Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Procedure
2.3. Measures
2.3.1. Predictor Variable: Sexual Satisfaction
2.3.2. Criterion Variables: Anxiety and Depression
2.3.3. Moderating Variables: Relationship Status and Gender
2.4. Data Analysis
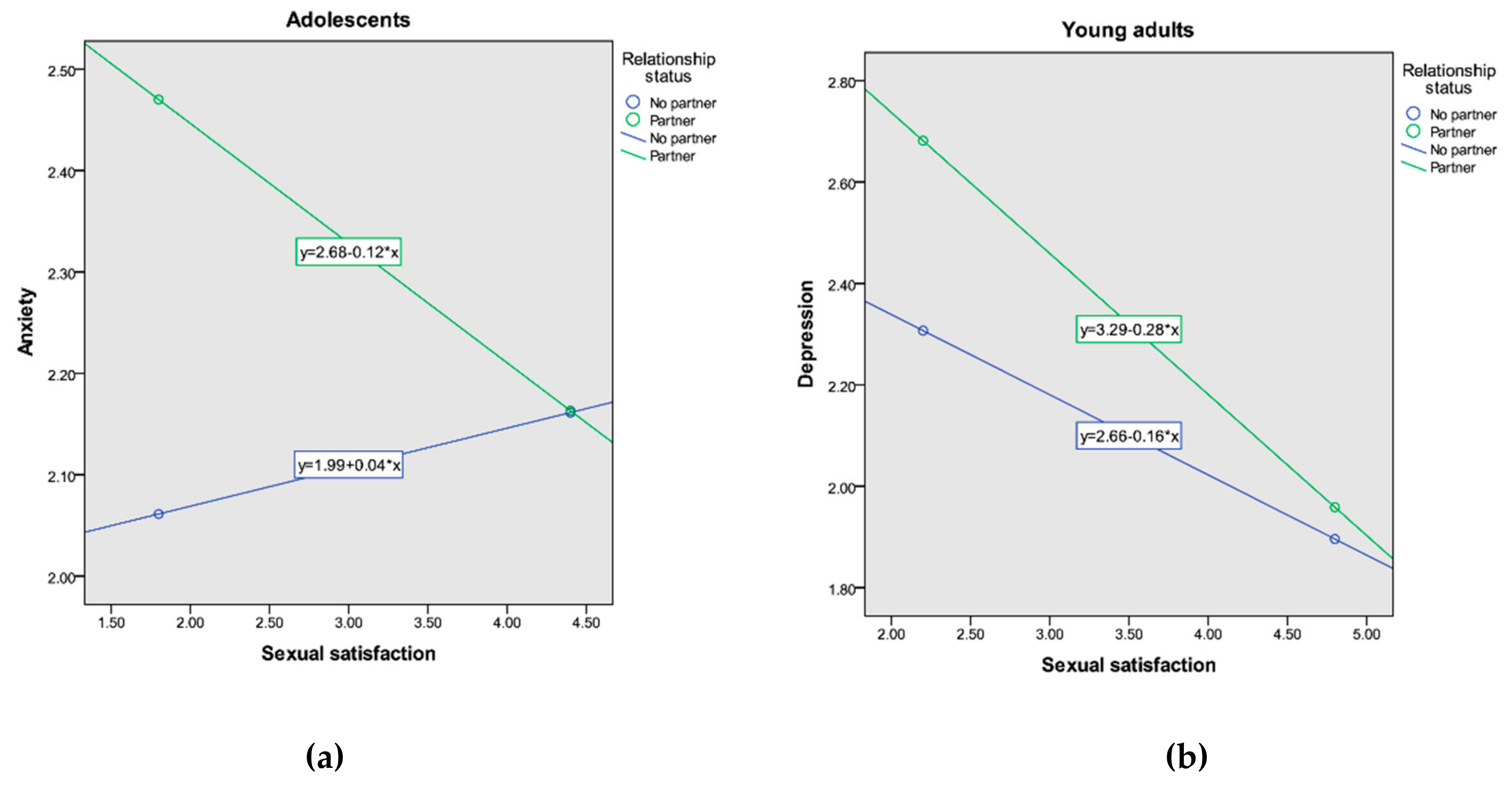
3. Results
4. Discussion
4.1. Limitations and Further Directions
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Boislard, M.; van de Bongardt, D.; Blais, M. Sexuality (and lack thereof) in adolescence and early adulthood: A review of the literature. Behav. Sci. 2016, 6, 8. [Google Scholar] [CrossRef]
- Moshman, D. Sexuality development in adolescence and beyond. Hum. Dev. 2014, 57, 287–291. [Google Scholar] [CrossRef]
- Arbeit, M.R. What does healthy sex look like among youth? Towards a skills-based model for promoting adolescent sexuality development. Hum. Dev. 2014, 57, 259–286. [Google Scholar] [CrossRef]
- Espinosa-Hernández, G.; Vasilenko, S.A.; McPherson, J.L.; Gutierrez, E.; Rodriguez, A. Brief report: The role of three dimensions of sexual well-being in adolescents’ life satisfaction. J. Adolesc. 2017, 55, 61–65. [Google Scholar] [CrossRef]
- Romeo, K.E.; Kelley, M.A. Incorporating human sexuality content into a positive youth development framework: Implications for community prevention. Child. Youth Serv. Rev. 2009, 31, 1001–1009. [Google Scholar] [CrossRef]
- Tolman, D.L.; McClelland, S.I. Normative sexuality development in adolescence: A decade in review, 2000-2009. J. Res. Adolesc. 2011, 21, 242–255. [Google Scholar] [CrossRef]
- Byers, E.S.; Rehman, U.S. Sexual well-being. In APA Handbook of Sexuality and Psychology; Tolman, D.L., Hamilton, L.M., Eds.; APA: Washington, DC, USA, 2014; Volume 1, pp. 317–337. [Google Scholar]
- World Health Organization. Measuring Sexual Health: Conceptual and Practical Considerations and Related Indicators; WHO: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/bitstream/handle/10665/70434/who_rhr_10.12_eng.pdf;jsessionid=BB8433DF476CE2BAEE9045BE08E52DEA?sequence=1 (accessed on 16 January 2020).
- McClelland, S.I. Who is the “self” in self-reports of sexual satisfaction? Research and policy implications. Sex. Res. Social Policy 2011, 8, 304–320. [Google Scholar] [CrossRef]
- Sprecher, S.; Cate, R.M.; Harvey, J.H.; Wenzel, A. Sexual satisfaction and sexual expression as predictors of relationship satisfaction and stability. In The Handbook of Sexuality in Close Relationships; Harvey, J.H., Wenzel, A., Sprecher, S., Eds.; Erlbaum: Mahwah, NJ, USA, 2004; pp. 235–256. [Google Scholar]
- Lawrence, K.A.; Byers, E.S. Sexual satisfaction in long-term heterosexual relationships: The interpersonal exchange model of sexual satisfaction. Pers. Relat. 1995, 2, 267–285. [Google Scholar] [CrossRef]
- Pascoal, P.M.; Narciso, I.D.S.B.; Pereira, N.M. What is sexual satisfaction? Thematic analysis of lay people’s definitions. J. Sex. Res. 2014, 51, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.A.; Willoughby, B.J.; Nelson, L.J. Young Adults’ Perceived Purposes of Emerging Adulthood: Implications for Cohabitation. J. Psychol. 2016, 150, 485–501. [Google Scholar] [CrossRef]
