Examining the Impact of Knowledge Mobilization Strategies to Inform Urban Stakeholders on Accessibility: A Mixed-Methods study




Abstract
1. Introduction
1.1. Knowledge Mobilization
1.2. Aim
2. Methods
2.1. Data Collection
2.1.1. Development of the KM Strategies
2.1.2. Evaluation of the KM Strategies
2.2. Data Analyses
3. Findings
3.1. KM Strategies Development and Sharing
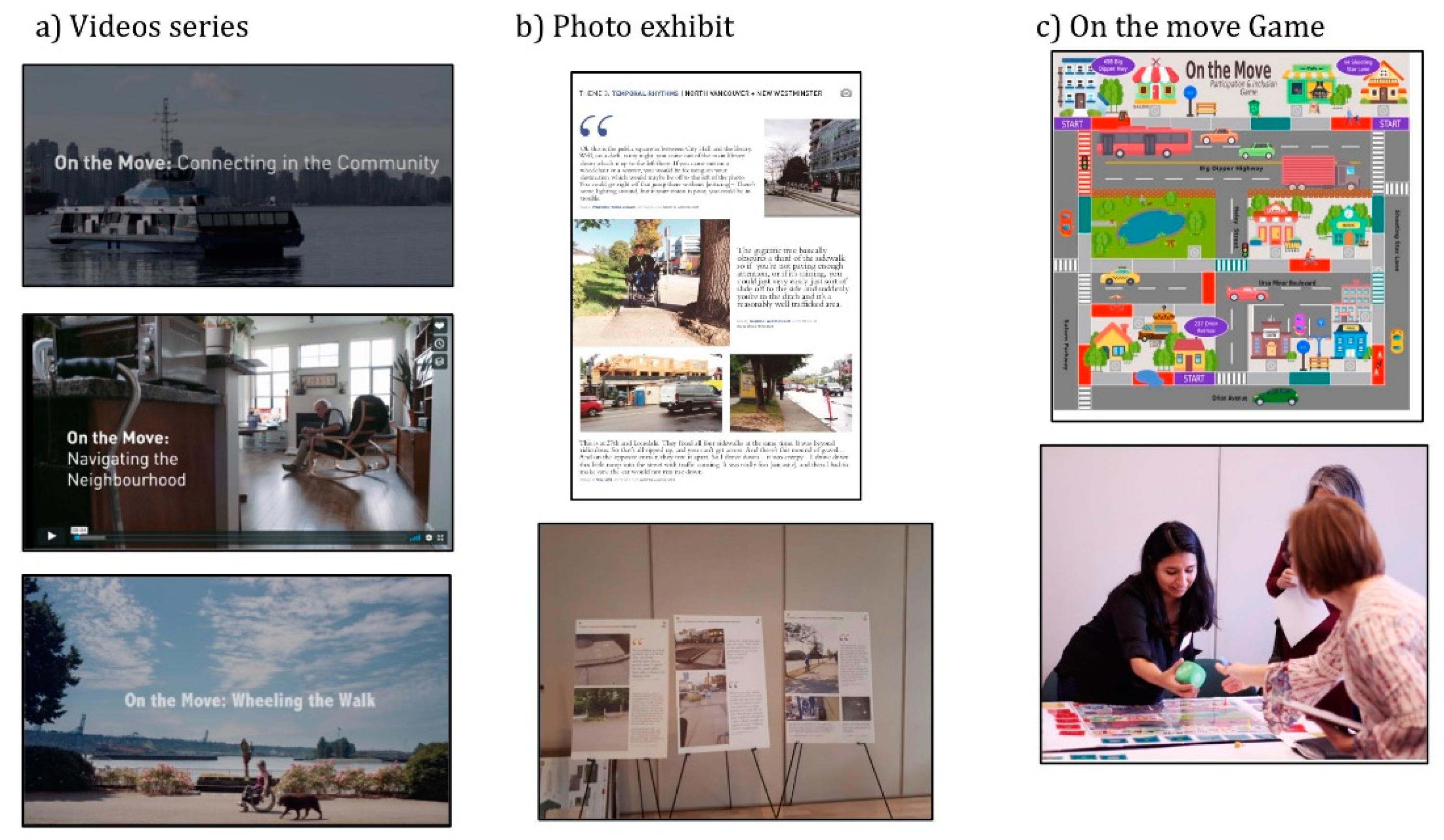
3.1.1. A Video series
3.1.2. Photo Exhibit
3.1.3. Interactive Game
3.2. KM Evaluation
3.2.1. Journal and Observations
3.2.2. Questionnaire
“I think the most valuable aspect of this video is the various perspectives presented on the various access issues the two individuals confront, as well as their words. These help to point out the uniqueness of the individual needs of each user of a mobility device.”(Female caregiver, 66 years of age)
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Disability. 2011. Available online: http://www.who.int/disabilities/world_report/2011/report.pdf (accessed on 11 November 2019).
