The Role of Vitamins in Oral Health. A Systematic Review and Meta-Analysis

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Information Sources and Search Strategy
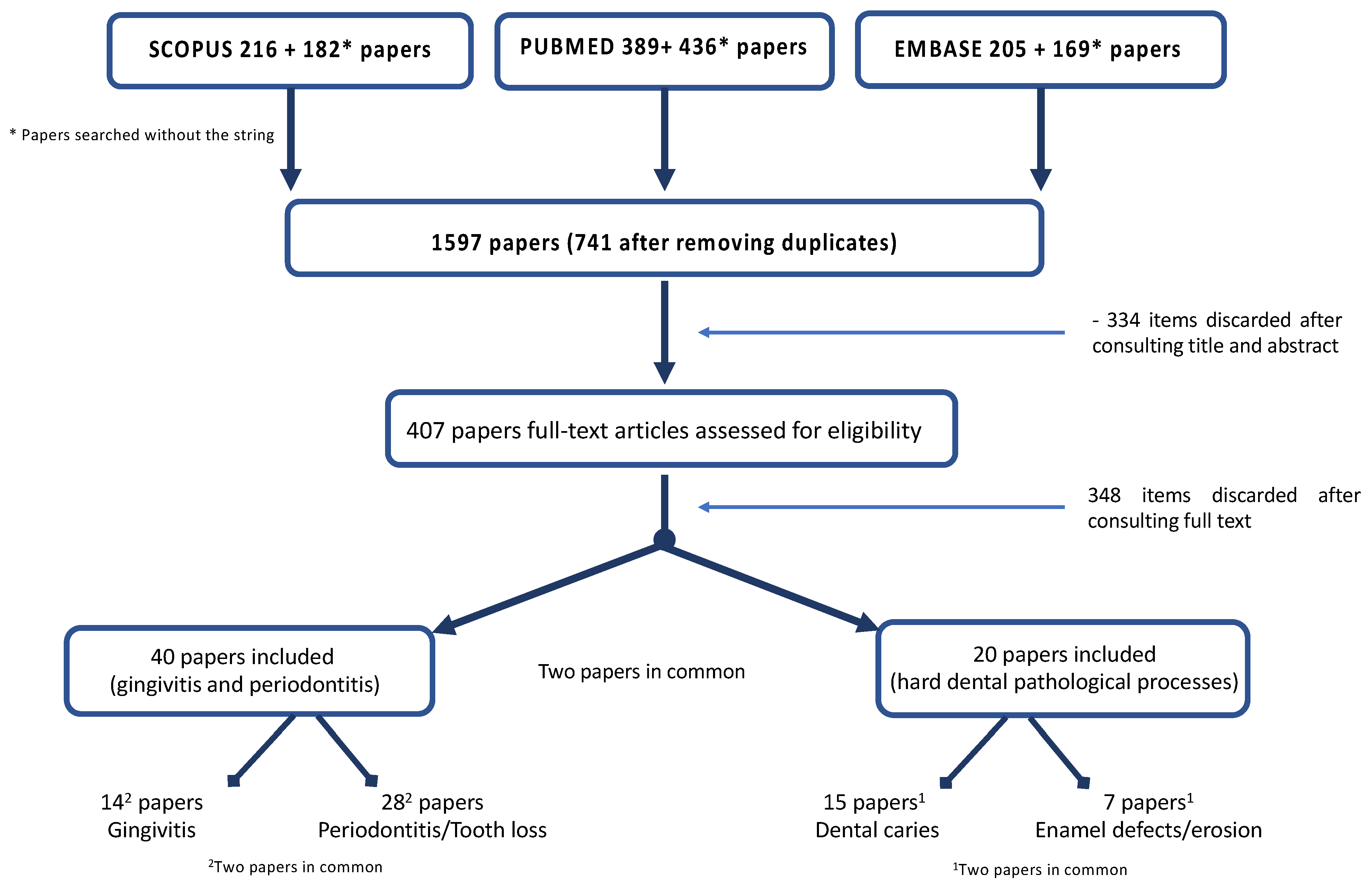
2.4. Study Selection
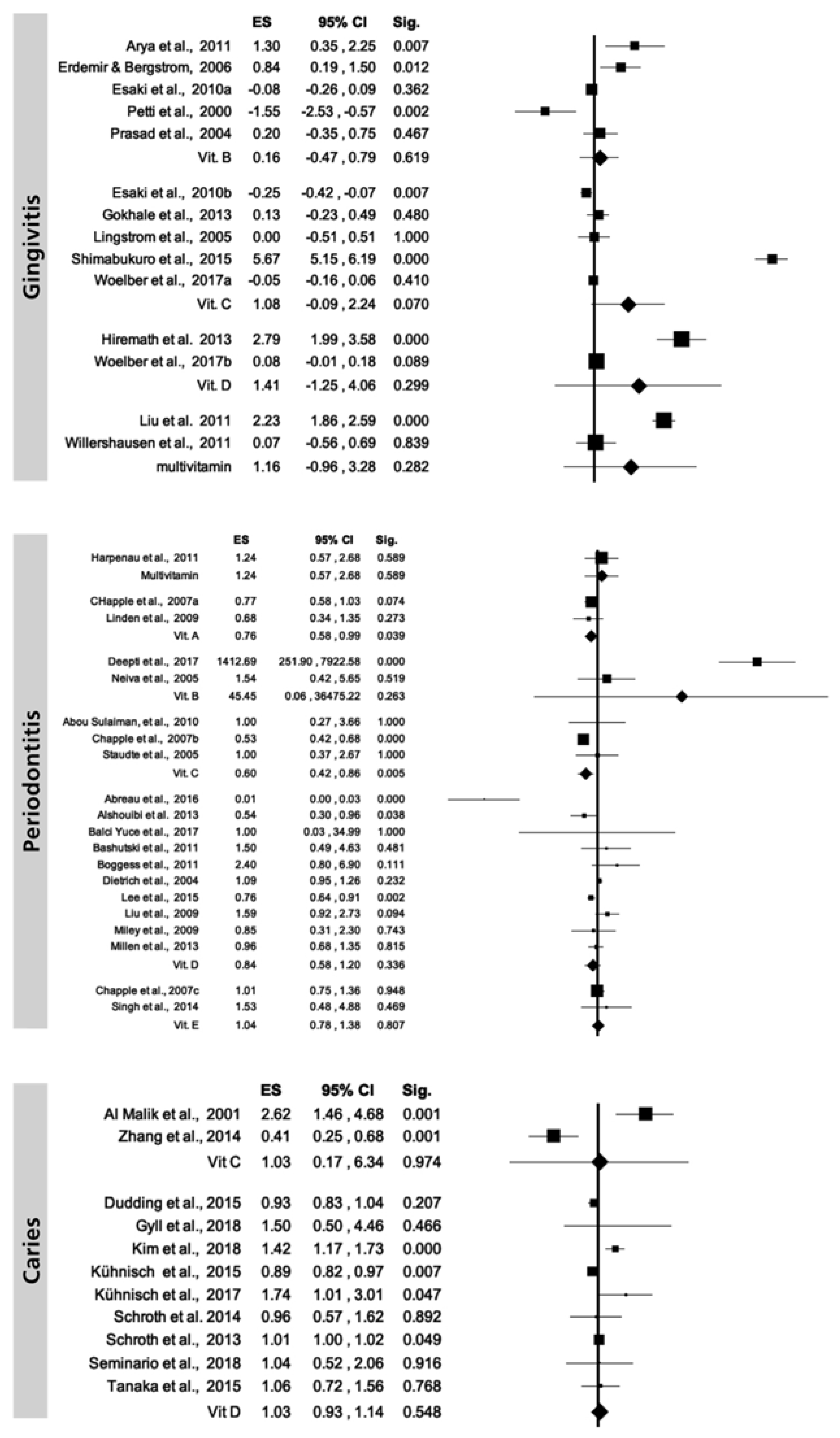
2.5. Data Collection, Summary Measures and Synthesis of Results
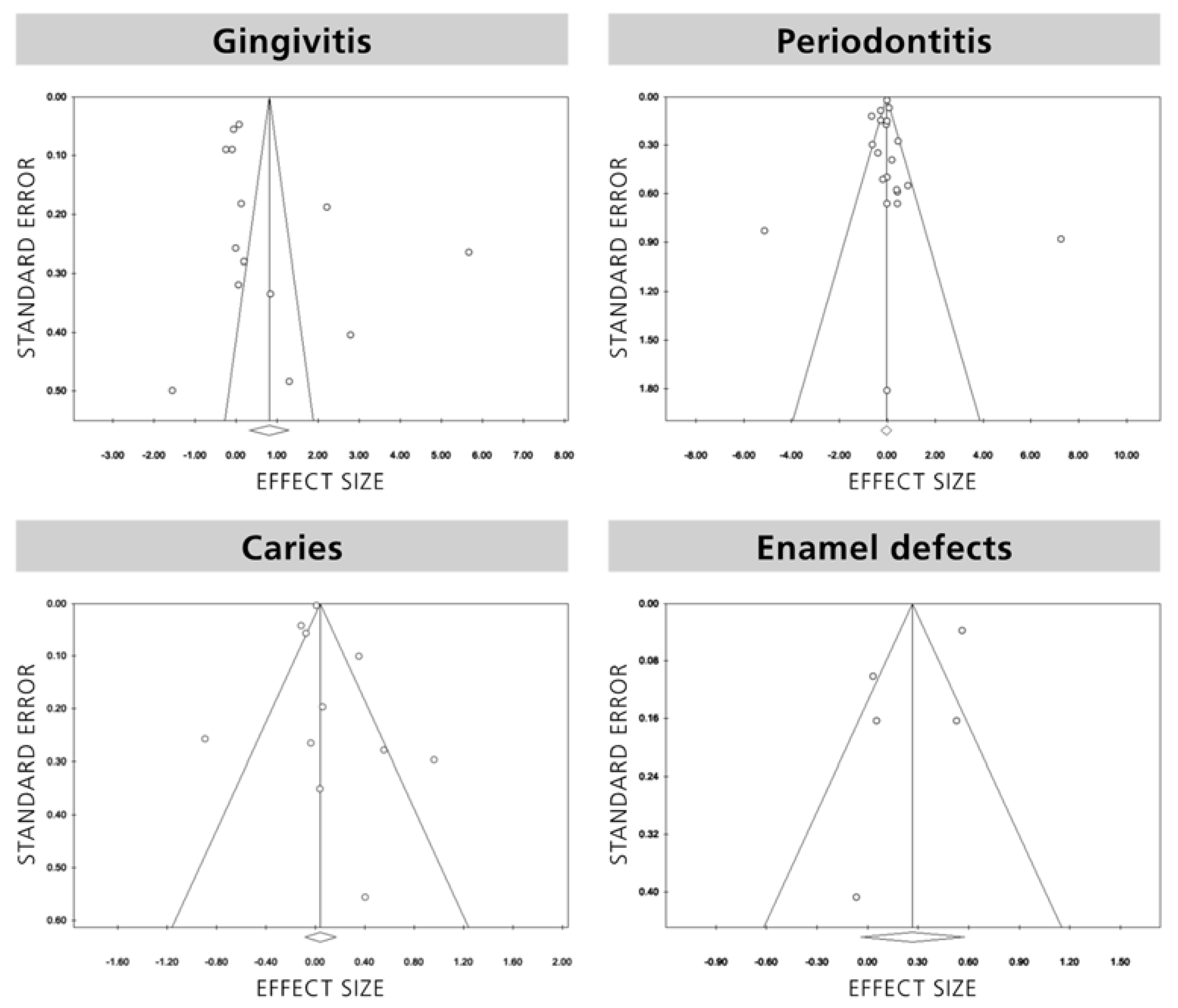
2.6. Assessment of Bias across Studies
3. Results
3.1. Gingival/Periodontal Disease
3.2. Hard Dental Pathological Processes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Varela-López, A.; Navarro-Hortal, M.D.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J.L. Nutraceuticals in Periodontal Health: A Systematic Review on the Role of Vitamins in Periodontal Health Maintenance. Molecules 2018, 20, 23. [Google Scholar]
- Dickinson, A.; MacKay, D. Health habits and other characteristics of dietary supplement users: A review. Nutr. J. 2014, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.J. The relationship between nutrition and systemic and oral well-being in older people. J. Am. Dent. Assoc. 2007, 138, 493–497. [Google Scholar] [CrossRef] [PubMed]
- McKenna, G.; Allen, P.F.; O’Mahony, D.; Flynn, A.; Cronin, M.; Da Mata, C.; Woods, N. Comparison of functionally orientated tooth replacement and removable partial dentures on the nutritional status of partially dentate older patients: A randomised controlled clinical trial. J. Dent. 2014, 42, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Gaewkhiew, P.; Sabbah, W.; Bernabé, E. Does tooth loss affect dietary intake and nutritional status? A systematic review of longitudinal studies. J. Dent. 2017, 67, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Graells, J.; Ojeda, R.M.; Muniesa, C.; Gonzalez, J.; Saavedra, J. Glossitis with linear lesions: An early sign of vitamin B12 deficiency. J. Am. Acad. Dermatol. 2009, 60, 498–500. [Google Scholar] [CrossRef] [PubMed]
- Jagelavičienė, E.; Vaitkevičienė, I.; Šilingaitė, D.; Šinkūnaitė, E.; Daugėlaitė, G. The Relationship between Vitamin D and Periodontal Pathology. Medicina 2018, 54, 3. [Google Scholar] [CrossRef]
- Psoter, W.J.; Reid, B.C.; Katz, R.V. Malnutrition and dental caries: A review of the literature. Caries Res. 2005, 39, 441–447. [Google Scholar] [CrossRef]
- Kanchanakamol, U.; Tuongratanaphan, S.; Tuongratanaphan, S.; Lertpoonvilaikul, W.; Chittai-Song, C.; Pattanaporn, K.; Navia, J.M.; Davies, G.N. Prevalence of developmental enamel defects and dental caries in rural pre-school Thai children. Commun. Dent. Health 1996, 13, 204–207. [Google Scholar]
- Gyll, J.; Ridell, K.; Öhlund, I.; Karlsland Åkeson, P.; Johansson, I.; Lif Holgerson, P. Vitamin D status and dental caries in healthy Swedish children. Nutr. J. 2018, 17, 11. [Google Scholar]
- Lussi, A.; Carvalho, T.S. Erosive tooth wear: A multifactorial condition of growing concern and increasing knowledge. Monogr. Oral. Sci. 2014, 25, 1–15. [Google Scholar] [PubMed]
- Li, H.; Zou, Y.; Ding, G. Dietary factors associated with dental erosion: A meta-analysis. PLoS ONE 2012, 7, e42626. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Harbord, R.M.; Egger, M.; Sterne, J.A. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tang, L.; Lin, Y.F.; Xie, G.F. Role of vitamin C in wound healing after dental implant surgery in patients treated with bone grafts and patients with chronic periodontitis. Clin. Implant Dent. Relat. Res. 2018, 20, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Balci Yuce, H.; Gokturk, O.; Aydemir Turkal, H.; Inanir, A.; Benli, I.; Demir, O. Assessment of local and systemic 25-hydroxy-vitamin D, RANKL, OPG, and TNF levels in patients with rheumatoid arthritis and periodontitis. J. Oral. Sci. 2017, 59, 397–404. [Google Scholar] [CrossRef]
- Deepti, J.; Tewari, S.; Narula, S.C.; Singhal, S.R.; Sharma, R.K. Effect of non-surgical periodontal therapy along with myo-inositol on high-sensitivity c-reactive protein and insulin resistance in women with polycystic ovary syndrome and chronic periodontitis: A randomized controlled trial. J. Periodontol. 2017, 88, 999–1011. [Google Scholar] [CrossRef]
- Abreu, O.J.; Tatakis, D.N.; Elias-Boneta, A.R.; Lopez Del Valle, L.; Hernandez, R.; Pousa, M.S.; Palacios, C. Low vitamin D status strongly associated with periodontitis in Puerto Rican adults. BMC Oral Health 2016, 16, 89. [Google Scholar] [CrossRef]
- Adegboye, A.R.; Boucher, B.J.; Kongstad, J.; Fiehn, N.E.; Christensen, L.B.; Heitmann, B.L. Calcium, vitamin D, casein and whey protein intakes and periodontitis among Danish adults. Public Health Nutr. 2016, 19, 503–510. [Google Scholar] [CrossRef]
- Gümüş, P.; Öztürk, V.Ö.; Bozkurt, E.; Emingil, G. Evaluation of the gingival inflammation in pregnancy and postpartum via 25-hydroxy-vitamin D3, prostaglandin E2 and TNF-α levels in saliva. Arch. Oral Biol. 2016, 63, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Pavlesen, S.; Mai, X.; Wactawski-Wende, J.; LaMonte, M.J.; Hovey, K.M.; Genco, R.J.; Millen, A.E. Vitamin D Status and Tooth Loss in Postmenopausal Females: The Buffalo Osteoporosis and Periodontal Disease (OsteoPerio) Study. J. Periodontol. 2016, 87, 852–863. [Google Scholar] [CrossRef] [PubMed]
- Woelber, J.P.; Bremer, K.; Vach, K.; König, D.; Hellwig, E.; Ratka-Krüger, P.; Al-Ahmad, A.; Tennert, C. An oral health optimized diet can reduce gingival and periodontal inflammation in humans—A randomized controlled pilot study. BMC Oral Health 2016, 17, 28. [Google Scholar] [CrossRef]
