu-Ambrose, T.; et al. Consensus on Shared Measures of Mobility and Cognition: From the Canadian Consortium on Neurodegeneration in Aging (CCNA). J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 897–909. [Google Scholar] [CrossRef] [PubMed]
- MacAulay, R.K.; Wagner, M.T.; Szeles, D.; Milano, N.J. Improving Sensitivity to Detect Mild Cognitive Impairment: Cognitive Load Dual-Task Gait Speed Assessment. J. Int. Neuropsychol. Soc. 2017, 23, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Speechley, M.; Wells, J.; Borrie, M.; Gopaul, K.; Montero-Odasso, M. Gait assessment in mild cognitive impairment and Alzheimer’s disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture 2012, 35, 96–100. [Google Scholar] [CrossRef]
- De Cock, A.M.; Fransen, E.; Perkisas, S.; Verhoeven, V.; Beauchet, O.; Vandewoude, M.; Remmen, R. Comprehensive Quantitative Spatiotemporal Gait Analysis Identifies Gait Characteristics for Early Dementia Subtyping in Community Dwelling Older Adults. Front. Neurol. 2019, 10, 313. [Google Scholar] [CrossRef]
- Montero-Odasso, M. Gait as a biomarker of cognitive impairment and dementia syndromes. Quo vadis? Eur. J. Neurol. 2016, 23, 437–438. [Google Scholar] [CrossRef]
- Montero-Odasso, M.M.; Sarquis-Adamson, Y.; Speechley, M.; Borrie, M.J.; Hachinski, V.C.; Wells, J.; Riccio, P.M.; Schapira, M.; Sejdic, E.; Camicioli, R.M.; et al. Association of Dual-Task Gait With Incident Dementia in Mild Cognitive Impairment: Results From the Gait and Brain Study. JAMA Neurol. 2017, 74, 857–865. [Google Scholar] [CrossRef]
- Lima, L.C.; Ansai, J.H.; Andrade, L.P.; Takahashi, A.C. The relationship between dual-task and cognitive performance among elderly participants who exercise regularly. Braz. J. Phys. Ther. 2015, 19, 159–166. [Google Scholar] [CrossRef]
- Borges Sde, M.; Radanovic, M.; Forlenza, O.V. Functional mobility in a divided attention task in older adults with cognitive impairment. J. Mot. Behav. 2015, 47, 378–385. [Google Scholar] [CrossRef]
- Cedervall, Y.; Kilander, L.; Aberg, A.C. Declining physical capacity but maintained aerobic activity in early Alzheimer’s disease. Am. J. Alzheimers Dis. Other Dement. 2012, 27, 180–187. [Google Scholar] [CrossRef]
- Gillain, S.; Warzee, E.; Lekeu, F.; Wojtasik, V.; Maquet, D.; Croisier, J.L.; Salmon, E.; Petermans, J. The value of instrumental gait analysis in elderly healthy, MCI or Alzheimer’s disease subjects and a comparison with other clinical tests used in single and dual-task conditions. Ann. Phys. Rehabil. Med. 2009, 52, 453–474. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, G.A.; Thabane, L. Guidelines for reporting non-randomised pilot and feasibility studies. Pilot Feasibility Stud. 2019, 5, 114. [Google Scholar] [CrossRef] [PubMed]
- Åberg, A.C.; Lindmark, B.; Lithell, H. Evaluation and application of the General Motor Function assessment scale in geriatric rehabilitation. Disabil. Rehabil. 2003, 25, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Åberg, A.C.; Lindmark, B.; Lithell, H. Development and reliability of the General Motor Function Assessment Scale (GMF)—A performance-based measure of function-related dependence, pain and insecurity. Disabil. Rehabil. 2003, 25, 463–472. [Google Scholar] [CrossRef]
- Solomon, P.R.; Pendlebury, W.W. Recognition of Alzheimer’s disease: The 7 Minute Screen. Fam. Med. 1998, 30, 265–271. [Google Scholar]
- Henry, J.D.; Crawford, J.R.; Phillips, L.H. Verbal fluency performance in dementia of the Alzheimer’s type: A meta-analysis. Neuropsychologia 2004, 42, 1212–1222. [Google Scholar] [CrossRef]
- Vaughan, R.M.; Coen, R.F.; Kenny, R.; Lawlor, B.A. Semantic and Phonemic Verbal Fluency Discrepancy in Mild Cognitive Impairment: Potential Predictor of Progression to Alzheimer’s Disease. J. Am. Geriatr. Soc. 2018, 66, 755–759. [Google Scholar] [CrossRef]
- Tallberg, I.M.; Ivachova, E.; Jones Tinghag, K.; Ostberg, P. Swedish norms for word fluency tests: FAS, animals and verbs. Scand. J. Psychol. 2008, 49, 479–485. [Google Scholar] [CrossRef]