- United Nations. Convention on the Rights of Persons with Disabilities (CRPD). 2016. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/convention-on-the-rights-of-persons-with-disabilities-2.html (accessed on 28 October 2019).
- Morris, S.; Fawcett, G.; Brisebois, L.; Hughes, J. A Demographic, Employment and Income Profile of Canadians with Disabilities Aged 15 Years and Over, 2017; Statistique Canada: Ottawa, ON, Canada, 2018. [Google Scholar]
- Statistic Canada. Population Size and Growth in Canada: Key Results From the 2016 Census. 2016. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/170208/dq170208a-eng.htm?HPA=1 (accessed on 1 May 2019).
- Heitor, T.; Medeiros, V.; Nascimento, R.; Tomé, A. Investigating accessibility to achieve inclusive environments: The spatial experience of disability at a University Precinct in Lisbon. In Inclusive Designing: Joining Usability, Accessibility, and Inclusion; Langdon, P.M., Lazar, J., Heylighen, A., Dong, H., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 93–103. [Google Scholar]
- Hästbacka, E.; Nygård, M.; Nyqvist, F. Barriers and facilitators to societal participation of people with disabilities: A scoping review of studies concerning European countries. Alter Eur. J. Disabil. Res./Rev. Eur. Recher Handi 2016, 10, 201–220. [Google Scholar] [CrossRef]
- Lid, I.M.; Solvang, P.K. (Dis)ability and the experience of accessibility in the urban environment. Alter Eur. J. Disabil. Res. Rev. Eur. Recher Handi 2016, 10, 181–194. [Google Scholar] [CrossRef]
- United Nations. New Urban Agenda (#A/RES/71/256). 2017. Available online: http://habitat3.org/wp-content/uploads/New-Urban-Agenda-GA-Adopted-68th-Plenary-N1646655-E.pdf (accessed on 4 October 2018).
- Imrie, R.; Luck, R. Designing inclusive environments: Rehabilitating the body and the relevance of universal design. Disabil. Rehabil. 2014, 36, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Rieger, J.; Strickfaden, M. Taken for granted: Material relations between disability and codes/guidelines. Societies 2016, 6, 1–11. [Google Scholar] [CrossRef]
- Meagher, L.; Lyall, C.; Nutley, S. Flows of knowledge, expertise and influence: A method for assessing policy and practice impacts from social science research. Res. Eval. 2008, 17, 163–173. [Google Scholar] [CrossRef]
- Milligan, N.V.; Nieuwenhuijsen, E.R.; Grawi, C.L. Using a participatory action strategic approach to enhance accessibility and participation in arts and cultural events: Results of four focus groups. Disabil. Health J. 2014, 7, 105–113. [Google Scholar] [CrossRef]
- Larkin, H.; Hitch, D.; Watchorn, V.; Ang, S. Working with policy and regulatory factors to implement universal design in the built environment: The Australian experience. Int. J. Environ. Res. Public Health 2015, 12, 8157–8171. [Google Scholar] [CrossRef]
- Lid, I.M. Implementing universal design in a Norwegian context: Balancing core values and practical priorities. Disabil. Stud. Q. 2016, 36, 1–15. [Google Scholar] [CrossRef]
- Boys, J. Doing Disability Differently: An Alternative Handbook on Architecture, Dis/ability and Designing for Everyday Life; Routledge: New York, NY, USA, 2014; 243p. [Google Scholar]
- Steinfeld, E.; Maisel, J. Universal Design: Creating Inclusive Environments; Wiley: Hoboken, NJ, USA, 2012; 408p. [Google Scholar]
- Rains, M.; Butland, R. Lifting the barriers: Planning for increased mobility and accessibility through the Adelaide CBD. In Proceedings of the State of Australian Cities Conference 2013, Sydney, Australia, 26–29 November 2013. [Google Scholar]