- Shimabukuro, Y.; Nakayama, Y.; Ogata, Y.; Tamazawa, K.; Shimauchi, H.; Nishida, T.; Ito, K.; Chikazawa, T.; Kataoka, S.; Murakami, S. Effects of an ascorbic acid-derivative dentifrice in patients with gingivitis: A double-masked, randomized, controlled clinical trial. J. Periodontol. 2015, 86, 27–35. [Google Scholar] [CrossRef]
- Lee, H.J.; Je, D.I.; Won, S.J.; Paik, D.I.; Bae, K.H. Association between vitamin D deficiency and periodontal status in current smokers. Community Dent. Oral Epidemiol. 2015, 43, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Chander Narula, S.; Kumar Sharma, R.; Tewari, S.; Kumar Sehgal, P. Vitamin E supplementation, superoxide dismutase status, and outcome of scaling and root planing in patients with chronic periodontitis: A randomized clinical trial. J. Periodontol. 2014, 85, 242–249. [Google Scholar] [CrossRef]
- Jimenez, M.; Giovannucci, E.; Krall Kaye, E.; Joshipura, K.J.; Dietrich, T. Predicted vitamin D status and incidence of tooth loss and periodontitis. Public Health Nutr. 2014, 17, 844–852. [Google Scholar] [CrossRef]
- Alshouibi, E.N.; Kaye, E.K.; Cabral, H.J.; Leone, C.W.; Garcia, R.I. Vitamin D and periodontal health in older men. J. Dent. Res. 2013, 92, 689–693. [Google Scholar] [CrossRef]
- Gokhale, N.H.; Acharya, A.B.; Patil, V.S.; Trivedi, D.J.; Thakur, S.L. A short-term evaluation of the relationship between plasma ascorbic acid levels and periodontal disease in systemically healthy and type 2 diabetes mellitus subjects. J. Diet Suppl. 2013, 10, 93–104. [Google Scholar] [CrossRef]
- Hiremath, V.P.; Rao, C.B.; Naik, V.; Prasad, K.V. Anti-inflammatory effect of vitamin D on gingivitis: A dose-response randomised control trial. Oral Health Prev. Dent. 2013, 11, 61–69. [Google Scholar] [CrossRef]
- Iwasaki, M.; Moynihan, P.; Manz, M.C.; Taylor, G.W.; Yoshihara, A.; Muramatsu, K.; Watanabe, R.; Miyazaki, H. Dietary antioxidants and periodontal disease in community-based older Japanese: A 2-year follow-up study. Public Health Nutr. 2013, 16, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Millen, A.E.; Andrews, C.A.; LaMonte, M.J.; Hovey, K.M.; Swanson, M.; Genco, R.J.; Wactawski-Wende, J. Vitamin D status and 5-year changes in periodontal disease measures among postmenopausal women: The Buffalo OsteoPerio Study. J. Periodontol. 2014, 85, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Teles, F.R.; Teles, R.P.; Martin, L.; Socransky, S.S.; Haffajee, A.D. Relationships among interleukin-6, tumor necrosis factor-α, adipokines, vitamin D, and chronic periodontitis. J. Periodontol. 2012, 83, 1183–1191. [Google Scholar] [CrossRef]
- Arya, R.; Gulati, S.; Kabra, M.; Sahu, J.K.; Kalra, V. Folic acid supplementation prevents phenytoin-induced gingival overgrowth in children. Neurology 2011, 76, 1338–1343. [Google Scholar] [CrossRef] [PubMed]
- Bashutski, J.D.; Eber, R.M.; Kinney, J.S.; Benavides, E.; Maitra, S.; Braun, T.M.; Giannobile, W.V.; McCauley, L.K. The impact of vitamin D status on periodontal surgery outcomes. J. Dent. Res. 2011, 90, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Boggess, K.A.; Espinola, J.A.; Moss, K.; Beck, J.; Offenbacher, S.; Camargo, C.A., Jr. Vitamin D status and periodontal disease among pregnant women. J. Periodontol. 2011, 82, 195–200. [Google Scholar] [CrossRef]
- Harpenau, L.A.; Cheema, A.T.; Zingale, J.A.; Chambers, D.W.; Lundergan, W.P. Effects of nutritional supplementation on periodontal parameters, carotenoid antioxidant levels, and serum C-reactive protein. J. Calif. Dent. Assoc. 2011, 39, 309–312. [Google Scholar]
- Liu, Y.; Jing, H.; Wang, J.; Zhang, R.; Zhang, Y.; Zhang, Y.; Xu, Q.; Yu, X.; Xue, C. Micronutrients decrease incidence of common infections in type 2 diabetic outpatients. Asia Pac. J. Clin. Nutr. 2011, 20, 375–382. [Google Scholar]
- Willershausen, B.; Ross, A.; Försch, M.; Willershausen, I.; Mohaupt, P.; Callaway, A. The influence of micronutrients on oral and general health. Eur. J. Med. Res. 2011, 10, 514–518. [Google Scholar] [CrossRef]
- Abou Sulaiman, A.E.; Shehadeh, R.M. Assessment of total antioxidant capacity and the use of vitamin C in the treatment of non-smokers with chronic periodontitis. J. Periodontol. 2010, 81, 1547–1554. [Google Scholar] [CrossRef]
- Esaki, M.; Morita, M.; Akhter, R.; Akino, K.; Honda, O. Relationship between folic acid intake and gingival health in non-smoking adults in Japan. Oral Dis. 2010, 16, 96–101. [Google Scholar] [CrossRef]
- Liu, K.; Meng, H.; Tang, X.; Xu, L.; Zhang, L.; Chen, Z.; Shi, D.; Feng, X.; Lu, R. Elevated plasma calcifediol is associated with aggressive periodontitis. J. Periodontol. 2009, 80, 1114–1120. [Google Scholar] [CrossRef]
- Llena, C.; Forner, L.; Vento, C. Anticalculus efficacy of a new dentifrice. Quintessence Int. 2009, 40, 497–501. [Google Scholar] [PubMed]
- Linden, G.J.; McClean, K.M.; Woodside, J.V.; Patterson, C.C.; Evans, A.; Young, I.S.; Kee, F. Antioxidants and periodontitis in 60-70-year-old men. J. Clin. Periodontol. 2009, 36, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Miley, D.D.; Garcia, M.N.; Hildebolt, C.F.; Shannon, W.D.; Couture, R.A.; Anderson Spearie, C.L.; Dixon, D.A.; Langenwalter, E.M.; Mueller, C.; Civitelli, R. Cross-sectional study of vitamin D and calcium supplementation effects on chronic periodontitis. J. Periodontol. 2009, 80, 1433–1439. [Google Scholar] [CrossRef]
- Chapple, I.L.; Milward, M.R.; Dietrich, T. The prevalence of inflammatory periodontitis is negatively associated with serum antioxidant concentrations. J. Nutr. 2007, 137, 657–664. [Google Scholar] [CrossRef]
