Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants?

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source for HL
2.2. Data Source for Sociodemographic, Health-Related Behaviours and Outcome Variables
2.3. Statistical Analysis
3. Results
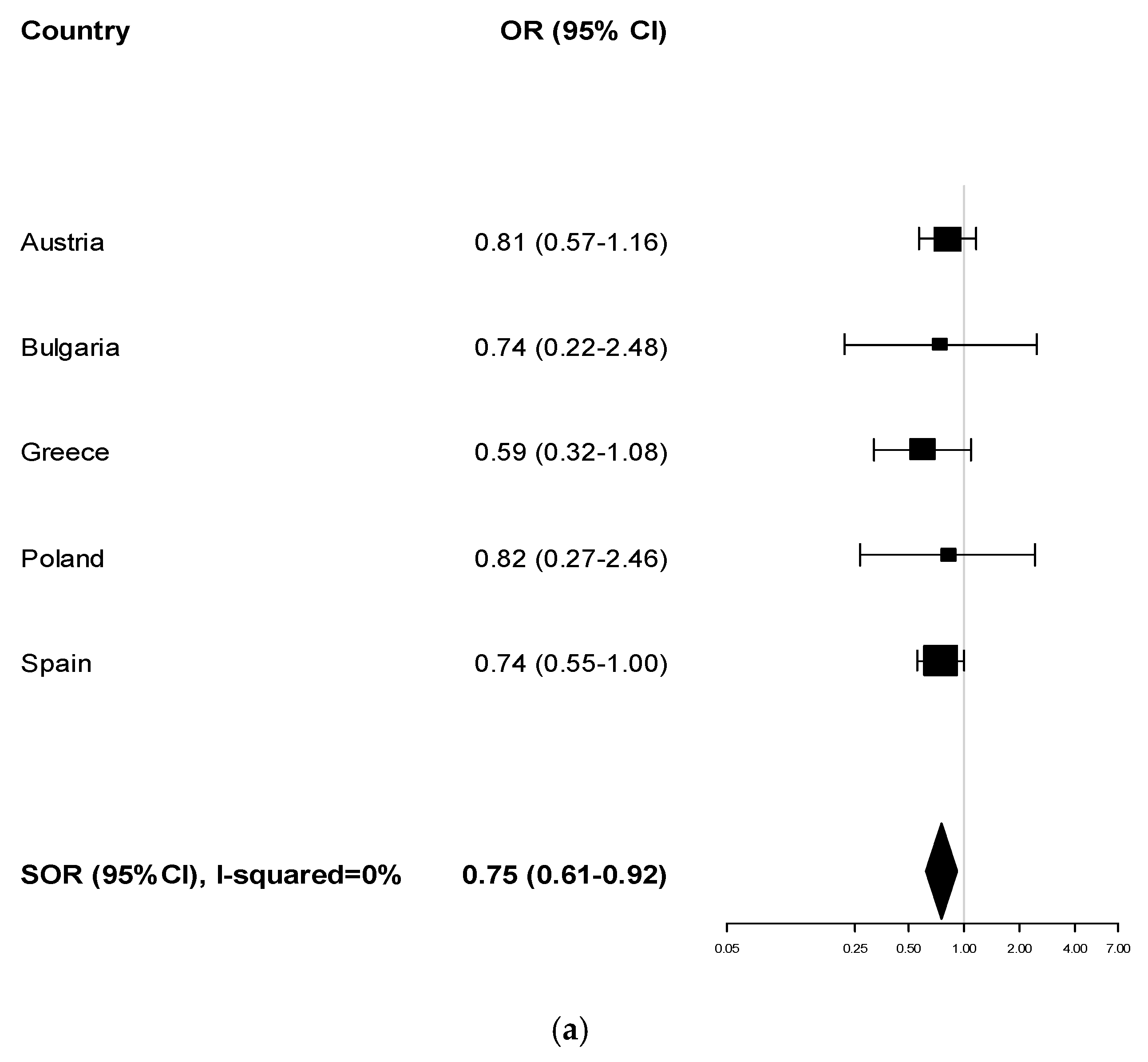
3.1. Perceived Health Status
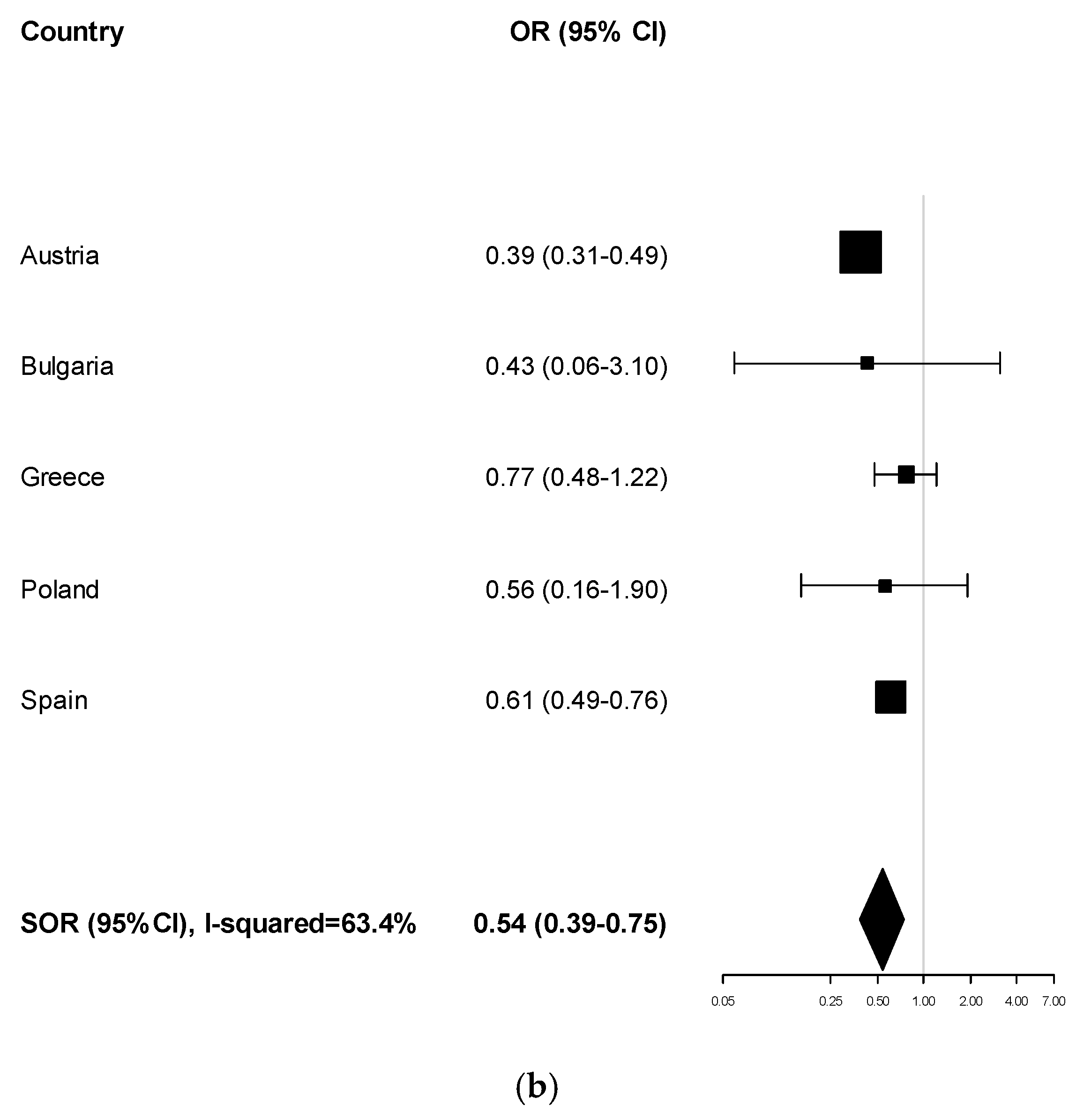
3.2. Body Mass Index
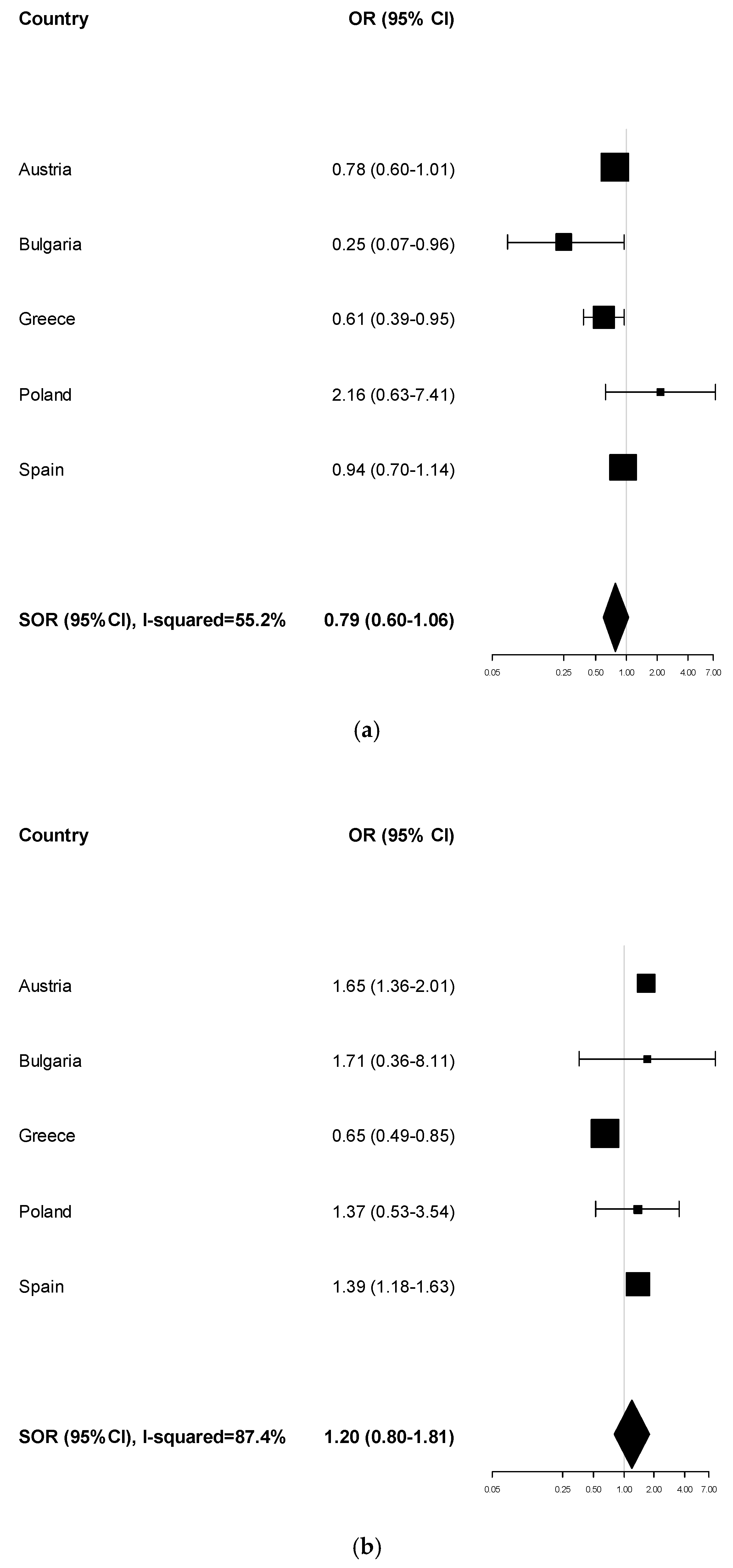
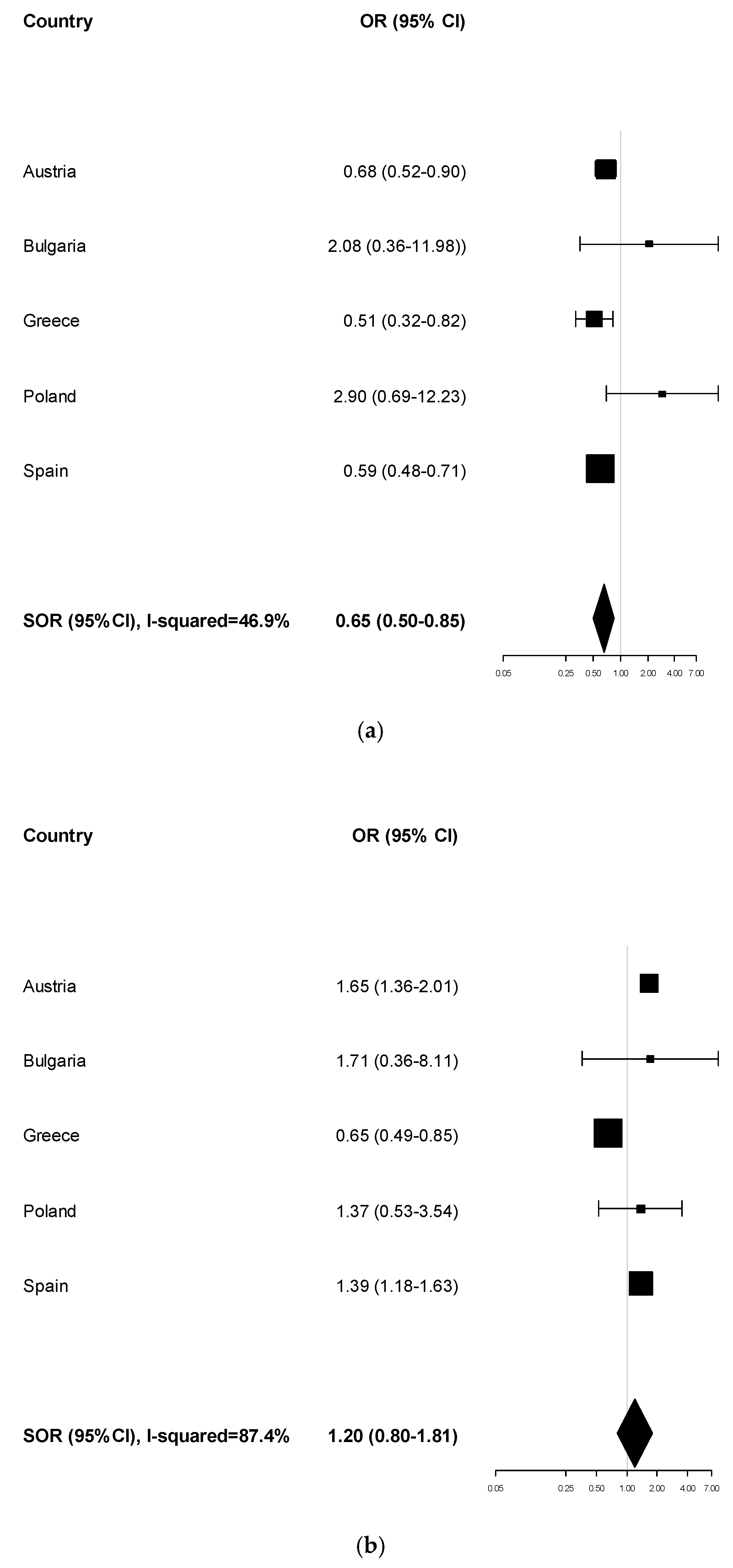
3.3. Smoking Habits
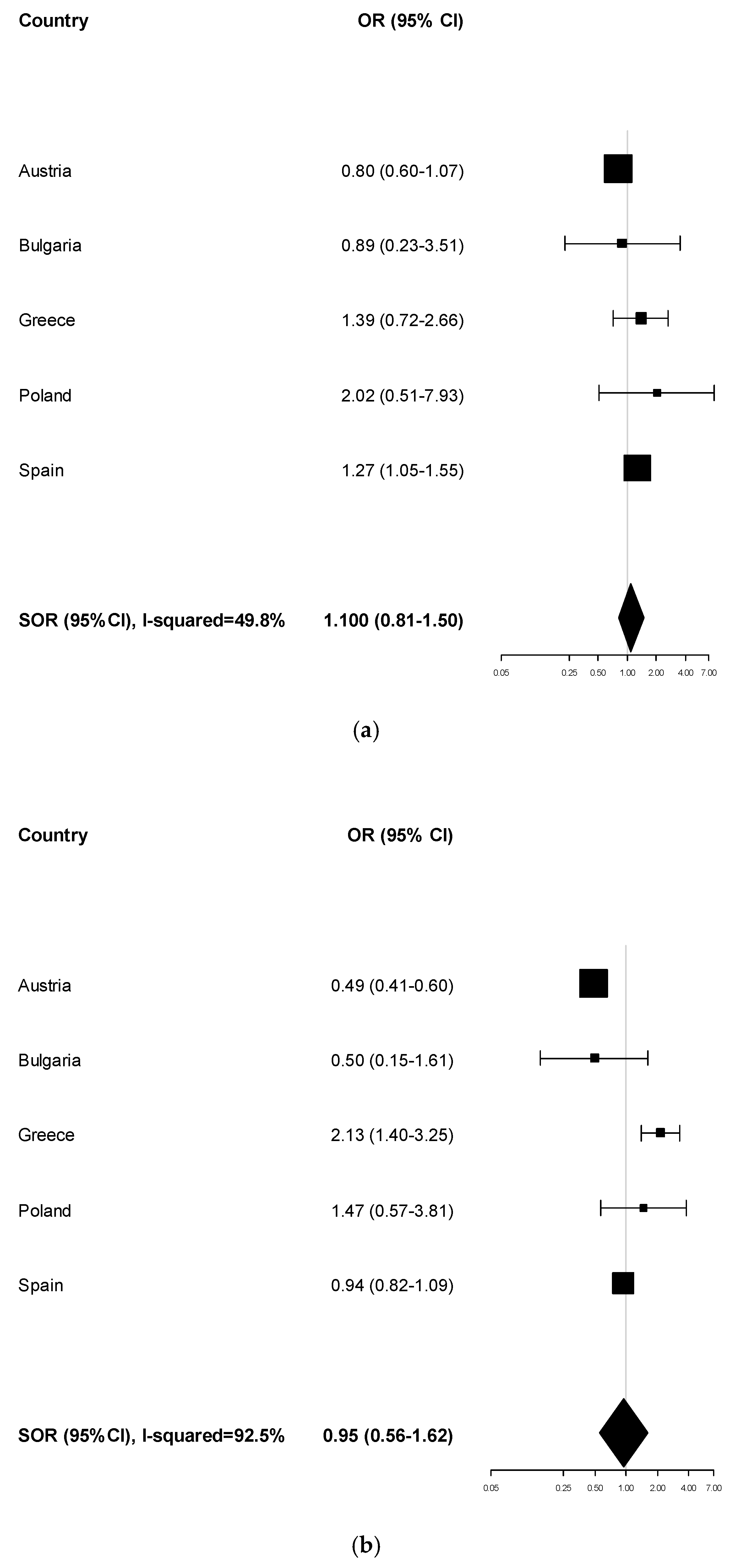
3.4. Physical Activity Levels
3.5. Attendance at Breast Cancer Screening Programmes
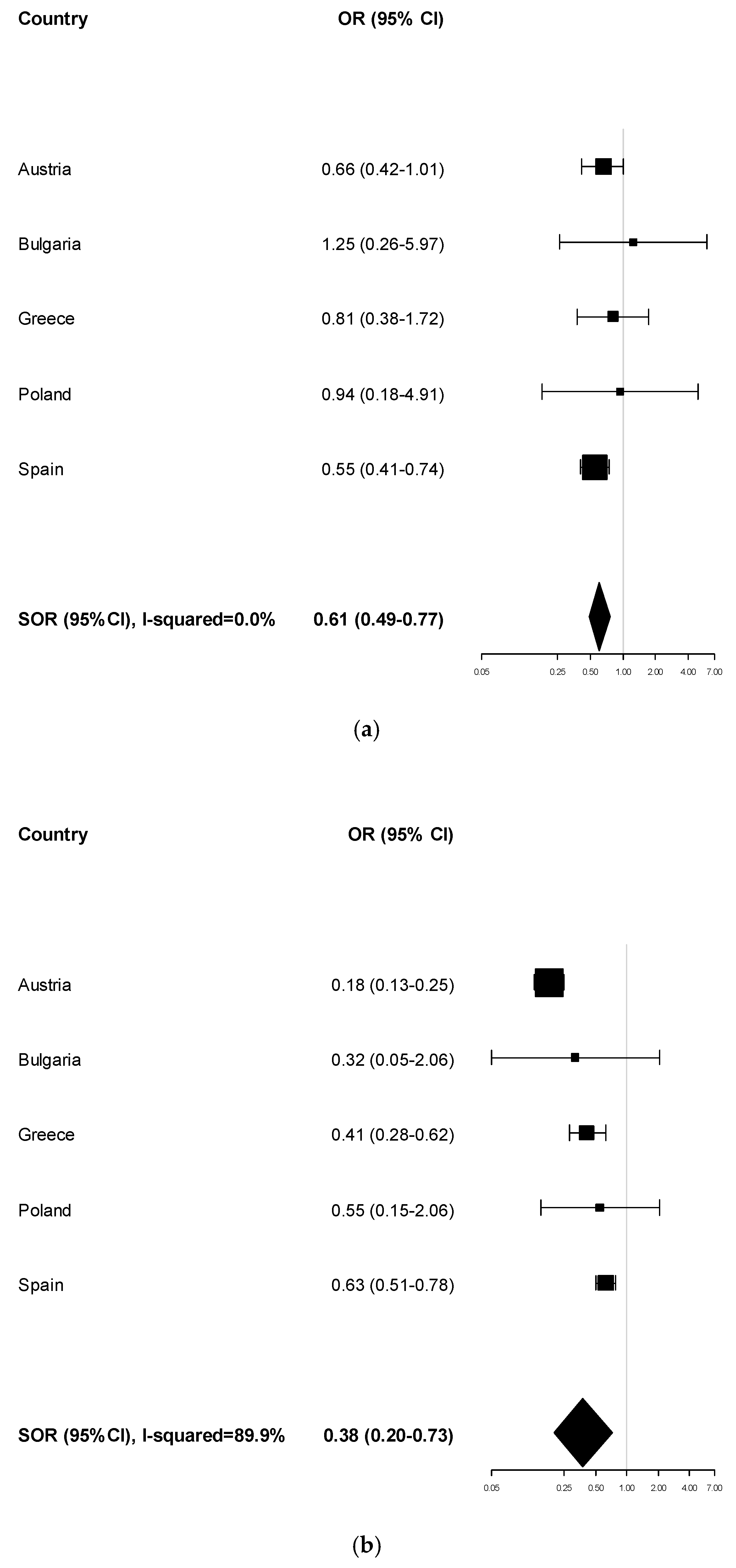
3.6. Attendance at Cervical Cancer Screening Programmes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A







References
- Van der Broucke, S. Health literacy: A critical concept for public health. Arch. Public Health 2014, 72, 10. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.A.; Bess, K.D.; Tucker, H.A.; Boyd, D.L.; Tuchman, A.M.; Wallston, K.A. Public health literacy defined. Am. J. Prev. Med. 