- López, F.; Carcedo, R.J.; Fernández-Rouco, N.; Blázquez, M.I.; Kilani, A. Sex differences in adolescent sexuality: Feelings and behaviours. An. Psicol. 2011, 27, 791–799. [Google Scholar]
- Sánchez-Fuentes, M.M.; Santos-Iglesias, P.; Sierra, J.C. A systematic review of sexual satisfaction. Int. J. Clin. Health Psychol. 2014, 14, 67–75. [Google Scholar] [CrossRef]
- Lehmann, V.; Tuinman, M.A.; Braeken, J.; Vingerhoets, A.J.; Sanderman, R.; Hagedoorn, M. Satisfaction with relationship status: Development of a new scale and the role in predicting well-being. J. Happiness Stud. 2015, 16, 169–184. [Google Scholar] [CrossRef]
- Blunt-Vinti, H.D.; Wheldon, C.; McFarlane, M.; Brogan, N.; Walsh-Buhi, E.R. Assessing relationship and sexual satisfaction in adolescent relationships formed online and offline. J. Adolesc. Health 2016, 58, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Melin, R.; Fugl-Meyer, K.S. Life satisfaction in 18-to 64-year-old Swedes: In relation to gender, age, partner and immigrant status. J. Rehabil. Med. 2002, 34, 239–246. [Google Scholar] [CrossRef]
- Van den Brink, F.; Vollmann, M.; Smeets, M.A.; Hessen, D.J.; Woertman, L. Relationships between body image, sexual satisfaction, and relationship quality in romantic couples. J. Fam. Psychol. 2018, 32, 466–474. [Google Scholar] [CrossRef]
- Umberson, D.; Thomeer, M.; Williams, K. Family status and mental health: Recent advances and future directions. In Handbook of the Sociology of Mental Health; Aneshensel, C.S., Phelan, J.C., Bierman, A., Eds.; Kluwer Academic Pubs: Dordrecht, The Netherlands, 2013; pp. 405–431. [Google Scholar]
- Connolly, J.A.; Goldberg, A. Romantic relationships in adolescence: The role of friends and peers in their emergence and development. In The Development of Romantic Relationships in Adolescence; Furman, W., Brown, B.B., Feiring, C., Eds.; Cambridge University Press: New York, NY, USA, 1999; pp. 266–290. [Google Scholar]
- Tolpin, L.H.; Cohen, L.H.; Gunthert, K.C.; Farrehi, A. Unique effects of depressive symptoms and relationship satisfaction on exposure and reactivity to daily romantic relationship stress. J. Soc. Clin. Psychol. 2006, 25, 565–583. [Google Scholar] [CrossRef]
- Campbell, L.; Simpson, J.A.; Boldry, J.; Kashy, D.A. Perceptions of conflict and support in romantic relationships: The role of attachment anxiety. J. Pers. Soc. Psychol. 2005, 88, 510–531. [Google Scholar] [CrossRef]
- Olson, J.S.; Crosnoe, R. Are you still bringing me down? Romantic involvement and depressive symptoms from adolescence to young adulthood. J. Health Soc. Behav. 2017, 58, 102–115. [Google Scholar] [CrossRef]
- Davila, J.; Karney, B.R.; Hall, T.W.; Bradbury, T.N. Depressive symptoms and marital satisfaction: Within-subject associations and the moderating effects of gender and neuroticism. J. Fam. Psychol. 2003, 17, 557–570. [Google Scholar] [CrossRef]