- Dietrich, T.; Kaye, E.K.; Nunn, M.E.; Van Dyke, T.; Garcia, R.I. Gingivitis susceptibility and its relation to periodontitis in men. J. Dent. Res. 2006, 85, 1134–1137. [Google Scholar] [CrossRef]
- Erdemir, E.O.; Bergstrom, J. Relationship between smoking and folic acid, vitamin B12 and some haematological variables in patients with chronic periodontal disease. J. Clin. Periodontol. 2006, 33, 878–884. [Google Scholar] [CrossRef]
- Lingstrom, P.; Fure, S.; Dinitzen, B.; Fritzne, C.; Klefbom, C.; Birkhed, D. The release of vitamin C from chewing gum and its effects on supragingival calculus formation. Eur. J. Oral Sci. 2005, 113, 20–27. [Google Scholar] [CrossRef]
- Neiva, R.F.; Al-Shammari, K.; Nociti, F.H., Jr.; Soehren, S.; Wang, H.L. Effects of vitamin-B complex supplementation on periodontal wound healing. J. Periodontol. 2005, 76, 1084–1091. [Google Scholar] [CrossRef]
- Staudte, H.; Sigusch, B.W.; Glockmann, E. Grapefruit consumption improves vitamin C status in periodontitis patients. Br. Dent. J. 2005, 199, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Joshipura, K.J.; Dawson-Hughes, B.; Bischoff-Ferrari, H.A. Association between serum concentrations of 25-hydroxyvitamin D3 and periodontal disease in the US population. Am. J. Clin. Nutr. 2004, 80, 108–113. [Google Scholar]
- Prasad, V.N.; Chawla, H.S.; Goyal, A.; Gauba, K.; Singhi, P. Folic acid and phenytoin induced gingival overgrowth--is there a preventive effect. J. Indian Soc. Pedod. Prev. Dent. 2004, 22, 82–91. [Google Scholar] [PubMed]
- Krall, E.A.; Wehler, C.; Garcia, R.I.; Harris, S.S.; Dawson-Hughes, B. Calcium and vitamin D supplements reduce tooth loss in the elderly. Am. J. Med. 2001, 111, 452–456. [Google Scholar] [CrossRef]
- Petti, S.; Cairella, G.; Tarsitani, G. Nutritional variables related to gingival health in adolescent girls. Community Dent. Oral Epidemiol. 2000, 28, 407–413. [Google Scholar] [CrossRef]
- Syed, S.; Yassin, S.M.; Dawasaz, A.A.; Amanullah, M.; Alshahrani, I.; Togoo, R.A. Salivary 1,5-Anhydroglucitol and Vitamin Levels in Relation to Caries Risk in Children. Biomed. Res. Int. 2019, 4503450. [Google Scholar] [CrossRef]
- Kim, I.J.; Lee, H.S.; Ju, H.J.; Na, J.Y.; Oh, H.W. A cross-sectional study on the association between vitamin D levels and caries in the permanent dentition of Korean children. BMC Oral Health 2018, 18, 43. [Google Scholar] [CrossRef]
- Seminario, A.L.; Jumani, K.; Velan, E.; Scott, J.M.; Latimer, J.; Schroth, R.J. Suboptimal Serum Vitamin D Associated with Early Childhood Caries in Special Health Care Needs Children. J. Dent. Child. 2018, 85, 93–101. [Google Scholar]
- van der Tas, J.T.; Elfrink, M.E.C.; Heijboer, A.C.; Rivadeneira, F.; Jaddoe, V.W.V.; Tiemeier, H.; Schoufour, J.D.; Moll, H.A.; Ongkosuwito, E.M.; Wolvius, E.B.; et al. Foetal, neonatal and child vitamin D status and enamel hypomineralization. Community Dent. Oral. Epidemiol. 2018, 46, 343–351. [Google Scholar] [CrossRef]
- Wójcik, D.; Krzewska, A.; Szalewski, L.; Pietryka-Michałowska, E.; Szalewska, M.; Krzewski, S.; Pels, E.; Beń-Skowronek, I. Dental caries and vitamin D3 in children with growth hormone deficiency: A STROBE compliant study. Medicine 2018, 97, e981. [Google Scholar]
- Kühnisch, J.; Thiering, E.; Heinrich-Weltzien, R.; Hellwig, E.; Hickel, R.; Heinrich, J. Fluoride/vitamin D tablet supplementation in infants-effects on dental health after 10 years. Clin. Oral Investig. 2017, 21, 2283–2290. [Google Scholar] [CrossRef]
- Reed, S.G.; Voronca, D.; Wingate, J.S.; Murali, M.; Lawson, A.B.; Hulsey, T.C.; Ebeling, M.D.; Hollis, B.W.; Wagner, C.L. Prenatal vitamin D and enamel hypoplasia in human primary maxillary central incisors: A pilot study. Pediatr. Dent. J. 2017, 27, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Dudding, T.; Thomas, S.J.; Duncan, K.; Lawlor, D.A.; Timpson, N.J. Re-Examining the Association between Vitamin D and Childhood Caries. PLoS ONE 2015, 10, e0143769. [Google Scholar] [CrossRef] [PubMed]
- Kühnisch, J.; Thiering, E.; Kratzsch, J.; Heinrich-Weltzien, R.; Hickel, R.; Heinrich, J.; GINI-10 Plus Study Group; LISA-10 Plus Study Group. Elevated serum 25(OH)-vitamin D levels are negatively correlated with MIH. J. Dent. Res. 2015, 94, 381–387. [Google Scholar]
- Tanaka, K.; Hitsumoto, S.; Miyake, Y.; Okubo, H.; Sasaki, S.; Miyatake, N.; Arakawa, M. Higher vitamin D intake during pregnancy is associated with reduced risk of dental caries in young Japanese children. Ann. Epidemiol. 2015, 25, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Lavelle, C.; Tate, R.; Bruce, S.; Billings, R.J.; Moffatt, M.E. Prenatal vitamin D and dental caries in infants. Pediatrics 2014, 133, e1277–e1284. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chau, A.M.; Lo, E.C.; Chu, C.H. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Health 2014, 14, 7. [Google Scholar] [CrossRef]
- Schroth, R.J.; Levi, J.A.; Sellers, E.A.; Friel, J.; Kliewer, E.; Moffatt, M.E. Vitamin D status of children with severe early childhood caries: A case-control study. BMC Pediatr. 2013, 13, 174. [Google Scholar] [CrossRef]
- El Aidi, H.; Bronkhorst, E.M.; Huysmans, M.C.D.N.J.M.; Truin, G.J. Multifactorial Analysis of Factors Associated with the Incidence and Progression of Erosive Tooth Wear. Caries Res. 2011, 45, 303–312. [Google Scholar] [CrossRef]
- MacKeown, J.M.; Cleaton-Jones, P.E.; Fatti, P. Caries and micronutrient intake among urban South African children: A cohort study. Community Dent. Oral Epidemiol. 2003, 31, 213–220. [Google Scholar] [CrossRef]