- Heylighen, A.; Van der Linden, V.; Van Steenwinkel, I. Ten questions concerning inclusive design of the built environment. Build. Environ. 2017, 114, 507–517. [Google Scholar] [CrossRef]
- LaRocca, R.; Yost, J.; Dobbins, M.; Ciliska, D.; Butt, M. The effectiveness of knowledge translation strategies used in public health: A systematic review. BMC Public Health 2012, 12, 751. [Google Scholar] [CrossRef]
- Newberry, J. Enhancing the Research and Knowledge Mobilization Capacity of Disability Community Organizations. 2017. Available online: http://www.communitybasedresearch.ca/resources/RKM/RKM%20FINAL%20REPORT.pdf (accessed on 8 November 2019).
- Ismail, W.A.W.; Said, I. Integrating the community in urban design and planning of public spaces: A review in Malaysian cities. Procedia Soc. Behav. Sci. 2015, 168, 357–364. [Google Scholar] [CrossRef][Green Version]
- Bromley, R.D.F.; Matthews, D.L.; Thomas, C.J. City centre accessibility for wheelchair users: The consumer perspective and the planning implications. Cities 2007, 24, 229–241. [Google Scholar] [CrossRef]
- Hernandez, B.; Balcazar, F.; Keys, C.; Hidalgo, M.A.; Rosen, J. Taking it to the streets: Ethnic minorities with disabilities seek community inclusion. Community Dev. 2006, 37, 13–25. [Google Scholar] [CrossRef]
- Phipps, D.J.; Jensen, K.E.; Myers, J.G. Applying social sciences research for public benefit using knowledge mobilization and social media. In Theoretical and Methodological Approaches to Social Sciences and Knowledge Management; Azcárate, A.L.-V., Ed.; InTech: Rijeka, Croatia, 2012; pp. 167–197. [Google Scholar]
- Kapucu, N. Community-Based research in generating usable knowledge for public policy and administration. Adm. Soc. 2016, 48, 683–710. [Google Scholar] [CrossRef]
- Dobbins, M.; Rosenbaum, P.; Plews, N.; Law, M.; Fysh, A. Information transfer: What do decision makers want and need from researchers? Implement. Sci. 2007, 2, 1–12. [Google Scholar] [CrossRef]
- Ferguson, L.; Chan, S.; Santelmann, M.; Tilt, B. Exploring participant motivations and expectations in a researcher-stakeholder engagement process: Willamette Water 2100. Landsc. Urban Plan. 2017, 157, 447–456. [Google Scholar] [CrossRef]
- Oliver, K.; Innvar, S.; Lorenc, T.; Woodman, J.; Thomas, J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv. Res. 2014, 14, 751. [Google Scholar] [CrossRef]
- Gainforth, H.L.; Latimer-Cheung, A.E.; Athanasopoulos, P.; Ginis, K.A.M. Examining the effectiveness of a knowledge mobilization initiative for disseminating the physical activity guidelines for people with spinal cord injury. Disabil. Health J. 2013, 6, 260–265. [Google Scholar] [CrossRef]
- Phillipson, J.; Lowe, P.; Proctor, A.; Ruto, E. Stakeholder engagement and knowledge exchange in environmental research. J. Environ. Manag. 2012, 95, 56–65. [Google Scholar] [CrossRef]
- Watchorn, V.; Larkin, H.; Hitch, D.; Ang, S. Promoting participation through the universal design of built environments: Making it happen. J. Soc. Incl. 2014, 5, 65–88. [Google Scholar] [CrossRef]
- Landry, R.; Amara, N.; Lamari, M. Climbing the ladder of research utilization evidence from social science research. Sci. Commun. 2001, 22, 396–422. [Google Scholar] [CrossRef]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Fazey, I.; Bunse, L.; Msika, J.; Pinke, M.; Preedy, K.; Evely, A.C.; Lambert, E.; Hastings, E.; Morris, S.; Reed, M.S. Evaluating knowledge exchange in interdisciplinary and multi-stakeholder research. Glob. Environ. Chang. 2014, 25, 204–220. [Google Scholar] [CrossRef]