2009, 36, 446–451. [Google Scholar] [CrossRef]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. Distributed health literacy: Longitudinal qualitative analysis of the roles of health literacy mediators and social networks of people living with a long-term health condition. Health Exp. 2015, 18, 1180–1193. [Google Scholar] [CrossRef]
- Papen, U. Literacy, learning and health—A social practices view of health literacy. Lit. Numer. Stud. 2009, 16, 19–34. [Google Scholar] [CrossRef]
- Levin-Zamir, D.; Leung, A.Y.M.; Dodson, S.; Rowlands, G. Health literacy in selected populations: Individuals, families, and communities from the international and cultural perspective. Stud. Health Technol. Inform. 2017, 240, 392–414. [Google Scholar] [CrossRef] [PubMed]
- Batterham, R.W.; Hawkins, M.; Collins, P.A.; Buchbinder, R.; Osborne, R.H. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef]
- Abreu, L.; Nunes, J.A.; Taylor, P.; Silva, S. Distributed health literacy among people living with type 2 diabetes in Portugal: Defining levels of awareness and support. Health Soc. Care Commun. 2018, 26, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Abreu, L.; Arriscado-Nunes, J.; Taylor, P.; Silva, S. The Role of Distributed Health Literacy in Asthma Integrated Care: A Public Medical Context from Portugal. Int. J. Integr. Care 2018, 18, 18. [Google Scholar] [CrossRef]
- Sentell, T.; Zhang, W.; Davis, J.; Baker, K.K.; Braun, K.L. The influence of community and individual health literacy on self-reported health status. J. Gen. Intern. Med. 2014, 29, 298–304. [Google Scholar] [CrossRef]
- Lorini, C.; Ierardi, F.; Bachini, L.; Donzellini, M.; Gemmi, F.; Bonaccorsi, G. The Antecedents and Consequences of Health Literacy in an Ecological Perspective: Results from an Experimental Analysis. Int. J. Environ. Res. Public Health 2018, 15, 798. [Google Scholar] [CrossRef]
- Tegegne, M.A. Linguistic Integration and Immigrant Health: The Longitudinal Effects of Interethnic Social Capital. J. Health Soc. Behav. 