- Al-Malik, M.I.; Holt, R.D.; Bedi, R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int. J. Paediatr. Dent. 2001, 11, 430–439. [Google Scholar]
- Aine, L.; Backström, M.C.; Mäki, R.; Kuusela, A.L.; Koivisto, A.M.; Ikonen, R.S.; Mäki, M. Enamel defects in primary and permanent teeth of children born prematurely. J. Oral Pathol. Med. 2000, 29, 403–409. [Google Scholar] [CrossRef]
- Hujoel, P.P.; Lingstrom, P. Nutrition, dental caries and periodontal disease: A narrative review. J. Clin. Periodontol. 2017, 44, S79–S84. [Google Scholar] [CrossRef]
- Hujoel, P.P. Vitamin D and dental caries in controlled clinical trials: Systematic review and meta-analysis. Nutrition Reviews 2012, 71, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Zuzannna Slebioda, Z.; Szponar, E.; Dorocka-Bobkowska, B. Vitamin D and Its Relevance in the Etiopathogenesis of Oral Cavity Diseases. Arch. Immunol. Ther. Exp. 2016, 64, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Seminario, A.L.; Velan, E. Vitamin D and Dental Caries in Primary Dentition. J. Dent. Child. 2016, 83, 114–119. [Google Scholar]
- Shaik, P.S.; Pachava, S. The Role of Vitamins and Trace Elements on Oral Health: A Systematic Review. Int. J. Med. Rev. 2017, 4, 22–31. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Sources | Type of Study | Vitamins | Oral Conditions | Quality Assessment |
|---|---|---|---|---|---|
| Li et al., [16] | Clin. Implant. Dent. Relat. Res. 2018, 20, 793–98 | CT | Vit. C | Periodontitis | Good |
| Balci Yuce et al., [17] | J. Oral. Sci. 2017, 59,:397–404 | CT | Vit. D | Periodontitis | Good |
| Deepti et al., [18] | J. Periodontol. 2017, 88, 999–1011 | RCT | Vit. B7 | Gingivitis/Periodontitis | Good |
| Abreu et al. [19] | BMC Oral Health 2016, 16, 89 | CCS | Vit. D | Periodontitis | Fair |
| Adegboye et al., [20] | Public Health Nutr. 2016, 19, 503–51 | CSS | Vit. D | Periodontitis | Good |
| Gümüş et al., [21] | Arch. Or. Biol. 2016, 63, 1–6 | CS | Vit. D | Periodontitis | Good |
| Pavlesen et al., [22] | J. Periodontol 2016; 87, 852–63 | RCS | Vit. D | Periodontitis/Tooth loss/Caries | Good |
| Woelber et al., [23] | BMC Oral Health 2016, 17, 28 | RCT | Vit. C, D | Gingivitis/Periodontitis | Good |
| Shimabukuro et al., [24] | J. Periodontol 2015, 86, 27–35 | RCT | Vit. C | Gingivitis | Good |
| Lee et al., [25] | Comm Dent. Oral Ep. 2015, 43, 471–8 | CSS | Vit. D | Periodontitis | Good |
| Singh et al., [26] | J. Periodontol 2014, 85, 242–9 | RCT | Vit. E | Periodontitis | Good |
| Jimenez et al., [27] | Public Health Nutr. 2014, 17, 844–52 | CSS | Vit. D | Periodontitis/Tooth loss | Good |
| Alshouibi et al., [28] | J. Dent. Res. 2013, 92, 689–93 | CSS | Vit. D | Periodontitis | Good |
| Gokhale et al., [29] | J. Diet. Suppl. 2013, 10, 93–104. | RCT | Vit. C | Periodontitis | Fair |
| Hiremath et al., [30] | Oral Health Prev. Dent. 2013, 11, 61–9 | RCT | Vit. D | Gingivitis | Good |
| Iwasaki et al., [31] | Public Health Nutr 2013, 16, 330–38 | RCS | Vit. A, D E, B6, B9, B12 | Tooth loss | Good |
| Millen et al., [32] | J. Periodontol 2013, 84, 1243–56 | CSS | Vit. D | Periodontitis | Good |
| Teles e t al., [33] | J. Periodontol 2012, 83, 1183–91 | CSS | Vit. D | Periodontitis | Fair |
| Arya et al., [34] | Neurology 2011, 76,1338–43 | RCT | Vit. B9 | Gingivitis | Fair |
| Bashutski et al., [35] | J. Dent. Res. 2011, 90, 1007–12 | RCT | Vit. D | Periodontitis | Good |
| Boggess et al., [36] | J. Periodontol 2011, 82, 195–200 | CCS | Vit. D | Periodontitis | Good |
| Harpenau et al., [37] | J. Calif. Dent. Assoc. 2011, 39, 309–18 | CT | Vit A, C, E, B6, B9, B12 | Gingivitis | Poor |
| Liu et al., [38] | Asia Pac. J. Clin. Nutr., 2011, 20, 375–82 | RCT | Vit. A, B1, B2, B6, B9, C, D, E | Gingivitis | Fair |
| Willershausen et al., [39] | Eur. J. Med. Res. 2011, 16, 514–18 | CSS | Vit. B complex, C, D, E | Gingivitis | Fair |
| Abou Sulaiman, et al., [40] | J. Periodontol 2010, 81, 1547–54 | RCT | Vit. C | Periodontitis | Fair |
| Esaki et al., [41] | Oral Disease 2010, 16,96–101 | CSS | Vit. A, B1, B2 B9, C | Gingivitis | Good |
| Liu, et al., [42] | J. Periodontol 2009, 80, 1114–20 | CT | Vit. D | Periodontitis | Fair |
| Llena et al., [43] | Quintessence Int. 2009, 40, 497–501 | CT | Vit. B3, pro-vitamin B5 | Gingivitis | Poor |
| Linden et al., [44] | J. Clin Periodontol. 2009, 36, 843–4 | CSS | Vit. A | Periodontitis | Good |
| Miley et al., [45] | J. Periodontol. 2009, 80, 1433–39 | CSS | Vit. D | Periodontitis | Good |
| Chapple, et al., [46] | J. Nutr. 2007, 137, 657–64 | CSS | Vit. A, C, E | Periodontitis | Good |
| Dietrich et al., [47] | J. Dent. Res 2006, 85, 1134–37 | CSS | Vit. C | Periodontitis | Good |
| Erdemir & Bergstrom [48] | J. Clin. Periodontol. 2006, 33, 878–84 | CSS | Vit B9, B12 | Periodontitis | Good |
| Lingstrom et al., [49] | Eur. J. Oral Sci. 2005, 113, 20–27 | CT | Vit. C | Gingivitis | Good |
| Neiva et al., [50] | J. Periodontol 2005, 76, 1084–91 | RCT | Vit. B complex | Periodontitis | Fair |
| Staudte et al., [51] | Br. Dent. J. 2005, 199, 213–7 | CT | Vit. C | Gingivitis | Fair |
| Dietrich et al., [52] | Am. J. Clin. Nutr. 2004, 80, 108–13 | CSS | Vit. D | Periodontitis | Good |
| Prasad et al., [53] | J. Indian Soc. Pedo Prev. Dent. 2004 22, 82–91 | CT | Vit. B9 | Gingivitis | Fair |
| Krall et al., [54] | Am. J. Med. 2001, 111, 452-456 | RCT | Vit. D | Tooth loss | Good |
| Petti et al., [55] | Community Dent. Oral Epidemiol. 2000, 28, 407–413 | CCS | Vit. A, B1, B2, B3, C | Gingivitis/Caries | Fair |
| (a) | |||||
| Syed et al., [56] | BioMed. Res. Int.2019, 4503450 | CSS | Vit. A, C, E | Caries | Poor |