- Lavis, J.N.; Robertson, D.; Woodside, J.M.; McLeod, C.B.; Abelson, J. How can research organizations more effectively transfer research knowledge to decision makers? Milbank Q. 2003, 81, 221–248. [Google Scholar] [CrossRef]
- Straus, S.E.; Tetroe, J.; Graham, I.D.; Zwarenstein, M.; Bhattacharyya, O.; Shepperd, S. Monitoring use of knowledge and evaluating outcomes. Can. Med. Assoc. J. 2010, 182, E94–E98. [Google Scholar] [CrossRef]
- Kuah, C.T.; Wong, K.Y. Knowledge management performance measurement: A review. Afr. J. Bus. Manag. 2011, 5, 6021–6027. [Google Scholar] [CrossRef]
- Routhier, F.; Mortenson, W.B.; Demers, L.; Mahmood, A.; Chaudhury, H.; Martin Ginis, K.A.; Miller, W.C. Mobility and participation of people with disabilities using mobility assistive technologies: Protocol for a mixed-methods study. JMIR Res. Protoc. 2019, 8, e12089. [Google Scholar] [CrossRef]
- Barwick, M. Knowledge Translation Planning Template; The Hospital for Sick Children: Toronto, ON, Canada, 2013. [Google Scholar]
- Bowen, S.J.; Graham, I.D. From knowledge translation to engaged scholarship: Promoting research relevance and utilization. Arch. Phys. Med. Rehabil. 2013, 94, S3–S8. [Google Scholar] [CrossRef]
- Lillehagen, I.; Vøllestad, N.; Heggen, K.; Engebretsen, E. Protocol for a qualitative study of knowledge translation in a participatory research project. BMJ Open 2013, 3, 1–7. [Google Scholar] [CrossRef]
- Mazer, B.; Kairy, D.; Montpetit, A.; Alary Gauvreau, C.; Visintin, M.; Guindon, A.; Labbé, D.; Sebestyen, I. Evaluating the use of video presentation as a knowledge transfer strategy to promote social participation interventions in rehabilitation. In Proceedings of the 1st National Knowledge Translation Conference in Rehabilitation, Montreal, QC, Canada, 4–5 May 2016. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef]
- Bennett, G.; Jessani, N. La Boîte à Outils Sur L’application des Connaissances; Presses de l’Université du Québec: Québec, QC, Canada, 2011; 315p. [Google Scholar]
- Bigonnesse, C.; Mahmood, A.; Chaudhury, H.; Mortenson, W.B.; Miller, W.C.; Martin Ginis, K.A. The role of neighbourhood physical environment on mobility and social participation among people using mobility assistive technology: A systematic review. Disabil. Soc. 2018, 33, 866–893. [Google Scholar] [CrossRef]
- Catalani, C.; Minkler, M. Photovoice: A review of the literature in health and public health. Health Educ. Behav. 2010, 37, 424–451. [Google Scholar] [CrossRef] [PubMed]
- Labbé, D.; Mahmood, A.; Routhier, F.; Prescott, M.; Lacroix, E.; Miller, W.C.; Mortenson, W.B. Using photovoice to increase social inclusion of people with disabilities: Reflections on the benefits and challenges. J. Community Psychol. 2019. [Google Scholar]
- Mulligan, K.; Calder, A.; Mulligan, H. Inclusive design in architectural practice: Experiential learning of disability in architectural education. Disabil. Health J. 2018, 11, 237–242. [Google Scholar] [CrossRef]
- Kadir, S.A.; Jamaludin, M.; Rahim, A.A. Building managers’ views on accessibility and UD Implementation in public buildings: Putrajaya. J. Asian Behav. Stud. 2018, 3, 1–12. [Google Scholar]
- Lid, I.M. Universal design and disability: An interdisciplinary perspective. Disabil. Rehabil. 2014, 36, 1344–1349. [Google Scholar] [CrossRef]
- Henderson, B.; Clements, A.; Webb, M.; Kofinas, A. Exploration: Wardopoly—Game-Based experiential learning in nurse leadership education. In The Power of Play in Higher Education; Palgrave Macmillan: Cham, Switzerland, 2019; pp. 273–282. [Google Scholar]