- Davila, J.; Steinberg, S.J.; Kachadourian, L.; Cobb, R.; Fincham, F. Romantic involvement and depressive symptoms in early and late adolescence: The role of a preoccupied relational style. Pers. Relatsh. 2004, 11, 161–178. [Google Scholar] [CrossRef]
- Joyner, K.; Udry, J.R. You don’t bring me anything but down: Adolescent romance and depression. J. Health Soc. Behav. 2000, 41, 369–391. [Google Scholar] [CrossRef]
- La Greca, A.M.; Moore, H. Adolescent peer relations, friendships, and romantic relationships: Do they predict social anxiety and depression? J. Clin. Child. Adol. Psychol. 2005, 34, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.L.; Hyde, J.S. A meta-analytic review of research on gender differences in sexuality, 1993–2007. Psychol. Bull. 2010, 136, 21–38. [Google Scholar] [CrossRef] [PubMed]
- McKinney, K.; Sprecher, S. Sexuality in Close Relationships; Lawrence Erlbaum Associates: New Jersey, NY, USA, 2014. [Google Scholar]
- Navarro-Bravo, B.; Ros-Segura, L.; Latorre-Postigo, J.M.; Escribano-Villafruela, J.C.; López-Honrubia, V.; Romero-Marchante, M. Hábitos, preferencias y satisfacción sexual en estudiantes universitarios. Rev. Clin. Med. Fam. 2010, 3, 150–157. [Google Scholar] [CrossRef][Green Version]
- Sánchez-Fuentes, M.M.; Sierra, J.C. Sexual satisfaction in a heterosexual and homosexual Spanish sample: The role of socio-demographic characteristics, health indicators, band relational factors. Sex. Relation. Ther. 2015, 30, 226–242. [Google Scholar] [CrossRef]
- Zahn-Waxler, C.; Shirtcliff, E.A.; Marceau, K. Disorders of childhood and adolescence: Gender and psychopathology. Annu. Rev. Clin. Psychol. 2008, 4, 275–303. [Google Scholar] [CrossRef] [PubMed]
- Cardila, F.; Martos, A.; Barragán, A.B.; Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J. Prevalencia de la depresión en España: Análisis de los últimos 15 años. European J. Investiga. 2015, 5, 267–279. [Google Scholar] [CrossRef]
- Martínez-Otero, V. Ansiedad en estudiantes universitarios: Estudio de una muestra de alumnos de la Facultad de Educación. Ensayos 2014, 29, 63–78. [Google Scholar]
- Orgilés, M.; Méndez, X.; Espada, J.P.; Carballo, J.L.; Piqueras, J.A. Síntomas de trastornos de ansiedad en niños y adolescentes: Diferencias en función de la edad y el sexo en una muestra comunitaria. Rev. Psiquiatr. Salud. Ment. 2012, 5, 115–120. [Google Scholar] [CrossRef]
- Bresin, K.; Schoenleber, M. Gender differences in the prevalence of nonsuicidal self-injury: A meta-analysis. Clin. Psychol. Rev. 2015, 38, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Bor, W.; Dean, A.J.; Najman, J.; Hayatbakhsh, R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust. N.Z. J. Psychiatry 2014, 48, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Flisher, A.J.; Hetrick, S.; McGorry, P. Mental health of young people: A global public-health challenge. The Lancet 2007, 369, 1302–1313. [Google Scholar] [CrossRef]