- Cullen, S.; Montero-Odasso, M.; Bherer, L.; Almeida, Q.; Fraser, S.; Muir-Hunter, S.; Li, K.; Liu-Ambrose, T.; McGibbon, C.A.; McIlroy, W.; et al. Guidelines for Gait Assessments in the Canadian Consortium on Neurodegeneration in Aging (CCNA). Can. Geriatr. J. 2018, 21, 157–165. [Google Scholar] [CrossRef]
- Parihar, R.; Mahoney, J.R.; Verghese, J. Relationship of Gait and Cognition in the Elderly. Curr. Transl. Geriatr. Exp. Gerontol. Rep. 2013, 2. [Google Scholar] [CrossRef]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Bohannon, R.W. Standing balance, lower extremity muscle strength, and walking performance of patients referred for physical therapy. Percept. Mot. Skills 1995, 80, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Ostberg, P.; Hansson, V.; Haagg, S. Adult norms and test-retest reliability for the Months Backward test: Durational and response accuracy measures. Logoped. Phoniatr. Vocol. 2012, 37, 11–17. [Google Scholar] [CrossRef]
- Lancaster, G.A. Pilot and feasibility studies come of age! Pilot Feasibility Stud. 2015, 1, 1. [Google Scholar] [CrossRef]
- Lemke, N.C.; Wiloth, S.; Werner, C.; Hauer, K. Validity, test-retest reliability, sensitivity to change and feasibility of motor-cognitive dual task assessments in patients with dementia. Arch. Gerontol. Geriatr. 2017, 70, 169–179. [Google Scholar] [CrossRef]
- Verghese, J.; Wang, C.; Holtzer, R. Relationship of clinic-based gait speed measurement to limitations in community-based activities in older adults. Arch. Phys. Med. Rehabil. 2011, 92, 844–846. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Simonsen, A.H.; Siersma, V.; Hasselbalch, S.G.; Hoegh, P. The Diagnostic and Prognostic Value of a Dual-Tasking Paradigm in a Memory Clinic. J. Alzheimers Dis. 2018, 61, 1189–1199. [Google Scholar] [CrossRef]
- Lundin-Olsson, L.; Nyberg, L.; Gustafson, Y. "Stops walking when talking" as a predictor of falls in elderly people. Lancet 1997, 349, 617. [Google Scholar] [CrossRef]
- Hauer, K.; Oster, P. Measuring functional performance in persons with dementia. J. Am. Geriatr. Soc. 2008, 56, 949–950. [Google Scholar] [CrossRef]
- Viteckova, S.; Cejka, V.; Dusek, P.; Krupicka, R.; Kutilek, P.; Szabo, Z.; Růžička, E. Extended Timed Up & Go test: Is walking forward and returning back to the chair equivalent gait? J. Biomech. 2019, 89, 110–114. [Google Scholar] [PubMed]
- Åhman, H.B.; Giedraitis, V.; Cedervall, Y.; Lennhed, B.; Berglund, L.; McKee, K.; Kilander, L.; Rosendahl, E.; Ingelsson, M.; Åberg, A.C. Dual-Task Performance and Neurodegeneration: Correlations Between Timed Up-and-Go Dual-Task Test Outcomes and Alzheimer’s Disease Cerebrospinal Fluid Biomarkers. J. Alzheimers Dis. 2019, 71, S75–S83. [Google Scholar] [CrossRef] [PubMed]
- Åhman, H.B.; Cedervall, Y.; Kilander, L.; Giedraitis, V.; Berglund, L.; McKee, K.; Rosendahl, E.; Ingelsson, M.; Åberg, A.C. Dual-Task Test Outcomes Discriminate between Dementia Disorder, Cognitive Impairment Diagnoses, and Healthy Controls. BMC Geriatrics 2020. under review for publication. [Google Scholar]
- Cao, Z.; Hidalgo Martinez, G.; Simon, T.; Wei, S.E.; Sheikh, Y.A. OpenPose: Realtime multi-person 2D pose estimation using Part Affinity Fields. arXiv 2018, arXiv:1812.08008. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Dementia Diagnosis | No Dementia Diagnosis | All | |
|---|---|---|---|
| Total sample (n) | 25 | 18 | 43 |
| Age (years), Md (range) | 77 (59–87) | 72 (58–83) | 74 (58–87) |
| Female n, (%) | 10 (40) | 7(38) | 17 (37) |
| MMSE (scores), Md (range) | 22 (20–24) | 26 (21–29) | 22 (20–27) |
| Sub-sample (n) | 10 | 12 | 22 |
| Age (years), Md (range) | 78 (62–87) | 70 (58–76) | 71 (58–87) |
| Female n, (%) | 4 (40) | 6 (50) | 10 (45.5) |
| MMSE (scores), Md (range) | 20.0 (15–27) | 27.5 (19–30) | 26.0 (15–30) |
| Mobility- | A) Observations of Deviant Performance | B) Verification Protocol (Based on A) | ||
|---|---|---|---|---|
| Sequence | Mobility | Verbal | Normal Performance | Deviant Performance |
