Relationship between Serum Vitamin D and Leg Strength in Older Adults with Pre-Dialysis Chronic Kidney Disease: A Preliminary Study


 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Measurements
2.3. Statistical Analysis
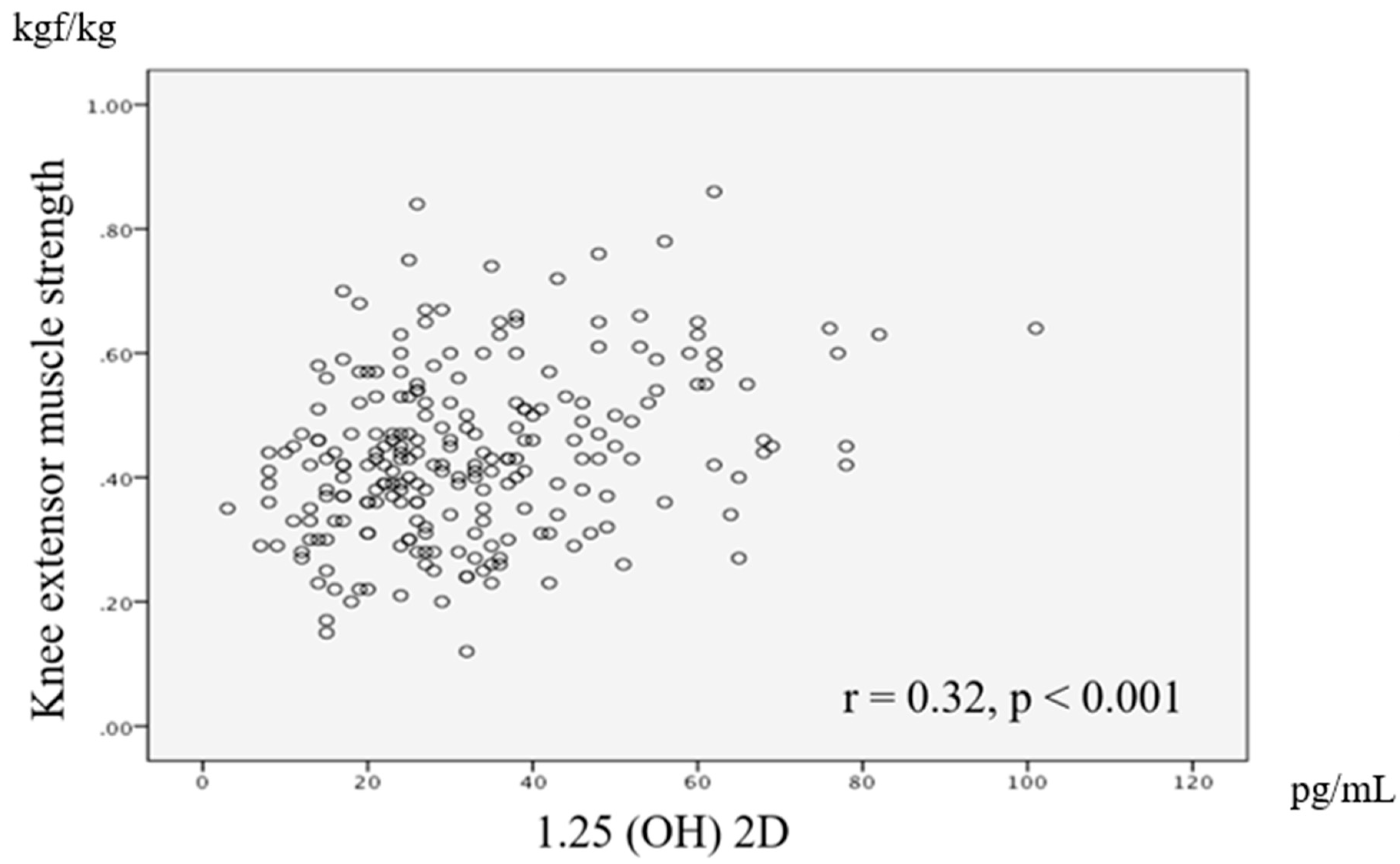
3. Results
4. Discussion
4.1. The Relationship between Knee Extensor Muscle Strength and Active Vitamin D
4.2. Clinical Implication and Future Research
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Imai, E.; Horio, M.; Watanabe, K.; Iseki, K.; Yamagata, K.; Hara, S.; Ura, N.; Kiyohara, Y.; Moriyama, T.; Ando, Y.; et al. Prevalence of chronic kidney disease in the Japanese general population. Clin. Exp. Nephrol. 2009, 13, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Japanese Society of Nephrology. Evidence-based practice guideline for the treatment of CKD. Clin. Exp. Nephrol. 2009, 13, 537–566. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Chonchol, M.; Gutiérrez, O.M.; Kalantar-Zadeh, K.; Kendrick, J.; Norris, K.; Scialla, J.J.; Thadhani, R. The role of vitamin D in CKD stages 3 to 4: Report of a scientific workshop sponsored by the National Kidney Foundation. Am. J. Kidney Dis. 2018, 72, 834–845. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Deeg, D.J.; Lips, P. Longitudinal Aging Study Amsterdam, Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): The Longitudinal Aging Study Amsterdam. J. Clin. Endocrinol. Metab. 2003, 88, 5766–5772. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, S.V.; Fischer, K.; Dawson-Hughes, B.; Freystaetter, G.; Beuschlein, F.; Schietzel, S.; Egli, A.; Bischoff-Ferrari, H.A. Association between 25-hydroxyvitamin D status and components of body composition and glucose metabolism in older men and women. Nutrients 2019, 10, 1826. [Google Scholar] [CrossRef] [PubMed]
- Romy, C.; Eva, G.; Heike, A.B.; Uta, F.; Alexander, H.; Wolfgang, K.; Annette, P. Vitamin D in Relation to Incident Sarcopenia and Changes in Muscle Parameters Among Older Adults: The KORA-Age Study. Calcif. Tissue Int. 2019, 105, 173–182. [Google Scholar]
- Ceglia, L.; Harris, S.S. Vitamin D and its role in skeletal muscle. Calcif. Tissue Int. 2013, 92, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Hiraki, K.; Yasuda, T.; Hotta, C.; Izawa, K.P.; Morio, Y.; Watanabe, S.; Sakurada, T.; Shibagaki, Y.; Kimura, K. Decreased physical function in pre-dialysis patients with chronic kidney disease. Clin. Exp. Nephrol. 2013, 17, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Molina, P.; Carrero, J.J.; Bover, J.; Chauveau, P.; Mazzaferro, S.; Torres, P.U. European Renal Nutrition (ERN) and Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Working Groups of the European Renal Association-European Dialysis Transplant Association (ERA-EDTA), Vitamin D, a modulator of musculoskeletal health in chronic kidney disease. J. Cachexia Sarcopenia Muscle 2017, 8, 686–701. [Google Scholar] [PubMed]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The roles of vitamin D in skeletal muscle: Form, function, and metabolism. Endocr. Rev. 2013, 34, 33–83. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Sun, Z. Molecular basis of Klotho: From gene to function in aging. Endocr. Rev. 2015, 36, 174–193. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Fujimori, T.; Nabeshima, Y. Mediation of unusually high concentrations of 1,25-dihydroxyvitamin D in homozygous klotho mutant mice by increased expression of renal 1alpha-hydroxylase gene. Endocrinology 2002, 143, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Shardell, M.; Semba, R.D.; Kalyani, R.R.; Hicks, G.E.; Bandinelli, S.; Ferrucci, L. Serum 25-hydroxyvitamin D, plasma klotho, and lower-extremity physical performance among older adults: Findings from the InCHIANTI Study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1156–1162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total |
|---|---|
| Number of patients | 231 |
| Age, years | 76 (65−92) |
| Male, n (%) | 159 (68.8) |
| Body mass index, kg/m2 | 24.1 ± 3.8 |
| Calcitriol, pg/mL | 32.5 ± 16.5 |
| eGFR, mL/min/1.73 m2 | 21.5 (6.2−57.0) |
| Intact PTH, pg/mL | 88 (6–607) |
| Phosphorus, mg/dL | 3.7 ± 0.8 |
| Calucium, mg/dL | 9.1 (6.1−10.3) |
| Albumin, g/dL | 3.9 ± 0.5 |
| Knee extensor muscle strength, kgf/kg | 0.44 ± 0.13 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, A.; Hiraki, K.; Otobe, Y.; P. Izawa, K.; Sakurada, T.; Shibagaki, Y. Relationship between Serum Vitamin D and Leg Strength in Older Adults with Pre-Dialysis Chronic Kidney Disease: A Preliminary Study. Int. J. Environ. Res. Public Health 2020, 17, 1433. https://doi.org/10.3390/ijerph17041433
Saito A, Hiraki K, Otobe Y, P. Izawa K, Sakurada T, Shibagaki Y. Relationship between Serum Vitamin D and Leg Strength in Older Adults with Pre-Dialysis Chronic Kidney Disease: A Preliminary Study. International Journal of Environmental Research and Public Health. 2020; 17(4):1433. https://doi.org/10.3390/ijerph17041433
Chicago/Turabian StyleSaito, Akira, Koji Hiraki, Yuhei Otobe, Kazuhiro P. Izawa, Tsutomu Sakurada, and Yugo Shibagaki. 2020. "Relationship between Serum Vitamin D and Leg Strength in Older Adults with Pre-Dialysis Chronic Kidney Disease: A Preliminary Study" International Journal of Environmental Research and Public Health 17, no. 4: 1433. https://doi.org/10.3390/ijerph17041433
APA StyleSaito, A., Hiraki, K., Otobe, Y., P. Izawa, K., Sakurada, T., & Shibagaki, Y. (2020). Relationship between Serum Vitamin D and Leg Strength in Older Adults with Pre-Dialysis Chronic Kidney Disease: A Preliminary Study. International Journal of Environmental Research and Public Health, 17(4), 1433. https://doi.org/10.3390/ijerph17041433