| Gyll et al., [10] | Nutr. J.2018, 17, 11 | CSS | Vit. D | Caries | Good |
| Kim et al., [57] | BMC Oral Health2018, 18, 43 | CSS | Vit. D | Caries | Good |
| Seminario et al., [58] | J. Dent. Child2018, 3, 93–101 | CSS | Vit. D | Caries | Good |
| van der Tas et al., [59] | Community Dent. Oral Epidemiol.2018, 46, 343-51 | CS | Vit. D | Enamel defects | Good |
| Wójcik et al., [60] | Medicine2018, 97, 8(e9811) | CSS | Vit. D | Caries | Poor |
| Kühnisch et al., [61] | Clin. Oral Invest.2017, 21, 2283–2290 | RCS | Vit. D | Caries | Good |
| Reed et al., [62] | Ped. Dent. J.2017, 27, 21e28 | PiS | Vit. D | Enamel defects | Good |
| Pavlesen et al., [22] | J Periodontol2016; 87, 852–63 | CSS/PS | Vit. D | Periodontitis/Tooth loss/Caries | Good |
| Dudding et al., [63] | PLoS One2015, 10, e0143769 | MRS | Vit. D | Caries | Good |
| Kühnisch et al., [64] | J. Dent. Res.2015, 94, 381–87 | CSS | Vit. D | Enamel Defects | Good |
| Tanaka et al., [65] | Annals of Epidemiology2015, 25, 620e625 | PSA | Vit. D | Caries | Good |
| Schroth et al., [66] | Ped.2014, 133, e1277-e1284 | RCS | Vit D | Caries | Fair |
| Zhang et al., [67] | BMC Pub. Health2014, 14,7 | CSS | Vit. C | Caries/Erosion | Fair |
| Schroth et al., [68] | BMC Pediatrics2013, 13:174 | CCS | Vit. D | Caries | Good |
| El Aidi et al., [69] | Caries Res2011, 45, 303–312 | PS | vitamins (unspecified) | Erosion | Good |
| MacKeown et al., [70] | Community Dent Oral Epidemiol2003, 31, 213–20 | CSS | Vit. A, B complex, C, D | Caries | Good |
| Al Malik et al., [71] | Int. J. Paed. Dent.2001, 11, 430–39 | CSS | Vit. C | Caries/Erosion | Good |
| Aine et al., [72] | J Oral Pathol Med2000, 29, 403–9 | CCS | Vit. D | Enamel defects | Good |
| Petti et al., [55] | Community Dent Oral Epidemiol2000; 28, 407–13 | CCS | Vit. B12 | Gingivitis/Caries | Fair |
| (b) | |||||
| Author (Year) | Type of Study | Location | N Subjects Age-Range | M/F | Study Length | Vitamins Administration | Study Design (Groups Treatment) | Physical/Pathologic Condition | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Gümüş et al., (2016) [21] | CS | USA | 176 (19–40 yy) | F | --- | Vit. D --- | 3 groups: -pregnancy (n = 59) -post-partum (n = 47) -non pregnant woman (n = 70) Oral examination Vit. D in saliva | Pregnancy post-partum | In pregnancy and post-partum low level of Vit. D were statistically significantly associated to bleeding on probing |
| Shimabukuro et al., (2015) [24] | RCT | Japan | 300 (20–64 yy) | M/F | 3 months | Vit. C toothpaste | 2 groups: -toothpaste with Vit. C -control toothpaste | None | Vit. C toothpaste statistically significantly reduced gingival inflammation (p < 0.01) |
| Woelber et al., (2017) [23] | RCT | Germany | 15 (23–70 yy) | M/F | 8 weeks | Vit. C, D --- | 2 groups: -diet modification (n = 10) -no diet modification (n = 5) | None | In diet modification group gingival parameters improved (p < 0.05) |
| Gokhale et al., (2013) [29] | RCT | India | 120 (30–60 yy) | M/F | 2 weeks | Vit. C --- | 4 groups: -healthy subjects -chronic gingivitis -chronic periodontitis -chronic periodontitis and type 2 diabetes Scaling and root planing with or without vit. C supplementation (450 mg) | Type 2 diabetes | A statistically significantly reduction in the bleeding score in the following groups that received Vit. C: -chronic gingivitis -chronic periodontitis and type 2 diabetes |
| Hiremath et al., (2013) [30] | RCT | India | 110 (18–64 yy) | M/F | 3 months | Vit. D tablets | 4 groups: -2000 UI Vit. D -1000 UI Vit. D -500 UI Vit. D -placebo | None | Gingivitis scores improved: -2000 UI Vit. D: 2.4 at baseline to 0.3 at 3mo. -1000 UI Vit. D: 2.3 at baseline to 0.5 at 3 mo. -500 UI Vit. D: 2.2 at baseline to 0.8 at 3 mo. -placebo: 2.2 at baseline to 1.8 at 3 mo. |
| Arya et al., (2011) [34] | RCT | India | 120 (6–15 yy) | M/F | 6 months | Vit. B9 tablets | 2 groups: -Vit. B9 (5mg/die) (n = 62) -placebo (n = 68) Oral examination | Epilepsy | Vit. B9 group 21% developed PIGO Placebo group 88% developed PIGO |
| Liu et al., (2011) [38] | RCT | China | 196 (54–72 yy) | M/F | 6 months | Vit. A, B1, B2, B6, B9, C, D, E --- | 2 groups: -multivitamin formula (n = 97) -placebo (n = 99) | Type 2 diabetes | Gingivitis and oral ulcer incidences were lower in multivitamin formula group (p < 0.05) |
| Willershausen et al., (2011) [39] | CSS | Germany | 40 (24–30 yy) | M/F | 3 months | Vit. B complex, C, D, E --- | 2 groups: -multivitamin formula (n = 19) -no treatment (n = 21) Oral examination, dietary questionnaire, microbiology and blood analysis | None | A slight improvement of gingival inflammation in micronutrients group. |
| Esaki et al., (2010) [41] | CSS | Japan | 497 (---) | M/F | --- | Vit. A, B1, B2, B9, C --- | Oral examination Dietary questionnaire | None | Higher bleeding on probing scores statistically significantly associated to lower levels of Vit. C and Vit. B9 (p < 0.01) and Vit. A (p < 0.05) |
| Llena et al., (2009) [43] | CT | Spain | 4 8(20–34 yy) | M/F | 3 months +3 months | Vit. B3, Pro-vit. B5 toothpaste | 2 groups (cross-over design): -fluoridated toothpaste -fluoridated toothpaste with Vit. B3/Provit. B5, Oral examination/calculus presence | None | Fluoridated toothpaste with Vit. B3/Provit. B5 provided a statistically significant reduction in calculus presence (p = 0.01) |
| Erdemir &Bergstrom, (2006) [48] | CSS | Sweden | 88(30–69 yy) | M/F | --- | Vit. B9, B12 --- | 2 groups: -current smokers (n = 45) -non smokers (n = 43) Oral examination/Vit. B9, B12 serum level | None | In smokers higher gingival index scores and lower Vit. B9 levels (p < 0.05 for both) |