- Coles, M.E.; Ravid, A.; Gibb, B.; George-Denn, D.; Bronstein, L.R.; McLeod, S. Adolescent mental health literacy: Young people’s knowledge of depression and social anxiety disorder. J. Adol. Health 2016, 58, 57–62. [Google Scholar] [CrossRef]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry 2010, 10, 113. [Google Scholar] [CrossRef] [PubMed]
- Shindel, A.W.; Eisenberg, M.L.; Breyer, B.N.; Sharlip, I.D.; Smith, J.F. Sexual function and depressive symptoms among female North American medical students. J. Sex. Med. 2011, 8, 391–399. [Google Scholar] [CrossRef]
- Smith, J.F.; Breyer, B.N.; Eisenberg, M.L.; Sharlip, I.D.; Shindel, A.W. Sexual function and depressive symptoms among male North American medical students. J. Sex. Med. 2010, 7, 3909–3917. [Google Scholar] [CrossRef] [PubMed]
- Flynn, K.E.; Lin, L.; Bruner, D.W.; Cyranowski, J.M.; Hahn, E.A.; Jeffery, D.D.; Weinfurt, K.P. Sexual satisfaction and the importance of sexual health to quality of life throughout the life course of US adults. J. Sex. Med. 2016, 13, 1642–1650. [Google Scholar] [CrossRef]
- Kalmbach, D.A.; Pillai, V.; Kingsberg, S.A.; Ciesla, J.A. The transaction between depression and anxiety symptoms and sexual functioning: A prospective study of premenopausal, healthy women. Arch. Sex. Behav. 2015, 44, 1635–1649. [Google Scholar] [CrossRef]
- Yildiz, Y.; Akyol, M.; Alacacioglu, A.; Kucukzeybek, Y.; Asik, N.; Taskaynatan, H.; Tarhan, M.O. Sexual satisfaction, anxiety, depression and quality of life among Turkish gynecological cancer patients. Ann. Oncol. 2016, 27, 296–312. [Google Scholar] [CrossRef]
- Davison, S.L.; Bell, R.J.; LaChina, M.; Holden, S.L.; Davis, S.R. The relationship between self-reported sexual satisfaction and general well-being in women. J. Sex. Med. 2009, 6, 2690–2697. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, H.; Gonçalves Soares, A.L.; Bierhals, I.O.; Machado, A.; Fernandes, M.P.; Hirschmann, R.; Menezes, A. Age of sexual initiation and depression in adolescents: Data from the 1993 Pelotas (Brazil) Birth Cohort. J. Affec. Disord. 2017, 221, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Vasilenko, S.A. Age-varying associations between non-marital sexual behavior and depressive symptoms across adolescence and young adulthood. Dev. Psychol. 2017, 53, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Whitton, S.W.; Weitbrecht, E.M.; Kuryluk, A.D.; Bruner, M.R. Committed dating relationships and mental health among college students. J. Ame. Coll. Health 2013, 61, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Snell, W.E. The multidimensional sexual self-concept questionnaire. In Handbook of Sexuality-Related Measures, 3rd ed.; Fisher, T.D., Davis, C.M., Yarber, W.L., Davis, S.L., Eds.; Sage: New York, CA, USA, 2011; pp. 537–549. [Google Scholar]