2018, 59, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Son, E.; Moring, N.S.; Igdalsky, L.; Parish, S.L. Navigating the health-care system in community: Perspectives from Asian immigrant parents of children with special health-care needs. J. Child Health Care 2018, 22, 251–268. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report on the Health of Refugees and Migrants in the WHO European Region; WHO Regional Office for Europe: København, Denmark, 2018. [Google Scholar]
- Rechel, B.; Mladovsky, P.; Devillé, W.; Rijks, B.; Petrova-Benedict, R.; McKee, M. Migration and Health in the European Union; Mc Graw Hill: Berkshire, UK, 2011. [Google Scholar]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Bakhtiari, E.; Olafsdottir, S.; Beckfield, J. Institutions, Incorporation, and Inequality: The Case of Minority Health Inequalities in Europe. J. Health Soc. Behav. 2018, 59, 248–267. [Google Scholar] [CrossRef]
- Mantwill, S.; Schulz, P.J. Low Health literacy and healthcare utilization among immigrants and non-immigrants in Switzerland. Patient Educ. Couns. 2017, 100, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Mantwill, S.; Monestel-Umaña, S.; Schulz, P.J. The Relationship between Health Literacy and Health Disparities: A Systematic Review. PLoS ONE 2015, 10, e0145455. [Google Scholar] [CrossRef]
- Kristiansen, M.; Razum, O.; Tezcan-Güntekin, H.; Krasnik, A. Aging and health among migrants in a European perspective. Public Health Rev. 2016, 37, 20. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef]
- European Commission. Study on Sound Evidence for a Better Understanding of Health Literacy in the European Union; RfS Chafea/2014/health/01 Contract no. 20146201; Publications Office of the European Union: Luxembourg, 2014. Available online: https://ec.europa.eu/health/sites/health/files/health_policies/docs/2015_health_literacy_en.pdf (accessed on 16 December 2019).
- HLS-EU Consortium. Comparative Report on Health Literacy in Eight EU Member States; The European Health Literacy Survey HLS-EU; 2012; Available online: http://ec.europa.eu/chafea/documents/news/Comparative_report_on_health_literacy_in_eight_EU_member_states.pdf (accessed on 12 March 2018).