| Lingstrom et al., (2005) [49] | CT | Sweden | 30 (---) | M/F | 3 months | Vit. C gums | 2 groups: -5 pieces/day chewing gum vit. C/without vit. C, no gum use -10 pieces/day chewing gum with vit. C+ carbamide (30 mg + 30 mg), no gum use Calculus score/plaque/gingivitis | None | A significant reduction in the total calculus score after the use of Vit. C (33%) and Vit. C + carbamide (12%) gums compared with no gum use |
| Prasad et al., (2004) [53] | CT | India | 60 (8–13 yy) | M/F | 1 year | Vit. B9 tablets | 2 groups: -Vit. B9 (5mg/die) and oral hygiene instruction -oral hygiene instructions alone Oral examination | Epilepsy treated with phenytoin | Gingival overgrowth: 60% in oral hygiene instruction alone and 50% in Vit. B9 and oral hygiene instruction. Delay in onset of overgrowth in Vit. B9 and oral hygiene instruction |
| Petti et al., (2000) [55] | CCS | Italy | 54 (17–19 yy) | F | --- | Vit. A, B1, B2, B3, C --- | 2 groups: -gingivitis affected -no gingivitis affected Oral examination/ three-day food record | None | Vit. B1 and Vit. B2 levels statistically lower in subjects with gingivitis presence |
| (a) | |||||||||
| Balci Yuce et al., (2017) [17] | CT | Turkey | 53 (37–61 yy) | M/F | 6 weeks | Vit. D --- | 3 groups: -rheumatoid arthritis/periodontitis (RP) -periodontitis (P) -healthy (H) Treatment: initial periodontal treatment | Rheumatoid arthritis | Periodontal parameters statistically significantly improved in all groups Vit. D was higher in RP and P than in H group and decreased in RP group after treatment |
| Deepti et al., (2017) [18] | RCT | India | 60 (15–34 yy) | F | 3-6 months | Vit. B7 --- | 2 groups: - scaling-root planing+Vit. B7 - Vit. B7 | Polycystic ovary syndrome (PCOS) | In scaling-root planing+Vit. B7 group a statistically significantly reduction of C-reactive protein and insulin resistance at 3-6 mo. was found. Periodontal parameters also improved at 3-6 mo. |
| Abreu et al. (2016) [19] | CCS | Puerto Rico | 4 8(35-64 yy) | M/F | --- | Vit. D --- | 2 groups: -moderate/severe periodontitis -healthy | None | Lower OR for periodontitis (OR = 0.885; 95%CI= 0.785, 0.997) for each Vit. D unit increase |
| Adegboye et al., (2015) [20] | CSS | Denmark | 3287 (18–95 yy) | M/F | --- | Vit. D --- | Dietary questionnaire Oral examination | None | No association Vit. D levels between severe periodontitis presence |
| Lee et al., (2015) [25] | CSS | Korea | 6011 (---) | M/F | --- | Vit. D --- | Vit. D level Oral examination (CPI index) | None | No association between Vit. D level and periodontitis In smokers an association was found (OR 1.53, 95% CI 1.07–2.18) |
| Singh et al., (2014 [26]) | RCT | India | 60 (22–50 yy) | M/F | 3 months | Vit. E tablets | 2 groups: -periodontitis (n = 38): 19 treated with scaling/root planing (SRP) and 19 with SRP+300 IU Vit. E -healthy (n = 22) no treatment | None | Superoxide dismutase improved in both treatment groups, but was higher in SRP+300 IU Vit. E (p < 0.05) |
| Alshouibi et al. (2013) [28] | CS | USA | 562 (---) | M | --- | Vit. D --- | Vit. D intake Oral examination (4 times during 12 yy) | None | Vit. D intake ≥ 800 IU associated with lower odds of severe periodontal disease (OR = 0.67, 95% CI = 0.55-0.81) |
| Gokhale et al., (2013) [29] | RCT | India | 120 (30–60 yy) | NA | 2 weeks | Vit. C --- | 4 groups -healthy subjects; -chronic gingivitis; -chronic periodontitis, -chronic periodontitis and type 2 diabetes Scaling and root planing with or without vit. C supplementation (450 mg) | Type 2 diabetes | Statistically significant reduction of the bleeding score in the subgroups receiving Vit. C |
| Millen et al., (2013) [32] | CSS | USA | 920 (50–79 yy) | F | --- | Vit. D --- | -Vit. D level -oral examination | Post-menopausa | No association Vit. D and alveolar crestal height/ tooth loss OR = 0.96, (95%CI: 0.68–1.35). Vit. D associated to clinical attachment level and probing pocket depth (95%CI: 5–53%) |
| Teles et al., (2012 [33]) | CSS | USA | 56 (23–71 yy) | M/F | 6 months | Vit. D --- | Periodontal patients Scaling, root planing and hygiene instruction Bacteria in sub-gingival plaque Vit. D level | None | No associations between Vit. D and clinical and microbial parameters |
| Bashutski et al., (2011) [35] | RCT | USA | 40 (31–65 yy) | M/F | 6 months | Vit. D tablets | 2 groups: -periodontal surgery, Ca (1000 mg) and Vit. D (800 UI) supplements and self-administered teriparatide for 6 weeks - periodontal surgery, Ca (1000 mg) and Vit. D (800 UI) supplements and placebo for 6 weeks | None | Vit. D levels had no statistically significant impact on clinical attachment level and probing pocket depth improvements in teriparatide patients |
| Boggess et al., (2011) [36] | CCS | USA | 233 (21–33 yy) | F | --- | Vit. D --- | 2 groups: -pregnant woman with moderate to severe periodontitis -pregnant woman without periodontitis Vit. D level and Oral examination between 14 and 26 weeks of gestation | Pregnancy | Pregnant woman with periodontitis had statistically significant lower Vit. D levels and more likely to have Vit. D insufficiency (65% versus 29%) |
| Harpenau et al., (2011) [37] | CT | USA | 89 (18–70 yy) | M/F | 8 weeks | Vit. A, C, E, B6, B9, B12 tablets | 2 groups with mild to severe periodontitis: -multivitamin formula -placebo | None | Both groups showed non-significant trends for improvement in gingival, bleeding, probing depth and clinical attachment scores. |