- Kothari, A.; Wathen, C.N. A critical second look at integrated knowledge translation. Health Policy 2013, 109, 187–191. [Google Scholar] [CrossRef]
- Suarez-Balcazar, Y.; Harper, G.W. Community-Based approaches to empowerment and participatory evaluation. J. Prev. Interv. Community 2003, 26, 1–4. [Google Scholar] [CrossRef]
- Naples, N.; Mauldin, L.; Dillaway, H. From the guest editors: Gender, disability, and intersectionality. Gend. Soc. 2019, 33, 5–18. [Google Scholar] [CrossRef]


{kind=link}
| Type of Indicators | Subtype of Indicators | Method |
|---|---|---|
| Reach | Number of invitations distributed | Journal |
| Number of requests for the knowledge mobilization (KM) strategies | ||
| Number of downloads/hits | ||
| Media exposure (including social media) | ||
| Number of questionnaires completed | ||
| Usefulness | Number of participants and duration/type of participation | Journal |
| Number of participants who participated in development | ||
| Satisfaction with KM strategies | Questionnaire | |
| Usefulness of gained knowledgev | ||
| Changed views | ||
| Use | Number of users adapting the information | Observations |
| Number of people using the KM strategies to inform policy/advocacy/enhance programs, training, education, or research | ||
| Number of persons using the KM strategies to improve their practice | Questionnaire | |
| Intend to use | ||
| Partnership Collaboration | Number of products/services developed, or disseminated by the participants | Journal |
| Social network growth, influences, collaboration | Observations | |
| Practice change | Intention or commitment to change | Observations |
| Type of indicators | Subtype | Videos | Photo Exhibit | Interactive Game |
|---|---|---|---|---|
| Reach | Number distributed or invitations | In total, 1500 direct invitations via email In total, 11 email blast invitations sent through newsletters or online event-planning site | In total, 1500 direct invitations via email In total, 11 email blast sent through newsletters or online event-planning site | |
| Number of views | In total, 1411 views | |||
| Media exposure (include social media such as Facebook, Twitter) | Four Facebook posts In total, 11 Twitter posts (25 retweets) | One online newspaper article Two Facebook posts In total, 11 Twitter posts (41 retweets) | One online newspaper article Two Facebook posts In total, 11 Twitter posts (41 retweets) | |
| Usefulness | Number of participants | Eight presentations with 76 participants Three community outreach events with 206 participants | Four community outreach events with 236 participants | Four community outreach events with 236 participants |
| Duration of participation | Average view of 2 min 20s | Average of 25 min | Average of 20 min | |
| Type of participation | Passive | Interactive | Interactive | |
| Number of people who participated in the development of the KM Strategies | Six dEMAND participants | One member of the advisory committee Eight dEMAND participants | One member of the advisory committee | |
| Partnership and Collaboration | Number of products/services developed, or disseminated with partners | One development of research project | Two invitations to present the KM strategies to other city events | Three requests to use the game in other contexts |
| Social network growth, influences, new collaboration | Four new collaborations: two between MD users and city decision maker and staff; two between researchers and city staff | Two new collaborations between researchers and city staff | Two new collaborations between researchers and community-based organizations | |