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90: An outpatient psychiatric rating scale-preliminary report. Psychopharmacoll. Bull. 1973, 9, 13–28. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-based Approach; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Baumeister, R.F.; Catanese, K.R.; Vohs, K.D. Is there a gender difference in strength of sex drive? Theoretical views, conceptual distinctions, and a review of relevant evidence. Pers. Soc. Psychol. Rev. 2001, 5, 242–273. [Google Scholar] [CrossRef]
- Hantsoo, L.; Epperson, C.N. Anxiety disorders among women: A female lifespan approach. Focus 2017, 15, 162–172. [Google Scholar] [CrossRef]
- Sigmon, S.T.; Pells, J.J.; Boulard, N.E.; Whitcomb-Smith, S.; Edenfield, T.M.; Hermann, B.A.; Kubik, E. Gender differences in self-reports of depression: The response bias hypothesis revisited. Sex. Roles. 2005, 53, 401–411. [Google Scholar] [CrossRef]
- Davila, J. Depressive symptoms and adolescent romance: Theory, research, and implications. Child. Develop. Pers. 2008, 2, 26–31. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Palo, W.A.; Chen, Y.; Dragheim, M.; Clayton, A.H. Treatment-emergent sexual dysfunction in randomized trials of vortioxetine for major depressive disorder or generalized anxiety disorder: A pooled analysis. CNS Spectr. 2016, 21, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Huang, C.Y.S.; Shen, A.C.T. Romantic involvement and adolescents’ academic and psychosocial functioning in Chinese societies. Child. Youth Serv Rev. 2019, 96, 108–117. [Google Scholar] [CrossRef]
- St John, P.D.; Montgomery, P.R. Marital status, partner satisfaction, and depressive symptoms in older men and women. Can. J. Psychiatry 2009, 54, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Crawford, M.; Popp, D. Sexual double standards: A review and methodological critique of two decades of research. J. Sex. Res. 2003, 40, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Peleg-Sagy, T.; Shahar, G. The prospective associations between depression and sexual satisfaction among female medical students. J. Sex. Med. 2013, 10, 1737–1743. [Google Scholar] [CrossRef]
- Wilkins, A.; Limburg, A. Gender, class, and campus sexual cultures: white first-generation college students and the transition to college. In The Cambridge Handbook of Sexual Development: Childhood and Adolescence; Lamb, S., Gilbert, J., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 221–240. [Google Scholar]
- Rosen, N.O.; Dubé, J.P.; Corsini-Munt, S.; Muise, A. Partners experience consequences, too: A comparison of the sexual, relational, and psychological adjustment of women with sexual interest/arousal disorder and their partners to control couples. J. Sex. Med. 2019, 16, 83–95. [Google Scholar] [CrossRef]
- Stephenson, K.R.; Meston, C.M. The conditional importance of sex: Exploring association between sexual well-being and life satisfaction. J. Sex. Marital. Ther. 2015, 41, 25–38. [Google Scholar] [CrossRef]