| Abou Sulaiman, et al., (2010) [40] | RCT | Syria | 60 (23–65 yy) | M/F | 3 months | Vit. C tablets | 2 groups: -chronic periodontitis (n = 30)-15 subjects non-surgical treatment plus Vit. C and 15 subjects non surgical treatment alone -healthy controls(n = 30) | None | The two groups showed significant reductions in all clinical measures |
| Liu, et al., (2009) [41] | CT | China | 17 8(23–41 yy) | M/F | --- | Vit. D --- | 3 groups: -aggressive periodontitis (AgP) (n = 66) -chronic periodontitis (CP) (n = 52) -healthy controls (n = 60) Oral examination/Vit. D level | None | In AgP Vit. D was higher than in healthy controls (29.28 vs. 21.60 nmol/l; p < 0.05) and significantly correlated with bleeding index (r = 0.321; p < 0.05). |
| Linden et al., (2009) [44] | CSS | United Kingdom | 125 8(60–70 yy) | M | --- | Vit. A--- | Oral examination/questionnaire | None | Vit. A lower in the men with low-threshold periodontitis (p < 0.001) and high-threshold periodontitis (p = 0.002) compared to subjects without periodontitis |
| Miley et al., (2009) [45] | CSS | USA | 51 (50–80 yy) | M/F | --- | Vit. D tablets | 2 groups: -periodontal maintenance + Vit. D (400 IU/day) and Ca (1,000 mg/day) (n = 23) -periodontal maintenance only (n = 28) Oral examination | None | Periodontal maintenance + Vit. D (400 IU/day) and Ca (1000 mg/day) had lower but not statistically significant probing depths |
| Chapple, et al., (2007) [46] | CSS | USA | 11,480 (25–70 yy) | M/F | --- | Vit. A, C, E --- | Oral examination/questionnaire/ Vit. A, C, E level | None | Subjects with the highest values of serum Vit. C had 47% (95%CI 32, 58) lower odds of periodontitis than subjects with the lowest values (trend OR: 0.76, 95%CI 0.69, 0.84) |
| Dietrich et al., (2006) [47] | CSS | USA | 462 (47–92 yy) | M | --- | Vit. C --- | 2 groups: -periodontitis (n = 86) -no periodontitis (n = 376) Oral examination/Dietary questionnaire | None | Subjects with periodontitis had a Vit. C intake (mg) lower than subjects without periodontitis (120±201 vs 197±267) |
| Neiva et al., (2005) [50] | RCT | USA | 30 (38–65 yy) | M/F | 180 days | Vit. B complex tablets | 2 groups: - periodontal surgery and Vit-B for 30 days - periodontal surgery and placebo Oral examination/BANA test | None | Statistically significant difference between mean clinical attachment level between periodontal surgery and Vit. B (+0.41±0.12) and periodontal surgery and placebo (−0.52 ± 0.23) |
| Staudte et al., (2005) [51] | CT | Germany | 80 (22–75 yy) | M/F | 2 weeks | Vit. C diet | 2 groups: -healthy (n = 22) -periodontitis: using or not grapefruit (n = 38) Oral examination/Vit. C level | None | Bleeding index statistically significantly decreased after Grapefruit consumption |
| Dietrich et al., (2004) [52] | CSS | USA | 11,202 (20–75 yy) | M/F | --- | Vit. D --- | Oral examination/Vit. D level | None | Vit. D levels were statistically significantly lower in men/women >50 years with greater periodontal attachment loss |
| (b) | |||||||||
| Pavlesen et al., (2016) [22] | CSS/PS | USA | 70 (53–85 yy) | F | 5 years | Vit. D --- | Oral examination Vit. D level | Post-menopausa | No association between Vit. D levels and history or incidence of tooth loss caused by periodontal disease |
| Jimenez et al., (2014) [27] | CSS | USA | 42,730 (40–75 yy) | M | --- | Vit. D --- | Self-reported tooth loss and periodontitis Predicted Vit. D based on data on 1095 man | None | Men with highest levels of Vit. D exhibited a significantly lower risk of tooth loss compared with men with lowest levels |
| Iwasaki et al., (2013) [31] | RCS | Japan | 286 (75–80 yy) | M/F | 5 years | Vit. A, D E, B6, B9, B12 tablets | Dietary questionnaire (baseline and after 5 yy) Oral examination (functional tooth units) | None | Subjects with impaired dentition showed a significantly greater decline in nutrients intake (Vit. A and E) |
| Millen et al., (2013) [32] | CSS | USA | 920 (50–79 yy) | F | --- | Vit. D --- | Vit. D level Oral examination | Post-menopausa | No association between Vit. D and alveolar crestal height/ tooth loss OR = 0.96, (95%CI: 0.68–1.35) |
| (c) | |||||||||
| Author (Year) | Type of Study | Location | N Subjects Age-Range | M/F | Study Length | Vitamins Administration | Study Design (Groups Treatment) | Physical/Pathologic Condition | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Syed et al., (2019) [56] | CSS | Saudi Arabia | 100 (6–13 yy) | M/F | --- | Vit. A, C, E --- | Two groups: -DMFS/dmfs=0 -DMFS/dmfs>3 Saliva samples | None | Vit. A not statistically significantly correlated Vit. C and Vit. E. statistically significantly correlated to caries experience |
| Gyll et al., (2018) [10] | CSS | Sweden | 206 (8 yy) | M/F | --- | Vit. D --- | Vit. D serum level DMFT | None | Vit. D level statistically significantly associated to caries experience (OR = 0.96; p = 0.024) |
| Kim et al., (2018) [57] | CSS | Korea | 1688 (10-11 yy) | M/F | --- | Vit. D --- | Vit. D serum level DMFT | None | Vit. D < 0.25 nmol statistically significantly associated to caries experience (p < 0.05) |
| Seminario et al., (2018) [58] | CSS | USA | 276 (1–6 yy) | M/F | --- | Vit. D --- | Vit. D serum level DMFT | Neurologic and genetic disabilities | Vit. D level associated to caries in neurologic (p < 0.01) and genetic (p < 0.01) conditions |
| Wójcik et al., (2018) [60] | CS | Poland | 121 (6–17 yy) | M/F | 9 months | Vit. D --- | Human recombinant growth hormone Vit. D serum level DMFT | Growth problems | Caries prevalence reduced by 0.66 per each 10 ng/mL of Vit. D increase |