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H.; et al. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef]
- van Houwelingen, A.H.; de Jager, S.C.; Kool, M.; van Heuven-Nolsen, D.; Kraneveld, A.D.; Nijkamp, F.P. Hypersensitivity reactions in mouse airways after a single and a repeated hapten challenge. Inflamm. Res. 2002, 51, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. How Health Systems Can Address Health Inequities Linked to Migration and Ethnicity; WHO Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Giannoni, M.; Franzini, L.; Masiero, G. Migrant integration policies and health inequalities in Europe. BMC Public Health 2016, 16, 463. [Google Scholar] [CrossRef] [PubMed]
- Malmusi, D. Immigrants’ health and health inequality by type of integration policies in European countries. Eur. J. Public Health 2015, 25, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Guzys, D.; Kenny, A.; Dickson-Swift, V.; Threlkeld, G. A critical review of population health literacy assessment. BMC Public Health 2015, 15, 215. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Sykes, S.; Wills, J.; Rowlands, G.; Popple, K. Understanding critical health literacy: A concept analysis. BMC Public Health 2013, 13, 150. [Google Scholar] [CrossRef]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef]
- Ledoux, C.; Pilot, E.; Diaz, E.; Krafft, T. Migrants’ access to healthcare services within the European Union: A content analysis of policy documents in Ireland, Portugal and Spain. Glob. Health 2018, 14, 57. [Google Scholar] [CrossRef]
- World Health Organization. New Action Network Strengthens Health Literacy Measurement in Europe. Available online: http://www.euro.who.int/en/data-and-evidence/news/news/2018/4/new-action-network-strengthens-health-literacy-measurement-in-europe (accessed on 16 December 2019).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Description in the European Health Interview Survey (EHIS) Database (Questions to Participants and Answers) and Categorisation for This Study |
|---|---|
| Age | Age of the person at the moment of interview Modes: the numerical value has been ranged into four classes (15–29; 30–44; 45–60; 60+) |
| Gender | Modes: “Male”, “Female” |
| Citizenship | What is your citizenship? Modes: “nationals”, “nationals of other EU Member States”, “nationals of non-EU countries” |
| Degree of urbanisation of the area of residence | Three modes based on a combination of geographical contiguity and population density, measured by minimum population thresholds applied to 1 km2 population grid cells: “densely-populated area”, “Intermediate area”, “thinly-populated area” |
| Legal marital status | What is your legal marital status? Modes: “never married”, “married”, “widows and not remarried” and “divorced and not remarried” |
| Education level | What is the highest education leaving certificate, diploma or education degree you have obtained? Seven modes summarised into three final modes following the International Standard Classification of Education: “Less than primary, primary and lower secondary education”, “Upper secondary and post-secondary non-tertiary education”, “Tertiary education” |
| Employment status | How would you define your current labour status? Eight modes summarised into three final modes: “worker”, “not a worker”, “former worker” |
| Presence of chronic illnesses | Do you have any longstanding illness or (longstanding) health problem? Modes: “yes”, “no” |
| Body Mass Index (BMI) | How much are you weight without shoes and shoes? and How tall are you without shoes? BMI calculated as weight/height2, and then categorised into two categories: underweight/normal subject” (BMI ≤ 25 kg/m2) and “overweight/obese subject” (BMI ≥ 25 kg/m2) |
| Physical activity | During the last 7 days, on how many days did you do vigorous physical activities? During the last 7 days, on how many days did you do moderate physical activities? The answers to the two questions were combined in a dichotomous variable, with “Active” and “Inactive” modes. The “Active” mode included those who stated that they performed moderate physical activity at least 2/3 times a week or intense at least 1/2 times a week. The “Inactive” mode included those who stated that they performed moderate physical activity less than 2/3 times a week or intense less than 1/2 times a week |
| Smoking habits | Do you smoke at all nowadays? Modes: “regularly”, “occasionally”, “never”. Modes dicotomised as “Smoker” (both regular and occasional) and “Non-smoker” |
| Adherence to breast cancer screening | Have you ever had a mammography, which is an X-ray of one or both of your breasts? Modes: “yes”, “no” The women ≥50 years were selected. The women who declared they had adhered to the screening every two years have been included in the “Adherent” mode; the women who have declared that they have not performed screening or have performed it at intervals of more than two years have been included in “Non-adherent” mode. |