- Braithwaite, S.; Holt-Lunstad, J. Romantic relationships and mental health. Curr. Opin. Psychol. 2017, 13, 120–125. [Google Scholar] [CrossRef]
- Price, M.; Hides, L.; Cockshaw, W.; Staneva, A.; Stoyanov, S. Young love: Romantic concerns and associated mental health issues among adolescent help-seekers. Behav. Sci. 2016, 6, 9. [Google Scholar] [CrossRef]
- O’Connor, E.; Gaynes, B.; Burda, B.; Williams, C.; Whitlock, E. Screening for suicide risk in primary care: A systematic evidence review for the US Preventive Service Task Force Agency for Healthcare Research and Quality. Report 2013, 158, 741–754. [Google Scholar]
- Byers, E.S.; Demmons, S.; Lawrance, K. Sexual satisfaction within dating relationships: A test of the interpersonal exchange model of sexual satisfaction. J. Soc. Pers. Relatsh. 1998, 15, 257–267. [Google Scholar] [CrossRef]
- Lefkowitz, E.S.; Vasilenko, S.A. Healthy sex and sexual health: New directions for studying outcomes of sexual health. In Positive and Negative Outcomes of Sexual Behaviors. New Directions for Child and Adolescent Development; Lefkowitz, E.S., Vasilenko, S.A., Eds.; Wiley: San Francisco, CA, USA, 2014; pp. 87–98. [Google Scholar] [CrossRef]
- Bodenmann, G.; Ledermann, T.; Bradbury, T.N. Stress, sex, and satisfaction in marriage. Pers. Relatsh. 2007, 14, 551–569. [Google Scholar] [CrossRef]
- Scroggs, B.; Madrigal, R.; Faflick, N. Adolescent sexual guilt and the development of self-esteem during the transition to adulthood: The moderating effect of race. Sex. Cult. 2019, 23, 641–656. [Google Scholar] [CrossRef]
- McCabe, M.P.; Sharlip, I.D.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Segraves, R.T. Definitions of sexual dysfunctions in women and men: A consensus statement from the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 135–143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Groups | Adolescents | Young Adults | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SE | F | ηp2 | Mean | SE | F | ηp2 | ||
| Sexual satisfaction | Gender | 2.93 | 0.004 | 0.82 | 0.001 | ||||
| Men | 3.38 | 0.07 | 3.57 | 0.05 | |||||
| Women | 3.23 | 0.05 | 3.51 | 0.04 | |||||
| Partner status | 168.68 *** | 0.173 | 402.77 *** | 0.317 | |||||
| No partner | 2.73 | 0.04 | 2.87 | 0.04 | |||||
| Partner | 3.88 | 0.08 | 4.20 | 0.05 | |||||
| Gender × Partner st. | 0.46 | 0.000 | 0.54 | 0.001 | |||||
| Men without partner | 2.82 | 0.06 | 2.92 | 0.06 | |||||
| Men with partner | 3.95 | 0.12 | 4.21 | 0.08 | |||||
| Women without partner | 2.65 | 0.06 | 2.81 | 0.06 | |||||
| Women with partner | 3.82 | 0.09 | 4.20 | 0.06 | |||||
| Anxiety | Gender | 17.68 *** | 0.021 | 21.11 *** | 0.024 | ||||
| Men | 1.99 | 0.05 | 1.85 | 0.04 | |||||
| Women | 2.28 | 0.04 | 2.08 | 0.03 | |||||
| Partner status | 2.05 | 0.003 | 6.71 ** | 0.008 | |||||
| No partner | 2.09 | 0.03 | 2.03 | 0.03 | |||||
| Partner | 2.18 | 0.06 | 1.90 | 0.04 | |||||
| Gender × Partner st. | 0.248 | 0.000 | 2.61 | 0.003 | |||||
| Men without partner | 1.93 | 0.05 | 1.95 | 0.05 | |||||