| Practice Change | Intent or commitment to change | Development of guidelines to change workers practice Intention to include the knowledge in accessibility strategy | Development of guideline to change workers practice Intention to include the knowledge in accessibility strategy |
| Type of Indicators | Questions | Video (n = 134) Mean (SD) | Photo Exhibit (n = 75) Mean (SD) | Interactive Game (n = 70) Mean (SD) |
|---|---|---|---|---|
| Usefulness | The length of the [name of activity] is appropriate. | 4.36 (0.77) | 4.39 (0.77) | 4.27 (0.83) |
| Usefulness | The content corresponds to my needs and interest. | 4.30 (0.79) | 4.42 (0.75) | 4.37 (0.89) |
| Usefulness | The [name of the activity] enabled me to increase my knowledge about environmental barriers encountered by mobility device users. | 4.30 (0.86) | 4.39 (0.88) | 4.43 (0.84) |
| Usefulness | This [name of the activity] changed my perspective on the experiences of mobility device users in their environment. | 3.96 (0.99) | 4.23 (0.89) | 4.17 (0.96) |
| Use | I intend to apply the knowledge I got from [name of activity]. | 4.17 (0.83) | 4.25 (0.82) | 4.26 (0.87) |
| Use | I would share this [name of the activity] with my network. | 4.30 (0.85) | 4.47 (0.78) | 4.45 (0.84) |
| Use | This kind of [name of the activity] is very useful for me and/or my work. | 4.20 (0.84) | 4.31 (0.85) | 4.24 (1.00) |
| Question | Urban Planners | Advisory Board Committee | Social Planners | Community Organization | Engineers | Rehabilitation Professionals | Students | People with a Disability | Researchers | General Public |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (S.D) | ||||||||||
| In my opinion, these activities would be useful for the following target audiences | 4.55 * (0.85) | 4.50 (0.84) | 4.51 * (0.79) | 4.40 (0.86) | 4.50 (0.89) | 4.07 ** (0.96) | 4.31 (0.85) | 3.99 * (0.99) | 4.36 (0.88) | 4.49 (0.78) |
| Categories | Videos | Photo Exhibit | Interactive Game |
|---|---|---|---|
| Using Visuals | x | x | |
| Seeing it from the MD users’ perspective | x | x | |
| Offering tangible, real-life examples | x | ||
| Understanding better the barriers and challenges | x | x | x |
| Informing about the facilitators and possible solutions | x | ||
| Raising awareness | x | ||
| Interactivity and role playing | x | ||
| Entertaining | x |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labbé, D.; Mahmood, A.; Miller, W.C.; Mortenson, W.B. Examining the Impact of Knowledge Mobilization Strategies to Inform Urban Stakeholders on Accessibility: A Mixed-Methods study. Int. J. Environ. Res. Public Health 2020, 17, 1561. https://doi.org/10.3390/ijerph17051561
Labbé D, Mahmood A, Miller WC, Mortenson WB. Examining the Impact of Knowledge Mobilization Strategies to Inform Urban Stakeholders on Accessibility: A Mixed-Methods study. International Journal of Environmental Research and Public Health. 2020; 17(5):1561. https://doi.org/10.3390/ijerph17051561
Chicago/Turabian StyleLabbé, Delphine, Atiya Mahmood, William C. Miller, and W. Ben Mortenson. 2020. "Examining the Impact of Knowledge Mobilization Strategies to Inform Urban Stakeholders on Accessibility: A Mixed-Methods study" International Journal of Environmental Research and Public Health 17, no. 5: 1561. https://doi.org/10.3390/ijerph17051561
APA StyleLabbé, D., Mahmood, A., Miller, W. C., & Mortenson, W. B. (2020). Examining the Impact of Knowledge Mobilization Strategies to Inform Urban Stakeholders on Accessibility: A Mixed-Methods study. International Journal of Environmental Research and Public Health, 17(5), 1561. https://doi.org/10.3390/ijerph17051561