| Kühnisch et al., (2017) [61] | RCS | Germany | 406 (at birth) | M/F | 10 yy | Vit. D tablets | Vit. D supplementation Fluoride varnish dmfs | None | Vit. D + fluoride < 6 months associated to caries OR = 2.47 (95%CI = 1.32–4.63) Vit. D + fluoride >6 mo. associated to caries OR = 2.08 (95%CI = 1.00–4.32) |
| Pavlesen et al., (2016) [22] | CSS/PS | USA | 558 (53–85 yy) | F | 5 yy | Vit. D --- | Oral examination Vit. D serum level | Post-menopausa | Tooth loss due to caries associated to Vit. D OR = 1.03 (95%CI =0.62/1.72) |
| Dudding et al., (2015) [63] | MRS | UK | 5545 (3–8 yy) | M/F | --- | Vit- D --- | Vit. D serum level DMFT/dmft | None | Caries not statistically significantly associated to 10 ng/mL of Vit. D increase OR 0.93 (95%CI = 0.83-1.05) |
| Kühnisch et al., (2015) [64] | CSS | Germany | 1148 (--) | M/F | 10 yy | Vit. D tablets | Vit. D supplementation DMFT/dmft MIH | None | Vit. D statistically significantly associated to caries OR 0.90 (95%CI = 0.82–0.97) per each 10 ng/mL of Vit. D increase |
| Tanaka et al., (2015) [65] | PSA | Japan | 1210 mother-child (36–46 mo) | M/F | --- | Vit. D diet | Vit. D intake in pregnancy dmft in children | None | OR for dmft 1.06 (95%CI = 0.72–1.56) of Vit. D during pregnancy, quartiles 2, 3 OR for dmft 0.67 (95%CI = 0.44–1.22) of Vit. D during pregnancy, quartiles 4. |
| Schroth et al., (2014) [66] | RCS | Canada | 207 mother-child (--) | M/F | --- | Vit. D--- | Serum Vit. D in pregnancy ECC Enamel defects | None | Low serum Vit. D in pregnancy was statistically significantly associated ECC experience |
| Zhang et al., (2014) [67] | CSS | Hong Kong | 600 (12 yy) | M/F | 1 yy | Vit. C tablets | Vit, C intake DMFT BEWE | None | OR for caries experience 1.75 (95%CI = 1.14–2.69) in girls Vit. C supplements |
| Schroth et al., (2013) [68] | CCS | Canada | 266 (--) | M/F | 2 yy | Vit. D --- | Serum level Vit. D ECC | None | Low Vit. D associated to high ECC levels |
| MacKeown et al., (2003) [70] | CSS | South Africa | 259 (2–5 yy) | M/F | 4 yy | Vit. A, B complex, C, D diet | Vitamins intake dmft | None | Vit. B2, B7, B12 statistically significantly associated to caries incidence |
| Al Malik et al., (2001) [71] | CSS | Saudi Arabia | 987 (2–5 yy) | M/F | Vit. C --- | Vit. C intake dmft/s, Tooth Erosion | None | Vit. C intake not statistically significantly significant associated to caries. | |
| (a) | |||||||||
| van der Tas et al., (2018) [59] | CS | the Netherlands | 4750 (6 yy) | M/F | --- | Vit. D --- | Foetal Vit. D MIH at 6 yy | None | Vit. D not statistically significantly associated to MIH |
| Reed et al., (2017) [62] | PS | USA | 37 (--) | M/F | --- | Vit. D tablets | Vit. D supplementation (first year of age) | None | Maternal pregnant Vit. D level statistically significantly associated to Enamel hypoplasia in children |
| Kühnisch et al., (2017) [61] | RCS | Germany | 406 (at birth) | M/F | 10 yy | Vit. D tablets | Vit. D supplementation Fluoride varnish MIH | None | MIH not statistically significantly associated with Vit. D + Fluoride <6 mo. OR = 1.71 (95%CI = 0.67–4.38) and Vit. D + fluoride >6 mo. OR = 0.57 (95%CI = 0.21–1.55) |
| Kühnisch et al., (2015) [64] | CSS | Germany | 1148 (--) | M/F | 10 yy | Vit. D tablets | Vit. D supplémentation dmft/DMFT MIH | None | MIH statistically significantly associated to 10 ng/mL of Vit. D increase OR 0.89 (95%CI = 0.82–0.97) |
| Schroth et al., (2014) [66] | RCS | Canada | 207 mother-child (--) | M/F | --- | Vit. D --- | Serum Vit. D in pregnancy ECC Enamel defects | None | Low serum Vit. D in pregnancy was statistically significantly associated ECC experience |
| Zhang et al., (2014) [67] | CSS | Hong Kong | 600 (12 yy) | M/F | 1 yy | Vit. C diet | Vit. C intake DMFT BEWE | None | Tooth erosion not statistically significantly associated to frequency of Vit. C supplement drinks (p = 0.064) |
| El Aidi et al., (2011) [69] | PS | the Netherlands | 572 (10–12 yy) | M/F | --- | Vitamins (unspecified) tablets | Vitamins intake Tooth Erosion | None | Vitamins intake statistically significantly associated to erosion progression OR = 2.03 (95%CI = 1.14–3.62) |
| Al Malik et al., (2001) [71] | CSS | Saudi Arabia | 987 (2–5-yy) | M/F | --- | Vit. C --- | Vit. C intake dmft/s, Tooth Erosion | None | Vit. C intake statistically significantly associated to erosion. |
| Aine et al., (2000) [72] | CCS | Finland | 96 (1–2 yy) | M/F | --- | Vit. D tablets | Vit. D supplementation Enamel defects | Preterm children | Vit. D supplementation was not statistically significantly enamel defects. |
| (b) | |||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cagetti, M.G.; Wolf, T.G.; Tennert, C.; Camoni, N.; Lingström, P.; Campus, G. The Role of Vitamins in Oral Health. A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 938. https://doi.org/10.3390/ijerph17030938
Cagetti MG, Wolf TG, Tennert C, Camoni N, Lingström P, Campus G. The Role of Vitamins in Oral Health. A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(3):938. https://doi.org/10.3390/ijerph17030938
Chicago/Turabian StyleCagetti, Maria Grazia, Thomas Gerhard Wolf, Christian Tennert, Nicole Camoni, Peter Lingström, and Guglielmo Campus. 2020. "The Role of Vitamins in Oral Health. A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 3: 938. https://doi.org/10.3390/ijerph17030938
APA StyleCagetti, M. G., Wolf, T. G., Tennert, C., Camoni, N., Lingström, P., & Campus, G. (2020). The Role of Vitamins in Oral Health. A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(3), 938. https://doi.org/10.3390/ijerph17030938