| Adherence to cervical smear screening | Have you ever had a cervical smear test? Modes: “yes”, “no” The women ≥ 25 years were selected. The women who declared they had adhered to the screening every two years have been included in the “Adherent” mode; the women who have declared that they have not performed screening or have performed it at intervals of more than two years have been included in “Non-adherent” mode. |
| Perceived Health Status | How is your health in general? Five modes: “very good”, “good”, “fair”, “bad”, and “very bad”. The final variable was dichotomous: “good” (very good, good) and “bad” (fair, bad, very bad). |
| Variables | Total (1) (n = 84,503) | Austria (1) (n = 15,382) | Bulgaria (1) (n = 5661) | Greece (1) (n = 6172) | Poland (1) (n = 35,100) | Spain (1) (n = 22,188) | p-Value (2) | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 15–29 | 26.6% | 27.1% | 23.1% | 20.7% | 31.4% | 21.2% | <0.001 |
| 30–44 | 16.7% | 18.9% | 14.0% | 16.0% | 14.5% | 19.7% | ||
| 45–60 | 33.3% | 31.2% | 36.2% | 30.4% | 35.2% | 32.0% | ||
| 60+ | 23.3% | 22.8% | 26.7% | 32.9% | 18.9% | 27.2% | ||
| Gender | Male | 45.3% | 45.4% | 47.4% | 39.1% | 46.0% | 45.3% | <0.001 |
| Female | 54.7% | 54.6% | 52.6% | 60.9% | 54.0% | 54.7% | ||
| Citizenship | Nationals | 96.9% | 94.5% | 99.6% | 94.5% | 99.9% | 93.8% | <0.001 |
| Nationals of other EU countries | 1.0% | 1.8% | 0.2% | 1.3% | 0.1% | 2.2% | ||
| Nationals of non-EU countries | 2.1% | 3.7% | 0.2% | 4.2% | 0.1% | 4.0% | ||
| Education level (highest attained) | Less than secondary education | 23.4% | 0.9% | 8.9% | 37.9% | 21.1% | 42.3% | <0.001 |
| Upper secondary and post-secondary non-tertiary | 55.5% | 71.6% | 72.5% | 38.2% | 61.5% | 35.5% | ||
| Tertiary | 21.1% | 27.5% | 18.5% | 23.7% | 17.5% | 22.2% | ||
| Employment status | Worker | 46.3% | 52.4% | 47.9% | 38.4% | 45.6% | 45.0% | <0.001 |
| Not a worker | 22.8% | 18.1% | 17.2% | 28.7% | 21.6% | 27.7% | ||
| Former worker | 30.9% | 30.0% | 35.9% | 33.7% | 32.0% | 27.8% | ||
| Marital status | Never married | 25.4% | 28.4% | 21.7% | 20.7% | 24.7% | 26.5% | <0.001 |
| Married | 57.9% | 56.6% | 58.4% | 60.1% | 60.3% | 54.1% | ||
| Widowed, not remarried | 11.7% | 8.9% | 14.7% | 15.5% | 10.8% | 13.0% | ||
| Divorced, not remarried | 5.1% | 6.1% | 5.2% | 3.7% | 4.1% | 6.3% | ||
| Degree of urbanisation of the area of residence | Densely-populated area | 36.8% | 22.4% | 43.9% | 42.5% | 32.9% | 49.5% | <0.001 |
| Intermediate area | 16.5% | 23.7% | 7.8% | 11.6% | 12.9% | 20.6% | ||
| Thinly-populated area | 46.8% | 54.0% | 48.2% | 45.9% | 54.2% | 29.9% | ||
| Underlying illness or health problem | Yes | 49.6% | 39.0% | 43.2% | 48.2% | 51.1% | 56.5% | <0.001 |
| No | 50.4% | 61.2% | 56.6% | 51.9% | 48.7% | 43.7% | ||
| Perceived health status | Good/very good | 35.1% | 26.8% | 36.5% | 34.8% | 40.5% | 32.2% | <0.001 |
| Fair/bad/very bad | 64.9% | 79.0% | 60.7% | 71.0% | 52.7% | 73.6% | ||
| Body mass index | Underweight/normal | 37.2% | 45.8% | 36.1% | 34.6% | 34.4% | 36.5% | <0.001 |
| Overweight/obesity | 62.8% | 64.4% | 61.6% | 71.3% | 59.1% | 65.7% | ||
| Smoking habits | Smoker | 27.8% | 23.4% | 37.8% | 36.2% | 26.2% | 28.6% | <0.001 |
| Non-smoker | 72.2% | 83.1% | 68.2% | 70.3% | 67.6% | 73.5% | ||
| Physical activity | Active | 34.7% | 26.7% | 36.9% | 28.7% | 30.1% | 48.7% | <0.001 |
| Inactive | 65.3% | 75.8% | 53.4% | 73.5% | 68.4% | 53.7% | ||
| Attendance of breast cancer screening | Adherent | 45.5% | 68.8% | 15.8% | 31.9% | 42.6% | 48.0% | <0.001 |
| Non-adherent | 54.5% | 35.1% | 81.8% | 71.2% | 53.4% | 54.8% | ||
| Attendance of cervical cancer screening | Adherent | 52.8% | 78.8% | 28.7% | 47.2% | 51.8% | 44.7% | <0.001 |
| Non-adherent | 47.2% | 26.2% | 65.1% | 57.3% | 43.7% | 58.5% | ||
| Variables | Austria | Bulgaria | Greece | Poland | Spain |
|---|---|---|---|---|---|
| No. participants | 978 | 925 | 998 | 921 | 974 |
| Health Literacy (HLS-EU-Q47) | |||||
| Excellent HL (%) | 9.9% | 11.3% | 15.6% | 19.5% | 9.1% |
| Sufficient HL (%) | 33.7% | 26.6% | 39.6% | 35.9% | 32.6% |
| Problematic HL (%) | 38.2% | 35.2% | 30.9% | 34.4% | 50.8% |
| Inadequate HL (%) | 18.2% | 26.9% | 13.9% | 10.2% | 7.5% |
| Mean value | 31.9 | 30.5 | 33.6 | 34.4 | 32.9 |
| Citizenship | Austria | Bulgaria | Greece | Poland | Spain | Pooled Estimate | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR (1) | 95% CI | OR (1) | 95% CI | OR (1) | 95% CI | OR (1) | 95% CI | OR (1) | 95% CI | SOR (2) | 95% CI | I2 | |
| Perceived health status (very good or good vs. fair, bad, or very bad) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.81 | 0.57–1.16 | 0.74 | 0.22–2.46 | 0.59 | 0.32–1.08 | 0.82 | 0.27–2.44 | 0.74 | 0.55–1.00 | 0.75 | 0.61–0.92 | 0.0% |