| Men with partner | 2.06 | 0.09 | 1.74 | 0.06 | |||||
| Women without partner | 2.24 | 0.05 | 2.10 | 0.05 | |||||
| Women with partner | 2.31 | 0.07 | 2.06 | 0.05 | |||||
| Depression | Gender | 29.88 *** | 0.036 | 53.17 *** | 0.058 | ||||
| Men | 2.01 | 0.05 | 1.94 | 0.04 | |||||
| Women | 2.37 | 0.04 | 2.31 | 0.03 | |||||
| Partner status | 0.03 | 0.000 | 8.35 ** | 0.010 | |||||
| No partner | 2.19 | 0.03 | 2.20 | 0.03 | |||||
| Partner | 2.20 | 0.06 | 2.05 | 0.04 | |||||
| Gender × Partner st. | 1.59 | 0.002 | 7.35 ** | 0.008 | |||||
| Men without partner | 1.96 | 0.05 | 2.08 | 0.05 | |||||
| Men with partner | 2.06 | 0.09 | 1.80 | 0.06 | |||||
| Women without partner | 2.41 | 0.05 | 2.32 | 0.05 | |||||
| Women with partner | 2.34 | 0.07 | 2.31 | 0.05 | |||||
| Adolescents | Young Adults | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety | Depression | Anxiety | Depression | |||||||||
| ΔR2 | B | 95% CI | ΔR2 | B | 95% CI | ΔR2 | B | 95% CI | ΔR2 | B | 95% CI | |
| Step 1 | 0.037 *** | 0.061 *** | 0.045 *** | 0.111*** | ||||||||
| Sexual satisfaction | 0.05 | (−0.11, −0.21) | 0.02 | (−0.14, 0.18) | −0.07 | (−0.22, 0.07) | −0.23 ** | (−0.37, −0.09) | ||||
| Gender | 0.31 | (−0.01, 0.62) | 0.48 ** | (0.17, 0.79) | 0.25 | (−0.05, 0.56) | 0.17 | (−0.13, 0.47) | ||||
| Relationship status | 0.64 ** | (0.16, 1.11) | 0.38 | (−0.09, 0.84) | (−0.15, 0.72) | 0.68 ** | (0.21, 1.06) | |||||
| Step 2 | 0.007 * | 0.003 | 0.002 | 0.007 * | ||||||||
| Sexual satisfaction × Gender | 0.000 | −0.01 | (−0.10, 0.09) | 0.000 | −0.03 | (−0.12, 0.7) | 0.000 | −0.01 | (−0.10, 0.07) | 0.001 | 0.05 | (−0.04, 0.13) |
| Sexual satisfaction × Relation st. | 0.007 * | −0.16* | (−0.28, −0.03) | 0.003 | −0.09 | (−0.22, 0.03) | 0.002 | −0.07 | (−0.18, 0.04) | 0.006 * | −0.13 * | (−0.24, −0.03) |
| Total R2 | 0.044 *** | 0.064 *** | 0.047 *** | 0.118 *** | ||||||||
| n | 809 | 809 | 873 | 873 | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carcedo, R.J.; Fernández-Rouco, N.; Fernández-Fuertes, A.A.; Martínez-Álvarez, J.L. Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 841. https://doi.org/10.3390/ijerph17030841
Carcedo RJ, Fernández-Rouco N, Fernández-Fuertes AA, Martínez-Álvarez JL. Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults. International Journal of Environmental Research and Public Health. 2020; 17(3):841. https://doi.org/10.3390/ijerph17030841
Chicago/Turabian StyleCarcedo, Rodrigo J., Noelia Fernández-Rouco, Andrés A. Fernández-Fuertes, and José Luis Martínez-Álvarez. 2020. "Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults" International Journal of Environmental Research and Public Health 17, no. 3: 841. https://doi.org/10.3390/ijerph17030841
APA StyleCarcedo, R. J., Fernández-Rouco, N., Fernández-Fuertes, A. A., & Martínez-Álvarez, J. L. (2020). Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults. International Journal of Environmental Research and Public Health, 17(3), 841. https://doi.org/10.3390/ijerph17030841