| Initiation and rising up from the chair | Starts during the instructions Rises and stands still/ and asks: Shall I start at once? | Asks: Shall I start with the animals?/Shall I say it out loud? | Starts after finished instructions Rises and starts walking | Asks about the verbal and/or mobility performance at the start |
| Walking 3 m to the line | Stops walking Stops walking before the line Stops after the turn Asks: Shall I turn? | Tells a story about animals Asks: Shall I talk about the animals now? | Walks without any stops | Stands still >1 s. |
| Line crossing and turning | Turns before the line/with one foot on/two feet on the line Wide turn Walks (2 m) up to the camera before turning Asks: Shall I turn here? | Passes the line. Turns with at least one foot over the line | No foot over the line More than two stances (i.e., more than one step) before the turn is initiated Stands still >1 s. | |
| Walking back 3 m to chair | Stops walking | Asks: Shall I say the same thing now? | Walks without any stops to the chair and turns (to sit down) | Stands still >1 s. |
| Sitting down on chair | Walks to/past the chair and stands still Asks: Shall I sit down? / Is this enough? | Sits down spontaneously | Does not spontaneously sit down Walks past the chair | |
| General | Discontinues the test | Says nothing, i.e., no animals Small talk | Names animals Verbal hesitation or correction of words Small talk combined with naming animals | Says nouns that are not animals Says nothing Discontinues the test Asks questions about the mobility or verbal tasks during the test |
| Variable | With Dementia (N = 10) | No Dementia (N = 12) | Adjusted p-Value * | ||||
|---|---|---|---|---|---|---|---|
| Min | Md | Max | Min | Md | Max | ||
| TUG time (s) | 10.4 | 18.1 | 30.2 | 7.5 | 14.4 | 19.4 | 0.342 |
| TUGdt time (s) | 13.9 | 28.7 | 55.0 | 10.2 | 17.6 | 41.9 | 0.149 |
| TUGdt cost (%) | 15.3 | 37.8 | 217.6 | 1.0 | 27.3 | 115.9 | 0.972 |
| TUGdt animals before turning (n) | 1 | 3 | 7 | 0 | 4 | 6 | 0.418 |
| TUGdt animals after turning (n) | 0 | 1 | 3 | 0 | 3.5 | 5 | 0.045 |
| TUGdt animals difference after/before turning (n) | −5 | −2 | 0 | −4 | −1.5 | 5 | 0.418 |
| TUGdt animals per 10 (s) | 0.76 | 1.8 | 4.3 | 1.3 | 4.9 | 8.2 | 0.245 |
| TUG SL before turning (m) | 0.251 | 0.415 | 0.625 | 0.431 | 0.588 | 0.746 | 0.149 |
| TUG SL after turning (m) | 0.254 | 0.386 | 0.637 | 0.351 | 0.534 | 0.704 | 0.342 |
| TUG SL difference after/before turning (m) | −0.175 | −0.017 | 0.012 | −0.222 | −0.020 | 0.084 | 0.597 |
| TUGdt SL before turning (m) | 0.215 | 0.385 | 0.593 | 0.353 | 0.568 | 0.718 | 0.062 |
| TUGdt SL after turning (m) | 0.236 | 0.373 | 0.605 | 0.320 | 0.502 | 0.671 | 0.379 |
| TUGdt SL difference after/before turning (m) | −0.047 | −0.020 | 0.027 | −0.118 | −0.049 | −0.023 | 0.032 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cedervall, Y.; Stenberg, A.M.; Åhman, H.B.; Giedraitis, V.; Tinmark, F.; Berglund, L.; Halvorsen, K.; Ingelsson, M.; Rosendahl, E.; Åberg, A.C. Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol. Int. J. Environ. Res. Public Health 2020, 17, 1715. https://doi.org/10.3390/ijerph17051715
Cedervall Y, Stenberg AM, Åhman HB, Giedraitis V, Tinmark F, Berglund L, Halvorsen K, Ingelsson M, Rosendahl E, Åberg AC. Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol. International Journal of Environmental Research and Public Health. 2020; 17(5):1715. https://doi.org/10.3390/ijerph17051715
Chicago/Turabian StyleCedervall, Ylva, Anna M. Stenberg, Hanna B. Åhman, Vilmantas Giedraitis, Fredrik Tinmark, Lars Berglund, Kjartan Halvorsen, Martin Ingelsson, Erik Rosendahl, and Anna Cristina Åberg. 2020. "Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol" International Journal of Environmental Research and Public Health 17, no. 5: 1715. https://doi.org/10.3390/ijerph17051715
APA StyleCedervall, Y., Stenberg, A. M., Åhman, H. B., Giedraitis, V., Tinmark, F., Berglund, L., Halvorsen, K., Ingelsson, M., Rosendahl, E., & Åberg, A. C. (2020). Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol. International Journal of Environmental Research and Public Health, 17(5), 1715. https://doi.org/10.3390/ijerph17051715