| nationals of non-EU countries | 0.39 | 0.31–0.49 | 0.43 | 0.06–3.10 | 0.77 | 0.48–1.22 | 0.56 | 0.16–1.90 | 0.61 | 0.49–0.76 | 0.54 | 0.39–0.75 | 63.4% |
| Body mass index (≥25 vs. <25 kg/m2) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.78 | 0.60–1.01 | 0.25 | 0.07–0.96 | 0.61 | 0.39–0.95 | 2.16 | 0.63–7.41 | 0.94 | 0.70–1.14 | 0.79 | 0.60–1.06 | 55.2% |
| nationals of non-EU countries | 1.65 | 1.36–2.01 | 1.71 | 0.36–8.11 | 0.65 | 0.49–0.85 | 1.37 | 0.53–3.54 | 1.39 | 1.18–1.63 | 1.20 | 0.80–1.81 | 87.4% |
| Smoking habits (smoker vs. non-smoker) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.68 | 0.52–0.90 | 2.08 | 0.36–11.98 | 0.51 | 0.32–0.82 | 2.90 | 0.69–12.23 | 0.59 | 0.48–0.71 | 0.65 | 0.50–0.85 | 46.9% |
| nationals of non-EU countries | 0.58 | 0.48–0.70 | 1.40 | 0.27–7.26 | 1.96 | 1.48–2.60 | 0.56 | 0.24–1.31 | 1.73 | 1.46–2.04 | 1.10 | 0.57–2.11 | 95.5% |
| Physical activity (active vs. inactive) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.80 | 0.60–1.07 | 0.89 | 0.23–3.51 | 1.39 | 0.72–2.66 | 2.02 | 0.51–7.93 | 1.27 | 1.05–1.55 | 1.10 | 0.81–1.50 | 49.8% |
| nationals of non-EU countries | 0.49 | 0.41–0.60 | 0.50 | 0.15–1.61 | 2.13 | 1.40–3.25 | 1.47 | 0.57–3.81 | 0.94 | 0.82–1.09 | 0.95 | 0.56–1.62 | 92.5% |
| Attendance of breast cancer screening (yes vs. no) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.82 | 0.46–1.45 | 2.52 | 0.40–15.76 | 1.19 | 0.23–6.10 | 0.38 | 0.05–3.07 | 0.30 | 0.17–0.52 | 0.66 | 0.31–1.39 | 60.6% |
| nationals of non-EU countries | 0.55 | 0.30–1.02 | - | - | 0.28 | 0.11–0.72 | 1.26 | 0.12–13.69 | 0.17 | 0.09–0.32 | 0.34 | 0.16–0.71 | 64.0% |
| Attendance of cervical cancer screening (yes vs. no) | |||||||||||||
| nationals | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| nationals of other EU countries | 0.66 | 0.42–1.01 | 1.25 | 0.26–5.97 | 0.81 | 0.38–1.72 | 0.94 | 0.18–4.91 | 0.55 | 0.41–0.74 | 0.61 | 0.49–0.77 | 0.0% |
| nationals of non-EU countries | 0.18 | 0.13–0.25 | 0.32 | 0.05–2.06 | 0.41 | 0.28–0.62 | 0.55 | 0.15–2.06 | 0.63 | 0.51–0.78 | 0.38 | 0.20–0.73 | 89.9% |
| Citizenship | SOR | 95% CI | I2 | Explanatory Variable in Meta-Regression Models (1) | ||
|---|---|---|---|---|---|---|
| Health Literacy (HLS-EU-Q47) | ||||||
| Continuous | % Population with Inadequate HL (2) | % Population with Problematic or Inadequate HL (2) | ||||
| Perceived health status (very good or good vs. fair, bad, or very bad) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 0.75 | 0.61–0.92 | 0.0% | - | - | - |
| nationals of non-EU countries | 0.54 | 0.39–0.75 | 63.4% | 0.056 | ns (3) | ns (3) |
| Body mass index (≥25 vs. <25 kg/m2) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 0.79 | 0.60–1.06 | 55.2% | ns (3) | ns (3) | ns (3) |
| nationals of non-EU countries | 1.20 | 0.80–1.81 | 87.4% | ns (3) | ns (3) | 0.075 |
| Smoking habits (smoker vs. non-smoker) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 0.65 | 0.50–0.85 | 46.9% | - | - | - |
| nationals of non-EU countries | 1.10 | 0.57–2.11 | 95.5% | ns (3) | ns (3) | ns (3) |
| Physical activity (active vs. inactive) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 1.10 | 0.81–1.50 | 49.8% | - | - | - |
| nationals of non-EU countries | 0.95 | 0.56–1.62 | 92.5% | 0.065 | ns (3) | ns (3) |
| Attendance of breast cancer screening (yes vs. no) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 0.66 | 0.31–1.39 | 60.6% | ns (3) | ns (3) | ns (3) |
| nationals of non-EU countries | 0.34 | 0.16–0.71 | 64.0% | ns (3) | ns (3) | ns (3) |
| Attendance of cervical cancer screening (yes vs. no) | ||||||
| nationals | 1.00 | |||||
| nationals of other EU countries | 0.61 | 0.49–0.77 | 0.0% | - | - | - |
| nationals of non-EU countries | 0.38 | 0.20–0.73 | 89.9% | ns (3) | 0.039 | ns (3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorini, C.; Caini, S.; Ierardi, F.; Bachini, L.; Gemmi, F.; Bonaccorsi, G. Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants? Int. J. Environ. Res. Public Health 2020, 17, 1149. https://doi.org/10.3390/ijerph17041149
Lorini C, Caini S, Ierardi F, Bachini L, Gemmi F, Bonaccorsi G. Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants? International Journal of Environmental Research and Public Health. 2020; 17(4):1149. https://doi.org/10.3390/ijerph17041149
Chicago/Turabian StyleLorini, Chiara, Saverio Caini, Francesca Ierardi, Letizia Bachini, Fabrizio Gemmi, and Guglielmo Bonaccorsi. 2020. "Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants?" International Journal of Environmental Research and Public Health 17, no. 4: 1149. https://doi.org/10.3390/ijerph17041149
APA StyleLorini, C., Caini, S., Ierardi, F., Bachini, L., Gemmi, F., & Bonaccorsi, G. (2020). Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants? International Journal of Environmental Research and Public Health, 17(4), 1149. https://doi.org/10.3390/ijerph17041149